Embed Size (px)
Citation preview
Transanal Surgery for Large Rectal Polyps
and Early Rectal Cancer
AB HarikrishnanConsultant Colorectal Surgeon, Sheffield
Honorary Clinical Senior Lecturer, Sheffield University
Associate TPD General Surgery, Yorkshire Deanery
ACPGBI Yorkshire Chapter Representative
Sheffield Colorectal
Clinicopathologic assessment
• What is it?• TVA / HGD / T1 / T2
• How does it look?• Size, sessile, flat, stalk, residual scar from previous surgery or
EMR
• Where is it?• Rectum / rectosigmoid / peritoneal reflection• Distance from anal verge• Rectal folds• Lateral orientation• Circumference
Sheffield Colorectal
Options
• Colonoscopic EMR / ESD
• Transanal Surgery• Transanal excision (Parks) / TART• TEMS / TEO• TAMIS• TASER• RATS
• Radical surgery
• Contact radiotherapy
• Follow up
Sheffield Colorectal
Sheffield Colorectal
Options
• Colonoscopic EMR / ESD
• Transanal Surgery• Transanal excision (Parks) / TART• TEMS / TEO• TAMIS• TASER• RATS
• Radical surgery
• Contact radiotherapy
• Follow up
Sheffield Colorectal
Options
• Colonoscopic EMR / ESD
• Transanal Surgery• Transanal excision (Parks) / TART• TEMS / TEO• TAMIS• TASER• RATS
• Radical surgery
• Contact radiotherapy
• Follow up
Sheffield Colorectal
Surgery – Transanal excision/TART
• Lower rectum < 5 cm from verge
• Posterior lesions – full thickness excision
• Lloyd Davies, prone or lateral position
• Kit – Parks anal retractor, diathermy
• Local infiltration to lift – excise - direct closure of defect
• 1 cm margin
• Anterior lesions – injury to vagina, prostate or urethra
Sheffield Colorectal
Transanal excision limitations
• Views
• Retraction
• Distance from anal verge
• Transanal excision results
Sheffield Colorectal
Options
• Colonoscopic EMR / ESD
• Transanal Surgery• Transanal excision (Parks) / TART• TEMS / TEO• TAMIS• TASER• RATS
• Radical surgery
• Contact radiotherapy
• Follow up
Sheffield Colorectal
Transanal Endoscopic Microsurgery - TEM
• Prof Gerhard Buess, Germany 1983
• Proctoscope (fixed, beveled), camera, light source, working channels, suction irrigation (Richard Wolff)
• 180 deg -210 deg view
• Target lesion is inferior (lower) to working channels
• Patient position
• n=383, 4% recurrence, 10% complications (Buess, 1985)
Sheffield Colorectal

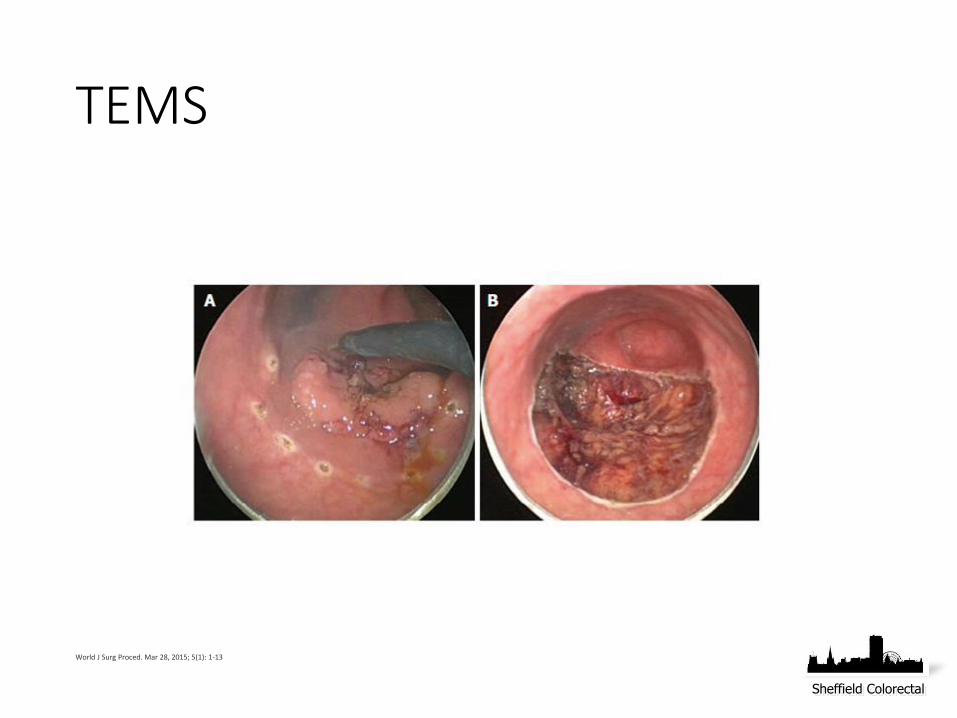
TEMS
World J Surg Proced. Mar 28, 2015; 5(1): 1-13
Sheffield Colorectal
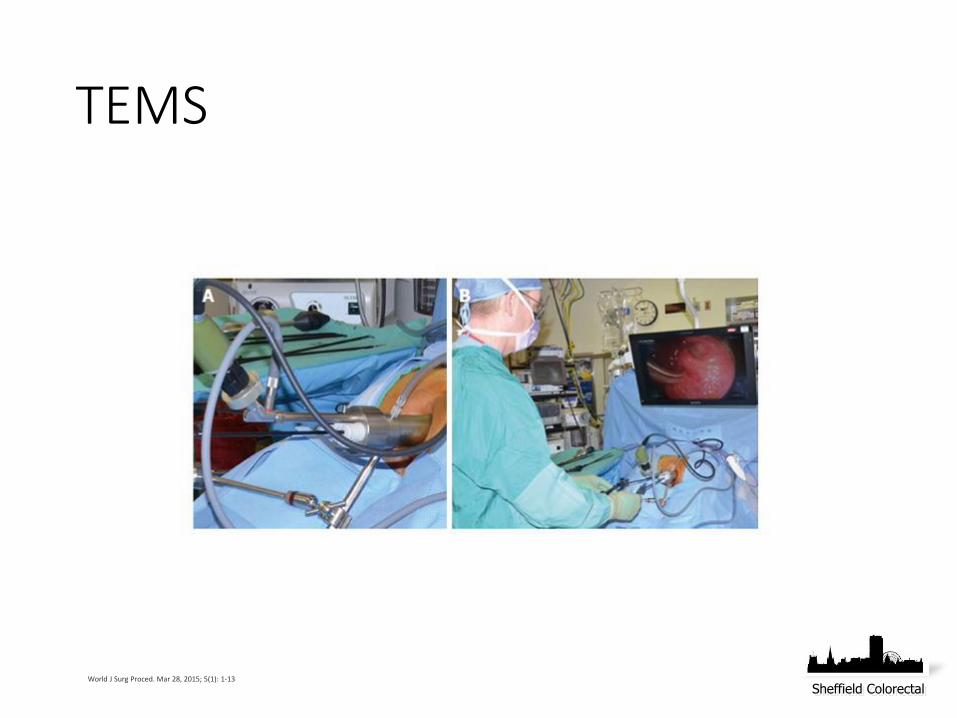
TEMS
World J Surg Proced. Mar 28, 2015; 5(1): 1-13
Sheffield Colorectal
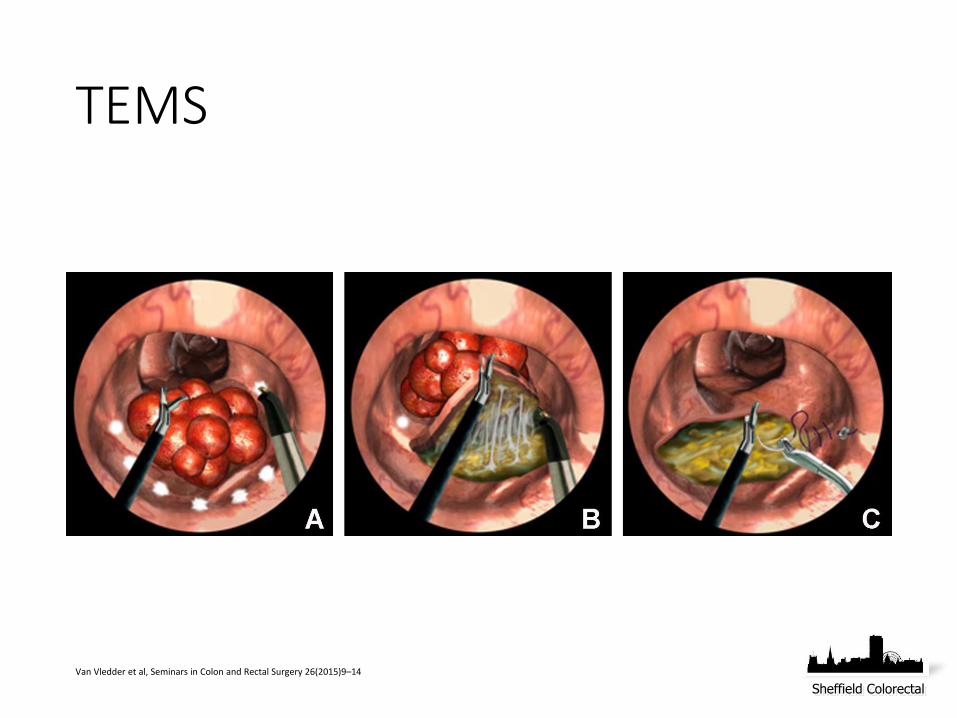
TEMS
Van Vledder et al, Seminars in Colon and Rectal Surgery 26(2015)9–14
Sheffield Colorectal
TEMS
World J Surg Proced. Mar 28, 2015; 5(1): 1-13
Sheffield Colorectal
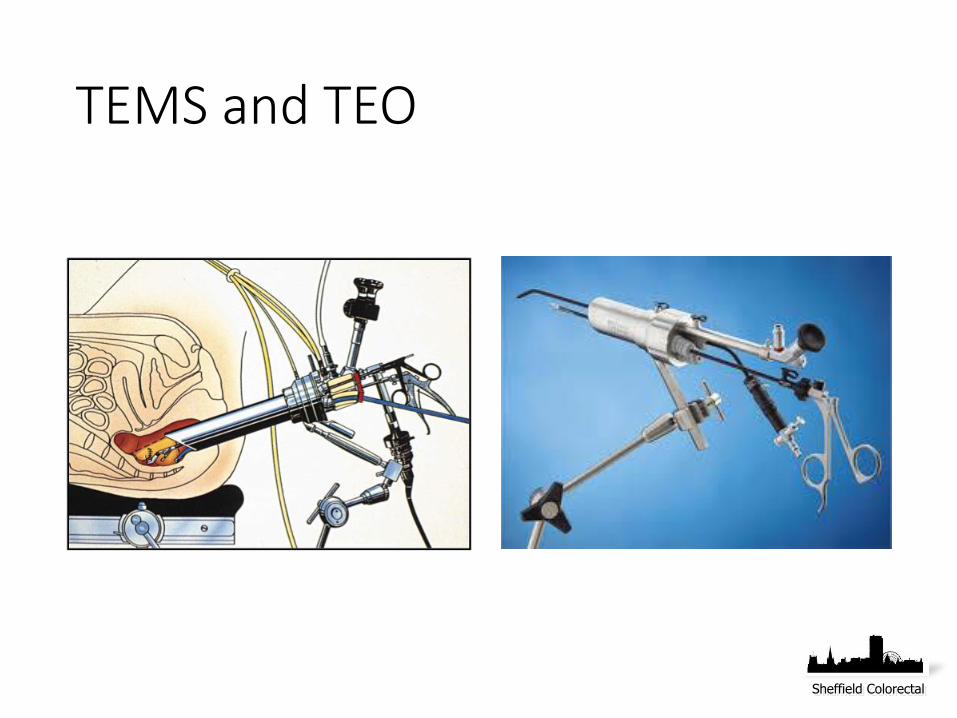
TEMS and TEO
Sheffield Colorectal

TEMS vs TA Excision
• Systematic review – Moore et al, DCR 2008• 55 case series + 3 comparative studies
• Negative margins 90% vs 71%
• Non-fragmented specimens 94% vs 65%
• Local recurrence 5% vs 27%
Sheffield Colorectal

TEMS vs Transanal Excision SR and MA, Clancy et al, DCR 2015
• 6 comparative series, No RCT, n=927
• Post op complications OR 1.018 p=0.937
• Negative margins OR 5.281 p<0.001
• Fragmented specimens OR 0.096 p<0.001
• Local recurrence OR 0.248 p<0.001
Sheffield Colorectal

TEMS and peritoneal perforation
• n= 481, 13 rectal cancers
• Perforation = 28 (5.8%)
• Conversion to abdominal procedure = 3/28 (10%) 2 lap, 1 open
• Morbidity – 1/28 (3.8%) rectovesical fistula - APER
• Mortality – Nil
• Perforation group• Longer op time (120 vs 60 min) p<0.001• Longer hospital stay (6 vs 4 days) p=0.003
• Multivariate analysis – distance from verge >7cm (p=0.010)
• Overall survival/distant mets – no difference
Morino et al. Surg Endosc (2013) 27:181–188Sheffield Colorectal
TEMS and anorectal function
• Resting and squeeze pressures fall in first 3 months
• Return to baseline in 6 – 12 months
• Rectal sensitivity thresholds reduced at 3 months• Urgency• Increase Wexner score• Return to normal in 1 year
• QOL scores at 1 year and 5 years are high
• Longterm QOL scores are better than TME group
Allaix et al. Surg Endosc (2016) 30:4841–4852 Sheffield Colorectal
TEMS vs radical resection T1/T2
• n=942, 10 trials, TEMS 445, RR 438 – systematic review and meta-analysis
TEMS RR OR
• Local recurrence 48 13 2.78
• Overall recurrence 62 31 2.01
• Distant recurrence 14 16 0.87
• Overall survival 190 193 0.80
• Mortality 14 17 0.7
• TEMS – shorter op time & LoS, reduced complications
Sajid et al. Colorectal Dis. 2014 Jan;16(1):2-14. Sheffield Colorectal
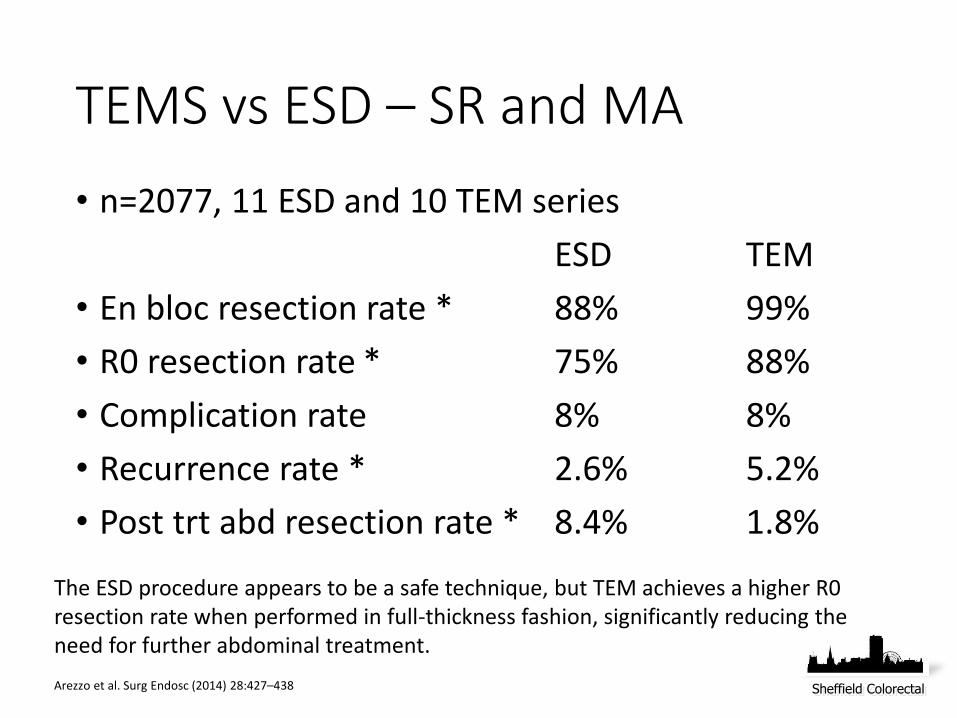
TEMS vs ESD – SR and MA
• n=2077, 11 ESD and 10 TEM series
ESD TEM
• En bloc resection rate * 88% 99%
• R0 resection rate * 75% 88%
• Complication rate 8% 8%
• Recurrence rate * 2.6% 5.2%
• Post trt abd resection rate * 8.4% 1.8%
Arezzo et al. Surg Endosc (2014) 28:427–438
The ESD procedure appears to be a safe technique, but TEM achieves a higher R0 resection rate when performed in full-thickness fashion, significantly reducing the need for further abdominal treatment.
Sheffield Colorectal
Recurrence after TEMS
• Restage and reassess the patient
• Locoregional / distant
• Redo TEMS – benign, HGD, fitness
• Malignant lesion• Anterior resection / APER/ TaTME• Ext Radiotherapy – locoregional control• Contact radiotherapy
• Distant disease• Chemotherapy
Sheffield Colorectal
TEMS Complications• Operative mortality <1%
• Major complications <2%• Rectal wound dehiscence• Bleeding – reactionary and delayed• Rectal pain• Perirectal abscess and fistula• Rectovaginal fistula• Rectal stricture
• Minor complications <10%• Urinary retention• Mucus discharge• Minor bleeding
• Functional outcomes• QOL preserved at 1 year and 5 years• QOL and sexual function impaired for post RTX group
Sheffield Colorectal
TEMS for rectal Ca – new perspectives
• Lymph node staging• Endoscopic posterior mesorectal excision (EPMR). Tarantino et al, 2008.• Safe, low morbidity, comparable oncological data !
• Sentinel lymph node biopsy• NTEMS – nucleotide guided TEMS and LN sampling. Lezoche et al, 2013.• Indocyanine Green (ICG) / near IR camera sampling. Arezzo et al, 2014.
• Predictive biomarkers• Chromosome 8q23-24 gain = marker for LN +ve. Ghadimi et al, 2003.• Chromosomal copy number. Chen et al, 2013.
• PROGRESSS – perirectal oncologic gateway for RP endoscopic single-site surgery. Leroy et al 2013.
• Robotic assisted transanal surgery (RATS). Atallah et al, 2015.Sheffield Colorectal
Early Rectal Cancer – other treatment options
• Selective post op radiotherapy
• Neoadjuvant radiotherapy followed by TEM
• Neoadjuvant chemorad followed by TEM• Rectal wound complications are high• Oncological outcome similar to standard resection• Functional outcomes are poor
• TrialsSheffield Colorectal

Trials
• TREC• T1-2N0 • TME/APER vs SCRT + TEMS
• STAR-TREC• T1-3bN0• TME vs SCRT/CRT followed by w&w or TEMS
• TESAR• T1-2, medium risk• Post TEMS – Adjuvant chemorad vs TME
• TREND• Large rectal adenomas• TEMS vs EMR
• CARTS• Neoadjuvant long course chemorad followed by TEMS
Sheffield Colorectal
Options
• Colonoscopic EMR / ESD
• Transanal Surgery• Transanal excision (Parks) / TART• TEMS / TEO• TAMIS• TASER• RATS
• Radical surgery
• Contact radiotherapy
• Follow up
Sheffield Colorectal
Trans Anal Minimally Invasive Surgery (TAMIS)• Atallah et al, Surg Endo 2010
• Single-incision, multiport device
• Laparoscopic instruments and energy source
• Laparoscopic surgical skills – parallel choreography
• Applied to transanal surgery
• FDA approval• GelPOINT Path (Applied Medical)
• SILS Port (Medtronic)
Sheffield Colorectal
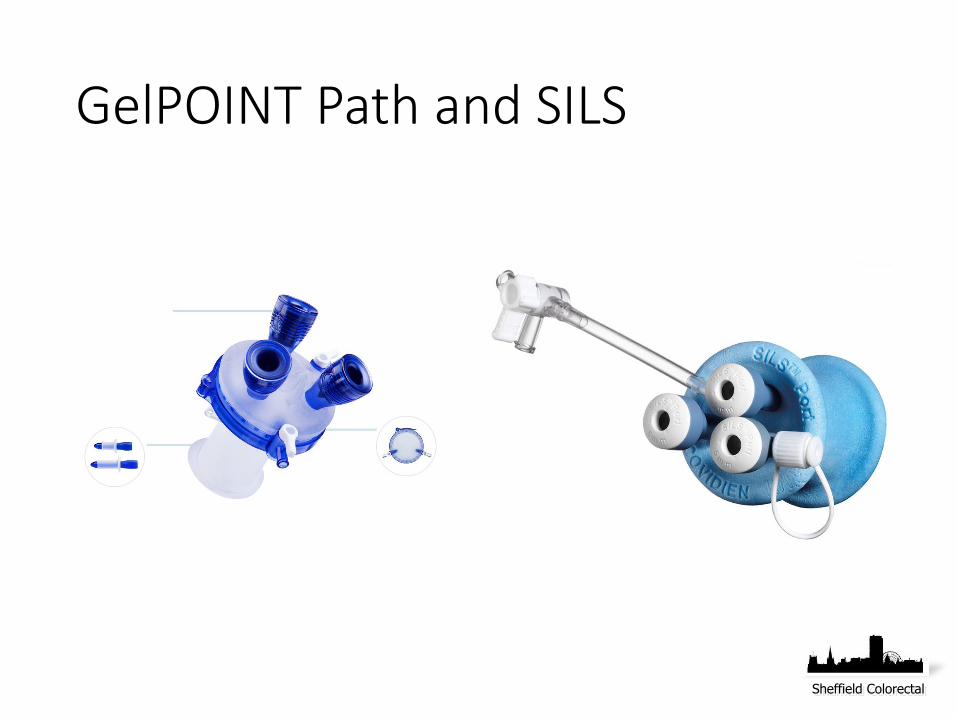
GelPOINT Path and SILS
Sheffield Colorectal
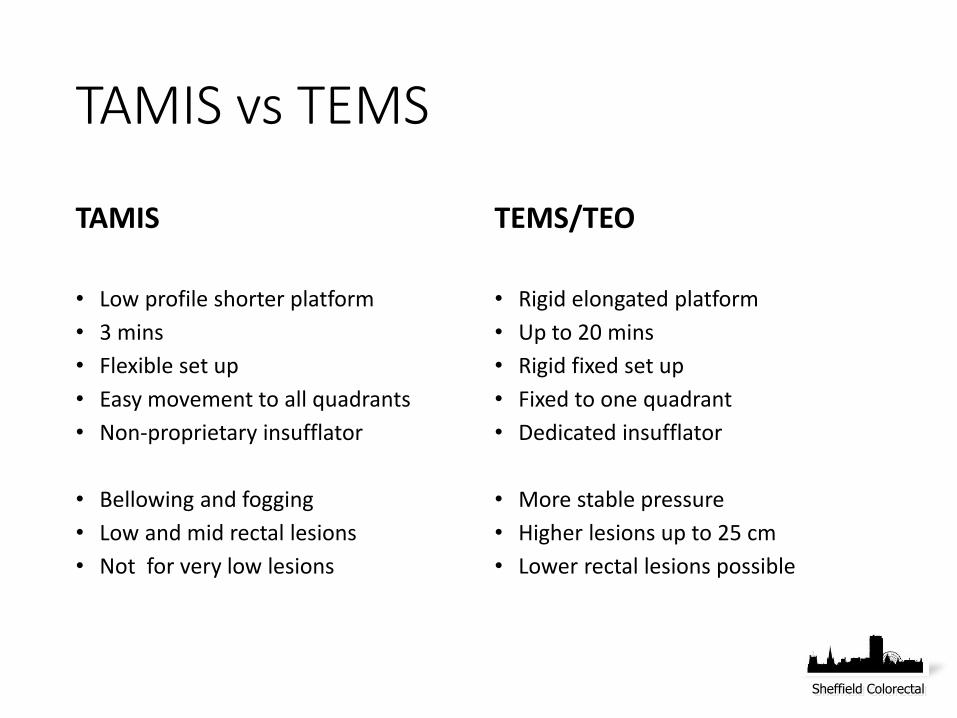
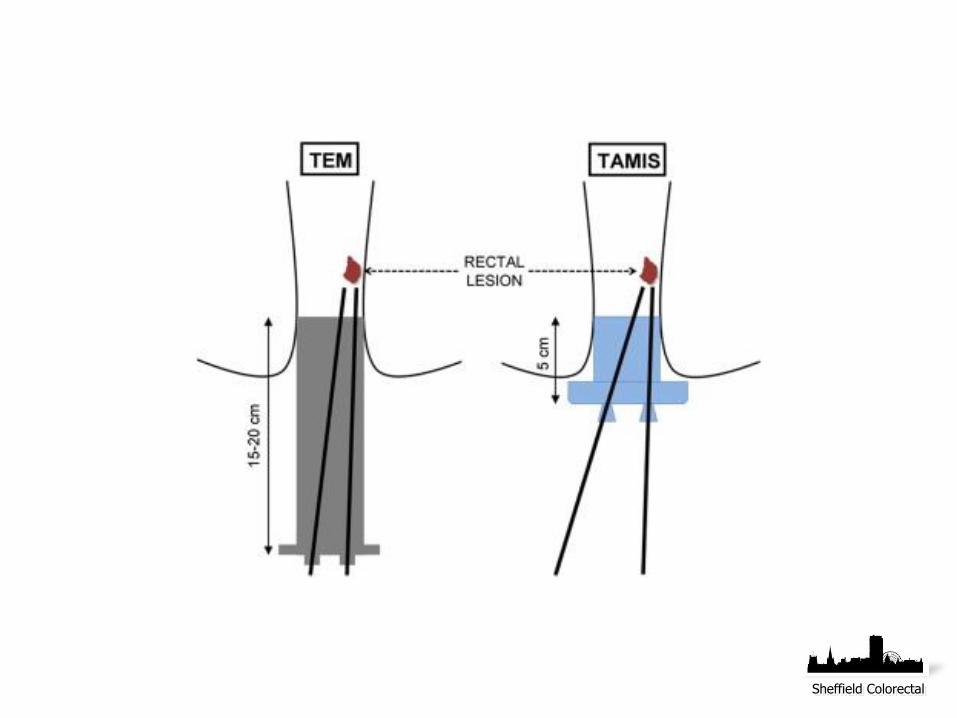
TAMIS vs TEMS
TAMIS
• Low profile shorter platform
• 3 mins
• Flexible set up
• Easy movement to all quadrants
• Non-proprietary insufflator
• Bellowing and fogging
• Low and mid rectal lesions
• Not for very low lesions
TEMS/TEO
• Rigid elongated platform
• Up to 20 mins
• Rigid fixed set up
• Fixed to one quadrant
• Dedicated insufflator
• More stable pressure
• Higher lesions up to 25 cm
• Lower rectal lesions possible
Sheffield Colorectal
Sheffield Colorectal
TEMS vs TAMIS
• Transferable skills
• Complementary approaches
• Cost effective to choose one
• Foundation for other procedures• TaTME
• SILS
• TASER
Sheffield Colorectal
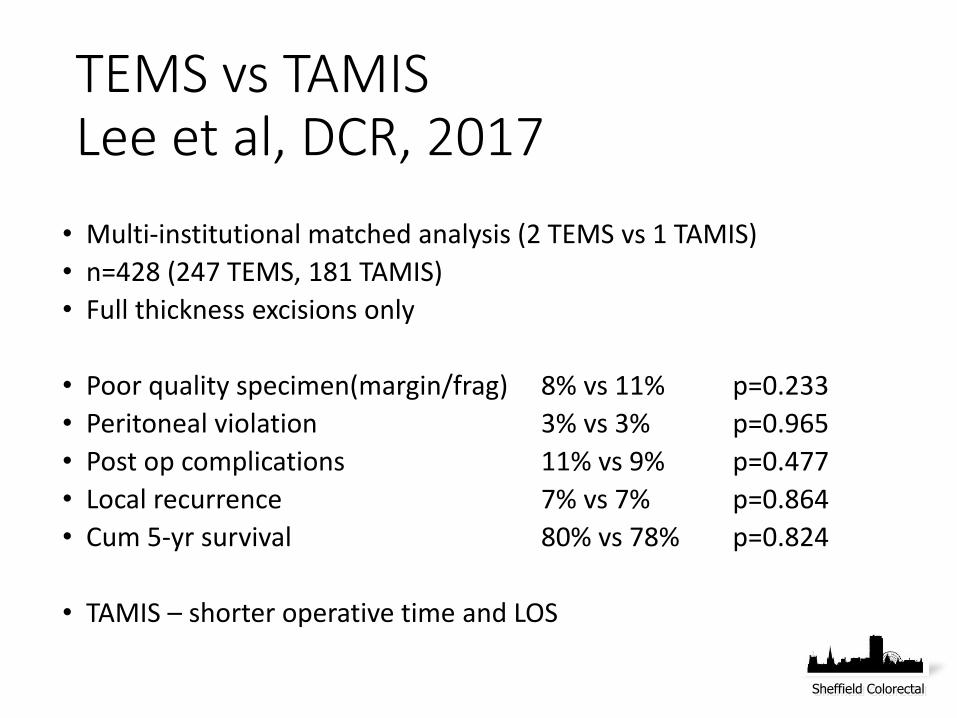
TEMS vs TAMIS Lee et al, DCR, 2017
• Multi-institutional matched analysis (2 TEMS vs 1 TAMIS)
• n=428 (247 TEMS, 181 TAMIS)
• Full thickness excisions only
• Poor quality specimen(margin/frag) 8% vs 11% p=0.233
• Peritoneal violation 3% vs 3% p=0.965
• Post op complications 11% vs 9% p=0.477
• Local recurrence 7% vs 7% p=0.864
• Cum 5-yr survival 80% vs 78% p=0.824
• TAMIS – shorter operative time and LOS
Sheffield Colorectal
Risk of residual disease
Lymph node involvement
Depth of invasion
Resection margins
Lymphovascularinvasion
Differentiation
Sheffield Colorectal
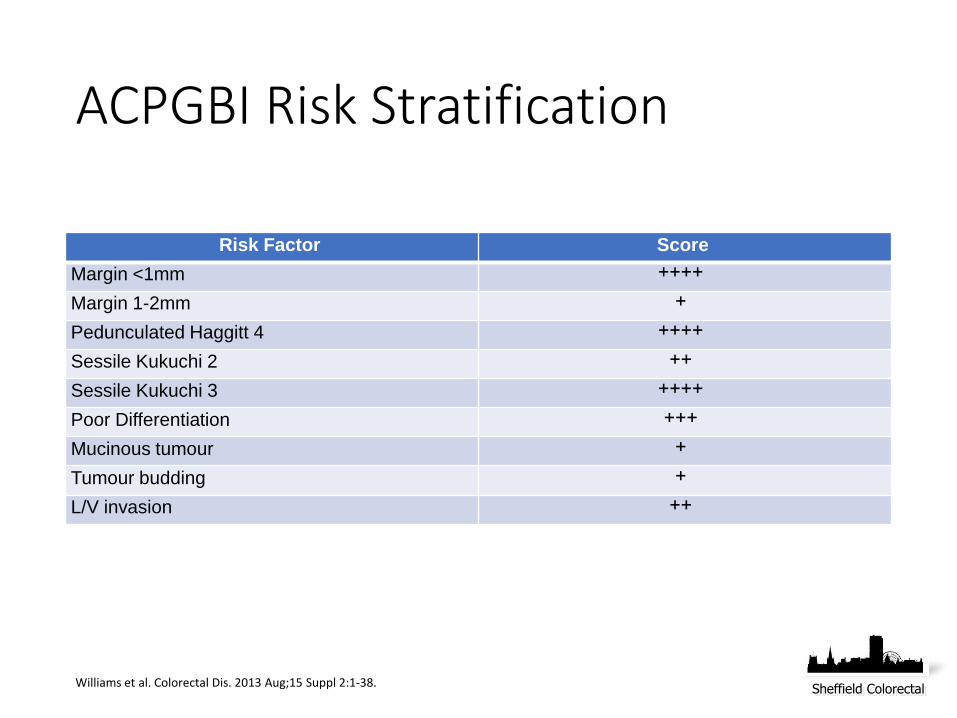
ACPGBI Risk Stratification
Risk Factor Score
Margin <1mm ++++Margin 1-2mm +Pedunculated Haggitt 4 ++++Sessile Kukuchi 2 ++Sessile Kukuchi 3 ++++Poor Differentiation +++Mucinous tumour +Tumour budding +L/V invasion ++
Williams et al. Colorectal Dis. 2013 Aug;15 Suppl 2:1-38.Sheffield Colorectal

ACPGBI Risk Stratification
Total Score GradeEstimated
RiskAction
0 Very low <3% Routine follow up
+ Low <5% Careful follow up
++ Medium 5-10% Discuss risk / benefit of surgery or follow up
+++ High 8-15% Discuss towards surgery
++++ Very high >20% Recommend surgery unless unfit
Williams et al. Colorectal Dis. 2013 Aug;15 Suppl 2:1-38.
Sheffield Colorectal
Plan
• The lesion
• The patient• Fitness, co-morbidity, preference
• The unit
Sheffield Colorectal

Sheffield Colorectal
Sheffield Colorectal
Balancing the risk of surgery
R0
Primary lesion
Nodal clearance
Morbidity
Mortality
of Surgery
Sheffield Colorectal

















![Cloacogenic Polyps: An Unrecognized Cause of Rectal Bleeding · presents with rectal bleeding and in some cases tenesmus, [2, 6] but 20% of the patients are asymptomatic [3]. We present](https://img.pdfslide.us/doc/110x75/5ec8ecb547a4c641285da058/cloacogenic-polyps-an-unrecognized-cause-of-rectal-bleeding-presents-with-rectal.jpg)











