Embed Size (px)
Citation preview

Resistant Gram Positives and Use of Newer Antimicrobials in SOT
Dr. Dino SgarabottoTransplant ID Unit
Padova General HospitalPadova - Italy

Short Case: MRSE vascular graft-related septic shock
• 52 yr old male patient was diagnosed an ascending aortic pseudoanerysm at the level of the end to end anastomosis between donor and recipient aorta and an aortic arch aneurysm, three years after a HTx
• A conventional repair was inappropriate because of significant comorbidities. Therefore, the patient underwent a debranching of the aneurysmatic neck vessels associated with vascular graft anastomosis between the left and right common carotid artery and the left subclavian artery and an aortic arch stent insertion for aneurysm exclusion, via transapical access in mini-thoracotomy
• Two months after surgery, after a few days of low grade fever, the patient developed hypotension and he was admitted to ICU with a clinical diagnosis of septic shock
• 6 blood cultures grew Methicillin-Resistant Staphylococcus epidermidis (MRSE) with a Vancomycin/Teicoplanin MIC of 4, Daptomycin MIC of 1 and Doxycycline MIC of 1 ug/ml
1/2

%
• Empiric antibiotic therapy was Meropenem/Ciprofloxacin/Teicoplanin
• Therapy was then switched to Daptomycin 8 mg/kg/24h associated with Doxycycline 100 mg/12h, with steady clinical improvement
• Four weeks later, the patient was transferred from ICU to a heart rehabilitation center, where the antibiotic treatment was continued over the next 4 weeks
• In conclusion, the patient received 8 weeks of Daptomycin/Doxycycline without any further maintenance antibiotic therapy. At 11 month follow-up, the clinical course has been uneventful
• This case report suggests that MRSE was deeply embedded in the stent biofilm, posing a serious limitation to antibiotic efficacy
• Our long term follow-up may suggest that Daptomycin/ Doxycycline association might not only have achieved suppression but perhaps even MRSE eradication from the biofilm
2/2

Resistant Gram Positive Bacteria
• Resistance to Penicillin • Resistance to Methicillin• Resistance (or tolerance) to
Vancomycin/Teicoplanin• Resistance to new antibiotic
(occasionally)

•CNS & MRSA
1
•VISA & hVISA
2
3
•VRE and Enterococcus
4
Resistant Gram Positive
● Pen R Strept pneum

Crit Care Med. 1999 May;27(5):853-4.
Nosocomial infections in medical intensive care units in the United States
CNS
EnterococcusStaph aureus
Fungi
Others

Epidemiology of Microorganisms Causing CVC-Related BI in Patients Receiving TPN, 1997–2008
Collins C J et al. Clin Infect Dis. 2009;49:1769-1770
YEAR
1997-1999 2002-2002 2003-2005 2006-2008 Overall (%)
No of CVC 653 619 620 684 2,576
CVC days 3675 3608 3844 4334 15,461
Organism
CoNS 49 36 43 26 154 (69.4)
MSSA 20 7 5 0 32 (14.4)
Candida 3 2 4 2 11 (5.0)
GNB 3 3 2 3 11 (5.0)
MRSA 1 2 4 0 7 (3.2)
NFGNB 0 1 2 2 5 (2.3)
Enterococci 1 0 0 1 2 (0.9)
TOTAL 77 51 60 34 222 (100.2)
Infection Ratea 21.7 13.7 15.6 7.7 14.4
Data are no of cases, unless otherwise indicated. GNB, Enterobacteriaceae; NFGNB, non-fermenting Gram-negative bacilli.a No of cases per 1000 CVC days.

Increasing Frequency of Resistance
MRSA = methicillin-resistant Staphylococcus aureus; VRE = Vancomycin-resistant enteroccoci FQRP = Fluoroquinolone-resistant Pseudomonas aeruginosa

• New drug development: $800,000,000 and 8 yrs
• Other markets are better
• Agency is indecisive
• Expectations are unclear
• Changes are common
• Delays have become norm
Introduction of New Antibacterial Classes

Declining New Antibacterial Drug Approvals
Spellberg, CID 2004, Modified
Ap
pro
vals

New drugs• Synercid (Quinupristin/dalfopristin)
• Linezolid
• Tigecycline
• Daptomycin
• Lipoglycopeptides Telavancin approved for cSSSI (phase III clinical trial for nosocomial pneumonia)
Dalbavancin for cSSSI in phase III clinical trial (MRSA and MRSE, VISA and VRE)
• Fifth generation cephalosporins Ceftobiprole approved for cSSSI in Canada and Swissland, more studies
needed for USA and EU
Ceftaroline approved for cSSSI and CAP
• Iclaprim in phase III clinical trial for cSSSI and nosocomial pneumonia

Bacteria (no. of isolates) MIC90 (µg/mL)
Telavancin Vancomycin Linezolid Daptomycin Quinupristin-dalfopristin
MSSA (n=1217) 0.5 1 2 0.5 0.5MRSA (n=1082) 0.25 1 2 0.5 0.5MSSE (n=100)
0.5 2 1 1 0.25
MRSE (n=272)0.5 2 1 1 0.25
E. faecalis vancomycin susceptible (n=429) 1 2 0.25 1 1E. faecalis
harboring VanA gene (n=22) 16 >512 2 1 N/AE. faeciumvancomycin susceptible (n=92) 0.25 1 2 4 2E. faecium
harboring VanA gene (n=223) 8 512 2 4 1E. faecium
harboring VanB gene (n=17) 2 0.5 1 4 4S. Pneumoniae penicillin susceptible (n=204) 0.03 0.5 1 N/A N/AS. Pneumoniae penicillin nonsusceptible (n=72) 0.015 0.5 1 N/A N/A

Acquisition costsDrug Dosage Regimen a,b Cost/Day/patient ($) Cost/14 day therapy ($)
Telavancin 10 mg/kg IV q 24 hours1 (750 mg) + 1 (250mg) vial = $131.60/day
$1842.40
Vancomycin 15 mg/kg IV q 12 hours 3 (1000 mg) vials =$12.15/day
$170.10
Daptomycin 4mg/kg IV q 24 hours 1 (500 mg) vial = $129.82/day
$1817.48
Linezolid 600 mg IV q 12 hours2 (600 mg) vials = $115.76/day $1620.64
Quinupristin-dalfopristin
7.5 mg/kg IV q 12 hours 3 (500 mg) vials = $267.99/day
$3751.86
Tigecycline Loading dose of 100 mg x 1 then 50 mg IV q 12 hours
2 (50 mg) vials = $75.20/day
$1090.40
Ceftaroline 600 mg IV q 12 hours2 (600 mg) vials = $ 82/day $1148

In the last ten years – despite being a bacteriostatic for the good penetration in soft
tissues, lungs, and CSF- several studies have considered non inferiority of linezolid in
the following settings:
• cSSSI
• nosocomial pneumonia
• neurosurgical meningitis
However,
not even in nosocomial pneumonia (see: “Linezolid versus vancomycin or teicoplanin for nosocomial pneumonia: a systematic review and meta-analysis” by Kalil AC, Murthy MH, Hermsen ED, Neto FK, Sun J, Rupp ME in Crit Care Med. 2010 Sep;38(9):1802-8)
MRSA: Linezolid vs Vancomycin
good tissue penetration does not mean
clinical superiority

Left sided endocarditis
• If MRSA is the cause: none of the new drugs is non-inferior to vancomycin
• If VRE is the cause: still missing a replacement for vancomycin

10 novel antibacterial drugs by 2020

-8
-7
-6
-5
-4
-3
-2
-1
0
1
2
Rifam
Vanco
/Rifa
m
LZD/Rifa
m
LVX/Rifa
m
Dapto
4/R
ifam
Dapto
6/R
ifam
Vanco
Dapto
4
Dapto
6
P<0,05
P<0,001
P<0,01
Animal Model of Implant-Associated Infection:Killing of planktonic MRSA in cage fluid 5 days after
the completion of therapy
Modified from John AK, Baldoni D, Haschke M, Rentsch K, Schaerli P, Zimmerli W, and Trampuz A: AAC 2009, 53: 2719-2724
ΔL
og10
CF
U/m
l
Saline

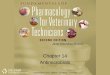
Animal Model of Implant-Associated Infection:cure rate of adherent MRSA in explanted cages
Salin
e
Vanco
Dapto
4
Dap
to 6
Rifam
Vanco
/Rifa
m
LZD/Rifa
m
LVX/Rifa
m
Dapto
4/Rifa
m
Dapto
6/Rifa
m
010203040506070
Cure rate (%)P<0.001
P<0.05
Modified from Antimicrobial Agents and Chemiotherapy 2009, 53: 2719-2724

Summary
• New antimicrobials against Gram positive bacteria are available and some other are on the way: the future looks better compared with what we have against MRD Gram negative
• VRE still is the most difficult to be treated in particular settings
• Device-related infections are highly challenging once the device cannot be removed
• For the time being there is still the need of using antibiotic associations for exploiting the synergistic effects
• Animal data suggest all rifampin associations have not the same potency: some are better than others
• Still a lot has to be done:
Doxycycline or tigecycline can substitute Rifampin? 3 antibiotics instead of 2 against a biofilm can be better like in TB and in
HIV therapy?