Embed Size (px)
Citation preview
PULMONARY EMBOLISM
PRESENTERS; Evans omondi Munyaga byanjo

Outline• Epidemiology
Epidemiology
• US incidence =1 case per 1000 persons per year• 60-80% of patients with DVT, even though more than half these
patients are asymptomatic.• Death rates from P.E were 20-30% higher among men than
among women.• The incidence higher in blacks than in whites. Mortality rates for
blacks have been 50% higher than those for whites• Globally, incidence of PE = 60 to 70 per 100,000,
ETIOLOGYThree primary influences predispose a patient to thrombus formation; ( Virchow triad) which consists of the following[12, 13, 14] :
• Endothelial injury • Stasis or turbulence of blood flow • Blood hypercoagulability
• Originate primarily from deep venous system of lower extremities • Pelvic, renal, upper extremity veins or right heart chambers albeit
rarely. • Air , amniotic fluid and fat emboli are rarer causes

PATHOPHYSIOLOGY• Large thrombi lodge at the bifurcation of the main pulmonary artery or the
lobar branches and cause hemodynamic compromise. • Smaller thrombi travel more distally, occluding smaller vessels in the lung
periphery initiating an inflammatory response adjacent to the parietal pleura producing pleuritic chest pain.
• There are both respiratory and hemodynamic consequences associated with pulmonary embolism.
Respiratory consequences• Increased alveolar dead space • Hypoxemia • Hyperventilation • Regional loss of surfactant and pulmonary infarction
Hemodynamic consequences-Pulmonary embolism reduces the cross-sectional area of the pulmonary vascular bed, resulting in an increment in pulmonary vascular resistance, which, in turn, increases the right ventricular afterload. If the afterload is increased severely, right ventricular failure may ensue. -Chronic pulmonary hypertension may occur with failure of the initial embolus to undergo lyses or in the setting of recurrent thromboemboli.
Risk Factors for PE and DVT
• Immobilization• Surgery within the last 3 months• Stroke• History of venous
thromboembolism• Malignancy• Preexisting respiratory disease• Chronic Heart Disease• Age >60• Surgery requiring >30mins of
anesthesia
• Recent travel (past 2weeks, >4 hours)
• Varicose veins• Superficial vein thrombosis• Central VV
catheter/port/pacemaker
Additional RF in Women:• Obesity BMI >/=29• Heavy smoking (>25cigs/day)• Hypertension• Pregnancy
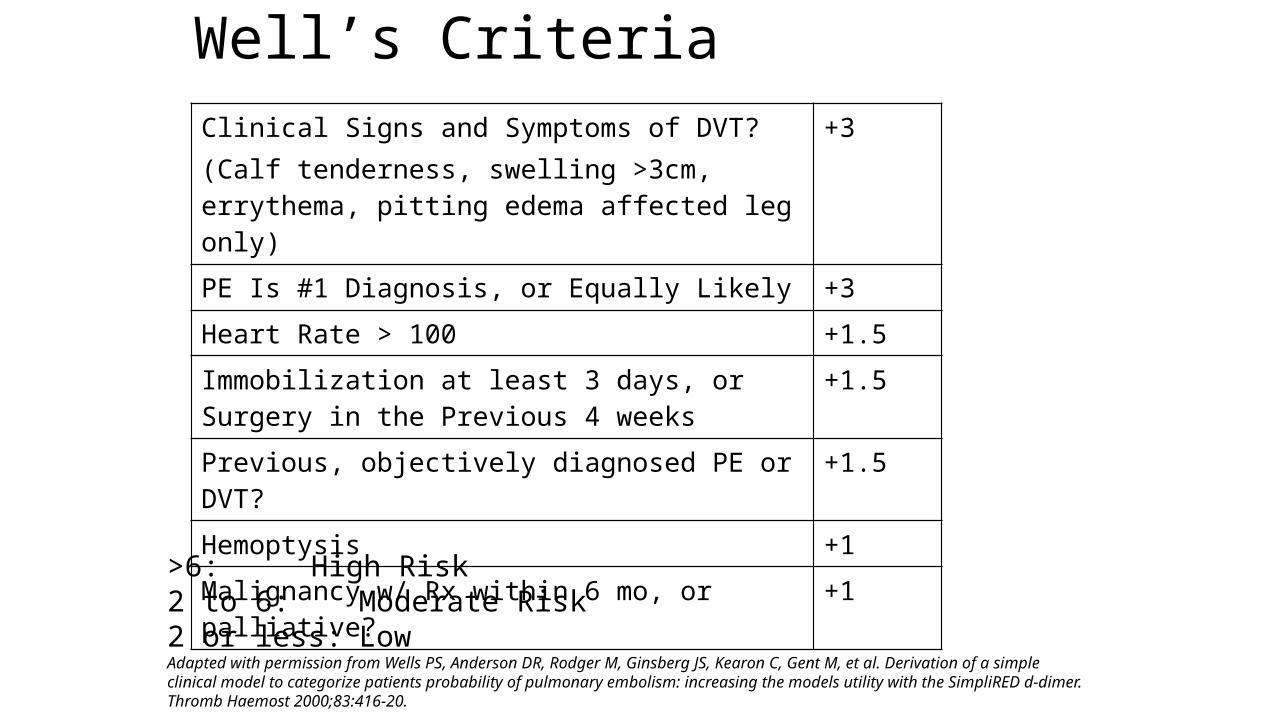
Well’s CriteriaClinical Signs and Symptoms of DVT?(Calf tenderness, swelling >3cm, errythema, pitting edema affected leg only)
+3
PE Is #1 Diagnosis, or Equally Likely +3
Heart Rate > 100 +1.5
Immobilization at least 3 days, or Surgery in the Previous 4 weeks
+1.5
Previous, objectively diagnosed PE or DVT? +1.5
Hemoptysis +1
Malignancy w/ Rx within 6 mo, or palliative? +1
>6: High Risk2 to 6: Moderate Risk2 or less: LowAdapted with permission from Wells PS, Anderson DR, Rodger M, Ginsberg JS, Kearon C, Gent M, et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED d-dimer.Thromb Haemost 2000;83:416-20.

Symptoms of P.E.• Dyspnea (73%) • Pleuritic chest pain (66%) • Cough (37%) • Hemoptysis (13%)
Signs of P.E.The incidence of physical signs has been reported as follows:• Tachypnea (respiratory rate >16/min) - 96% • Rales - 58% • Accentuated second heart sound - 53% • Tachycardia (heart rate >100/min) - 44% • Fever (temperature >37.8°C) - 43% • Diaphoresis - 36% • S 3 or S 4 gallop - 34% • Clinical signs and symptoms suggesting thrombophlebitis - 32% • Lower extremity edema - 24% • Cardiac murmur - 23% • Cyanosis - 19%
Signs in Massive P.E.• “Massive PE”: hemodynamic instability with SBP <90 or a drop in
baseline SBP by >/=40mmHg• Signs as before PLUS:
• Acute right heart failure• Elevated J.V.P.• Right-sided S3• Parasternal lift
Lab & Radiologic Findings in P.E.
• ABG• BNP• Cardiac Enzymes: Troponin• D-dimer• EKG• CXR• Ultrasound• V/Q Scan• Angiography
Lab investigations
• ABG:• Hypoxemia• Hypocapnia (low CO2)• Respiratory Alkalosis• Massive PE: hypercapnia,
mix resp and metabolic acidosis (inc lactic acid)
• Sp02 <95% -risk of rep failure
• D-dimer:• Degredation product of
fibrin• >500 is abnormal• Sensitivity: High, 95% of PE
pts will be positive• Specificity: Low• Negative Predictive Value:
Excellent

Lab Findings in P.E.(ABG)• ABG:
• Hypoxemia• Hypocapnia (low CO2)• Respiratory Alkalosis• Massive PE: hypercapnia, mix resp and metabolic acidosis (inc lactic acid)• Patients with RA pulse ox readings <95% are at increased risk of in-hospital
complications, resp failure, cardiogenic shock, death
Lab Findings in P.E. (BNP)
• BNP (beta natruretic peptide)• Insensitive test• Patient’s with PE have higher levels than pts without, but not ALL patients
with PE have high BNP• Good prognostic value measure: if BNP >90 associated with adverse clinical
outcomes (death, CPR, mechanical vent, pressure support, thrombolysis, embolectomy)
• Troponin• High in 30-50% of pts with mod to large PE

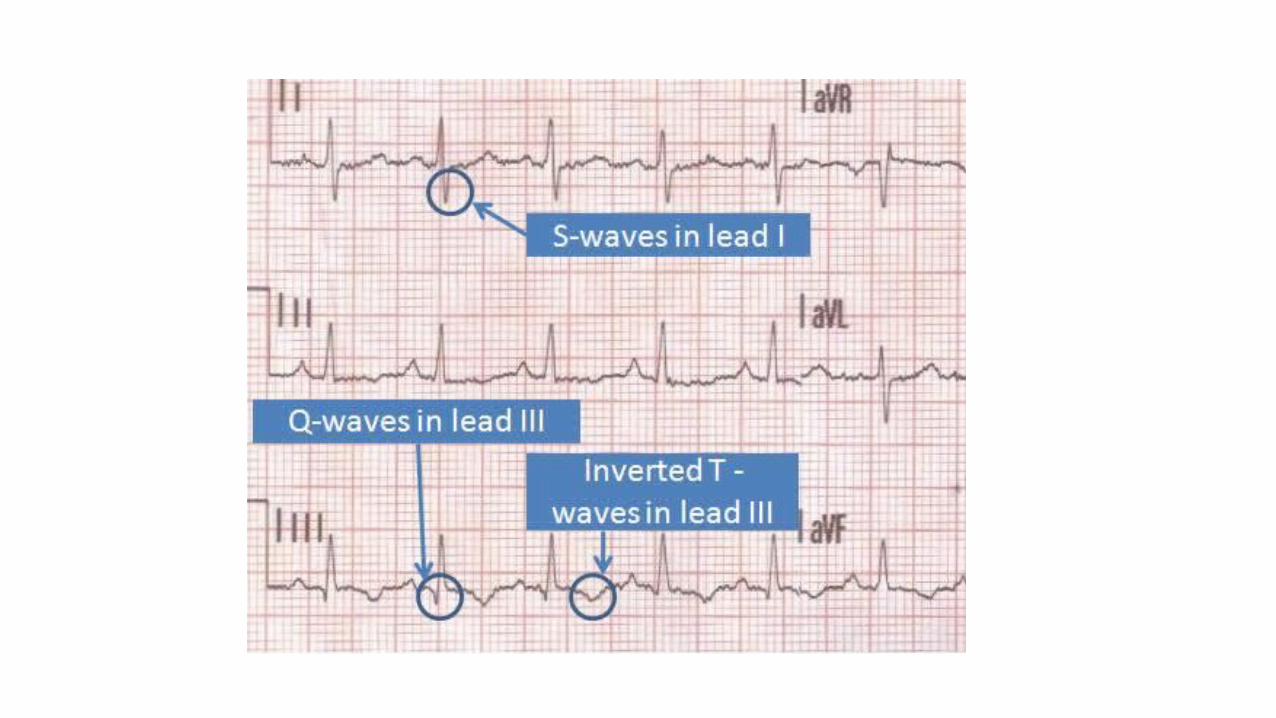
ECG• 2 Most Common finding on EKG:
• Nonspecific ST-segment and T-wave changes• Sinus Tachycardia
• Historical abnormality suggestive of PE• S1Q3T3• Right ventricular strain• New incomplete RBBB
Radiology Findings in P.E. (cont’d)
• CXR:• Normal• Atelectasis and/or pulmonary parenchymal abnormality• Pleural Effusion• Cardiomegaly• Hampton hump• Westermark’s sign

What’s This???
Hampton’s Hump
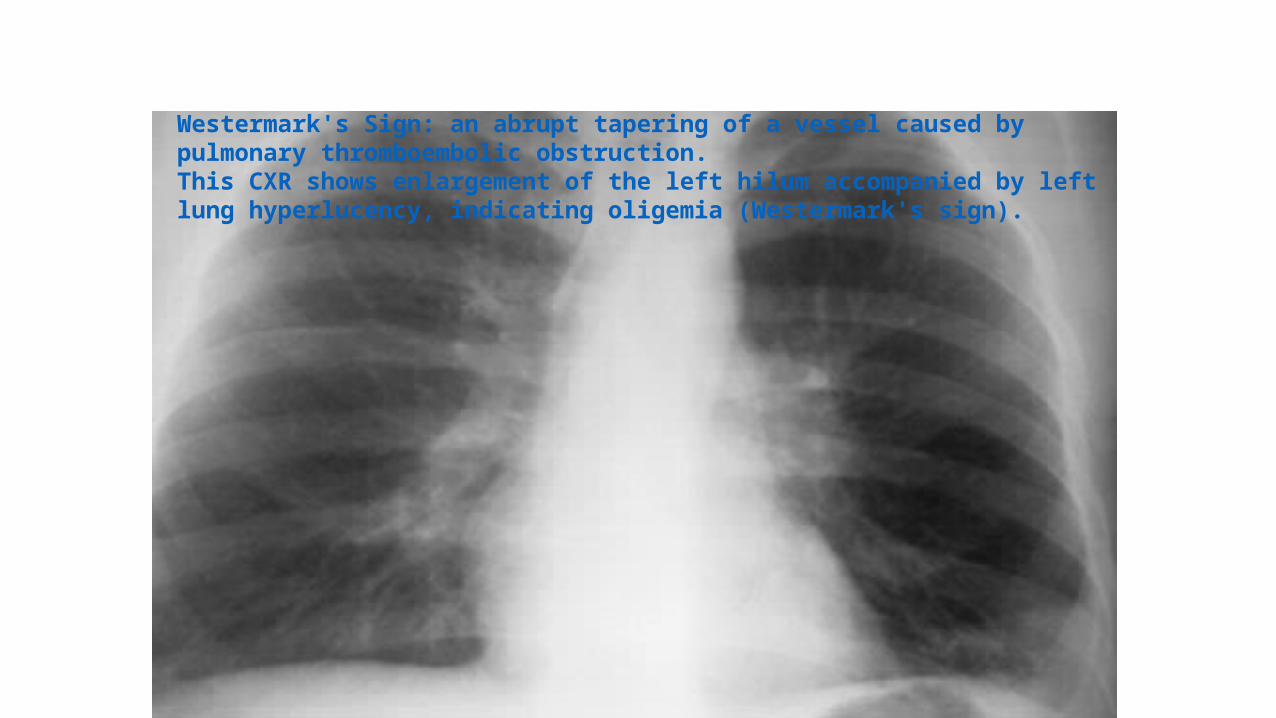
How About This???Westermark's Sign: an abrupt tapering of a vessel caused by pulmonary thromboembolic obstruction. This CXR shows enlargement of the left hilum accompanied by left lung hyperlucency, indicating oligemia (Westermark's sign).

Radiology Findings in P.E. (cont’d)
Echocardiogram• Increased Right Ventricle Size• Decreased Right Ventricular Function• Tricuspid Regurgitation
Rarely:• RV thrombus• Regional wall motion abnormalities that spare the right ventricle apex
(McConnell’s Sign)
Others
V/Q ScanLower limb U/SPulmonary Angiograms
Treatment of P.E.
• Respiratory Support: Oxygen, intubation• Hemodynamic Support: IVF, vasopressors• Anticoagulation• Thrombolysis• IVC Filter

Anticoagulation• Start during resuscitation phase itself• If suspicion high, start emperic anticoagulation • Evaluate patient for absolute contraindication
(i.e.: active bleeding)
Anticoagulation (cont’d)• HEPARIN:
• Lovenox: if hemodynamically stable, normal renal function• 1mg/kg BID OR 1.5mg/kg QDay
• Heparin gtt: if hypotension, renal failure• 80units/kg bolus then 18units/kg infusion• Goal PTT1.5 to 2.5 times the upper limit of normal
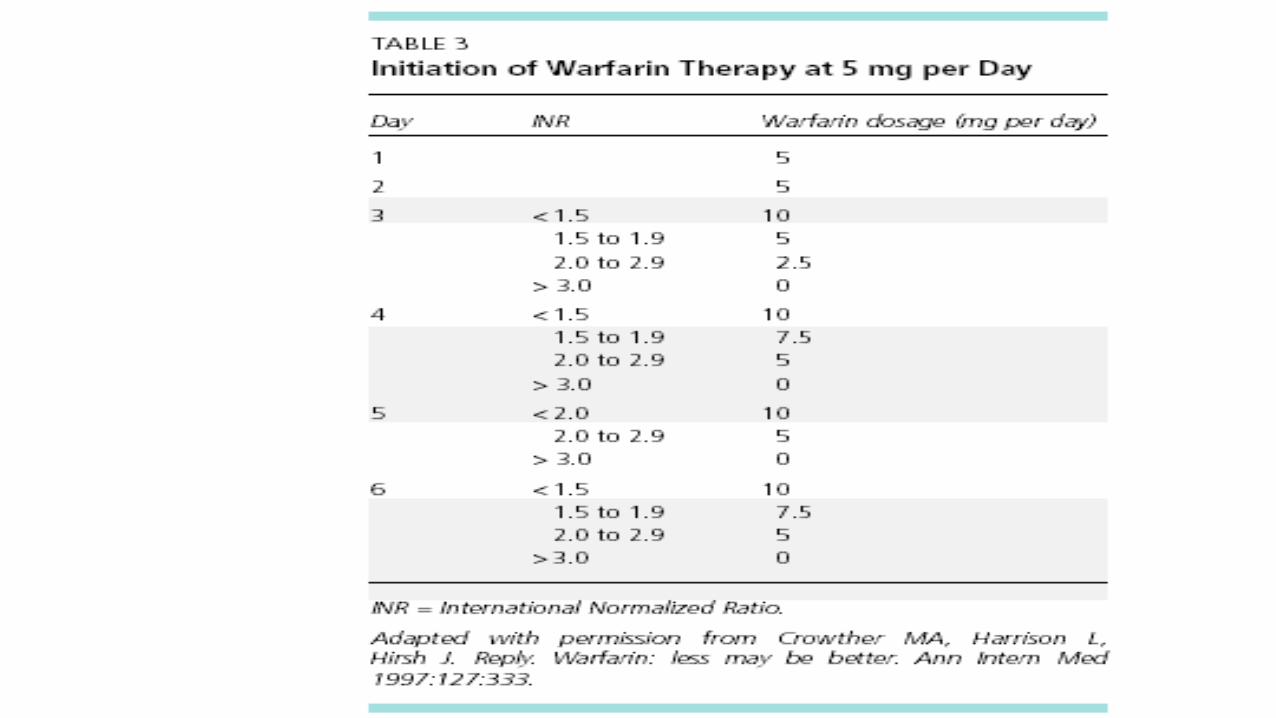
• COUMADIN:• Start once acute anticoagulation achieved• Start with 5mg PO qday OR 10mg PO q day• If start with 10mg then achieve therapeutic INR 1.4 days sooner• Complications and morbidity no different in 5mg or 10mg start • Goal INR 2 to 3
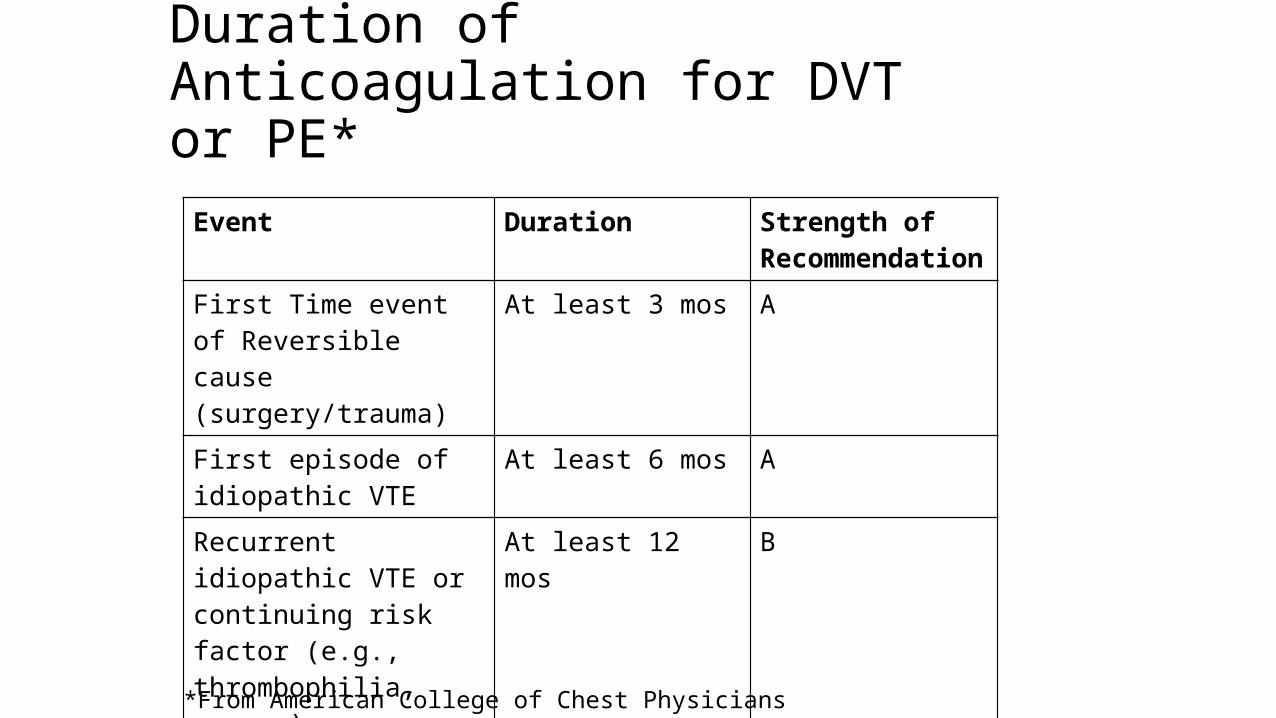
Duration of Anticoagulation for DVT or PE*
Event Duration Strength of Recommendation
First Time event of Reversible cause (surgery/trauma)
At least 3 mos A
First episode of idiopathic VTE
At least 6 mos A
Recurrent idiopathic VTE or continuing risk factor (e.g., thrombophilia, cancer)
At least 12 mos B
Symptomatic isolated calf-vein thrombosis
6 to 12 weeks A
*From American College of Chest Physicians
Thrombolysis• Considered once P.E. diagnosed• If chosen, hold anticoagulation during thrombolysis infusion, then
resumed• Associated with higher incidence of major hemorrhage • Indications: persistent hypotension, severe hypoxemia, large
perfusion defecs, right ventricular dysfunction, free floating right ventricular thrombus, paten foramen ovale
• Activase or streptokinase

IVC Filter
• Indication: • Absolute contraindication to anticoagulation (i.e.
active bleeding)• Recurrent PE during adequate anticoagulation• Complication of anticoagulation (severe bleeding)
• Also: • Pts with poor cardiopulmonary reserve• Recurrent P.E. will be fatal• Patient’s who have had embolectomy• Prophylaxis against P.E. in select patients (malignancy)
Embolectomy • Surgical or catheter• Indication:
• Those who present severe enough to warrant thrombolysis • In those where thrombolysis is contraindicated or fails
PROGNOSIS
• Depends on 2 factors: the underlying disease state and appropriate diagnosis and treatment.
• Approximately 10% of patients who develop pulmonary embolism die within the first hour, and 30% die subsequently from recurrent embolism.