Embed Size (px)
Citation preview

Results Of Mini-Open LatarjetProcedure In Failed Arthroscopic
Bankart repair
– A Retrospective analysis
Dr Rahul Kumar
Sports Injury centre, Safdarjung Hospital

DISCLOSURE
The authors have no financial conflicts to disclose

INTRODUCTION
Anterior shoulder instability is most common type of shoulder instability.
Arthroscopic bankart repair has become the procedure of choice of primary recurrent anterior shoulder instability
However, failures of stabilization can and do occur.

INTRODUCTION
Recurrent instability after Bankartrepair is a difficult problem for boththe patient and treating physician.
• Open procedure: 10%
• Arthroscopic procedure: 0-43%.
Recurrence rates
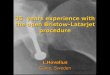
• Re-Dislocation
- no bone loss 4% recurrence
- inverted pear 61% recurrence
(>25% Glenoid Bone loss)
Burkhart SS, De Beer JF. Traumatic Glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the
humeralengaging Hill-Sachs lesion. Arthroscopy 2000;16:677-694.)
CAUSES OF FAILURES
GLENOID BONE LOSS

Humeral head bone defectsEngaging Hill sach’s lesion

Glenoid Tracking
Yamamoto at al. JSES 2007mapped track of glenoid onhumeral head throughsimulated motion started inmax ER Varied Abductionfrom 0 degree to 60 degree.

Humeral head defect -outside the glenoidtrack - high risk forengaging (OUT-E).
Humeral head defect– inside the track –Non engaging ( IN-NE)

Latarjet M. Traitement de la luxation récidivante de l’épaule. Treatment of recurrent dislocation of the shoulder. Lyon Chirurgical. 1954; 49:994–997.
Developed and reported in 1954 usingStandard delto-pectoral approach
Transfers a large segment of the coracoid (2.5to 3 cm in length) as bone graft to the anteriorinferior glenoid rim.
ORIGINAL LATARJET

Mini open Latarjet
Limited delto-pectoral approach
Skin incision: 1 cm above the tipof the coracoid extending 4-5 cmtoward the axillary fold.
Slightly medial to coracoid, sothat anterior inferior glenoidneck is exposed easily.

Materials and MethodsStudy design: Retrospective study
Sample size : 24
Study period: June 2010 – May 2012
Inclusion criteria: Patients who had undergone arthroscopic Bankart repair for recurrent anterior shoulder instability who presented with persistent instability after surgery with positive apprehension test.
Exclusion Criteria: Primary latarjet procedures were excluded from the study.

Pre-op workup
Clinical and radiological evaluation done.
• Size of Hill sach’slesion
• Glenoid Bone Loss
3D CT was performed

Surgical Technique

Surgical Technique
Post op Rehabilitation
Shoulder immobiliser upto 2 weeks
Shoulder pendulum exercises are started fromday 1.
Passive abduction & forward elevation upto 900
and External rotation upto 300 is initiated from3rd week after suture removal.

Follow Up
Minimum Follow up: 2 years
Radiographic assessment
• AP view
• scapular Y view
Functional results
• American shoulder and elbow score(ASES)
• Western Ontario shoulder instability score(WOSI).
Range of motion
• Loss of mean forward elevation
• Loss of external rotation
Follow Up
Data Analysis
•Range
•Mean
•Student’s T-test with statistical significance set at p value < .05

RESULTS
All patients were Male.
Mean age of patients was 31.8 years (range: 21-37years).
The right shoulder was involved in 13 cases (54.17 %),and the dominant arm was affected in 11 patients(45.83 %).
Average glenoid bone loss was 21% as assessed bythree dimensional computed tomography (range ; 15-29%).

CAUSE OF FAILURE
GLENOID BONE LOSS
HUMERAL HEAD DEFECT
TRAUMATIC
7
8 9

RESULTSRANGE OF MOTION
0
20
40
60
80
100
120
140
160
180
mean forwardelevation
mean externalrotation
preop
postop
Loss of 3.1 degree
Loss of 6.4 degree
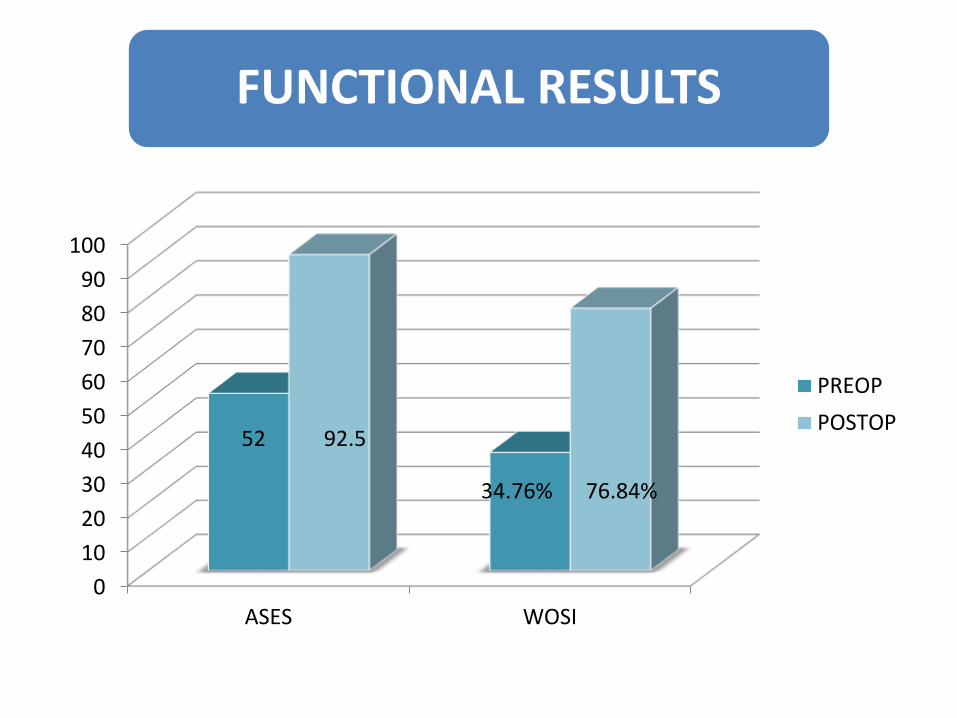
FUNCTIONAL RESULTS
0
10
20
30
40
50
60
70
80
90
100
ASES WOSI
PREOP
POSTOP92.5
76.84%
52
34.76%

COMPLICATIONS
Shoulder pain was found in 6 patients (32%) (4with mild pain and 2 with moderate pain)
One patient had hardware complication in terms ofscrew backing out from the plate. The implant wasremoved after 15 months of surgery.
One patient had superficial wound infection whichresponded to irrigation and oral antibiotics.

LITERATURE REVIEW POST OP ROM
Our study
• Flexion: 164.8 degree + 2.0 degree
• External rotation: 45.6 degree + 3.0 degree
Burkhart and De beer
• Flexion:179.6±2.0°
• external rotation: 50.2±12.6°
Allain et al
• Abduction: 42±17°
• external rotation: 48±18°
Allain J, Goutallier D, Glorion C. Long-term results of the latarjet procedure for the treatment of anterior instability of the shoulder. Journal of Bone and Joint Surgery A. 1998; 80(6):841–852.
Burkhart S, De Beer J, Barth J, et al. Results of modified Latarjet reconstruction in patients with anteroinferior instability and significant bone loss. . Arthroscopy.2007; 23(10):1033–1041. doi:
10.1016/j.arthro.2007.08.009.

LITERATURE REVIEW Redislocation & Subluxation
0
1
2
3
4
5
6
7
8
9
10
Our study Hill et al Allain et al Hovelius et al
Redislocation
Subluxation
26 mths 58 mths 14.3 yrs 15 yrs

Johanna Schulze-Borges, Dr.Eng: Arthroscopy: Vol 29, No 4 (April), 2013: pp 630-637 Biomechanical Comparison of Open and Arthroscopic Latarjet Procedures:
There is superior stabilization effect of theopen Latarjet technique in the ABDposition(Abduction with neutral rotation)- anterior capsular repair
In the ABER position, no difference
Literature review Arthroscopic vs open Latarjet

LIMITATIONS
Small sample size
Short follow up – effect of bone grafton gleno-humeral degenerativearthritis could not be assessed.

CONCLUSION
The mini-open Latarjet procedure provides satisfactoryoutcome and stabilization in this extremely challengingcategory of patients who present with dramatic boneloss and failed soft tissue reconstruction.
We recommend this procedure for young activepatients with recurrent anterior inferior shoulderinstability even after Arthroscopic Bankart repair.

CASE 1: 21yrs/Male Preop Radiographs and CT

Post op Radiographs
AP view Scapular Y view Scapular Y view at 6 months