Embed Size (px)
Citation preview

1PULMONARY EMBOLISM
Deep Vein Thrombosis and Pulmonary Embolism
Dr. Shatdal ChaudharySIS 12 Nov 2009

2PULMONARY EMBOLISM
DVT-PE – Epidemiology
• VTE-related deaths in the United States are estimated at 300,000 annually:– 7% diagnosed with VTE and treated,– 34% sudden fatal PE, – and 59% as undetected PE.
• In Europe- an estimated 370,000 per year PE-related deaths
• Approximately two-thirds of symptomatic VTE events are hospital acquired, and the remainder are community acquired.

3PULMONARY EMBOLISM
• DVT occurs about 3 times more often than PE.
• The major adverse outcome of DVT alone, without PE, is the development of postphlebitic syndrome.– It occurs in more than half of patients with DVT.

4PULMONARY EMBOLISM
• Genetic and acquired factors contribute to the likelihood of VTE.
• The two most common genetic factors are – the factor V Leiden – and the prothrombin gene mutations.
DVT – VTE Risk Factors

5PULMONARY EMBOLISM
DVT – VTE Risk Factors
• Acquired predispositions include– Malignancy
– Surgery
– Trauma
– Pregnancy
– Oral contraceptives or hormonal therapy
– Immobilization
– Presence of venous catheter

6PULMONARY EMBOLISM
– long-haul air travel, – obesity, – cigarette smoking, – and medical conditions such as
• antiphospholipid antibody syndrome,• Hyperviscosity• Nephrotic syndrome• Inflammatory bowel disease• systemic arterial hypertension, • chronic obstructive pulmonary disease, CCF• Thrombophilia contributes to the risk of venous thrombosis,
often due to an inherited risk factor in combination with an acquired predisposition.

7PULMONARY EMBOLISM
• About half of patients with pelvic vein thrombosis or proximal leg DVT develop PE
• Isolated calf vein thrombi pose a much lower risk of PE.

8PULMONARY EMBOLISM
Physiology• The most common gas exchange abnormalities are
hypoxemia and an increased alveolar-arterial O2 tension gradient.
• Anatomic and Physiologic dead space • Other pathophysiological abnormalities include:
– Increased pulmonary vascular resistance – Impaired gas exchange due to increased alveolar dead space
from vascular obstruction, – Alveolar hyperventilation due to reflex stimulation of irritant
receptors– Increased airway resistance due to constriction of airways distal
to the bronchi– Decreased pulmonary compliance due to lung edema, lung
hemorrhage, or loss of surfactant

9PULMONARY EMBOLISM
PULMONARY EMBOLISM
What are the SYMPTOMS and SIGNS of Pulmonary embolism?

10PULMONARY EMBOLISM
PULMONARY EMBOLISM SYMPTOMS
• Chest Pain
- pleuritic
-non pleuritic
• Dyspnea

11PULMONARY EMBOLISM
PULMONARY EMBOLISM SYMPTOMS
• Apprehension
• Cough
• Hemoptysis
• Leg pain and Cramps in calf
• Syncope

12PULMONARY EMBOLISM
PULMONARY EMBOLISM SIGNS
• Tachypnea • Crackles • Tachycardia • Fever• Increased “P2”• Phlebitis

13PULMONARY EMBOLISM
Differential Diagnosis• DVT
– Ruptured Baker's cyst
– Cellulitis
– Postphlebitic syndrome/venous insufficiency
• PE – Pneumonia, asthma, chronic obstructive pulmonary disease
– Congestive heart failure Pericarditis Pleurisy: "viral syndrome,"
– costochondritis, musculoskeletal discomfort Rib fracture,
– pneumothorax Acute coronary syndrome Anxiety

14PULMONARY EMBOLISM
Nonimaging Diagnostic Modalities
Blood Tests: D-dimer• The quantitative plasma D-dimer ELISA rises in the
presence of DVT or PE• The sensitivity is greater than 80% for DVT and
greater than 95% for PE. • The D-dimer is a useful "rule out" test. • The D-dimer assay is not specific.• Levels increase in patients with myocardial infarction,
pneumonia, sepsis, cancer, the postoperative state, and second or third trimester of pregnancy.

ECG FINDINGS• Sinus Tachycardia • “T” wave inversion V1-V4• ST segment depression • Low voltage • S1 Q3 T3 • ST elevation • R Bundle Branch Block

16PULMONARY EMBOLISM
Noninvasive Imaging Modalities
• Venous Ultrasonography – loss of vein compressibility– direct visualization of thrombus

17PULMONARY EMBOLISM
X-RAY FINDINGS
A normal or near-normal chest x-ray in a dyspneic
patient often occurs in PE.
• Focal oligemia (Westermark's sign)
• A peripheral wedged-shaped density above the
diaphragm (Hampton's hump),
• An enlarged right descending pulmonary artery
(Palla's sign).

18PULMONARY EMBOLISM
P.E. atelectasis

19PULMONARY EMBOLISM
P.E. effusion

20PULMONARY EMBOLISM
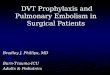
P.E. Hampton’s Hump

21PULMONARY EMBOLISM
P.E. subsegmental defect

22PULMONARY EMBOLISM
Chest CT
• Multidetector-row spiral CT of the chest with intravenous contrast is the principal imaging test for the diagnosis of PE.

23PULMONARY EMBOLISM
Pulm. Embolism CT
J. Galvin, M.D. J.Choi, B.S. The Diagnosis of P. E. Virtual Hospital:http://www.vh.org/Providers

24PULMONARY EMBOLISM
Lung Scanning
• Lung scanning is now a second-line diagnostic test for PE.– Small particulate aggregates of albumin labeled with a gamma-
emitting radionuclide are injected intravenously and are trapped in the pulmonary capillary bed.
– The perfusion scan defect indicates absent or decreased blood flow, possibly due to PE.
– Ventilation scans, obtained with radiolabeled inhaled gases such as xenon or krypton, improve the specificity of the perfusion scan.

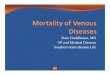
25PULMONARY EMBOLISM
High Probability V/Q Scan
J. Galvin, M.D. J.Choi, B.S. The Diagnosis of P. E. Virtual Hospital:http://www.vh.org/Providers

26PULMONARY EMBOLISM
MRI Contrast-Enhanced
• When ultrasound is equivocal, MR venography is an excellent imaging modality to diagnose DVT.
• MR imaging should be considered for suspected DVT or PE patients with renal insufficiency or contrast dye allergy.
• MR pulmonary angiography detects large proximal PE but is not reliable for smaller segmental and subsegmental PE.
Echocardiography• Echocardiography is not a reliable

27PULMONARY EMBOLISM
Invasive Diagnostic Modalities
Pulmonary Angiography– Chest CT with contrast has virtually replaced
invasive pulmonary angiography as a diagnostic test.
– visualization of an intraluminal filling defect– abrupt occlusion ("cut-off") of vessels, segmental
oligemia or avascularity
Contrast Phlebography– Venous ultrasonography has virtually replaced

28PULMONARY EMBOLISM
DIAGNOSIS
Based on:
• Relevant SYMPTOMS & SIGNS
• Associated RISK FACTORS
• Probability of ALTERNATIVE Diagnosis
• OBJECTIVE Confirmation

29PULMONARY EMBOLISM
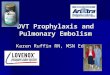
Low Clinical Likelihood of DVT If the Point Score Is Zero or Less• Clinical Variable Score• Active cancer 1• Paralysis, paresis, or recent cast 1• Bedridden for >3 days; major surgery <12 weeks 1• Tenderness along distribution of deep veins 1• Entire leg swelling 1• Unilateral calf swelling >3 cm 1• Pitting edema 1• Collateral superficial nonvaricose veins 1• Alternative diagnosis at least as likely as DVT –2
High Clinical Likelihood of PE if the Point Score Exceeds 4• Clinical Variable Score• Signs and symptoms of DVT 3.0• Alternative diagnosis less likely than PE 3.0• Heart rate >100/min 1.5• Immobilization >3 days; surgery within 4 weeks 1.5• Prior PE or DVT 1.5• Hemoptysis 1.0• Cancer 1.0

30PULMONARY EMBOLISM
Wells Score

31PULMONARY EMBOLISM
DVT-PE: Treatment
• Primary therapy – clot dissolution with thrombolysis – or removal of PE by embolectomy.
• Secondary prevention – Anticoagulation with heparin and warfarin – or placement of an inferior vena caval filter
constitutes

32PULMONARY EMBOLISM
Anticoagulation• Immediately effective anticoagulation is initiated with a
parenteral drug: unfractionated heparin, low molecular weight heparin (LMWH), or fondaparinux.
• These parenteral drugs are continued as a transition or "bridge" to stable, long-term anticoagulation with a vitamin K antagonist
• The first dose of warfarin may be given as soon as several hours after the bridging anticoagulant if LMWH or fondaparinux are used. Otherwise, with UFH a therapeutic aPTT must first be documented.
• Warfarin requires 5–7 days to achieve a therapeutic effect.• Continue parenteral anticoagulation for a minimum of 5 days
and until 2 sequential INR values, at least 1 day apart, return in the target range.

33PULMONARY EMBOLISM
Unfractionated Heparin
• anticoagulates by binding to and accelerating the activity of antithrombin III
• preventing additional thrombus formation and permitting endogenous fibrinolytic mechanisms to lyse clot that has already formed.
• intravenous bolus is 5000–10,000 units(80 units/kg) followed by a continuous infusion of 1000–1500 units/h (18 units/kg per hour).

34PULMONARY EMBOLISM
Low Molecular Weight Heparins
• Enoxaparin 1 mg/kg twice daily
• Tinzaparin 175 units/kg once daily

35PULMONARY EMBOLISM
Fondaparinux
• an anti-Xa pentasaccharide
• is administered by once-daily subcutaneous injection
• Patients weighing – <50 kg receive 5 mg, – 50–100 kg patients receive 7.5 mg, – >100 kg receive 10 mg.

36PULMONARY EMBOLISM
Warfarin
• vitamin K antagonist • prevents carboxylation activation of coagulation
factors II, VII, IX, and X. • In an average-sized adult, warfarin is usually initiated
in a dose of 5 mg. Doses of 7.5 or 10 mg can be used
• The warfarin dose is titrated to achieve the target INR • The target INR is usually 2.5, with a range of 2.0–3.0.

37PULMONARY EMBOLISM
Complications of Anticoagulants
• Hemorrhage
• Heparin-induced thrombocytopenia
• Osteopenia
• Alopecia (warfarin).
• Warfarin-induced skin necrosis
• During pregnancy, warfarin should be avoided

38PULMONARY EMBOLISM
Duration of Anticoagulation
• Patients with PE following surgery or trauma ordinarily have a low rate of recurrence after 3–6 months of anticoagulation.
• For DVT isolated to an upper extremity or calf that has been provoked by surgery or trauma, 3 months of anticoagulation suffices.
• For provoked proximal leg DVT or PE, 6 months of anticoagulation is sufficient.
• In patients with "idiopathic," unprovoked DVT or PE : anticoagulation for an indefinite duration with a target INR between 2.0 and 3.0

39PULMONARY EMBOLISM
Inferior Vena Caval (IVC) Filters
• active bleeding that precludes anticoagulation,
• recurrent venous thrombosis despite intensive anticoagulation.

40PULMONARY EMBOLISM
Prevention of VTE
• Early mobilization• Graduated compression stockings • pneumatic compression devices • mini-dose unfractionated heparin (5000
units subcutaneously twice or preferably three times daily),
• Low molecular weight heparin,• fondaparinux 2.5 mg daily