Embed Size (px)
Citation preview

Respiratory System & Drugs Associated
BY,
DEVANSH MEHTA
FACULTY | ICRI INDIA
DELHI CAMPUS

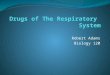
Respiratory System The respiratory system (called also respiratory apparatus, ventilatory system) is a biological system consisting of specific organs and structures used for the process of respiration in an organism.
The respiratory system is involved in the intake and exchange of oxygen and carbon dioxide between an organism and the environment.


Rubber cast of Lungs

Respiratory Pathways Air Enters the Nostrils
Then its passes through the Nasopharynx
The oral Pharynx
Through glottis
Into the Trachea
Into the right and left bronchi, which branches and rebranches into
Bronchioles , each of which terminates in a cluster of alveoli
Only in the alveoli does actual gas exchange takes place. There are some 300 million alveoli in two adult lungs. These provide a surface area of some 160 m2 (almost equal to the singles area of a tennis court and 80 times the area of our skin!).

Component of the Inhaled AirComposition of atmospheric air and expired air in a typical subject.Note that only a fraction of the oxygen inhaled is taken up by the lungs.
Component Atmospheric Air (%) Expired Air (%)N2 (plus inert gases) 78.62 74.9
O2 20.85 15.3CO2 0.03 3.6H2O 0.5 6.2
100.0% 100.0%
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/P/Pulmonary.html

Diseases of the Lungs
Pneumonia
Pneumonia is an infection of the alveoli. It can be caused by many kinds of both bacteria (e.g., Streptococcus pneumoniae) and viruses. Tissue fluids accumulate in the alveoli reducing the surface area exposed to air. If enough alveoli are affected, the patient may need supplemental oxygen.
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/P/Pulmonary.html

Asthma
In asthma, periodic constriction of the bronchi and bronchioles makes it more difficult to breathe in and, especially, out.
Attacks of asthma can be triggered by airborne irritants such as chemical fumes and cigarette smoke
Airborne particles to which the patient is allergic
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/P/Pulmonary.html

Emphysema
In this disorder, the delicate walls of the alveoli break down, reducing the gas-exchange area of the lungs. The condition develops slowly and is seldom a direct cause of death. However, the gradual loss of gas-exchange area forces the heart to pump ever-larger volumes of blood to the lungs in order to satisfy the body's needs. The added strain can lead to heart failure.
The immediate cause of emphysema seems to be the release of proteolytic enzymes as part of the inflammatory process that follows irritation of the lungs. Most people avoid this kind of damage during infections, etc. by producing an enzyme inhibitor (a serpin) called alpha-1 antitrypsin. Those rare people who inherit two defective genes for alpha-1 antitrypsin are particularly susceptible to developing emphysema.
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/P/Pulmonary.html

Chronic Bronchitis
Any irritant reaching the bronchi and bronchioles will stimulate an increased secretion of mucus. In chronic bronchitis the air passages become clogged with mucus, and this leads to a persistent cough. Chronic bronchitis is usually associated with cigarette smoking.
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/P/Pulmonary.html

Chronic Obstructive Pulmonary Disease (COPD)
Irritation of the lungs can lead to asthma, emphysema, and chronic bronchitis. And, in fact, many people develop two or three of these together. This constellation is known as chronic obstructive pulmonary disease (COPD).
Among the causes of COPD arecigarette smoke (often)
cystic fibrosis (rare)
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/P/Pulmonary.html

Cystic fibrosis is a genetic disorder caused by inheriting two defective genes for the cystic fibrosis transmembrane conductance regulator (CFTR), a transmembrane protein needed for the transport of Cl−and HCO3
− ions through the plasma membrane of epithelial cells. In healthy lungs, secretion of Cl− (along with Na+ through a different channel) draws water by osmosis into the fluid bathing the cells. In cystic fibrosis, inadequate secretion of Cl− and the resulting lack of water produces a thick, sticky mucus covering the epithelia and hampering the ability of ciliated cells to move it up out of the lungs. In addition, diminished secretion of HCO3
− lowers the pH of this liquid making it more hospitable to colonization by inhaled bacteria. The resulting inflammation increases the accumulation of mucus which plugs the airways interfering with breathing and causing a persistent cough. Cystic fibrosis is the most common inherited disease in the U.S. white population.
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/P/Pulmonary.html

Lung Cancer
Lung cancer is the most common cancer and the most common cause of cancer deaths in U.S. males. Although more women develop breast cancer than lung cancer, since 1987 U.S. women have been dying in larger numbers from lung cancer than from breast cancer.
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/P/Pulmonary.html

Lung cancer, like all cancer, is an uncontrolled proliferation of cells. There are several forms of lung cancer, but the most common (and most rapidly increasing) types are those involving the epithelial cells lining the bronchi and bronchioles.
Ordinarily, the lining of these airways consists of two layers of cells. Chronic exposure to irritants
causes the number of layers to increase. This is especially apt to happen at forks where the bronchioles branch.
The ciliated and mucus-secreting cells disappear and are replaced by a disorganized mass of cells with abnormal nuclei.
If the process continues, the growing mass penetrates the underlying basement membrane.
At this point, malignant cells can break away and be carried in lymph and blood to other parts of the body where they may lodge and continue to proliferate.
It is this metastasis of the primary tumor that eventually kills the patient.
http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/P/Pulmonary.html

Cough Cough in latin is called tussis, is a sudden and often repetitive occurring reflex which helps to clear the large breathing passages from secretions, irritants, foreign particles and microbes.
The cough reflex consists of three phases: an inhalation, a forced exhalation against a closed glottis, and a violent release of air from the lungs following opening of the glottis, usually accompanied by a distinctive sound.
Coughing is either voluntary or involuntary.

Pathophysiology of Cough A cough is a protective reflex in healthy individuals which is influenced by psychological factors. The cough reflex is initiated by stimulation of two different classes of afferent nerves, namely the myelinated rapidly adapting receptors, and nonmyelinated C-fibers with endings in the lungs. However it is not certain that the stimulation of nonmyelinated C-fibers leads to cough with a reflex as it's meant in physiology (with its own five components): this stimulation may cause mast cells degranulation (through an asso-assonic reflex) and edema which may work as a stimulus for rapidly adapting receptors.

Drugs Associated with Respiratory System
Pharyngeal demulcents: Lozenges, cough drops, linctuses containing syrup, glycerine, liquorice
Expectorants (Mucokinetics)◦ Bronchial secretions enhancers: Sodium or potassium citrate, Potassium iodide, Guaiphenesin (Glyceryl
guaiacolate), balsum of tolu, Vasaka, Ammonium Chloride.
◦ Mucolytics: Bromhexine, Ambroxol, Acetyl cysteine, Carbocistene

Anti-tussives: ◦ Opioids: Codeine, Pholcodeine.
◦ Nonopioids: Noscapine, Dextromethorphan, Chlophedianol.
◦ Antihistaminics: Chlorpheniramine, Diphenhydramine, Promethazine
◦ Adjucant Anti-tussives: Bronchodialators: Salbutamol, Terbutalin

Demulcents and Expectorants Pharyngeal demulcents sooth the throat, and reduce, afferent, impulses from the inflamed/ irritated pharyngeal mucosa, thus provide symptomatic relief in dry cough arising from throat.
Expectorants also known as Mucokinetics are drugs believed to increase bronchial secretion or reduce its viscosity, facilitating its removal by coughing.

Sodium and potassium citrate are considered to increase bronchial secretion by salt action. Potassium iodide, is secreted by bronchial glands and can irritate the airway mucosa.
Prolonged use can affect thyroid function and produce iodism. It is rarely used now.
Guaiphenesin, Vasaka, tolu balsum are plant products which are supposed to enhance bronchial secretion and mucociliary function while being secreted by tracheobronchial glands.

Mucolytics Bromhexine: A derivative of the alkaloid vaccine obtained from Adhatoda vasica is potent mucolytic and mucokinetic, capable of inducing thin copious bronchial secretion. It depolymerizes mucopolysaccharides directly as well as by liberating lysosomal enzymes-network of fibres in tenacious sputum is broken.
It is particularly useful if mucus plugs are present.
Side effects: Are Rhinorrhea and lacrimation, gastric irritation and Hypersensitivity
Dose: Adults 8 mg TDS, Children 1-5 is 4 mg BD, 5-10 years is 4 mg TDS

Anti-tussives These are drugs that act in the CNS to raise the threshold of cough centre or act peripherally in the respiratory tract to reduce tussal impulses, or both these actions.
Because they aim to control rather than eliminate cough, anti-tussives should be used only for dry cough, antitussives should be used only for dry cough (Unproductive), Or if, cough is unduly tiring, disturbs sleep, or is hazardous

Opioids Codeine, an opium alkaloid, qualitatively similar to but less potent than morphine. It is more selective for cough centre and is treated as the standard antitussives, suppresses cough for about 6 hours.
The antitussive action is blocked by naloxone indicating that it is exerted through opioid receptors in brain.
Abuse liability is low, but present, constipation is the chief draw back.
At higher doses respiratory depression and drowsiness can occur, driving may be impaired. Like Morphine, it is contraindicated in asthmatics and in patients with diminished respiratory reserve.
Dose: 10-30 mg; children 2-6 years 2.5-5 mg, 6-12 years 5-10mg, frequently used as syrup codeine phosp. 4-8 ml
Other drug is Pholcodeine

Non-opioids Noscapine (Narcotine): It depresses cough but has no narcotic, analgesic, or dependence inducing properties. It is nearly equipotent antitussive as codeine, especially useful in spasmodic cough. Headache and nausea occur occasionally as side effect. It can release histamine and produce bronchoconstriction in asthmatics
Dose: 15-30 mg, children 2-6 years: 7.5 mg, 6-12 years: 15 mg.
Other drugs are, Dextromethorphan and Chlophedianol

Antihistamines They afford relief in cough due to their sedative and anticholinergic actions, but lack selectivity for the cough centres.
They have no expectorant property, may even reduce secretions by anticholinergic actions.
They have been specially promoted for cough in respiratory allergic states, though their lack of efficacy in asthma is legendary.
Chlorpheniramine (2-5 mg), Diphenhyramine ( 15-25 mg ) and Promethazine (15-25 mg) are commonly used.

Bronchodialators Bronchospasm can induce or aggravate cough. Stimulation of pulmonary receptors can trigger both cough and bronchoconstriction, especially in individuals with bronchial hyperreactivity.
Bronchodilators relieve cough in such individuals and improve the effectiveness of cough in clearing secretions by increasing surface velocity of airflow during cough.
They should be used only when an element of bronchoconstriction is present and not routinely. Their fixed dose combinations with antitussives are not satisfactory because of differences in time course of action of the components and liability for indiscriminate use.

Drugs for Asthma Treatment strategies or Approaches
◦ Prevention of AG:AB reaction: Avoidance of antigen, hyposensitization – possible in extrinsic asthma and if antigen can be identified.
◦ Neutralization of IgE: Omalizumab
◦ Suppression of inflammation and bronchial hyperreactivity: Corticosteroids
◦ Prevention of released mediators: Mast cell stabilizers

Treatment Strategies or Approaches
◦ Antagonism of released mediators: Leukotriene antagonists, antihistamines, PAF antagonists
◦ Blockade of constrictor neurotransmitters: Anticholinergics
◦ Mimicking dilator Neurotransmitter: Sympathomimetics
◦ Directly acting bronchodilators: Methylxanthines

Drug Classification for AsthmaBronchodilators
Sympathomimetics: Salbutamol, Terbutaline, Bambuterol, Salmetrol, Formoterol, Ephedrine
Methylxanthines:
Theophylline (Anhydrous), Aminophylline, Choline theophyllinate, Hydroxyethyl theophylline, Theophylline ethanolate of piperazine, Doxophylline

◦ Anticholinergics: Ipratropium bromide, Tiotropium bromide
◦ Leukotriene antagonists: Montelukast, Zafirlukast
◦ Mast cell stabilizers: Sodium cromoglycate, Ketotifen
◦ Corticosteroids: Systemic: Hydrocortisone, Prednisolone and others
◦ Inhalational: Beclomethasone, Dipropionate, Budesonide, Fluticasone Propionate, Flunisolide, Ciclesonide
◦ Anti-IgE antibody: Omalizumab

Sympathomimetics Adrenergic drugs cause bronchodilation through Beta receptor stimulation: increased cAMP formation in bronchial muscle cell: Relaxation
In addition, increased cAMP in mast cells and other inflammatory cells decreases mediator release. Since Beta Receptors on inflammatory cells are more prone to desensitization, the contribution of this action to the beneficial effect of Beta agonists in asthma is uncertain.
Adrenergic drugs are the mainstay of treatment of reversible airway obstruction but should be cautiously used in hypertensives, ischaemic heart disease patients and in those receiving digitalis
Though adrenaline and isoprenaline are effective bronchodialators, it is the selective Beta agonists that are now used in asthma to minimize cardiac side effects

Salbutamol: A highly selective Beta agonist, cardiac side effects are less prominent.
Selectivity is further increased by inhaling the drug.
Inhaled salbutamol produces bronchodilation within 5 min and the action lasts for 2-4 hours.
Because of more frequent side effects, oral Beta agonists therapy is reserved for patients who cannot correctly use inhalers, or as alternative/ adjuvant drugs in Severe asthma
Dose: 2-4 mg oral, 0.25-0.5 mg i.m./s.c., 100 microgram by inhalation

Other drugs are,
◦ Terbutaline: Dose : - 5 mg oral, 0.25 mg s.c. 250 microgram by inhalation.
◦ Bambuterol: Dose : - 10mg oral
◦ Salmetrol and Formoterol
◦ Find out the Appropriate doses for Bambuterol, Salmetrol and Formoterol

Methyl Xanthines Theophylline and its compounds have been extensively used in asthma, but are not considered first line drugs any more. They are used more often in COPD.
Theophylline is one of the three naturally occurring methylated xanthine alkaloids caffeine, theophylline and theobromine.

Pharmacological actions CNS: Caffeine and theophylline are CNS stimulants, primarily affect the higher centres. Caffeine 150-250 mg produces a sense of well being, alertness, beats boredom, allays fatigue, thinking becomes clearer even when dullness has tended to prevail after a sustained intellectual effort.
It tends to improve performance and increase motor activity. Caffeine is more active than theophylline in producing these effects.
Higher doses cause nervousness, restlessness, panic, insomnia and excitement.
Still higher doses produce tremors, delirium and convulsions.
They also stimulate medullary vagal, respiratory and vasomotor centres.
Vomiting at high doses is due both to gastric irritation and CTZ stimulation

Pharmacological actions CVS: Methylxanthines directly stimulate the heart and increase force of myocardial contractions. They tend to increase heart rate by direct action, but decrease it by causing vagal stimulation – net effect is variable.
Tachycardia is more common with theophylline, but caffeine generally decreases heart rate. Cardiac output and cardiac work are increased. At high doses cardiac arrhythmias may be produced

Pharmacological actions Smooth Muscles: All smooth muscles are relaxed, most prominent effect is exerted on bronchi, especially in asthmatics. Theophylline is more potent than caffeine. Slow and sustained dose-related bronchodilation is produced, but the effect is much less marked compared to inhaled Beta 2 Agonists. Vital capacity is increased. Biliary spasms is relieved, but effect on intestines and urinary tract is negligible.
Kidney: Methylxanthines are mild diuretics, act by inhibiting tubular reabsorption of Na + and water. In addition, vascular effects may result in increased renal blood flow and g.f.r. Theophylline is more potent, but action is brief.

Pharmacological actions Skeletal muscles: Caffeine enhances contractile power of skeletal muscles. At higher concentration it increases release of Ca+2 from sarcoplasmic reticulum by direct action. At low doses, twitch response to nerve stimulation is augmented, while at toxic doses contraction is produced.
Stomach: Methylxanthines enhances secretion of acid and pepsin in stomach, even on parenteral injection. They are also gastric irritants: Theophylline more than caffeine.
Metabolism: Caffeine and to a smaller extent theophylline increases BMR: plasma free fatty acid levels are raised. Release of endogenous catecholamines appears to be partly responsible for these effects.

Mechanism of actionThree distinct cellular actions of methylxanthines have been defined
A) Release of Ca+2 from Sarcoplasmic reticulum, especially in skeletal and cardiac muscle.
B) Inhibition of phosphodiesterase (PDF) which degrades cyclic nucleotides intracellularly
ATPOr
GTP
cAMPOr
cGMP
5- AMPOr
5- GMP
Phosphodiestraseadenylylcyclase
guanylylcyclase Inhibited by Theophylline

C) Blockade of Adenosine receptors: Adenosine acts as a local mediator in CNS, CVS and other organs : contracts smooth muscles, especially bronchial, dilates cereberal blood vessels, depresses cardiac pacemaker and inhibits gastric secretion.
METHYLXANTHINES PRODUCES OPPOSITE EFFECTS

Action A) is exerted only at concentrations much higher than therapeutic plasma concentrations of caffeine and theophylline (Ranging from 5-20 microgram/ml)
Action B) and C) are exerted at concentration in the therapeutic range and appear to contribute to bronchodilation. Raised cAMP levels in inflammatory cells may attenuate mediator release and add to the the therapeutic effect of theophylline in asthma.

Pharmacokinetics Theophylline is well absorbed orally, rectal absorption from suppositories is erratic. It is distributed in all tissues- crosses placenta and is secreted in milk. 50 % plasma protein bound and extensively metabolized in liver by demethylation and oxidation. Only 10 % is excreted unchanged in urine.
Its elimination rate varies considerably with age. At therapeutic concentrations, the t ½ in adults is 7-12 hours.
Theophylline metabolizing enzymes are saturable, t ½ is prolonged with higher doses as kinetics changes from first to zero order: plasma concentrations, therefore, increase disproportionately.

Anticholinergics Atropinic drugs cause bronchodilatation by blocking cholinergic constrictor tone; act primarily in the larger airways.
Inhaled ipratropium bromide is less efficacious than sympathomimetics. Patients of asthmatic bronchitis, COPD and psychogenic asthma respond better to anticholinergics.
Inhaled ipratropium / tiotropium are bronchodilators of choice in COPD.

Leukotriene Antagonists Since it was realized that cystenyl leukotriens are important mediators of bronchial asthma, efforts were made to develop their antagonists and synthesis inhibitors.
Motelukast and Zafirlukast: Both have similar actions and clinical utility. They competitively antagonize cys LT receptor mediated bronchoconstriction increased vascular permeability and recruitment of eosinophil count, suppression of bronchial inflammation and hyperreactivity are noted in asthma patients.

Leukotriene Antagonists Montelukast and zafirlukast are indicated for prophylactic therapy of mild to moderate asthma as alternatives to inhaled glucocorticoids.
Though overall efficacy is lower than inhaled steroids, they may obviate need for the latter and may be more acceptable in children,
What is dose of Montelukast and Zafirlukast.?????

Mast Cell Stabilizers Sodium cromoglycate: It is a synthetic chromone derivative which inhibits degranulation of mast cells by trigger stimuli. Release of mediators of asthma like histamine, LTs, PAF, interleukins, etc, is restricted.
The basis of this effect is not well understood, but may involve a delayed Cl – channel in the membrane of these cells.
Chemotaxis of inflammatory cells is inhibited. Long term treatment decreases the cellular inflammatory response; bronchial hyperreactivity is reduced to variable extents. Bronchospasm induced by allergens, irritants, cold air, and exercise, may be prevented.

Corticosteroids Glucocorticoids are not bronchodilators. They benefit by reducing bronchial hyperreactivity, mucosal edema and by suppressing inflammatory response to AG: AB reaction or other trigger stimuli

Anti IgE Antibody Omalizumab: It is a humanized monoclonal antibody against IgE. Administered i.v. or s.c., it neutralizes free IgE in circulation without activating mast cells and other inflammatory cells. On antigen challenge, little IgE is available bound to the mast cell surface receptors to trigger mediator release and cause bronchoconstriction.
In severe extrinsic asthma, Omalizumab has been found to reduce exacerbations and steroid requirement. It is very expensive, use is reserved for resistant asthma patients with positive skin test or raised IgE levels who require frequent hospitalization. It is not itself immunogenic only injection site local reactions have been noted so far. It is being tried in other allergic diseases as well.

COPD Chronic Obstructive Pulmonary Disease (COPD) is the name for a group of conditions that occur because the lungs and airways have been damaged. Individuals with COPD have trouble breathing, and many have emphysema or a combination of asthma and chronic bronchitis.
COPD is often caused by smoking, but in a few cases it’s caused by inhaling toxins in the environment. The damage to the lungs and airways is permanent. There is no cure for COPD, but there are medications that can help you breathe easier by opening the airways and reducing the inflammation.
http://www.healthline.com/health/copd/drugs#Overview1

Short-Acting Bronchodilators
Bronchodilators are a type of medication that helps open the airways to make breathing easier. Your doctor may prescribe short-acting bronchodilators in an emergency situation or as needed for quick relief. Albuterol (Vospire ER, in Combivent, in Duoneb), levalbuterol (Xopenex), and ipratropium (Atrovent) are all short-acting bronchodilators. They come in the form of an inhaler or as a liquid that you can add to a nebulizer to inhale.
The side effects are few, but some people will experience dry mouth, blurred vision, or a cough. Other side effects include tremors (shaking), as well as the feeling that the heart is racing or beating faster than normal. If you have a heart condition, you should tell your doctor before taking these medications.
http://www.healthline.com/health/copd/drugs#Overview1

Long-Acting Bronchodilators
Long-acting bronchodilators are medications that are used to treat COPD over a longer period of time. They are usually taken once or twice daily over an extended period, and they come as inhalers or nebulizers. The long-acting bronchodilators are:
◦ Tiotropium (Spiriva)◦ Salmeterol (Serevent)◦ Formoterol (Foradil, Perforomist)◦ Arformoterol (Brovana)◦ Indacaterol (Arcapta)◦ Aclidinium (Tudorza)
http://www.healthline.com/health/copd/drugs#Overview1

Because these are used to gradually help with breathing, they are not effective in an emergency or as rescue medication.
There are some side effects that can happen when you use these medications. Some people complain of:
◦ dry mouth◦ dizziness◦ tremors◦ runny nose◦ an irritated or scratchy throat
Other more serious side effects that people have experienced include allergic reactions (rashes), blurred vision, and a rapid heart rate.
http://www.healthline.com/health/copd/drugs#Overview1

The FDA recently approved a new medication, olodaterol (Striverdi Respimat), for treatment of COPD as well. This medication comes as an inhaler that you use once a day. According to the FDA, olodaterol (Striverdi Respimat) should not be used for people who have severe COPD or in emergency situations. The side effects are the same as the other long-acting bronchodilators, though some people complain of diarrhea and back and joint pain after taking this inhaled medication.
http://www.healthline.com/health/copd/drugs#Overview1

Corticosteroids
For someone with COPD the airways can be inflamed, which makes it more difficult to breathe. Corticosteroids are a type of medication that reduce inflammation in the body, making air flow easier to the lungs. There are several corticosteroids. Some are prescribed with bronchodilators because these two medications can work together to make breathing more effective. Fluticasone (Flovent), budesonide (Pulmicort), and prednisolone are the ones doctors commonly prescribe for COPD.
http://www.healthline.com/health/copd/drugs#Overview1

Fluticasone comes as an inhaler that you use once or twice daily. Some people report headaches, sore throat, a change in their voice, and allergic reactions.
Budesonide comes as a powder, liquid, or in an inhaler. Some people who have used this medication get colds or an infection in the mouth (thrush).
Prednisolone comes as a pill, liquid, or as a shot and is usually given for emergency rescue.
http://www.healthline.com/health/copd/drugs#Overview1

Phosphodiesterase-4 Inhibitors
Your doctor may prescribe you a phosphodiesterase-4 inhibitor. This medication helps relieve inflammation, which can improve air flow to the lungs. Roflumilast (Daliresp) is a phosphodiesterase-4 inhibitor and comes as a pill that you take once per day. Your doctor will usually prescribe this along with a long-acting bronchodilator. The side effects of roflumilast are weight loss, diarrhea, cramps, and tremors. You should tell your doctor if you have liver problems before taking this medication.
http://www.healthline.com/health/copd/drugs#Overview1

Methylxanthines
Some people have severe difficulty with COPD and the regular or first-line treatments alone don’t seem to help. When this happens, some doctors will prescribe theophylline, which works as an anti-inflammatory and relaxes the muscles in the airway, to take along with a bronchodilator. Theophylline comes as a pill or a liquid that you take on a daily basis, and combined with other medications, it can help you breathe easier.
Some people have had side effects when they have used theophylline. Some people report feeling queasy or vomiting. People who take theophylline have also had tremors and trouble sleeping.
http://www.healthline.com/health/copd/drugs#Overview1