Embed Size (px)
Citation preview

Acute Respiratory Acute Respiratory Obstruction and Obstruction and
RestrictionRestriction
ICU nurses course 2004ICU nurses course 2004Tim SmithTim Smith

TopicsTopics
Asthma (acute bronchospasm)Asthma (acute bronchospasm)
Acute Exacerbation of COPDAcute Exacerbation of COPD
PneumothoraxPneumothorax
Pleural EffusionPleural Effusion

Acute AsthmaAcute Asthma

AsthmaAsthma
Chronic inflammatory condition of the Chronic inflammatory condition of the lung airways characterised by:lung airways characterised by:
• Reversible airflow limitationReversible airflow limitation
• Airway hyperresponsivenessAirway hyperresponsiveness
• Bronchial inflammationBronchial inflammation
Increasing prevalenceIncreasing prevalence10-15% of pop. In 210-15% of pop. In 2ndnd decade decade

PathogenesisPathogenesis
Extrinsic vs. Intrinsic Extrinsic vs. Intrinsic
Mast cells (histamine, LTCMast cells (histamine, LTC44, PGD, PGD22))
T cells (cytokines)T cells (cytokines) Eosinophils (ECP, MBP)Eosinophils (ECP, MBP) C-fibres (NKA, CGRP, SubP)C-fibres (NKA, CGRP, SubP)

Precipitating FactorsPrecipitating Factors AllergensAllergens
•FlourFlour•Washing powderWashing powder•AnimalsAnimals
Non-specificNon-specific•ExerciseExercise•Cold airCold air•EmotionEmotion
OccupationalOccupational•IsocyanatesIsocyanates•Colophony fumesColophony fumes

MechanismsMechanisms
BronchoconstrictionBronchoconstriction Airway inflammationAirway inflammation
• Microvascular leakMicrovascular leak• OedemaOedema
Increased (viscid) mucus productionIncreased (viscid) mucus production
AIRWAY OBSTRUCTIONAIRWAY OBSTRUCTION

Physiological EffectsPhysiological Effects
Increased work of breathingIncreased work of breathing• Accessory muscle useAccessory muscle use• Increased oxygen demandsIncreased oxygen demands
Air trappingAir trapping• Prolonged active expiratory phaseProlonged active expiratory phase• Auto-PEEPAuto-PEEP
V/Q mismatchV/Q mismatch• HypoxiaHypoxia
Increased respiratory driveIncreased respiratory drive

Clinical FeaturesClinical Features 11
Related to severity:Related to severity:
Moderate asthma exacerbationModerate asthma exacerbation• BreathlessnessBreathlessness• Wheeze (expiratory)Wheeze (expiratory)• PEF 50-75%PEF 50-75%

Clinical FeaturesClinical Features 22
Acute Severe AsthmaAcute Severe Asthma
One of:One of:
• PEF 33-50%PEF 33-50%
• RR >= 25 /minRR >= 25 /min
• HR >= 110/minHR >= 110/min
• Inability to complete sentencesInability to complete sentences

Clinical FeaturesClinical Features 33
One of:One of:• PEF <33%PEF <33%
• SpOSpO2 2 <92%<92%
• PPaaOO22 <8kPa <8kPa
• Normal PNormal PaaCOCO22
• Silent chestSilent chest• CyanosisCyanosis• Feeble respiratory effortFeeble respiratory effort
• BradycardiaBradycardia• DysrhythmiaDysrhythmia• HypotensionHypotension• ExhaustionExhaustion• ConfusionConfusion• ComaComa
Life threatening Life threatening AsthmaAsthma

Clinical FeaturesClinical Features 44
Near Fatal AsthmaNear Fatal Asthma
One of:One of:
• High PHigh PaaCOCO22
• Mechanical ventilationMechanical ventilation

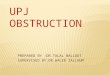
Chest X RayChest X Ray
HyperinflationHyperinflation Flattened Flattened
diaphragmdiaphragm

Chest X Ray 2Chest X Ray 2

CT ScanCT Scan

MRI with HeMRI with He33
Before 40 min after Albuterol

Medical TherapyMedical Therapy
OxygenOxygen ββ22-agonists-agonists
• Nebulised if possibleNebulised if possible SteroidsSteroids Ipratropium BromideIpratropium Bromide Magnesium SulphateMagnesium Sulphate
• Life threatening or poor responseLife threatening or poor response AminophyllineAminophylline
• Perhaps in some patientsPerhaps in some patients

Indications for ITUIndications for ITU
Deteriorating PEFDeteriorating PEF Worsening hypoxiaWorsening hypoxia HypercapniaHypercapnia Worsening acidosisWorsening acidosis Altered conciousnessAltered conciousness ExhaustionExhaustion Respiratory arrestRespiratory arrest

ITU treatmentITU treatment Continue full medical treatmentContinue full medical treatment NIVNIV
• PerhapsPerhaps IPPVIPPV
• For worsening hypoxia/hypercapniaFor worsening hypoxia/hypercapnia• ExhaustionExhaustion• Reduced concious levelReduced concious level
OptimiseOptimise• Fluid statusFluid status• Hypokalaemia (steroids, Hypokalaemia (steroids, ββ22-agonists)-agonists)

VentilationVentilation Conventionally volume controlledConventionally volume controlled Slow rateSlow rate Long expiratory timeLong expiratory time Low/no PEEPLow/no PEEP
eg. MV 115 ml/kg, TV 6-8 ml/kg, RR 8-10, PEEP 0eg. MV 115 ml/kg, TV 6-8 ml/kg, RR 8-10, PEEP 0
FFiiOO2 2 to keep SpOto keep SpO22 >=94% >=94%
Remember: hypotension, pneumothorax, EMDRemember: hypotension, pneumothorax, EMD

Acute Exacerbation of Acute Exacerbation of COPDCOPD

Acute Exacerbation of COPDAcute Exacerbation of COPD
COPD affects 5% of adult populationCOPD affects 5% of adult population
Fifth most common cause of death Fifth most common cause of death
world wide.world wide.
Chronic irreversible diseaseChronic irreversible disease
Acute deterioration can be Acute deterioration can be
precipitated by diverse causesprecipitated by diverse causes

Pathologic ProcessesPathologic Processes Bronchiolitis (inflam. airway narrowing)Bronchiolitis (inflam. airway narrowing) Loss of connective tissue tetheringLoss of connective tissue tethering Loss of alveoli and capillariesLoss of alveoli and capillaries Increased closing volumeIncreased closing volume Increased pulmonary vascular resistanceIncreased pulmonary vascular resistance
Resulting in:Resulting in:• V/Q mismatchV/Q mismatch• Increased resistanceIncreased resistance• Dynamic hyperinflationDynamic hyperinflation• Increased work of breathingIncreased work of breathing


Causes of ExacerbationsCauses of Exacerbations
Infection (50%)Infection (50%) Heart Failure (25%)Heart Failure (25%) Sputum RetentionSputum Retention PEPE PneumothoraxPneumothorax SedationSedation MedicationMedication MalnutritionMalnutrition

TreatmentTreatmentTreat underlying cause and support:Treat underlying cause and support: Oxygen (titrate avoiding carbonarcosis)Oxygen (titrate avoiding carbonarcosis) BronchodilatorsBronchodilators Steroids (not if pneumonic cause)Steroids (not if pneumonic cause) Antibiotics for infectious causeAntibiotics for infectious cause Clearance of secretionsClearance of secretions
• Physio, mucolytics, suctioning, bronchoscopyPhysio, mucolytics, suctioning, bronchoscopy Hydration, Diuretics, VasodilatorsHydration, Diuretics, Vasodilators DVT prophylaxisDVT prophylaxis NutritionNutrition no benefit from respiratory stimulantsno benefit from respiratory stimulants

Non-invasive Ventilation 1Non-invasive Ventilation 1
Ventilatory support via nasal/facemaskVentilatory support via nasal/facemask
Aims:Aims:• Unload respiratory musclesUnload respiratory muscles• Augment ventilationAugment ventilation• Improve oxygenationImprove oxygenation
• Reduce COReduce CO22

Non-invasive Ventilation 2Non-invasive Ventilation 2
Indicated for:Indicated for:
Worsening COPD with:Worsening COPD with:• Acute dyspnoeaAcute dyspnoea• RR >28/minRR >28/min
• PPaaCOCO22 > 6kPa and pH < 7.35 > 6kPa and pH < 7.35
in spite of maximal medical therapy in spite of maximal medical therapy and not related to XS Oand not related to XS O22

Invasive Ventilation 1Invasive Ventilation 1
Indications:Indications:• Exhaustion despite NIVExhaustion despite NIV• Deteriorating concious levelDeteriorating concious level• HypoxiaHypoxia• Failure of secretion clearanceFailure of secretion clearance• Respiratory arrestRespiratory arrest
Need for mechanical ventilation Need for mechanical ventilation dramatically decreases survival.dramatically decreases survival.
Weaning often difficult.Weaning often difficult.

Invasive Ventilation 2Invasive Ventilation 2
Strategy:Strategy:• Low RRLow RR• Low TVLow TV• Prolonged expirationProlonged expiration
Pitfalls:Pitfalls:• Dynamic hyperinflationDynamic hyperinflation• BarotraumaBarotrauma• Prolonged difficult weanProlonged difficult wean

Invasive Ventilation 3Invasive Ventilation 3
Outcome:Outcome:• ITU mortality 10-30%ITU mortality 10-30%• 1 year survival 50%1 year survival 50%• Depends more on previous state, Depends more on previous state,
nutrition, age than on measured nutrition, age than on measured variables.variables.

PneumothoraxPneumothorax
Pathological collection of extraalveolar Pathological collection of extraalveolar air in the pleural space.air in the pleural space.

CausesCauses
Spontaneous:Spontaneous:• Primary – no underlying lung diseasePrimary – no underlying lung disease• Secondary – COPD/CF/AIDS/Ca/chemo Secondary – COPD/CF/AIDS/Ca/chemo
Traumatic: Traumatic: • blunt or penetrating chest traumablunt or penetrating chest trauma• iatrogenic – central lines/surgeryiatrogenic – central lines/surgery
Barotrauma: Barotrauma: • positive pressure ventilation (4-15%)positive pressure ventilation (4-15%)• ARDS & IPPV (up to 60%)ARDS & IPPV (up to 60%)• (COPD/asthma)(COPD/asthma)

Clinical Features 1Clinical Features 1
Decreased or absent breath soundsDecreased or absent breath sounds Hyperresonant percussionHyperresonant percussion Chest painChest pain Dyspnoea (worse if secondary)Dyspnoea (worse if secondary) TachycardiaTachycardia Pleural line & lucent space on CXRPleural line & lucent space on CXR Hypoxaemia (if large)Hypoxaemia (if large)

PneumothoraxPneumothorax


Stab Stab woundwound

Clinical Features 2Clinical Features 2 Pneumothorax may be difficult to detect in Pneumothorax may be difficult to detect in
ventilated patient with poorly compliant ventilated patient with poorly compliant lungs:lungs:• Stiff lungs do not collapse readilyStiff lungs do not collapse readily• Gas exchange often already disorderedGas exchange often already disordered• Subtle early signs:Subtle early signs:
Decreased urine outputDecreased urine output Increased CVPIncreased CVP TachycardiaTachycardia Decreased CIDecreased CI
• High index of suspicionHigh index of suspicion• CT scanning may be usefulCT scanning may be useful


Tension PneumothoraxTension Pneumothorax
One way valve effectOne way valve effect Intrapleural gas accumulatesIntrapleural gas accumulates Displacement of mediastinumDisplacement of mediastinum Compression of contralateral lungCompression of contralateral lung Hypoxaemia due to shuntHypoxaemia due to shunt Decreased VR and CODecreased VR and CO Hypotension and EMD arrestHypotension and EMD arrest

Tension Pneumothorax Tension Pneumothorax


Treatment 1Treatment 1
Spontaneously breathing patientSpontaneously breathing patient
• Small pneumothorax (<20%) if Small pneumothorax (<20%) if asymptomatic can be treated asymptomatic can be treated conservatively.conservatively.
• Larger pneumothorax must be aspirated Larger pneumothorax must be aspirated or drained.or drained.
• Recurrence requires pleurodesisRecurrence requires pleurodesis

Treatment 2Treatment 2
Ventilated patient:Ventilated patient:
• Low threshold for draining Low threshold for draining pneumothoraces as risk of tensionpneumothoraces as risk of tension
• Place chest drain in patient with Place chest drain in patient with pneumothorax requiring ventilationpneumothorax requiring ventilation

Treatment 3Treatment 3
Tension pneumothorax:Tension pneumothorax:
• Potentially rapidly fatalPotentially rapidly fatal
• Rapid decompression based on clinical Rapid decompression based on clinical diagnosis improves survivaldiagnosis improves survival
• Don’t wait for the X-rayDon’t wait for the X-ray

Pleural EffusionPleural Effusion
Pathological collection of fluid within Pathological collection of fluid within the pleural space.the pleural space.
Starling Forces normally keep pleural Starling Forces normally keep pleural space dry.space dry.
Effusion results from:Effusion results from: Increased pulmonary capillary pressureIncreased pulmonary capillary pressure Increased capillary permeabilityIncreased capillary permeability HypoalbuminaemiaHypoalbuminaemia Lymphatic obstructionLymphatic obstruction

Clinical FeaturesClinical Features
Pleuritic painPleuritic pain CoughCough Dyspnoea.Dyspnoea. Decreased air entryDecreased air entry ““stony” dullnessstony” dullness Restrictive defectRestrictive defect

RadiologyRadiology
CXR (upright PA)CXR (upright PA)• >300ml loss of costophrenic angle>300ml loss of costophrenic angle• Larger effusions cause opacificationLarger effusions cause opacification
Lateral decubitus filmsLateral decubitus films• more sensitive (5ml)more sensitive (5ml)• Impractical on ITUImpractical on ITU
USSUSS• Extremely sensitive (2ml)Extremely sensitive (2ml)• Can be used to guide drainageCan be used to guide drainage




ThoracocentesisThoracocentesis
May help determine cause:May help determine cause: Transudate vs. ExudateTransudate vs. Exudate
• (prot >3g/dl, sg >1.016)(prot >3g/dl, sg >1.016)• Imbalance in Starling Forces vs increased Imbalance in Starling Forces vs increased
pleural membrane permeabilitypleural membrane permeability Low glucose suggests Low glucose suggests
infection/rheumatoidinfection/rheumatoid High amylase suggests pancreatitisHigh amylase suggests pancreatitis WCC>10mmWCC>10mm-3-3 suggests infection suggests infection Gram stain and culture may ID pneumonic Gram stain and culture may ID pneumonic
causecause pH <7.1 = empyemapH <7.1 = empyema

TreatmentTreatment
Treatment of underlying condition Treatment of underlying condition where appropriatewhere appropriate
Drainage if:Drainage if:• EmpyemaEmpyema• Ventilatory compromiseVentilatory compromise• h/o trauma (suspect haemothorax)h/o trauma (suspect haemothorax)
PleurodesisPleurodesis VATS/ThoracotomyVATS/Thoracotomy Pleuroperitoneal shuntsPleuroperitoneal shunts



![Intestinal Obstruction - mbbsmc.edu.pkmbbsmc.edu.pk/wp-content/uploads/2020/05/Intestinal-Obstruction... · Some definitions •obstruction [ uhb-struhk-shuhn ] noun •something](https://img.pdfslide.us/doc/110x75/607d6e609cb0912a6d0be577/intestinal-obstruction-some-deinitions-aobstruction-uhb-struhk-shuhn-noun.jpg)