Embed Size (px)
Citation preview

Respiratory Failureand Role of ABGs in ICU
(Presenter: Dr Hasheela T. U. N)

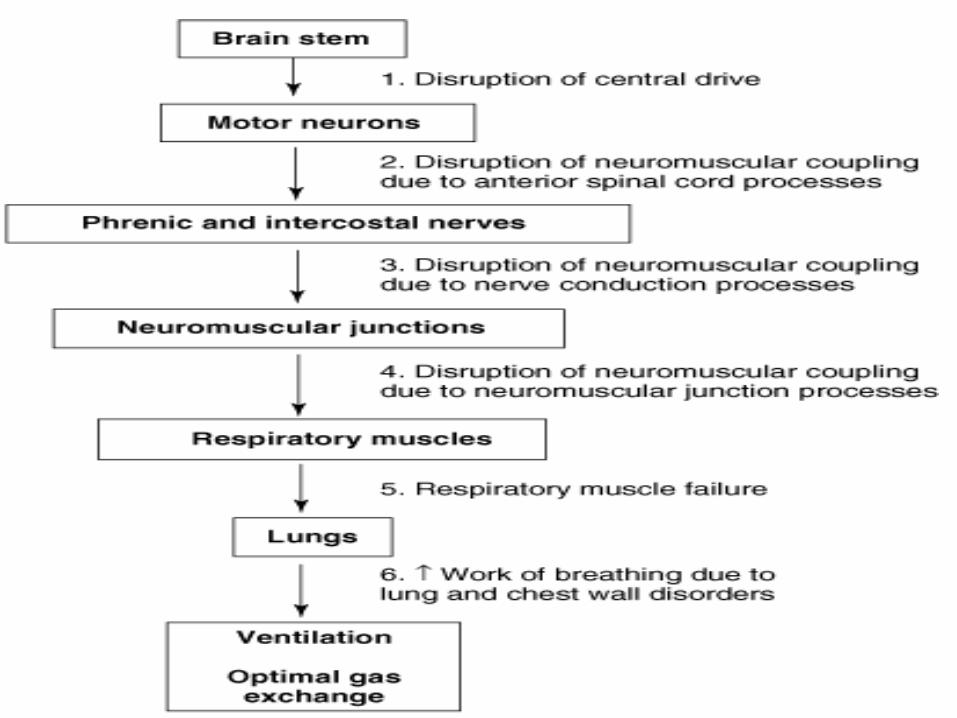
Components of the respiratory system
Gas-exchange (Interface)organ• Lungs (parenchyma)
• Blood vessels (pulmonary and
bronchial)
Ventilatory pump• Thoracic wall• Respiratory muscles• Brainstem and cortex• Anterior horn cells (S.C.)• Phrenic nerves and other
nerves

Definition
:- a syndrome in which the respiratory system fails in one or both of its gas exchange functions i.e. oxygenation and/or carbon dioxide elimination, such that the levels of arterial oxygen (PaO₂) and carbon dioxide (PaCO₂) partial pressures cannot be maintained within their normal ranges.
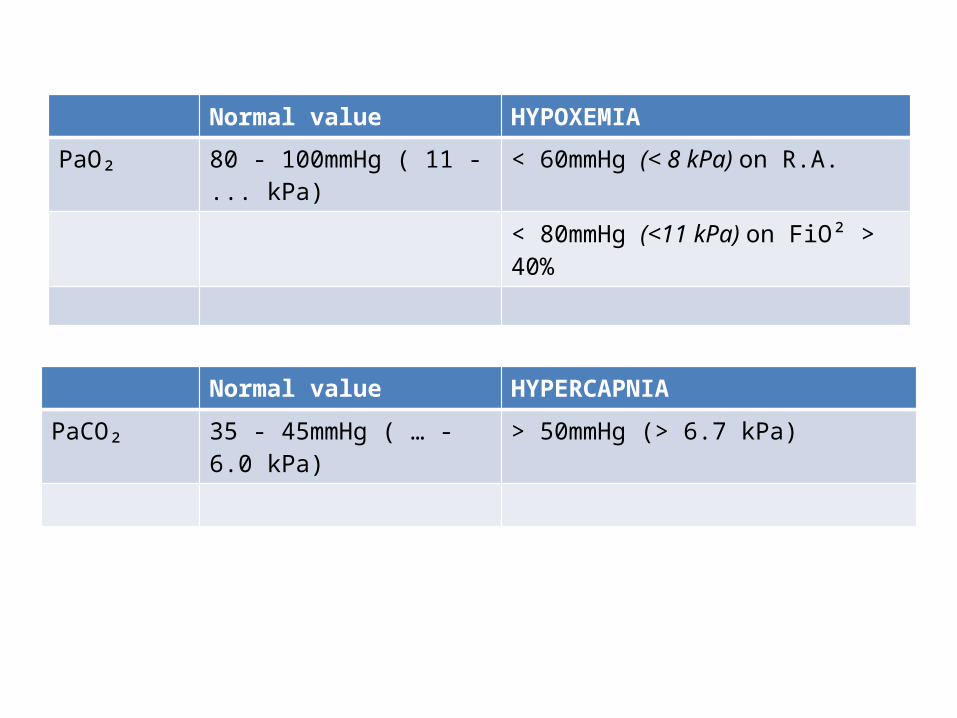
Normal value HYPOXEMIA
PaO₂ 80 - 100mmHg ( 11 - ... kPa) < 60mmHg (< 8 kPa) on R.A.
< 80mmHg (<11 kPa) on FiO² > 40%
Normal value HYPERCAPNIA
PaCO₂ 35 - 45mmHg ( … - 6.0 kPa) > 50mmHg (> 6.7 kPa)
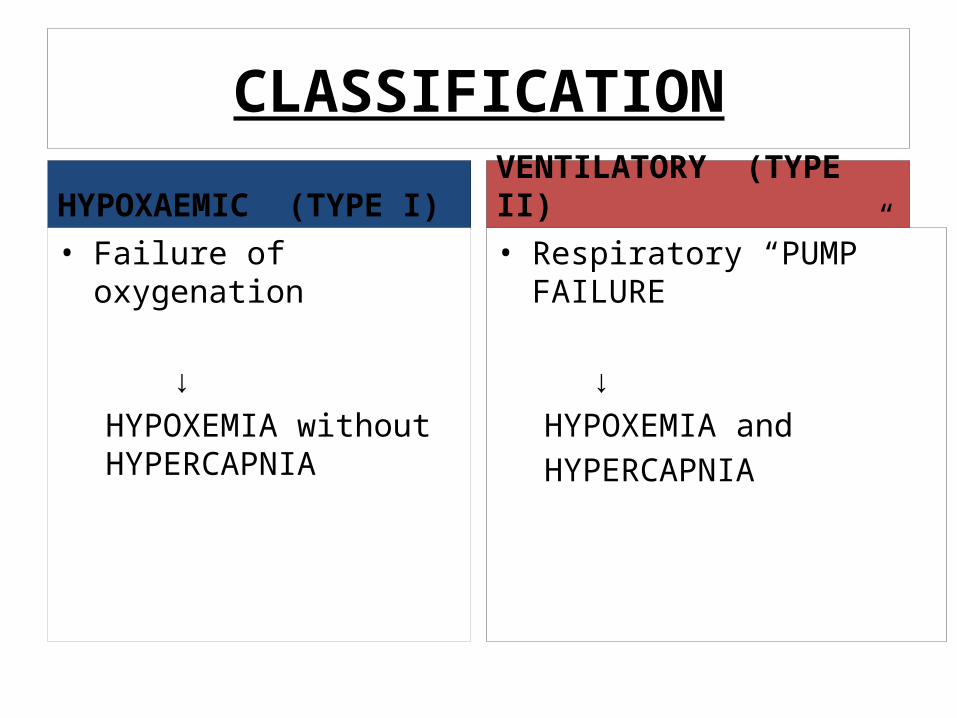
CLASSIFICATION
HYPOXAEMIC (TYPE I)• Failure of oxygenation
↓
HYPOXEMIA without HYPERCAPNIA
VENTILATORY (TYPE II)• Respiratory “PUMP” FAILURE
↓HYPOXEMIA and HYPERCAPNIA
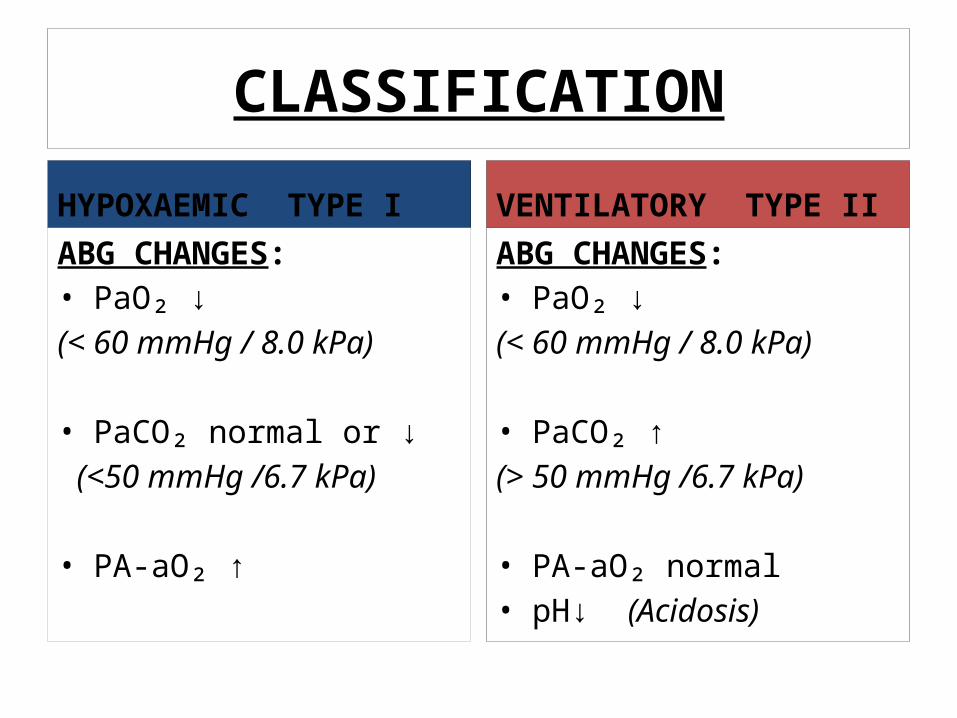
CLASSIFICATION
HYPOXAEMIC TYPE IABG CHANGES:• PaO₂ ↓(< 60 mmHg / 8.0 kPa)
• PaCO₂ normal or ↓ (<50 mmHg /6.7 kPa)
• PA-aO₂ ↑
VENTILATORY TYPE IIABG CHANGES:• PaO₂ ↓(< 60 mmHg / 8.0 kPa)
• PaCO₂ ↑(> 50 mmHg /6.7 kPa)
• PA-aO₂ normal• pH↓ (Acidosis)

Causes
Hypoxaemic (Type I) • Pneumonia• ARDS• Pulmonary fibrosis• Asthma• COPD• Pnemothorax• PE• Obesity• Pulmonary Hypertension
Hypercapnic (Type II)• COPD / Severe Asthma• Drug Overdose (Opiates
benzodiazepines,)• CNS Injury (SCI, CVA)• Primary muscle disorders
(Duchenne muscular dystrophy)• Neuromuscular junction disorders
(eg. Myasthenia gravis)• Anatomical chest deformities (eg. Kyphoscoliosis, Flail chest)• Obesity Hypo-ventilatory
(Pickwickian) syndrome
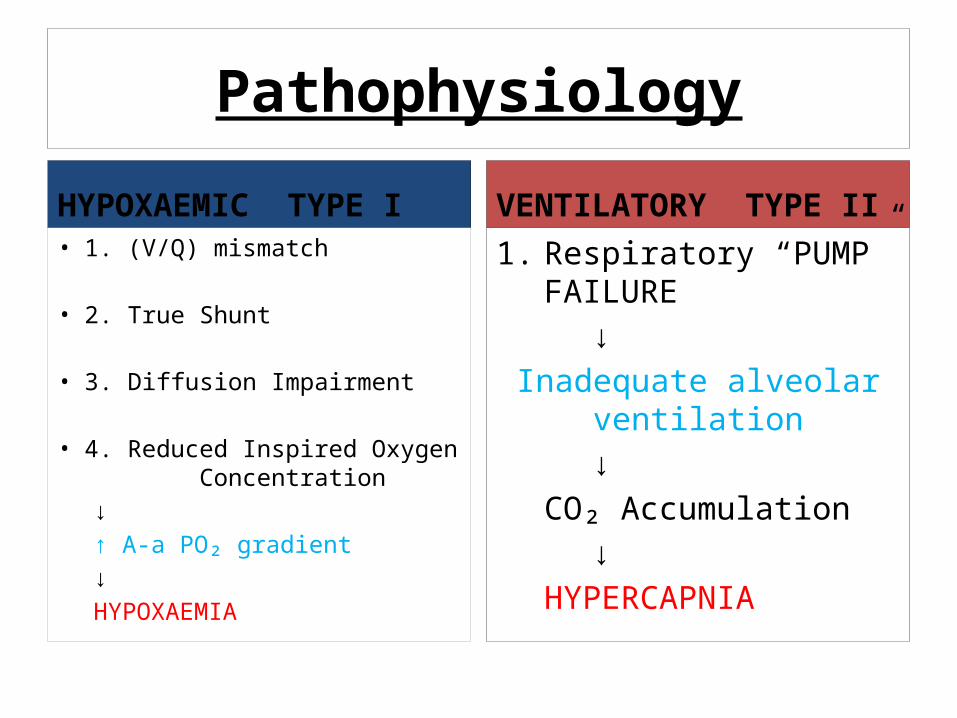
Pathophysiology
HYPOXAEMIC TYPE I• 1. (V/Q) mismatch
• 2. True Shunt
• 3. Diffusion Impairment
• 4. Reduced Inspired Oxygen Concentration
↓↑ A-a PO₂ gradient
↓HYPOXAEMIA
VENTILATORY TYPE II1. Respiratory “PUMP”
FAILURE↓
Inadequate alveolar ventilation↓
CO₂ Accumulation↓
HYPERCAPNIA
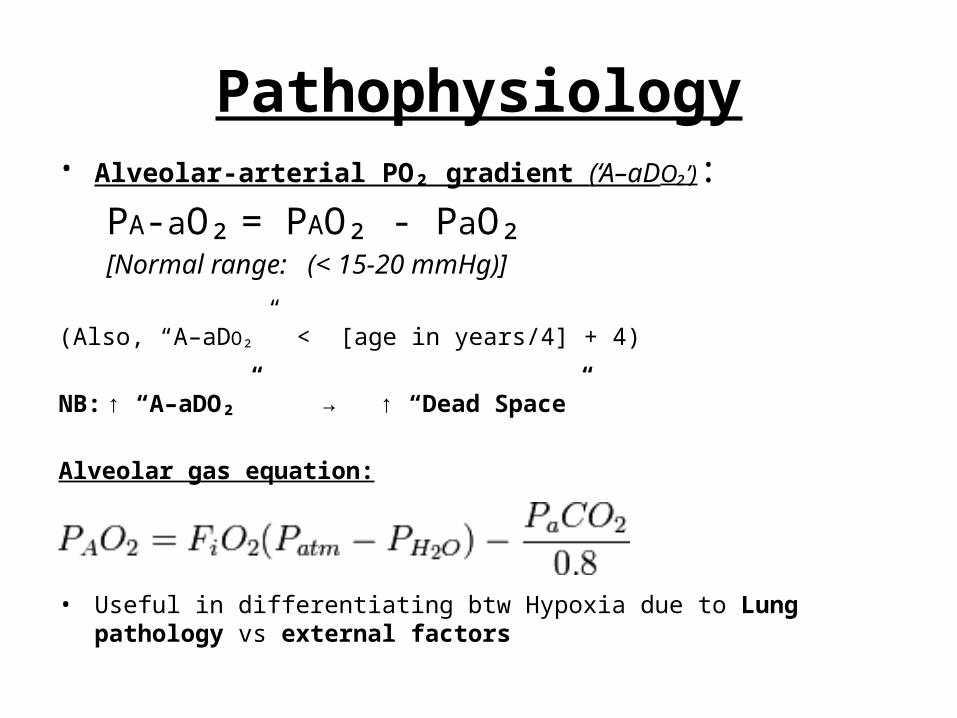
Pathophysiology• Alveolar-arterial PO₂ gradient (‘A–aDO₂’):
PA-aO₂ = PAO₂ - PaO₂[Normal range: (< 15-20 mmHg)]
(Also, “A–aDO₂” < [age in years/4] + 4)
NB: ↑ “A–aDO₂” → ↑ “Dead Space”
Alveolar gas equation:
• Useful in differentiating btw Hypoxia due to Lung pathology vs external factors
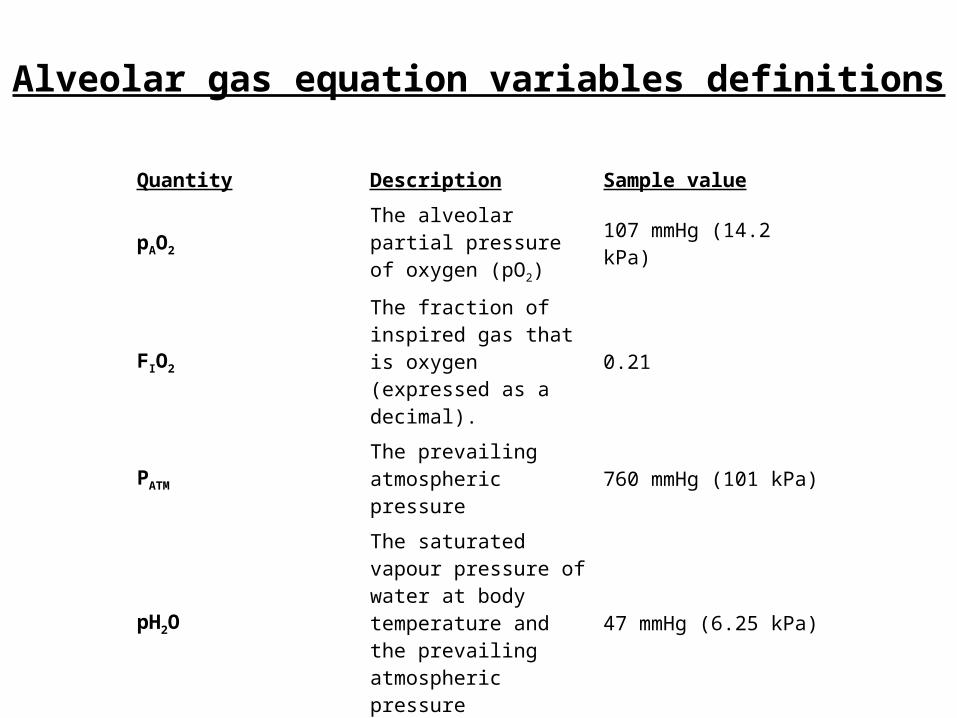
Alveolar gas equation variables definitions
Quantity Description Sample value
pAO2The alveolar partial pressure of oxygen (pO2)
107 mmHg (14.2 kPa)
FIO2
The fraction of inspired gas that is oxygen (expressed as a decimal).
0.21
PATMThe prevailing atmospheric pressure 760 mmHg (101 kPa)
pH2O
The saturated vapour pressure of water at body temperature and the prevailing atmospheric pressure
47 mmHg (6.25 kPa)
paCO2
The arterial partial pressure of carbon dioxide (pCO2)
40 mmHg (4.79 kPa)
RER The respiratory exchange ratio 0.8

CLINICAL PRESENTATIONRF may be preceded by signs of respiratory distress:
• Tachypnoea (>25/min)• Breathlessness• Gasping or pursed lip
breathing• Tight chest • Sweating, clamminess• Agitation• Sitting or hunched
posture
• Sense of impending doom
• Inability to complete a sentences
• Cyanosis• HYPOXAEMIA Sats<92%• HYPERCAPNEA
Pre-terminal Signs
• Bradycardia, dysrhythmias, hypotension• Bradypnoea or silent chest• Decreased L.O.C
DIAGNOSTICS
1) VITAL SIGNS AND INSPECTION(BP, O₂ Sat, RR, T°C, LOC, airway patency)
• Fever, tachycardia, tachypnea → Infection• Fever, lethargy → CNS infection /septic encephalopathy• ↑Pulsus paradoxus (>10 mmHg) → Asthma or COPD• Ethanol odour → Intoxication
DIAGNOSTICS
2) NEUROLOGICAL EXAMINATION
• Depressed mental status (lethargy or coma) → Central drive failure• Pupillary constriction (miosis) “pinpoint pupils” → Opiate overdose(Severe hypercarbia causes miosis as well)• Sensory deficits → Polyneuropathy (e.g. GBS)• Muscle fasciculations → Motor neuron diseases (e.g. ALS)

DIAGNOSTICS3) Head and Neck
• Stridor, drooling → upper airway obstruction
4) Chest• Pattern of respiratory muscle contraction, chest diameter and
intergrity (Flail chest), presence of abnormal breath sounds
5) Abdomen• Normal abdominal wall movement during inspiration is
outward, inward movement with inspiration is paradoxical and suggests diaphragmatic fatigue.
DIAGNOSTICSLaboratory Testing
1. Arterial Blood Gas (ABG)ABGs are required very early and should be obtained as soon as possible after C-A-B has been assessed.

DIAGNOSTICS
Normal values of arterial blood gases (at R.A., sea level, 37°C)
DIAGNOSTICSInterpretative remarks:
• PaO₂ < 60mmHg(8kPa) →HYPOXEMIA• PaCO₂ > 50 mmHg(6.7 kPa) →HYPERCAPNIA
• pH < 7.35 → ACIDOSIS• pH >7.45 → ALKALOSIS
DIAGNOSTICSInterpretative remarks:
• ↓PaO₂ → TYPE I (Hypoxemic) RF
• ↑PaCO₂, ↓pH →Acute TYPE II (Hypercapnic) RF
• ↑PaCO₂, slightly↓pH, ↑HCO₃⁻ → Chronic TYPE II (Hypercapnic) RF
DIAGNOSTICSInterpretative remarks:
• The "50–50 rule" of intubating is OUTDATED!• Respiratory acidosis (pH<7.20–7.25) is an indication
ventilatory support.• Interpretation of an inadvertent venous blood
gas (VBG) must be avoided.• Elevated HCO⁻₃ is evidence of chronic
respiratory acidosis.

DIAGNOSTICS
2. Complete Blood Count (CBC)• Leukocytosis → infection• Anemia (dyspnea,↓O₂ transport to tissues, but in isolation
will not cause ventilatory failure.
3. Lumbar Puncture (LP) • (essential in cases of suspected CNS infection or GBS)
4. Serum Chemistries• (↓Ca,Mg,PO⁻ may contribute to respiratory muscle fatigue)
5. Toxicology Tests6. Pulmonary Function Tests
DIAGNOSTICSImaging and Other Tests
• CXR • (Pneumonia, atelectasis, pulmonary oedema, evidence of chronic
lung disease, tumours, chest wall and pleural abnormalities)
• CT Scan • (tumours, parenchymal lung disease, pleural and chest wall
disease)
• MRI• (encephalitis, brain stem pathology, and spinal cord injury)
• ECG• (evidence of chronic lung disease, left ventricular failure or valve
disease)
Principles of treatment
• Emergency treatment should follow principles of cardiopulmonary resuscitation (C-A-B);
• Ensure patent airway• Administer oxygen to maintain sats >90%• Correct hypoperfusion/anaemia
followed by treatment of underlying (reversible) causes:• Acidosis/Alkalosis• Hypovolemia• Hypoxia• Pneumothorax• Pulmonary embolism
Principles of treatment (Cont…)
• All patients with acute VF not responding to simple measures in an emergency room, clinic, or hospital ward setting should be monitored in an intensive/intermediate care unit.
• Inhaled bronchodilators should be administered to all patients with bronchospasm.
• Fever reduction with acetaminophen will decrease CO₂ production.
• Avoid excessive caloric intake (which increases CO₂ production)
Principles of treatment (Cont…)
• Consider non-invasive ventilatory support:• CPAP: continous positive airway pressure• BiPAP: Biphasic positive airway pressure
• Evaluate patient for the need of Endotracheal intubation and mechanical ventilation (e.g. in cases of severe respiratory failure with PaO2 less than 50 mmHg).
Principles of treatment (Cont…)
• DRUGS:• Respiratory stimulants (eg. Doxapram) (rarely used)
• Antidote for sedative overdose» Opioids → naloxone» Benzodiazepines → flumazenil
• Physiotherapy to mobilise secretions.

***************The End***************
THANK YOU!!!
References1. Hanley M. E., Welsh. H., Current Diagnosis & Treatment in Pulmonary
Medicine,1st ed. Denver, Colorado, September 2003.2. Kim E. Barrett, Susan M. Barman, Scott Boitano, and Heddwen L. Brooks,
Ganong's Review of Medical Physiology, 24th ed., Singapore,2012. 3. BMJ Publishing Group Limited, BMJ Best Practice, 2015
http://bestpractice.bmj.com (accessed 13-04-2015).