Embed Size (px)
DESCRIPTION
Nick RiegerCiccocioppo A, Hewett P, Rodda D, Stephens J.Adelaide
Citation preview

Rectal Cancer and Radiotherapy:What is the Clinical Implication
of a Complete Response
Nick RiegerCiccocioppo A, Hewett P, Rodda D,
Stephens J.
Adelaide
No Disclosures

Advanced Rectal Cancer
T3, N1 or greater
Assessment Clinical, Rectal ultrasound, MRI.

Pre-operative Radiotherapy Improve expected survival Reduce local recurrence. Down staging of disease and convert a surgical
situation that may well be non curative to one that is curative.
Improved compliance with treatment if given before surgery
Radiation is given to tissues that are to be excised and not to tissues that form the reconstruction of the bowel continuity which may have an adverse effect on future bowel function
Radiotherapy is given to tissues and tumour with good blood supply and oxygenation, potentially improving its efficacy.

Complete ResponseLong Course Radiatiotherapy
Complete Clinical Response (CcR) Complete Pathological Response
(CpR)

Complete Clinical Response (CcR) Response to radiotherapy assessed prior to resection. No visible or palpable tumour this is labelled as a complete clinical
response. Some authors who are controversially advocating no surgery and
observation of the tumour or local excision over radical resection. Habr-Gama A, Perez RO, Nadalin W, Sabbaga J, Ribeiro U Jr,
Silva e Sousa AH Jr, Campos FG, Kiss DR, Gama-Rodrigues J. Operative versus nonoperative treatment for stage 0 distal rectal cancer following chemoradiation therapy. Ann Surg. 2004;240:711-718.)
265 patients treated with conventional CRT. Patients were assessed at 8 weeks after CRT. Incomplete clinical response were treated by radical surgical
resection (194 patients; 73%). Of these 22 patients had a complete pathological response.
Patients with a complete clinical response (71 patients; 27%) were managed by observation alone. No surgery was performed. At a mean follow-up of 57.3 months there were 3 systemic recurrences and 2 local recurrences (seen on endorectal ultrasound). The 5 year overall survival and disease free survival was 100% and 92% respectively.

Complete Clinical Response (CcR) The difficulty with this approach is that in the absence of a
resection there is no absolute means of determining an absence of tumour cells within the rectal wall, mesorectum or draining lymph nodes.
Hiotis SP, et al. Assessing the predictive value of clinical complete response to neoadjuvant therapy for rectal cancer: an analysis of 488 patients. J Am Coll Surg. 2002;194:131-5.
448 patients after preoperative chemoradiotherapy. Retrospective review of patients with T3, T4 or node
positive disease. A CcR was seen in 19% of the patients. All patients underwent resection and the complete
pathological response rate was 10%. Many patients therefore had persisting viable tumour cells
not otherwise detected.

Complete Clinical Response (CcR)
Zmora O, et al. Does rectal wall tumor eradication with preoperative chemoradiation permit a change in the operative strategy? Dis Colon Rectum. 2004;47:1607-12.
109 patients after chemoradiation. A clinical complete response was seen in 47 patients. After radical resection only 17 patients had an absence of
tumour in the rectal wall (T0). Importantly in these 17 T0 patients viable tumour cells were
found in the lymph nodes or mesorectum in 4 patients. The authors cautioned avoiding radical surgery in patients
with a complete clinical response in the rectal wall.

Complete Pathological Response (CpR)Does it influence choice of operation?
Another area of controversy is the statement by some authors that by giving preoperative CRT improved sphincter preservation may result.
Valentini V, et al. Does downstaging predict improved outcome after preoperative chemoradiation for extraperitoneal locally advanced rectal cancer? A long-term analysis of 165 patients. Int J Radiat Oncol Biol Phys. 2002;53:664-74.
The choice of operation is based on the distance from the lower pole of the tumour after chemoradiation to the anus. Such an approach may potentially risk increased local recurrence rates if clinical response is equated with pathological response. Viable tumour cells may persist at the site of the original cancer which has regressed after treatment. The nature of the operation to be performed is best determined at presentation and prior to receiving preoperative treatment.

Rectal Cancer and CpR well described in the literature.
Literature Review: CpR %Bozzetti et al. Cancer 1999; 86: p398
8.5
Videtic et al IJRBOP 1998; 42: p31913
Gavioli et al Dis Colon Rectum 2005; 48: p185117.9
Valentine et al. IJRBOP 1999; 45: p1175 23
Janjan et al. Am J Clin Oncol 2001; 24: p10727
• The Outcomes of these patients are less well described.

Adelaide Data
•A group of patients with locally advanced rectal cancer who had a complete histopathological response to preoperative long course radiotherapy were identified from our prospective database.

AIMS
• This study aims to evaluate the outcomes patients with locally advanced rectal cancer who had a CpR from long course pre-operative chemoradiotherapy.

Chemo-Radiotherapy Regimens
Chemotherapy:• All patients received 5FU as part of their pre-op
chemoradiotherapy treatment.
• After surgery all patients were recommended to complete a 4 further cycles of chemotherapy. All but one patient complied.
Radiotherapy: • 45 to 50.4 Gy in 25 to 28 fractions.
Surgery: • Median 6 weeks after radiotherapy.

Results• A total of 306 patients presented with Rectal Cancer (all
stages) between Nov 1998- Jul 2004.
• Forty (13.1%) of these patients had locally advanced disease and received long course preoperative Chemo-Radiotherapy (CRT)
• Of these 7 (17.5%) were found to have a complete response on histopathology with no residual tumour in the bowel or lymph nodes.
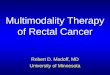
• At the time of diagnosis all 40 patients were staged as T3 tumours based on Endorectal Ultrasound and CT scan.

Endorectal Ultrasound: T3 Endorectal Ultrasound: T3 TumourTumour

Treatment RegimensProcedures Performed CpR Non-
CpRAbdomino-perineal Resection 2 (28%) 8 (24%)Ultra-low Anterior Resection 2 (28%) 13(39%)Low Anterior Resection 1 (14%) 6 (18%)Anterior Resection 1 (14%) 4 (12%)Low Hartmann Procedure 1 (14%) 0Recto-sigmoid Resection 0 1 (3%)Total Procto-colectomy 0 1 (3%)

STATISTIC CpR Non-CpR
No. of Patients 7 33
Male:Female 5M : 2F 21M : 12F
Median F/U Time (yrs)
6.0 (1.42-7.02)
3.8 (2.05-5.92)
Mortality 1 (14%) 7 (21%)
Disease Recurrence
0 20 (60.6%)

Results
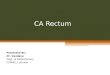
Fisher’s Exact Test revealed a significant difference in combined outcome of mortality and disease recurrence between the CpR and Non-CpR Groups (P = 0.0396)
0
20
40
60
80
Per
cen
tag
e
COMPLETE NON-COMPLETE
Mortality and Disease Recurrence Outcomes of Complete vs Non-Complete Responders
MORTALITY
RECURRENCE

Results
• One CpR patient is deceased as a result of non-tumour/surgery related causes. This patient was aged 75 years at diagnosis and had a TFS of 2.76 years.
• At present all complete responders remain disease free, with a median tumour free survival of 5.65 years (range 1.42-7.02 years).
• The deaths of all Non-CpR patients resulted from complications of recurrent disease.
• All patients have had follow up with clinical examination, CT scan, colonoscopy and CEA.

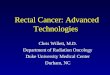
At Diagnostic At Diagnostic ColonoscopyColonoscopy
Following Pre-Following Pre-operative Long operative Long Course RadiotherapyCourse Radiotherapy
Ulcer-like Scar Ulcer-like Scar remainsremains
A COMPLETE RESPONDER- COLONOSCOPYA COMPLETE RESPONDER- COLONOSCOPY

Complications
Surgical• 1x re-laparotomy in CpR patient for bowel obstruction 1/52
following initial procedure.
• Ureteric injury and an anastomotic leak requiring reoperation in different Non-CpR patients.
Radiotherapy• Mild degrees of toxicity were noted in approximately 50% of ALL
patients.
• Mild proctitis, cystitis and mucositis settling soon after radiotherapy. One patient experienced erectile dysfunction.

Summary
• Pre-operative long course radiotherapy is generally well tolerated with few major adverse effects.
• The CpR rate of 17.5% in our patients compares to that described in the literature.

Conclusions
•For patients with Advanced (T3) Rectal Cancer, Complete Histopathological Response to Preoperative Chemo-radiotherapy is associated with excellent survival and recurrence outcomes.

Conclusions
Complete clinical response does not equate to complete pathological response.
Response to pre-operative therapy should not influence the nature of the surgery.