Embed Size (px)
Citation preview
Rising trend of cases of dengue fever admitted in a
tertiary care hospital in Vadodara - A retrospective
study
ww.sciencedirect.com
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e6
Available online at w
ScienceDirect
journal homepage: www.elsevier .com/locate/apme
Original Article
Rising trend of cases of dengue fever admitted in atertiary care hospital in Vadodara e A retrospectivestudy
Varsha Godbole a,*, Himanshu Rana b, Kedar Mehta c, Falgun Gosai d
a Professor & Head, Internal Medicine, GMERS Medical College, Gotri, Vadodara, Gujarat, Indiab Associate Professor, Internal Medicine, GMERS Medical College, Gotri, Vadodara, Gujarat, Indiac Assistant Professor, Community Medicine, GMERS Medical College, Gotri, Vadodara, Gujarat, Indiad Assistant Professor, Internal Medicine, GMERS Medical College, Gotri, Vadodara, Gujarat, India
a r t i c l e i n f o
Article history:
Received 20 October 2014
Accepted 30 October 2014
Available online xxx
Keywords:
Dengue
Dengue haemorrhagic fever
Thrombocytopenia
* Corresponding author. Tel.: þ91 9879181E-mail address: [email protected] (V
Please cite this article in press as: GodbolVadodara e A retrospective study, Apollo
http://dx.doi.org/10.1016/j.apme.2014.10.0010976-0016/Copyright © 2014, Indraprastha M
a b s t r a c t
Background & objective: Dengue has become a serious public threat globally. Increasing
number of cases are seen during the monsoon season. The incidence is increasing each
year. We undertook this study to document the rise in cases during 2013 and to study the
clinical spectrum of patients admitted in a tertiary care hospital.
Material and methods: It was a retrospective study of cases admitted from July to December
2013. The clinical profile, complications and outcome of the patients was studied. The
number of cases were compared with all the admitted as well as fever patients of 2013 and
with cases of the previous two consecutive years.
Results: Out of 63 patients, 30 (47.6%) belonged to the age group of 13e23 years, predomi-
nantly males (84%) and from urban areas. The presenting symptoms included, fever (100%),
myalgia (61.9%) vomiting (49.2%), abdominal pain, nausea and headache. Sixty patients
(95.2%) had non-severe dengue while 3 (4.8%) had dengue haemorrhagic fever.
Sevenpatients (11%)hadcomplications in the formofascites,pleural effusionandbleeding.
Discussion: Ourstudyconfirmstheseasonaloccurrenceof thecases. It isalso inaccordancewith
the other studies as regards the overall clinical spectrum. Most of our patients were from the
urban areas which is not comparable with other studies. Comparison with the previous
2 years as well as with the total admitted and fever cases revealed a statistically significant (p
value < 0.0001) rise in the number of cases during 2013. The clinical profile showed mostly
uncomplicated cases with good prognosis, who responded well to early treatment with hy-
dration and supportive therapy.
Conclusion: Documentation of a rise in the number of cases will have a major impact on
recognizing the burden of the disease and in formulating a plan for containment of cases in
the community.
Copyright © 2014, Indraprastha Medical Corporation Ltd. All rights reserved.
673; fax: þ91 265 2398009. Godbole).
e V, et al., Rising trend oMedicine (2014), http:/
edical Corporation Ltd. A
.
f cases of dengue fever admitted in a tertiary care hospital in/dx.doi.org/10.1016/j.apme.2014.10.001
ll rights reserved.
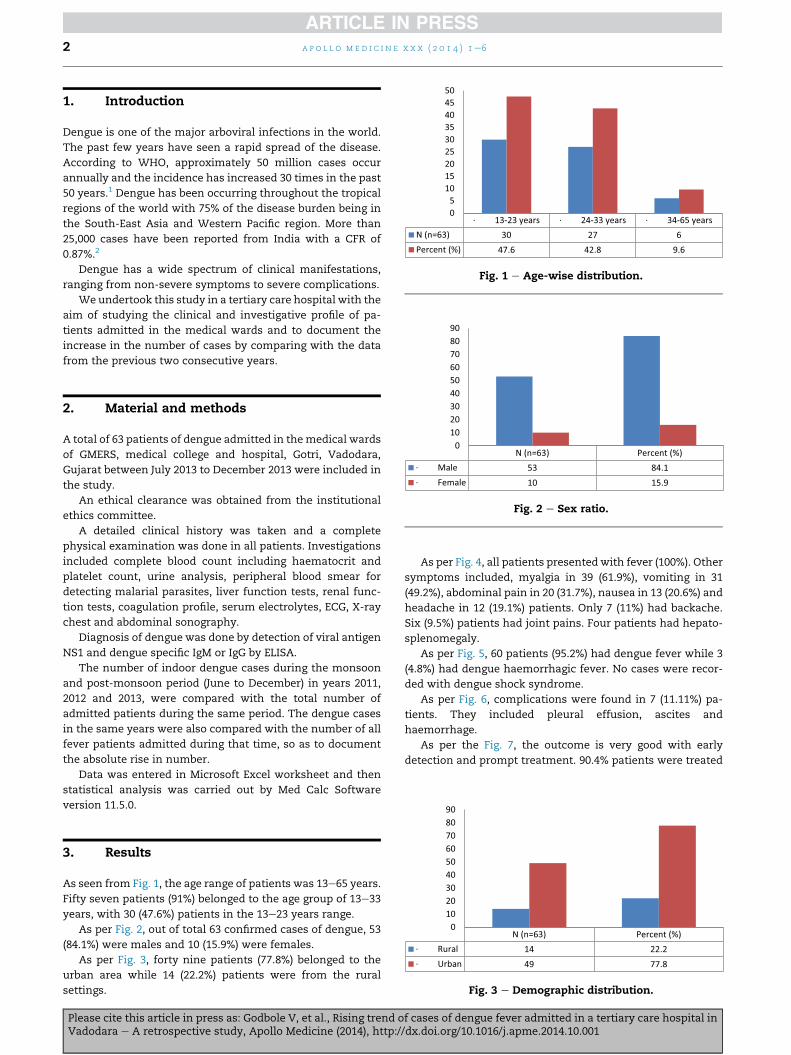
Fig. 1 e Age-wise distribution.
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e62
1. Introduction
Dengue is one of the major arboviral infections in the world.
The past few years have seen a rapid spread of the disease.
According to WHO, approximately 50 million cases occur
annually and the incidence has increased 30 times in the past
50 years.1 Dengue has been occurring throughout the tropical
regions of the world with 75% of the disease burden being in
the South-East Asia and Western Pacific region. More than
25,000 cases have been reported from India with a CFR of
0.87%.2
Dengue has a wide spectrum of clinical manifestations,
ranging from non-severe symptoms to severe complications.
We undertook this study in a tertiary care hospital with the
aim of studying the clinical and investigative profile of pa-
tients admitted in the medical wards and to document the
increase in the number of cases by comparing with the data
from the previous two consecutive years.
Fig. 2 e Sex ratio.
2. Material and methods
A total of 63 patients of dengue admitted in themedical wards
of GMERS, medical college and hospital, Gotri, Vadodara,
Gujarat between July 2013 to December 2013 were included in
the study.
An ethical clearance was obtained from the institutional
ethics committee.
A detailed clinical history was taken and a complete
physical examination was done in all patients. Investigations
included complete blood count including haematocrit and
platelet count, urine analysis, peripheral blood smear for
detecting malarial parasites, liver function tests, renal func-
tion tests, coagulation profile, serum electrolytes, ECG, X-ray
chest and abdominal sonography.
Diagnosis of dengue was done by detection of viral antigen
NS1 and dengue specific IgM or IgG by ELISA.
The number of indoor dengue cases during the monsoon
and post-monsoon period (June to December) in years 2011,
2012 and 2013, were compared with the total number of
admitted patients during the same period. The dengue cases
in the same years were also compared with the number of all
fever patients admitted during that time, so as to document
the absolute rise in number.
Data was entered in Microsoft Excel worksheet and then
statistical analysis was carried out by Med Calc Software
version 11.5.0.
Fig. 3 e Demographic distribution.
3. Results
As seen from Fig. 1, the age range of patients was 13e65 years.
Fifty seven patients (91%) belonged to the age group of 13e33
years, with 30 (47.6%) patients in the 13e23 years range.
As per Fig. 2, out of total 63 confirmed cases of dengue, 53
(84.1%) were males and 10 (15.9%) were females.
As per Fig. 3, forty nine patients (77.8%) belonged to the
urban area while 14 (22.2%) patients were from the rural
settings.
Please cite this article in press as: Godbole V, et al., Rising trend oVadodara e A retrospective study, Apollo Medicine (2014), http:/
As per Fig. 4, all patients presentedwith fever (100%). Other
symptoms included, myalgia in 39 (61.9%), vomiting in 31
(49.2%), abdominal pain in 20 (31.7%), nausea in 13 (20.6%) and
headache in 12 (19.1%) patients. Only 7 (11%) had backache.
Six (9.5%) patients had joint pains. Four patients had hepato-
splenomegaly.
As per Fig. 5, 60 patients (95.2%) had dengue fever while 3
(4.8%) had dengue haemorrhagic fever. No cases were recor-
ded with dengue shock syndrome.
As per Fig. 6, complications were found in 7 (11.11%) pa-
tients. They included pleural effusion, ascites and
haemorrhage.
As per the Fig. 7, the outcome is very good with early
detection and prompt treatment. 90.4% patients were treated
f cases of dengue fever admitted in a tertiary care hospital in/dx.doi.org/10.1016/j.apme.2014.10.001
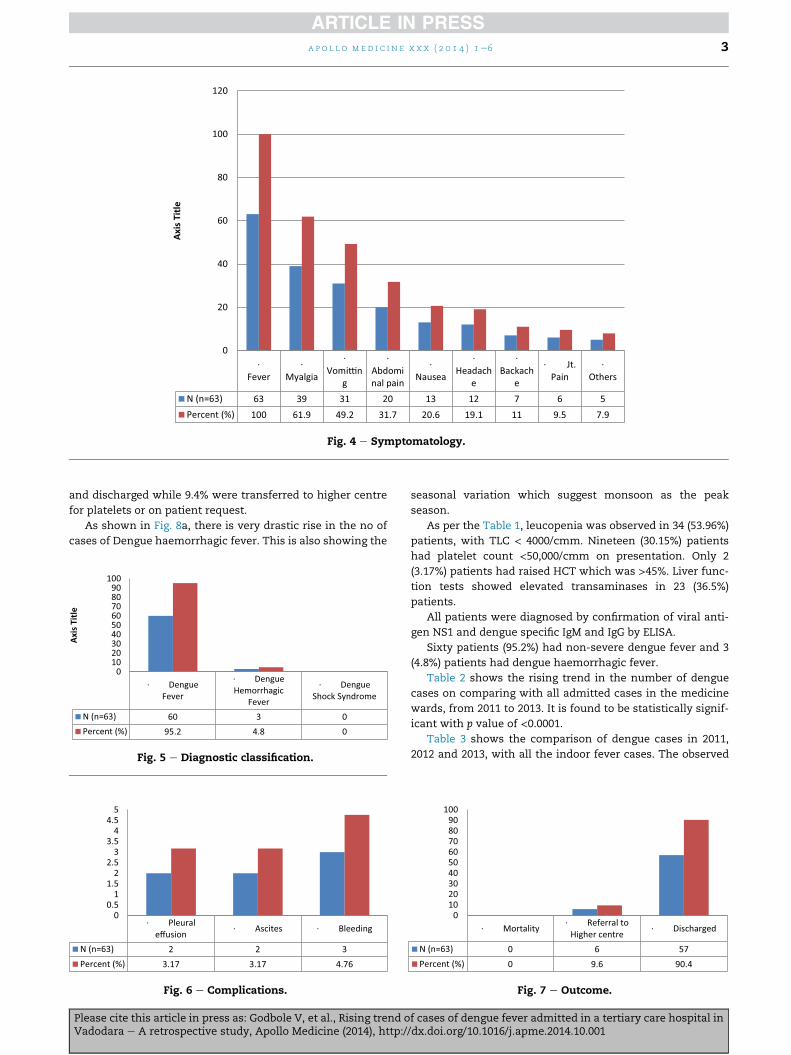
Fig. 4 e Symptomatology.
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e6 3
and discharged while 9.4% were transferred to higher centre
for platelets or on patient request.
As shown in Fig. 8a, there is very drastic rise in the no of
cases of Dengue haemorrhagic fever. This is also showing the
· DengueFever
· DengueHemorrhagic
Fever
· DengueShock Syndrome
N (n=63) 60 3 0Percent (%) 95.2 4.8 0
0102030405060708090
100
Axis
Titl
e
Fig. 5 e Diagnostic classification.
Fig. 6 e Complications.
Please cite this article in press as: Godbole V, et al., Rising trend oVadodara e A retrospective study, Apollo Medicine (2014), http:/
seasonal variation which suggest monsoon as the peak
season.
As per the Table 1, leucopenia was observed in 34 (53.96%)
patients, with TLC < 4000/cmm. Nineteen (30.15%) patients
had platelet count <50,000/cmm on presentation. Only 2
(3.17%) patients had raised HCT which was >45%. Liver func-
tion tests showed elevated transaminases in 23 (36.5%)
patients.
All patients were diagnosed by confirmation of viral anti-
gen NS1 and dengue specific IgM and IgG by ELISA.
Sixty patients (95.2%) had non-severe dengue fever and 3
(4.8%) patients had dengue haemorrhagic fever.
Table 2 shows the rising trend in the number of dengue
cases on comparing with all admitted cases in the medicine
wards, from 2011 to 2013. It is found to be statistically signif-
icant with p value of <0.0001.Table 3 shows the comparison of dengue cases in 2011,
2012 and 2013, with all the indoor fever cases. The observed
Fig. 7 e Outcome.
f cases of dengue fever admitted in a tertiary care hospital in/dx.doi.org/10.1016/j.apme.2014.10.001
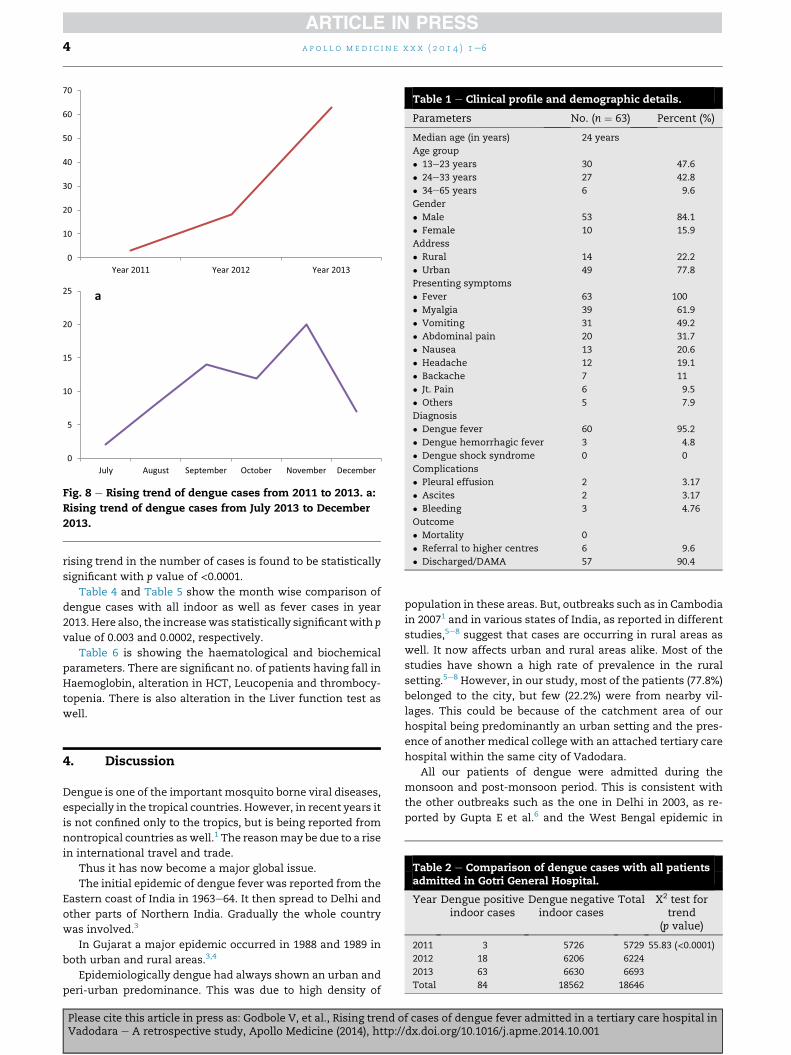
Fig. 8 e Rising trend of dengue cases from 2011 to 2013. a:
Rising trend of dengue cases from July 2013 to December
2013.
Table 1 e Clinical profile and demographic details.
Parameters No. (n ¼ 63) Percent (%)
Median age (in years) 24 years
Age group
� 13e23 years 30 47.6
� 24e33 years 27 42.8
� 34e65 years 6 9.6
Gender
� Male 53 84.1
� Female 10 15.9
Address
� Rural 14 22.2
� Urban 49 77.8
Presenting symptoms
� Fever 63 100
� Myalgia 39 61.9
� Vomiting 31 49.2
� Abdominal pain 20 31.7
� Nausea 13 20.6
� Headache 12 19.1
� Backache 7 11
� Jt. Pain 6 9.5
� Others 5 7.9
Diagnosis
� Dengue fever 60 95.2
� Dengue hemorrhagic fever 3 4.8
� Dengue shock syndrome 0 0
Complications
� Pleural effusion 2 3.17
� Ascites 2 3.17
� Bleeding 3 4.76
Outcome
� Mortality 0
� Referral to higher centres 6 9.6
� Discharged/DAMA 57 90.4
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e64
rising trend in the number of cases is found to be statistically
significant with p value of <0.0001.Table 4 and Table 5 show the month wise comparison of
dengue cases with all indoor as well as fever cases in year
2013. Here also, the increasewas statistically significantwith p
value of 0.003 and 0.0002, respectively.
Table 6 is showing the haematological and biochemical
parameters. There are significant no. of patients having fall in
Haemoglobin, alteration in HCT, Leucopenia and thrombocy-
topenia. There is also alteration in the Liver function test as
well.
Table 2 e Comparison of dengue cases with all patientsadmitted in Gotri General Hospital.
Year Dengue positiveindoor cases
Dengue negativeindoor cases
Total X2 test fortrend
(p value)
2011 3 5726 5729 55.83 (<0.0001)2012 18 6206 6224
2013 63 6630 6693
Total 84 18562 18646
4. Discussion
Dengue is one of the important mosquito borne viral diseases,
especially in the tropical countries. However, in recent years it
is not confined only to the tropics, but is being reported from
nontropical countries aswell.1 The reasonmay be due to a rise
in international travel and trade.
Thus it has now become a major global issue.
The initial epidemic of dengue fever was reported from the
Eastern coast of India in 1963e64. It then spread to Delhi and
other parts of Northern India. Gradually the whole country
was involved.3
In Gujarat a major epidemic occurred in 1988 and 1989 in
both urban and rural areas.3,4
Epidemiologically dengue had always shown an urban and
peri-urban predominance. This was due to high density of
Please cite this article in press as: Godbole V, et al., Rising trend oVadodara e A retrospective study, Apollo Medicine (2014), http:/
population in these areas. But, outbreaks such as in Cambodia
in 20071 and in various states of India, as reported in different
studies,5e8 suggest that cases are occurring in rural areas as
well. It now affects urban and rural areas alike. Most of the
studies have shown a high rate of prevalence in the rural
setting.5e8 However, in our study, most of the patients (77.8%)
belonged to the city, but few (22.2%) were from nearby vil-
lages. This could be because of the catchment area of our
hospital being predominantly an urban setting and the pres-
ence of another medical college with an attached tertiary care
hospital within the same city of Vadodara.
All our patients of dengue were admitted during the
monsoon and post-monsoon period. This is consistent with
the other outbreaks such as the one in Delhi in 2003, as re-
ported by Gupta E et al.6 and the West Bengal epidemic in
f cases of dengue fever admitted in a tertiary care hospital in/dx.doi.org/10.1016/j.apme.2014.10.001
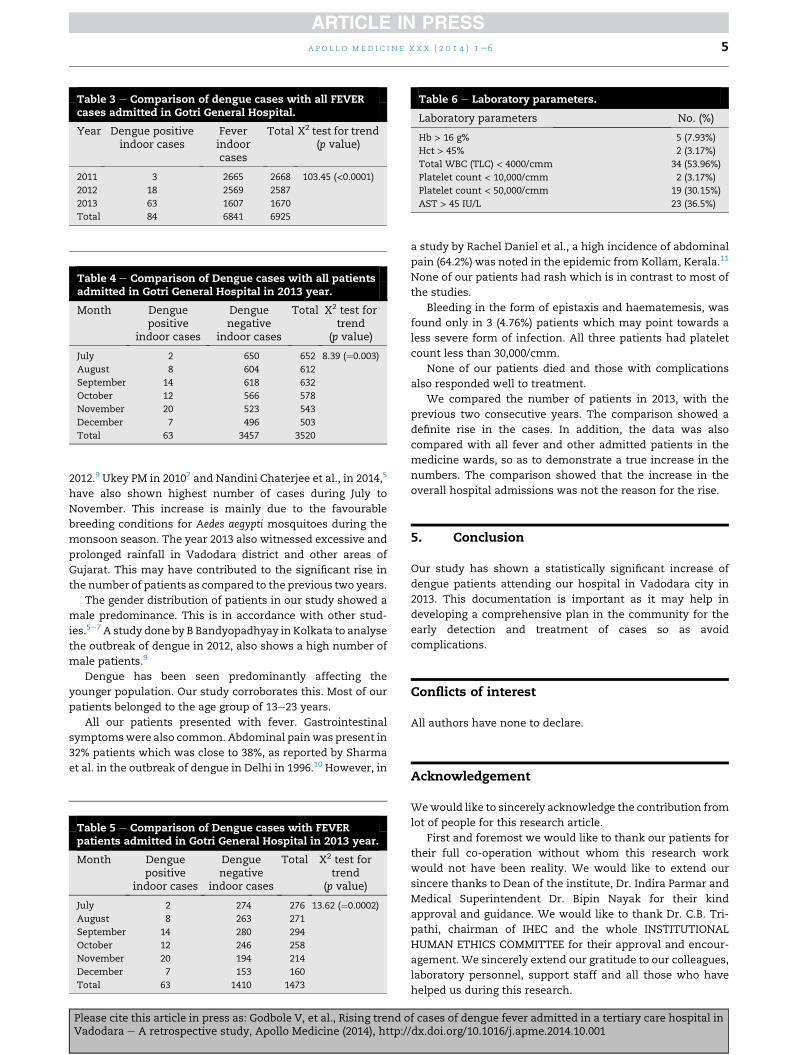
Table 3 e Comparison of dengue cases with all FEVERcases admitted in Gotri General Hospital.
Year Dengue positiveindoor cases
Feverindoorcases
Total X2 test for trend(p value)
2011 3 2665 2668 103.45 (<0.0001)2012 18 2569 2587
2013 63 1607 1670
Total 84 6841 6925
Table 4 e Comparison of Dengue cases with all patientsadmitted in Gotri General Hospital in 2013 year.
Month Denguepositive
indoor cases
Denguenegative
indoor cases
Total X2 test fortrend
(p value)
July 2 650 652 8.39 (¼0.003)
August 8 604 612
September 14 618 632
October 12 566 578
November 20 523 543
December 7 496 503
Total 63 3457 3520
Table 6 e Laboratory parameters.
Laboratory parameters No. (%)
Hb > 16 g% 5 (7.93%)
Hct > 45% 2 (3.17%)
Total WBC (TLC) < 4000/cmm 34 (53.96%)
Platelet count < 10,000/cmm 2 (3.17%)
Platelet count < 50,000/cmm 19 (30.15%)
AST > 45 IU/L 23 (36.5%)
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e6 5
2012.9 Ukey PM in 20107 and Nandini Chaterjee et al., in 2014,5
have also shown highest number of cases during July to
November. This increase is mainly due to the favourable
breeding conditions for Aedes aegypti mosquitoes during the
monsoon season. The year 2013 also witnessed excessive and
prolonged rainfall in Vadodara district and other areas of
Gujarat. This may have contributed to the significant rise in
the number of patients as compared to the previous two years.
The gender distribution of patients in our study showed a
male predominance. This is in accordance with other stud-
ies.5e7 A study done by B Bandyopadhyay in Kolkata to analyse
the outbreak of dengue in 2012, also shows a high number of
male patients.9
Dengue has been seen predominantly affecting the
younger population. Our study corroborates this. Most of our
patients belonged to the age group of 13e23 years.
All our patients presented with fever. Gastrointestinal
symptomswere also common. Abdominal painwas present in
32% patients which was close to 38%, as reported by Sharma
et al. in the outbreak of dengue in Delhi in 1996.10 However, in
Table 5 e Comparison of Dengue cases with FEVERpatients admitted in Gotri General Hospital in 2013 year.
Month Denguepositive
indoor cases
Denguenegative
indoor cases
Total X2 test fortrend
(p value)
July 2 274 276 13.62 (¼0.0002)
August 8 263 271
September 14 280 294
October 12 246 258
November 20 194 214
December 7 153 160
Total 63 1410 1473
Please cite this article in press as: Godbole V, et al., Rising trend oVadodara e A retrospective study, Apollo Medicine (2014), http:/
a study by Rachel Daniel et al., a high incidence of abdominal
pain (64.2%) was noted in the epidemic from Kollam, Kerala.11
None of our patients had rash which is in contrast to most of
the studies.
Bleeding in the form of epistaxis and haematemesis, was
found only in 3 (4.76%) patients which may point towards a
less severe form of infection. All three patients had platelet
count less than 30,000/cmm.
None of our patients died and those with complications
also responded well to treatment.
We compared the number of patients in 2013, with the
previous two consecutive years. The comparison showed a
definite rise in the cases. In addition, the data was also
compared with all fever and other admitted patients in the
medicine wards, so as to demonstrate a true increase in the
numbers. The comparison showed that the increase in the
overall hospital admissions was not the reason for the rise.
5. Conclusion
Our study has shown a statistically significant increase of
dengue patients attending our hospital in Vadodara city in
2013. This documentation is important as it may help in
developing a comprehensive plan in the community for the
early detection and treatment of cases so as avoid
complications.
Conflicts of interest
All authors have none to declare.
Acknowledgement
Wewould like to sincerely acknowledge the contribution from
lot of people for this research article.
First and foremost we would like to thank our patients for
their full co-operation without whom this research work
would not have been reality. We would like to extend our
sincere thanks to Dean of the institute, Dr. Indira Parmar and
Medical Superintendent Dr. Bipin Nayak for their kind
approval and guidance. We would like to thank Dr. C.B. Tri-
pathi, chairman of IHEC and the whole INSTITUTIONAL
HUMAN ETHICS COMMITTEE for their approval and encour-
agement. We sincerely extend our gratitude to our colleagues,
laboratory personnel, support staff and all those who have
helped us during this research.
f cases of dengue fever admitted in a tertiary care hospital in/dx.doi.org/10.1016/j.apme.2014.10.001

a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e66
r e f e r e n c e s
1. WHO. Guidelines for Diagnosis, Treatment, Prevention and Control.New Edition. 2009.
2. Dash AP, Bhatia R, Kalra NL. Dengue in South-East Asia: anappraisal of case management and vector control. DengueBull. Dec 2012;36.
3. Gupta Nivedita, Shrivastav Sakshi, Jain Amita. Dengue inIndia. Centenary review article. Indian J Med Res. Sept2012;136:373e390.
4. Mahadev PV, Kollali VV, Rawal ML, et al. Dengue in GujaratState, India during 1988 &1989. Indian J Med Res.1993;97:135e144.
5. Chaterjee Nandini, Mukhopadhyay Mainak, Ghosh Sinjon. Anobservational study of denguefever in a tertiary care hospitalof eastern India. JAPI. March 2014;62:224e227.
Please cite this article in press as: Godbole V, et al., Rising trend oVadodara e A retrospective study, Apollo Medicine (2014), http:/
6. Gupta E, Dar L, Narang P. Indian J Med Res. 2005 Jan;121:36e38.7. Ukey PM, Bondade SA, Akulwar SL. Study of seroprevalence of
dengue fever in central India. Indian J Community Med. 2010OcteDec;35:517e519.
8. Mehandale SM, Risbud AR, Rao JA. Outbreak of dengue feverin rural areas of Parbhani district of Maharashtra (India).Indian J Med Res. 1991 Jan;93:6e11.
9. Bandyopadhyay Bhaswati, Bhattacharyya Indrani,Adhikary Srima. A comprehensive study on the 2012 denguefever outbreak in Kolkata, India. ISRN Virol. 2013;2013. ArticleID 207580.
10. Sharma S, Sharma SK. Clinical profile of DHF in adults during1996 out break in Delhi, India. Dengue Bull. 1998;22:20e27.
11. Daniel Rachel, Mohanan Raja. A study of clinical profile ofdengue fever in Kollam, Kerala, India. Dengue Bull.2005;29:197e202.
f cases of dengue fever admitted in a tertiary care hospital in/dx.doi.org/10.1016/j.apme.2014.10.001

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/











![Dengue Fever/Severe Dengue Fever/Chikungunya Fever · Dengue fever and severe dengue (dengue hemorrhagic fever [DHF] and dengue shock syndrome [DSS]) are caused by any of four closely](https://img.pdfslide.us/doc/110x75/5e87bf3e7a86e85d3b149cd7/dengue-feversevere-dengue-feverchikungunya-dengue-fever-and-severe-dengue-dengue.jpg)