Embed Size (px)
Citation preview

Pulmonary Board Review

[1] A 46 y/o woman with persistent asthma is evaluated in clinic for scheduled follow-up visit. Since her most recent visit 6 months ago, her disease has been stable on a regimen of high-dose inhaled corticosteroids plus a long-acting B-agonist and as-needed albuterol, which she uses approximately once every 1 to 2 weeks. The patient is pleased with the current therapy, and the as-needed albuterol is continued.
Which of the following would be the best approach to this patient’s therapy?
A. Continue inhaled corticosteroids and the long-acting B-agonist at current doses.
B. Discontinue inhaled corticosteroids and the long-acting B-agonistC. Continue the long-acting B-agonist and reduce the dose on inhaled
corticosteroids.D. Discontinue the long-acting B-agonist and reduce the dose of inhaled
corticosteroids.

[1] A 46 y/o woman with persistent asthma is evaluated in clinic for scheduled follow-up visit. Since her most recent visit 6 months ago, her disease has been stable on a regimen of high-dose inhaled corticosteroids plus a long-acting B-agonist and as-needed albuterol, which she uses approximately once every 1 to 2 weeks. The patient is pleased with the current therapy, and the as-needed albuterol is continued.
Which of the following would be the best approach to this patient’s therapy?
A. Continue inhaled corticosteroids and the long-acting B-agonist at current doses.
B. Discontinue inhaled corticosteroids and the long-acting B-agonistC. Continue the long-acting B-agonist and reduce the dose on inhaled
corticosteroids.D. Discontinue the long-acting B-agonist and reduce the dose of inhaled
corticosteroids.

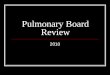
Classification of Asthma Severity: Clinical Features Before Treatment
Days With Nights With PEF or PEF
Symptoms Symptoms FEV1 Variability
Step 4 Continuous Frequent 60% 30%SeverePersistentStep 3 Daily 5/month 60%-<80% 30%ModeratePersistentStep 2 3-6/week 3-4/month 80% 20-30%MildPersistentStep 1 2/week 2/month 80% 20%MildIntermittent
Footnote: The patient’s step is determined by the most severe feature.

Stepwise Approach to Stepwise Approach to Therapy: Gaining ControlTherapy: Gaining Control
STEP 4STEP 4Severe PersistentSevere Persistent
STEP 3STEP 3Moderate Moderate PersistentPersistent
STEP 2STEP 2Mild PersistentMild Persistent
STEP 1STEP 1Mild IntermittentMild Intermittent
11 22
1. Start high and 1. Start high and step down. step down.
2. Start at initial2. Start at initiallevel of severity; level of severity;
gradually gradually step up.step up.

Stepwise Approach to Therapy for Stepwise Approach to Therapy for Adults and Children >Age 5: Adults and Children >Age 5:
Maintaining ControlMaintaining Control Step down if Step down if
possiblepossible Step up if Step up if
necessarynecessary Patient Patient
education and education and environmental environmental control at every control at every stepstep
Recommend Recommend referral to referral to specialist atspecialist atStep 4; consider Step 4; consider referral at Step 3referral at Step 3
STEP 4STEP 4Multiple long-term-Multiple long-term-
control medications, control medications, includeinclude
oral corticosteroidsoral corticosteroidsSTEP 3STEP 3 >> 1 Long-term-control 1 Long-term-control medicationsmedications
STEP 2STEP 21 Long-term-control 1 Long-term-control
medication: anti-inflammatorymedication: anti-inflammatory
STEP 1STEP 1
Quick-relief medication: PRNQuick-relief medication: PRN

[11] A 75-year-old woman with a long-standing history of asthma is evaluated for increased nocturnal asthma symptoms and frequent need to use an albuterol inhaler. Her treatment regimen now consists of daily moderate-dose inhaled corticosteroids. On physical examined she has occasional wheezing; the examination is otherwise unremarkable. Office spirometry shows an forced expiratory volume in 1 second (FEV1) of 2.2 (75% of predicted).
Which of the following is the most appropriate adjustment to this patient’s asthma therapy?
A. Doubling the inhaled corticosteroid doseB. Adding theophyllineC. Adding a leukotriene receptor antagonistD. Adding a long-acting b-agonistE. Adding anti-IgE antibody

[11] A 75-year-old woman with a long-standing history of asthma is evaluated for increased nocturnal asthma symptoms and frequent need to use an albuterol inhaler. Her treatment regimen now consists of daily moderate-dose inhaled corticosteroids. On physical examined she has occasional wheezing; the examination is otherwise unremarkable. Office spirometry shows an forced expiratory volume in 1 second (FEV1) of 2.2 (75% of predicted).
Which of the following is the most appropriate adjustment to this patient’s asthma therapy?
A. Doubling the inhaled corticosteroid doseB. Adding theophyllineC. Adding a leukotriene receptor antagonistD. Adding a long-acting b-agonistE. Adding anti-IgE antibody

[21] A 20-year old woman is evaluated in the emergency department for an acute exacerbation of asthma. The patient has a history of frequent visits to the emergency department and urgent care for asthma exacerbations. Between exacerbations she has normal pulmonary function.
On physical examination, she has inspiratory and expiratory wheezing and is in moderate discomfort. Oxygen saturation is 95% with the patient breathing room air. She is treated with methylprednisolone, 125mg intravenously, and given three treatments with nebulized albuterol/ipratropium. Two hours later, she is still wheezing, anxious, and appears to be in moderate respiratory distress. Oxygen saturation on room air is 96%; pulse rate is 100/min and respiration rate 24/min. Chest radiograph shows low lung volumes.
Which of the following is the most appropriate management for this patient?
A. Intravenous aminophyllineB. LaryngoscopyC. Intravenous terbutalineD. Cetriaxone/azithromycinE. Chest CT scan

[21] A 20-year old woman is evaluated in the emergency department for an acute exacerbation of asthma. The patient has a history of frequent visits to the emergency department and urgent care for asthma exacerbations. Between exacerbations she has normal pulmonary function.
On physical examination, she has inspiratory and expiratory wheezing and is in moderate discomfort. Oxygen saturation is 95% with the patient breathing room air. She is treated with methylprednisolone, 125mg intravenously, and given three treatments with nebulized albuterol/ipratropium. Two hours later, she is still wheezing, anxious, and appears to be in moderate respiratory distress. Oxygen saturation on room air is 96%; pulse rate is 100/min and respiration rate 24/min. Chest radiograph shows low lung volumes.
Which of the following is the most appropriate management for this patient?
A. Intravenous aminophyllineB. LaryngoscopyC. Intravenous terbutalineD. Cetriaxone/azithromycinE. Chest CT scan


PULMONARY FUNCTION TESTING
Spirometry

Upper Airway Obstruction
FIXED
•Thyroid tumors/goiters
•Tracheal stenosis (intubation)
VARIABLE
Extrathoracic
•Vocal cord dyskinesia
•Vocal cord paralysis
•Subglottic stenosis
•Tracheomalacia
Intrathoracic
•Tracheomalacia

PULMONARY FUNCTION TESTING Spirometry
FVC within 95% CI?Yes No
FEV1/ FVC within 95% CI?
FEV1/ FVC within 95% CI?
Yes
Normal
No
Obstructive
Yes
Restrictive
No
Mixed

Lung Volumes - Review4 Lung Volumes• Tidal volume• Inspiratory Reserve
Volume• Expiratory Reserve
Volume• Residual Volume4 Lung Capacities• Total Lung Capacity• Vital Capacity• Functional Residual
Capacity• Inspiratory Capacity


[37] A 38-year old woman is evaluated for worsening control of mild-persistent asthma. Her disease had been under good control on therapy with moderate-dose inhaled corticosteroids plus as-needed albuterol until 6 weeks ago when she had an acute respiratory tract infection. Since then she has had significant worsening of her symptoms, with nightly cough and wheezing and use of albuterol rescue inhaler six to eight times per day.
Which of the following is the most appropriate therapy for this patient?
A. A 7-day course of a fluoroquinolone antibioticB. Nebulized albuterol/ipratropium bromide at homeC. A short course of oral corticosteroid therapyD. A leukotriene receptor antagonist

[37] A 38-year old woman is evaluated for worsening control of mild-persist asthma. Her disease had been under good control on therapy with moderate-dose inhaled corticosteroids plus as-needed albuterol until 6 weeks ago when she had an acute respiratory tract infection. Since then she has had significant worsening of her symptoms, with nightly cough and wheezing and use of albuterol rescue inhaler six to eight times per day.
Which of the following is the most appropriate therapy for this patient?
A. A 7-day course of a fluoroquinolone antibioticB. Nebulized albuterol/ipratropium bromide at homeC. A short course of oral corticosteroid therapyD. A leukotriene receptor antagonist

[39] A 28 year old man is evaluated for a 6-month history of episodic dyspnea, cough, and wheezing. As a child, he had asthma, but he has been asymptomatic since his early teens. His recent symptoms, which began after an upper respiratory tract infection, are often triggered by exercise or exposure to cold air and awaken him from sleep three to four times per month.On physical examination, vital signs are normal. There is scattered wheezing in both lung fields. Office spirometry shows a forced expiratory volume in 2 second (FEV1) of 75% of predicted with a 15% improvement (370mL) after inhaled albuterol. Chest radiograph is normal.
Which of the following is the most appropriate therapy for this patient?A. Albuterol by metered dose inhaler as-neededB. Long-acting B-agonist plus as-needed albuterolC. Long-acting B-agonistD. Inhaled corticosteroids plus as-needed albuterolE. Long-term antibiotic therapy

[39] A 28 year old man is evaluated for a 6-month history of episodic dyspnea, cough, and wheezing. As a child, he had asthma, but he has been asymptomatic since his early teens. His recent symptoms, which began after an upper respiratory tract infection, are often triggered by exercise or exposure to cold air and awaken him from sleep three to four times per month.On physical examination, vital signs are normal. There is scattered wheezing in both lung fields. Office spirometry shows a forced expiratory volume in 2 second (FEV1) of 75% of predicted with a 15% improvement (370mL) after inhaled albuterol. Chest radiograph is normal.
Which of the following is the most appropriate therapy for this patient?A. Albuterol by metered dose inhaler as-neededB. Long-acting B-agonist plus as-needed albuterolC. Long-acting B-agonistD. Inhaled corticosteroids plus as-needed albuterolE. Long-term antibiotic therapy



[55] A 45 year-old woman with long-standing severe asthma is evaluated for new-onset fevers, fatigue, skin rash and increased respiratory symptoms. The patient typically uses an albuterol inhaler three to five times per day and wakes up at night with asthma symptoms two or three times per week despite taking high-dose inhaled corticosteroids, a long-acting b-agonist, and for the past years, prednisone 15 to 20 mg/day. Four weeks ago she began taking a leukotriene receptor antagonist and tapering off prednisone.Chest radiograph shows bilateral patchy infiltrates. Leukocyte count is 15,000/uL with 25% eosinophils.
Which of the following is the most appropriate next step in the management of this patient?
A. Increasing the dose of the leukotriene receptor antagonistB. Doubling the dose of the inhaled corticosteroidC. Starting antibiotic therapyD. Stopping the leukotriene receptor antagonist and restarting
prednisoneE. Referring for open lung biopsy

[55] A 45 year-old woman with long-standing severe asthma is evaluated for new-onset fevers, fatigue, skin rash and increased respiratory symptoms. The patient typically uses an albuterol inhaler three to five times per day and wakes up at night with asthma symptoms two or three times per week despite taking high-dose inhaled corticosteroids, a long-acting b-agonist, and for the past years, prednisone 15 to 20 mg/day. Four weeks ago she began taking a leukotriene receptor antagonist and taper off prednisone.Chest radiograph shows bilateral patchy infiltrates. Leukocyte count is 15,000/uL with 25% eosinophils.
Which of the following is the most appropriate next step in the management of this patient?
A. Increasing the dose of the leukotriene receptor antagonist.B. Doubling the dose of the inhaled corticosteroid.C. Starting antibiotic therapyD. Stopping the leukotriene receptor antagonist and restarting
prednisoneE. Referring for open lung biopsy

[57] An 18-year-old male high school football player is evaluated for recurrent episodes of dyspnea, chest tightness, and cough that have occurred during a game and limited his ability to participate. The symptoms resolve spontaneously in 20-30 minutes. The patient’s father has known allergies but no known lung disease.On physical examination, the patient is a healthy young man; the lungs are clear on auscultation. Office spirometry shows an FEV1 of 90% predicted and FEV1/FVC 80%.
Which of the following is the most appropriate next step in the evaluation of this patient?
A. Measure lung volumes and diffusion capacityB. Perform an exercise challenge testC. Perform allergy skin testingD. Prescribe a physical conditioning program

[57] An 18-year-old male high school football player is evaluated for recurrent episodes of dyspnea, chest tightness, and cough that have occurred during a game and limited his ability to participate. The symptoms resolve spontaneously in 20-30 minutes. The patient’s father has known allergies but no known lung disease.On physical examination, the patient is a healthy young man; the lungs are clear on auscultation. Office spirometry shows an FEV1 of 90% predicted and FEV1/FVC 80%.
Which of the following is the most appropriate next step in the evaluation of this patient?
A. Measure lung volumes and diffusion capacityB. Perform an exercise challenge testC. Perform allergy skin testingD. Prescribe a physical conditioning program


A 23-year-old woman with a long history of asthma, non-adherence to medical therapy, and previous exacerbations requiring intubations is evaluated in the emergency department for a 2-day history of increasing wheezing and dyspnea after the onset of a sore throat. She has a cough productive of small amounts of whitish mucous with some plugs. She has no fever or chills and says that she has used her albuterol inhaler many times in the past day. She had been taking montelukast daily but had not been using other inhalers because she previously felt well. On physical exam she is in severe respiratory distress; BP 160/80, HR 140/min, RR 36/min, and she is using accessory muscles for breathing. She has nasal flaring, and chest examination reveals diffuse inspiratory and expiratory wheezes. PEFR: 110 L/min. WBC: 16,5000/ul. ABG 7.32/44/76 on 5L o2. CXR shows hyperinflation but is otherwise clear. Intravenous corticosteroid therapy is begun.
Which of the following is the most appropriate next step in this patient’s
management?A. Prompt intubationB. Noninvasive positive pressure ventilationC. Helium combined with oxygen (Heliox) with bronchodilator aerosolD. Bronchodilators via aerosol consisting of a short-acting B-agonist and an
anticholinergic agentE. Intravenous or inhaled magnesium sulfate

A 23-year-old woman with a long history of asthma, non-adherence to medical therapy, and previous exacerbations requiring intubations is evaluated in the emergency department for a 2-day history of increasing wheezing and dyspnea after the onset of a sore throat. She has a cough productive of small amounts of whitish mucous with some plugs. She has no fever or chills and says that she has used her albuterol inhaler many times in the past day. She had been taking montelukast daily but had not been using other inhalers because she previously felt well. On physical exam she is in severe respiratory distress; BP 160/80, HR 140/min, RR 36/min, and she is using accessory muscles for breathing. She has nasal flaring, and chest examination reveals diffuse inspiratory and expiratory wheezes. PEFR: 110 L/min. WBC: 16,5000/ul. ABG 7.32/44/76 on 5L o2. CXR shows hyperinflation but is otherwise clear. Intravenous corticosteroid therapy is begun.
Which of the following is the most appropriate next step in this patient’s
management?A. Prompt intubationB. Noninvasive positive pressure ventilationC. Helium combined with oxygen (Heliox) with bronchodilator aerosolD. Bronchodilators via aerosol consisting of a short-acting B-agonist and an
anticholinergic agentE. Intravenous or inhaled magnesium sulfate


A 19-year-old woman is evaluated for possible asthma. She has known seasonal allergies manifesting as hay fever in fall and spring. Symptoms are restricted to nose/eyes, and she has no history of wheezing or chest tightness. The patient had a methacholine test, as part of a research study, which showed borderline response.
Which of the following would be most appropriate management for this patient?
A. Inhaled corticosteroids and a long-acting B-agonistB. Seasonal nasal corticosteroids and antihistamineC. Albuterol inhaler as neededD. Repeat methacholine challenge

A 19-year-old woman is evaluated for possible asthma. She has known seasonal allergies manifesting as hay fever in fall and spring. Symptoms are restricted to nose/eyes, and she has no history of wheezing or chest tightness. The patient had a methacholine test, as part of a research study, which showed borderline response.
Which of the following would be most appropriate management for this patient?
A. Inhaled corticosteroids and a long-acting B-agonistB. Seasonal nasal corticosteroids and antihistamineC. Albuterol inhaler as neededD. Repeat methacholine challenge

[91] A 75 year old woman with long-standing asthma is evaluated for palpitation, nausea, and vomiting of 3 days duration. Her asthma treatment regimen includes low-dose inhaled corticosteroids, albuterol as needed, and theophylline; her most recent theophylline level was 9 ug/mL. While out of state 1 week ago, she developed fever, cough, and sore throat. She was evaluated at a walk-in clinic, and the diagnosis of acute bronchitis was made; therapy with ciprofloxacin was started. A few days later, her respiratory symptoms had resolved, but soon afterward her current sxs developed.
Which of the following is the most appropriate management of this patient?
A. Continue current treatmentB. Check serum theophylline levelC. Prescribe for nausea/vomtingD. Check serum amylase/lipase

[91] A 75 year old woman with long-standing asthma is evaluated for palpitation, nausea, and vomiting of 3 days duration. Her asthma treatment regimen includes low-dose inhaled corticosteroids, albuterol as needed, and theophylline; her most recent theophylline level was 9 ug/mL. While out of state 1 week ago, she developed fever, cough, and sore throat. She was evaluated at a walk-in clinic, and the diagnosis of acute bronchitis was made; therapy with ciprofloxacin was started. A few days later, her respiratory symptoms had resolved, but soon afterward her current sxs developed.
Which of the following is the most appropriate management of this patient?
A. Continue current treatmentB. Check serum theophylline levelC. Prescribe for nausea/vomtingD. Check serum amylase/lipase

Theophylline
Increased Levels– Ciprofloxacin– Cimetidine– Erythromycin– Allopurinol– Zileuton– Elderly patients
Decreased levels– Rifampin– Phenobarbitol– Ethanol
•Metabolized in liver
•Narrow Window: “therapeutic” 8 to 12 ug/dL
•Toxicity: tremor, palpitations, nausea, vomiting, arrhythmias, seizures, death

[110] A 45-year-old woman is evaluated in the emergency department for asthma exacerbation. She developed an upper respiratory tract infection 4 days ago, and 2 days later she noted increased cough, sputum production, wheezing and chest tightness. She has used her albuterol inhaler many times over the past 2 days with limited benefit. On PE, she is alert but anxious; T37C, BP 140/85, HR 115/min, RR 32/min. O2 sats 93% on low flow oxygen. Examination shows reduced breath sounds over both lung fields with prolonged expiration and minimal wheezing. Spirometry revealed a FEV1 0.96L/31% predicted. After getting nebulized albuterol/atrovent, minimal improvement is noted. Repeat exam shows T 37C, HR130, RR 24. and lungs show decreased air entry and minimal wheezing; spirometry shows an FEV1 1.05L/34%. CXR is hyper-inflated.
Which of the following is the most appropriate next step in the evaluation of this patient?
A. Peak expiratory flowB. ElectrocardiographyC. Measurement of arterial blood gasesD. Complete blood count

[110] A 45-year-old woman is evaluated in the emergency department for asthma exacerbation. She developed an upper respiratory tract infection 4 days ago, and 2 days later she noted increased cough, sputum production, wheezing and chest tightness. She has used her albuterol inhaler many times over the past 2 days with limited benefit. On PE, she is alert but anxious; T37C, BP 140/85, HR 115/min, RR 32/min. O2 sats 93% on low flow oxygen. Examination shows reduced breath sounds over both lung fields with prolonged expiration and minimal wheezing. Spirometry revealed a FEV1 0.96L/31% predicted. After getting nebulized albuterol/atrovent, minimal improvement is noted. Repeat exam shows T 37C, HR130, RR 24. and lungs show decreased air entry and minimal wheezing; spirometry shows an FEV1 1.05L/34%. CXR is hyper-inflated.
Which of the following is the most appropriate next step in the evaluation of this patient?
A. Peak expiratory flowB. ElectrocardiographyC. Measurement of arterial blood gasesD. Complete blood count

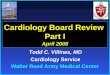
Oxygen Saturation Curve
Shift Right (unload)• Increased Temp• Increased H+• Increased 2,3,DPG
Pulse Oximetry• CO poisoning• Methemoglobinemia

Blood Gas
• Indicated only in severe exacerbations
• Respiratory drive typically increased hyperventilation
• Hypercapnea usually not seen unless FEV1 < 25%
• Normal or elevated CO2 sign of severity, but most do not require intubation

Hypercapnea
• 61/229 pts with PaCO2 > 38• Correlated with:
– Chronic, steroid dependent dz– Lower FEV1– Higher RR, PP– “Quiet chest”
• 5/61 required intubation• Resolution of hypercapnea
– 50% by 4 hours– All by 16 hours
Mountain RD, Sahn SA Am Rev Respir Dis 1988;138:535

[121] A 37 year-old man with asthma is evaluated because he continues to have frequent attacks and now believes that his short-acting B-agonist is not providing relief. He states that he is using his medications, including a long-acting B-agonist inhaler, inhaled high-dose corticosteroids, and a short-acting B-agonist inhaler as rescue medication. He has symptoms daily and nocturnal symptoms about twice per week. On PE, he is in mild respiratory distress. T 37C, BP 140/85, HR 90, RR 18. He has bilateral wheezing and oral thrush. Office spirometry showed FEV1:65% predicted, improving to 85% predicted with bronchodilators. He has no history of recent viral upper respiratory tract infections or rhinitis or symptoms of GERD.
Which of the following is the best step in this patient’s management?A. Add a leukotriene inhibitorB. Observe the patient using the metered-dose inhalerC. Start oral prednisone therapy and have the patient return for a pill
countD. Have the patient return with a symptom and treatment log

[121] A 37 year-old man with asthma is evaluated because he continues to have frequent attacks and now believes that his short-acting B-agonist is not providing relief. He states that he is using his medications, including a long-acting B-agonist inhaler, inhaled high-dose corticosteroids, and a short-acting B-agonist inhaler as rescue medication. He has symptoms daily and nocturnal symptoms about twice per week. On PE, he is in mild respiratory distress. T 37C, BP 140/85, HR 90, RR 18. He has bilateral wheezing and oral thrush. Office spirometry showed FEV1:65% predicted, improving to 85% predicted with bronchodilators. He has no history of recent viral upper respiratory tract infections or rhinitis or symptoms of GERD.
Which of the following is the best step in this patient’s management?A. Add a leukotriene inhibitorB. Observe the patient using the metered-dose inhalerC. Start oral prednisone therapy and have the patient return for a pill
countD. Have the patient return with a symptom and treatment log

[6] A 24-year-old woman is evaluate for episodes of falling asleep at inappropriate times during the day. Sleepiness occurs most often after lunch or while driving a car. She goes to bed at midnight and gets up for work at 6 AM. Her only medication is oral contraceptives. She has no symptoms of depression, drug use, restless leg syndrome, hypothyroidism, or insomnia. She does not know whether she snores, and no one in her family has sleep problems. Physical exam reveals normal weight and vital signs.
Which of the following is the most appropriate next step in the management of this patient?
A. Schedule polysomnographyB. Counsel for proper sleep hygiene with increase in sleep timeC. Schedule electroencephalographyD. Prescribe modafinil

[6] A 24-year-old woman is evaluate for episodes of falling asleep at inappropriate times during the day. Sleepiness occurs most often after lunch or while driving a car. She goes to bed at midnight and gets up for work at 6 AM. Her only medication is oral contraceptives. She has no symptoms of depression, drug use, restless leg syndrome, hypothyroidism, or insomnia. She does not know whether she snores, and no one in her family has sleep problems. Physical exam reveals normal weight and vital signs.
Which of the following is the most appropriate next step in the management of this patient?
A. Schedule polysomnographyB. Counsel for proper sleep hygiene with increase in sleep timeC. Schedule electroencephalographyD. Prescribe modafinil

[18] A 55-year-old man is evaluated for excessive daytime sleepiness and hypertension. His wife reports that he snores loudly, causing her to have to sleep in a separate bedroom. He also had a minor car accident when he fell asleep while driving. On PE, the patient is an obese man (BMI:32) with a thick neck; BP 145/90. Cardiopulmonary exam is otherwise normal.
What is the most appropriate next step in the management of this patient?
A. An attended laboratory polysomnographyB. Nighttime continuous pulse oximetryC. Automated positive airway pressure (APAP) therapyD. Modafinil therapy

[18] A 55-year-old man is evaluated for excessive daytime sleepiness and hypertension. His wife reports that he snores loudly, causing her to have to sleep in a separate bedroom. He also had a minor car accident when he fell asleep while driving. On PE, the patient is an obese man (BMI:32) with a thick neck; BP 145/90. Cardiopulmonary exam is otherwise normal.
What is the most appropriate next step in the management of this patient?
A. An attended laboratory polysomnographyB. Nighttime continuous pulse oximetryC. Automated positive airway pressure (APAP) therapyD. Modafinil therapy

Sleep Apnea
Apnea: brief periods of breathing cessation (>10 sec)• Obstructive: respiratory effort, upper airway
occlusion • Central: no respiratory effort Hypopnea: marked reduction (<50%) in tidal volumeAHI/RDI: total number of apnea + hypopnea
episodes per hour of sleep)Obstructive Sleep Apnea Syndrome: AHI of 5 or
more + excessive daytime somnolence

Merck.com

Polysomnogram in OSA

Central Sleep Apnea

Symptoms (History):• Snoring (loud, crescendo…)• Witnessed apneas; gasping or choking during sleep• Daytime somnelence (Epworth Sleep Score > 10)
– Motor vehicle accidents,work-related accidents, performance• Non-restorative sleep • Nocturnal wakening• Nocturia • Irritability, memory loss, personality change• AM headaches• Decreased libido

Risk Factors• Obesity (strongest predictor of AHI)
– Increase 1 SD BMI 4x increase in risk of AHI >=5– 10% weight loss 50% reduction in AHI
• Increased neck circumference• Gender (male:female - 2:1)• Tonsillar Hypertrophy• Nasal Septal Deviation• Craniofacial abnormalities (retrognathia, micrognathia)• Endocrine disorders (Hypothyroidism, Acromegaly)• Specific genetic disorders (Down’s Syndrome)• ETOH, sedatives, hypnotics

Associated Co-morbidities
• MVAs • HTN• Cardiovascular disease (CAD, CVA, CHF)• Glucose intolerance

[33] A 45-year-old woman is evaluated for fatigue and poor sleep quality. The patient is obese (BMI 33) and also has chronic nasal congestion. After initial evaluation, a nocturnal polysomnography shows an apnea-hyponea index (AHI) of 15 events/hour. In the supine position, the AHI was elevated at 35 events/hour compared with only 2 events per hour in the lateral position. Nasal CPAP reduced the supine AHI to 10 events/hour.
Which of the following is the most appropriate therapy for this patient?
A. Nasal CPAPB. Bi-level mechanical ventilationC. Oral applianceD. Avoidance of the supine sleep positionE. Laser-assisted uvuloplasty

[33] A 45-year-old woman is evaluated for fatigue and poor sleep quality. The patient is obese (BMI 33) and also has chronic nasal congestion. After initial evaluation, a nocturnal polysomnography shows an apnea-hyponea index (AHI) of 15 events/hour. In the supine position, the AHI was elevated at 35 events/hour compared with only 2 events per hour in the lateral position. Nasal CPAP reduced the supine AHI to 10 events/hour.
Which of the following is the most appropriate therapy for this patient?
A. Nasal CPAPB. Bi-level mechanical ventilationC. Oral applianceD. Avoidance of the supine sleep positionE. Laser-assisted uvuloplasty

Treatment Options• Nasal CPAP – titration study in lab (or home?)
– Short term compliance: 50-80%– Higher with severe OSA (higher AHI), loud snoring, or EDS
• Conservative/Behavioral Modifications– Weight loss, Lateral sleeping position– Avoid ETOH, sedatives, hypnotics
• Oral Appliances – mandibular or tongue advancement– Better than placebo, less effective than CPAP
• Surgery – UPPP (uvulopalatopharyngoplasty) – 50% effective– Laser-guided uvulopalatoplasty, tonsillectomy– Tracheostomy

[36] A 45-year-old man is evaluated for insomnia. The patient has a history of cardiomyopathy and his left ventricular ejection fraction is 20%. Nocturnal polysomnography shows Cheyne-Stokes respiratory pattern with crescendo-decrescendo clusters of breaths separated by central apneas lasting 10-20 seconds. Oxygen saturation oscillated between 85% and 95% during the breathing cycles.
What is the most likely mechanism for the patient’s sleep apnea?
A. HypoxiaB. HypocapniaC. Arousal from sleepD. Fluctuating blood pressure and cardiac output

[36] A 45-year-old man is evaluated for insomnia. The patient has a history of cardiomyopathy and his left ventricular ejection fraction is 20%. Nocturnal polysomnography shows Cheyne-Stokes respiratory pattern with crescendo-decrescendo clusters of breaths separated by central apneas lasting 10-20 seconds. Oxygen saturation oscillated between 85% and 95% during the breathing cycles.
What is the most likely mechanism for the patient’s sleep apnea?
A. HypoxiaB. HypocapniaC. Arousal from sleepD. Fluctuating blood pressure and cardiac output

[73] A 58-year-old man with progressive weakness has noted difficulty sleeping, headache on awakening in the morning, and a lack of refreshing sleep. He becomes dyspneic lying supine and has been sleeping in a reclining chair. According to his wife, he used to snore, but no longer does so. He has no swallowing difficulties, but slurs his speech slightly. On PE, RR 24/min; Palate elevates normally, but this are some tongue fasciculations, and he manifests dyspnea and abdominal paradox when lying flat. Nighttime pulse oximetry with the patient breathing room air reveals episodes of oxygen desaturation in the range of 85% to 88%, some episodes lasting longer than 5 minutes. FVC is 46% predicted when upright, and 34% predicted when supine. Arterial oxygen saturation is normal during the day, and the patient can walk slowly without difficulty.
Which of the following is the most appropriate management at this time?A. Continuous positive airway pressure (CPAP) by mask at nightB. Tracheostomy and nighttime mechanical ventilation by assist/control modeC. Noninvasive positive airway pressure ventilation by mask at nightD. Low-flow oxygen supplementation by nasal cannula at nightE. An oral hypnotic

[73] A 58-year-old man with progressive weakness has noted difficulty sleeping, headache on awakening in the morning, and a lack of refreshing sleep. He becomes dyspneic lying supine and has been sleeping in a reclining chair. According to his wife, he used to snore, but no longer does so. He has no swallowing difficulties, but slurs his speech slightly. On PE, RR 24/min; Palate elevates normally, but this are some tongue fasciculations, and he manifests dyspnea and abdominal paradox when lying flat. Nighttime pulse oximetry with the patient breathing room air reveals episodes of oxygen desaturation in the range of 85% to 88%, some episodes lasting longer than 5 minutes. FVC is 46% predicted when upright, and 34% predicted when supine. Arterial oxygen saturation is normal during the day, and the patient can walk slowly without difficulty.
Which of the following is the most appropriate management at this time?A. Continuous positive airway pressure (CPAP) by mask at nightB. Tracheostomy and nighttime mechanical ventilation by assist/control modeC. Noninvasive positive airway pressure ventilation by mask at nightD. Low-flow oxygen supplementation by nasal cannula at nightE. An oral hypnotic

Chronic Alveolar Hypoventilation
• Daytime hypercapnea– “Pickwickian” syndrome– Neuromuscular weakness
• Treated with Bipap

[94] A 28-year-old woman is evaluated for recurrent nighttime awakenings. The patient states that she awakens two to four times a night with wheezing and dyspnea; she has not had daytime symptoms. Her most recent evaluation was 4 years ago for mild asthma, for which she had been using an inhaled corticosteroid regularly and short-acting B-agonists for infrequent asthma episodes. The patient has gained 10 kg (22lb) since the last visit. Review of symptoms is unremarkable, with no features suggestive of chronic rhinosinusitis or gastroesophageal reflux. The patient states that her husband has commented on her loud snoring and that he had also mentioned that she has episodes of apnea. On exam, the patient is overweight (BMI 28), and her oropharynx is crowded with a low-lying palate. A PSG is done to evaluate for OSAS and shows an AHI of 28/hour.
Which of the following is the most appropriate management for this patient’s nighttime awakenings?
A. A sedative hypnotic agentB. Instruction on the use of inhaled bronchodilators for nighttime wheezing and
dyspneaC. CPAP therapyD. Avoid meals close to bedtime and elevating the head of her bedE. Proton pump inhibitor therapy

[94] A 28-year-old woman is evaluated for recurrent nighttime awakenings. The patient states that she awakens two to four times a night with wheezing and dyspnea; she has not had daytime symptoms. Her most recent evaluation was 4 years ago for mild asthma, for which she had been using an inhaled corticosteroid regularly and short-acting B-agonists for infrequent asthma episodes. The patient has gained 10 kg (22lb) since the last visit. Review of symptoms is unremarkable, with no features suggestive of chronic rhinosinusitis or gastroesophageal reflux. The patient states that her husband has commented on her loud snoring and that he had also mentioned that she has episodes of apnea. On exam, the patient is overweight (BMI 28), and her oropharynx is crowded with a low-lying palate. A PSG is done to evaluate for OSAS and shows an AHI of 28/hour.
Which of the following is the most appropriate management for this patient’s nighttime awakenings?
A. A sedative hypnotic agentB. Instruction on the use of inhaled bronchodilators for nighttime wheezing and
dyspneaC. CPAP therapyD. Avoid meals close to bedtime and elevating the head of her bedE. Proton pump inhibitor therapy

[108] A 53-year-old man is evaluated for management of obstructive sleep apnea, which was diagnosed 2 months ago when he was evaluated for excessive sleepiness. Polysomnography performed at that time showed an apnea-hypopnea index of 55 events per hour. The index normalized to 4 events per hour with CPAP at 18 cm H20 which was prescribed for his apnea. He says now that he cannot tolerate nasal CPAP because of nasal congestion and he has not used CPAP for 2 weeks. He has continued daytime sleepiness that affects his performance at work.
Which of the following is the most appropriate management for this patient’s condition at this time?
A. Refer for upper airway surgery for obstructive sleep apneaB. Change to an auto-titrating positive airway pressure (APAP) deviceC. Prescribe an oral device to be worn during sleepD. Manage nasal congestion and stress regular use of CPAP

[108] A 53-year-old man is evaluated for management of obstructive sleep apnea, which was diagnosed 2 months ago when he was evaluated for excessive sleepiness. Polysomnography performed at that time showed an apnea-hypopnea index of 55 events per hour. The index normalized to 4 events per hour with CPAP at 18 cm H20 which was prescribed for his apnea. He says now that he cannot tolerate nasal CPAP because of nasal congestion and he has not used CPAP for 2 weeks. He has continued daytime sleepiness that affects his performance at work.
Which of the following is the most appropriate management for this patient’s condition at this time?
A. Refer for upper airway surgery for obstructive sleep apneaB. Change to an auto-titrating positive airway pressure (APAP) deviceC. Prescribe an oral device to be worn during sleepD. Manage nasal congestion and stress regular use of CPAP

[3] A 38-year-old woman is evaluated for a moderate pleural effusion that layers out on a lateral decubitus chest film. Thorcentesis is done and analysis of the pleural fluid shows the following:Cell count/differential: 1000 RBCs, 300 WBCs (33% neutrophils, 52% lymphocytes, 12% mesothelial cells, and 3% eosinophils)Total Protein: 1.3 g/dLLDH 61 U/LAmylase 15 U/LGlucose 100 mg/dLAlbumin 0.7 g/dLTriglycerides 18 mg/dLCholesterol 35 mg/dLpH: 7.4
The pleural fluid is yellow and serous. Gram stain of the pleural fluid shows no organisms. Pleural fluid smears are negative for acid-fast bacilli. Cytology is negative for malignant cells. Serum total protein is 4.8 g/dL, serum albumin 2.3 g/dL, serum LDH 220 U/L, and INR 1.5 and a normal UA. ECG is normal.
Which of the following is the most likely diagnosis?A. TuberculosisB. Thoracic endometriosisC. Hepatic hydrothoraxD. LymphangioleiomyomatosisE. Esophageal rupture

[3] A 38-year-old woman is evaluated for a moderate pleural effusion that layers out on a lateral decubitus chest film. Thorcentesis is done and analysis of the pleural fluid shows the following:Cell count/differential: 1000 RBCs, 300 WBCs (33% neutrophils, 52% lymphocytes, 12% mesothelial cells, and 3% eosinophils)Total Protein: 1.3 g/dLLDH 61 U/LAmylase 15 U/LGlucose 100 mg/dLAlbumin 0.7 g/dLTriglycerides 18 mg/dLCholesterol 35 mg/dLpH: 7.4
The pleural fluid is yellow and serous. Gram stain of the pleural fluid shows no organisms. Pleural fluid smears are negative for acid-fast bacilli. Cytology is negative for malignant cells. Serum total protein is 4.8 g/dL, serum albumin 2.3 g/dL, serum LDH 220 U/L, and INR 1.5 and a normal UA. ECG is normal.
Which of the following is the most likely diagnosis?A. TuberculosisB. Thoracic endometriosisC. Hepatic hydrothoraxD. LymphangioleiomyomatosisE. Esophageal rupture

[14] A 25-year-old man is evaluated for a 2-month history of low-grade fevers, cough, night sweats, fatigue, pleuritic chest pain, and weight loss. The patient emigrated from Mexico almost 2 years ago and now lives in central California. On PE, T: 38DC, HR 96/min, RR 22/min, 94% sats on room air. There are diminished breath sounds and vocal fremitus over the right hemithorax. The left lung is clear. Peripheral blood WBC 9000/uL (60% neutrophils, 35% lymphs). LFTs are normal. CXR shows moderate right-sided pleural effusion with layering of 3cm of free-flowing fluid and no parenchymal infiltrates on R lateral decub. Thoracentesis yields 1.0 L of minimally turbid, yellow fluid with test results as follows:Cell count/differential: 3000 WBCs (5% neutrophils, 85% lymphocytes, 1% mesothelial cells, and 1% macrophages)Total Protein: 15.5 g/dLLDH 290 U/LGlucose 80 mg/dLpH: 7.36
Pleural fluid Gram, fungal, and acid-fast bacilli stains are negative. Tuberculin skin test is pending. Serologic tests for fungal organisms are negative. Cytology is negative.
Which of the following is the most likely diagnosis?A. TuberculosisB. Pneumococcal parapneumonic effusionC. Pulmonary embolismD. Malignant pleural effusionE. Pleural effusion due to coccidioidomycosis

[14] A 25-year-old man is evaluated for a 2-month history of low-grade fevers, cough, night sweats, fatigue, pleuritic chest pain, and weight loss. The patient emigrated from Mexico almost 2 years ago and now lives in central California. On PE, T: 38DC, HR 96/min, RR 22/min, 94% sats on room air. There are diminished breath sounds and vocal fremitus over the right hemithorax. The left lung is clear. Peripheral blood WBC 9000/uL (60% neutrophils, 35% lymphs). LFTs are normal. CXR shows moderate right-sided pleural effusion with layering of 3cm of free-flowing fluid and no parenchymal infiltrates on R lateral decub. Thoracentesis yields 1.0 L of minimally turbid, yellow fluid with test results as follows:Cell count/differential: 3000 WBCs (5% neutrophils, 85% lymphocytes, 1% mesothelial cells, and 1% macrophages)Total Protein: 15.5 g/dLLDH 290 U/LGlucose 80 mg/dLpH: 7.36
Pleural fluid Gram, fungal, and acid-fast bacilli stains are negative. Tuberculin skin test is pending. Serologic tests for fungal organisms are negative. Cytology is negative.
Which of the following is the most likely diagnosis?A. TuberculosisB. Pneumococcal parapneumonic effusionC. Pulmonary embolismD. Malignant pleural effusionE. Pleural effusion due to coccidioidomycosis

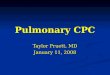
Light RW, Pleural Diseases, 4th Ed.

Pleural Effusions
Exudates (local)
• Infection• Malignancy• PE• Collagen Vascular• Post-CABG• GI (pancreatitis, esoph
rupture, liver abscess…)
Transudates (systemic)
• CHF• Cirrhosis• Nephrotic syndrome• PE• Myxedema• Urinothorax

Effusions
WBCs– >1000 (exudate), >10,000 parapneumonic,
>100,000 empyema/pus
• Eosinophils (>10%)– Pneumothorax, blood, drug reaction,
paragonimiasis
• Neutrophils– Pneumonia, pancreatitis, peritonitis, PE

Effusions
Lymphocytes >50%• Malignancy (lung, breast, lymphoma)
– Fluid cytology – 3 samples 90% yield– Lower pH, worse prognosis
• Tuberculosis– Fluid low yield (20%) for AFB, cultures– Pleural biopsy– Pleural fluid ADA, IFN-gamma– Rarely see mesothelial cells

[22] A 49-year-old man presents with shortness of breath, abdominal distension, and swelling of the legs. Six months ago he had hematemesis and had an EGD performed. He consumes a 12-pack of beer everyday. On physical examination, T 36.4C, HER 116/min, RR 26/min, 94% on 3L nc. He has spider nevi on the chest, dilated veins on the abdominal wall, gynecomastia and 1+ pitting leg edema. Breath sounds are decreased in the right hemithorax. Abdominal exam reveals ascites. CXR shows moderate R effusion that layers on lateral decubitus. Diagnostic thoracentesis shows:Cell count/differential: 1000 RBCs, 300 WBCs (33% neutrophils, 52% lymphocytes, 12% mesothelial cells, and 3% eosinophils)Total Protein: 1.3 g/dLLDH 61 U/LAmylase 15 U/LGlucose 100 mg/dLAlbumin 0.7 g/dLTriglycerides 18 mg/dLCholesterol35 mg/dLpH: 7.4
The pleural fluid is yellow and serous. Gram stain of the pleural fluid shows no organisms. Pleural fluid smears are negative for acid-fast bacilli. Cytology is negative for malignant cells. Serum total protein is 4.8 g/dL, serum albumin 1.8 g/dL, serum LDH 220 U/L, and INR 1.8 and a normal UA. ECG is normal.
Which of the following is the most appropriate management for this patient?A. Chest tube drainageB. Antibiotic therapyC. Salt restriction and diuretic therapyD. Bronchoscopy

[22] A 49-year-old man presents with shortness of breath, abdominal distension, and swelling of the legs. Six months ago he had hematemesis and had an EGD performed. He consumes a 12-pack of beer everyday. On physical examination, T 36.4C, HER 116/min, RR 26/min, 94% on 3L nc. He has spider nevi on the chest, dilated veins on the abdominal wall, gynecomastia and 1+ pitting leg edema. Breath sounds are decreased in the right hemithorax. Abdominal exam reveals ascites. CXR shows moderate R effusion that layers on lateral decubitus. Diagnostic thoracentesis shows:Cell count/differential: 1000 RBCs, 300 WBCs (33% neutrophils, 52% lymphocytes, 12% mesothelial cells, and 3% eosinophils)Total Protein: 1.3 g/dLLDH 61 U/LAmylase 15 U/LGlucose 100 mg/dLAlbumin 0.7 g/dLTriglycerides 18 mg/dLCholesterol35 mg/dLpH: 7.4
The pleural fluid is yellow and serous. Gram stain of the pleural fluid shows no organisms. Pleural fluid smears are negative for acid-fast bacilli. Cytology is negative for malignant cells. Serum total protein is 4.8 g/dL, serum albumin 1.8 g/dL, serum LDH 220 U/L, and INR 1.8 and a normal UA. ECG is normal.
Which of the following is the most appropriate management for this patient?A. Chest tube drainageB. Antibiotic therapyC. Salt restriction and diuretic therapyD. Bronchoscopy

[70] A 63 year-old man is evaluated for 2 week history of cough, fever, and increasing dyspnea. He has a dull ache in the R chest and has lost 4.4 lb in a week. He is a smoker and drinks heavily. He has poorly controlled DM2. On exam, T38.9C, BP 96/60 HR 120, RR 26/min. He has halitosis and poor dental hygiene. The trachea is not deviated. There is decreased respiratory excursion ion the right side with decreased breath sounds and egophany. Bronchial breathing is heard in the mid chest posteriorly. Peripheral blood WBC 24K, Hb 8.5. CXR shows moderatele R effusion and R lateral decubitus film shows free flowing fluid >3cm from chest wall. Thoracentesis yields 1L of foul smelling turbid fluid and GPC on gram stain. Pleural fluid shows;Cell count/differential: 1200 RBCs, 2495 WBCs (80% neutrophils, 15% lymphocytes, 2% mesothelial cells, and 3% eosinophils)Total Protein: 5.5 g/dLLDH: 3200 U/LGlucose: 25 mg/dLpH: 6.95
Which of the following would be the most appropriate next step in the management of this patient?
A. Intravenous ceftriaxone and azithromycinB. Intravenous pipercillin-tazobactam plus gentamicinC. Intravenous pipercillin-tazobactam plus gentamicin plus tube thoracostomyD. Intravenous ciprofloxacin and video-assisted thoracostomy with decorticationE. Intrapleural fibrinolytic therapy

[70] A 63 year-old man is evaluated for 2 week history of cough, fever, and increasing dyspnea. He has a dull ache in the R chest and has lost 4.4 lb in a week. He is a smoker and drinks heavily. He has poorly controlled DM2. On exam, T38.9C, BP 96/60 HR 120, RR 26/min. He has halitosis and poor dental hygiene. The trachea is not deviated. There is decreased respiratory excursion ion the right side with decreased breath sounds and egophany. Bronchial breathing is heard in the mid chest posteriorly. Peripheral blood WBC 24K, Hb 8.5. CXR shows moderatele R effusion and R lateral decubitus film shows free flowing fluid >3cm from chest wall. Thoracentesis yields 1L of foul smelling turbid fluid and GPC on gram stain. Pleural fluid shows;Cell count/differential: 1200 RBCs, 2495 WBCs (80% neutrophils, 15% lymphocytes, 2% mesothelial cells, and 3% eosinophils)Total Protein: 5.5 g/dLLDH: 3200 U/LGlucose: 25 mg/dLpH: 6.95
Which of the following would be the most appropriate next step in the management of this patient?
A. Intravenous ceftriaxone and azithromycinB. Intravenous pipercillin-tazobactam plus gentamicinC. Intravenous pipercillin-tazobactam plus gentamicin plus tube thoracostomyD. Intravenous ciprofloxacin and video-assisted thoracostomy with decorticationE. Intrapleural fibrinolytic therapy

Effusions
Glucose < 60• Parapneumonic • Malignancy• TB• Rheumatoid arthritis
pH < 7.3 – malignancy, infection, RApH < 7.0
– Empyema– Esophageal rupture (salivary amylase)

[60] A 75-year-old man with 80 pk-year smoking history is evaluated for a 3-month history of night sweats, weight loss, and progressive shortness of breath. He has a dull ache in his left chest. He has an occasional cough with mucoid sputum procuction, and is dyspneic with minimal exertion. On PE, T 36.8C, HR 112, RR 26, SBP: 96mmHg. The trachea is shifted to the left, and he has dullness to percussion and decreased breath sounds in the left hemithorax. No peripheral edema. WBC 6.8K, metabolic panel and liver panel are normal. Serum protein: 5.0 g/dL and serum LDH is 188 U/L. CXR shows complete opacificatoin of the left hemithorax and mediastinal shift to the right. Pleural fluid showed:Cell count/differential: 150,000 RBCs, 980 WBCs (20% neutrophils, 55% lymphocytes, 10% mesothelial cells, and 15% eosinophils)Total Protein: 4.5 g/dLLDH 1200 U/LGlucose 45 mg/dLpH: 7.2
Pleural fluid gram stain is negative. Cytology is pending.
Which of the following is the most likely diagnosis?A. Transudative pleural effusionB. Malignant pleural effusionC. Parapneumonic effusionD. Rheumatoid pleural effusionE. Pleural effusion associated with esophageal rupture

[60] A 75-year-old man with 80 pk-year smoking history is evaluated for a 3-month history of night sweats, weight loss, and progressive shortness of breath. He has a dull ache in his left chest. He has an occasional cough with mucoid sputum procuction, and is dyspneic with minimal exertion. On PE, T 36.8C, HR 112, RR 26, SBP: 96mmHg. The trachea is shifted to the left, and he has dullness to percussion and decreased breath sounds in the left hemithorax. No peripheral edema. WBC 6.8K, metabolic panel and liver panel are normal. Serum protein: 5.0 g/dL and serum LDH is 188 U/L. CXR shows complete opacificatoin of the left hemithorax and mediastinal shift to the right. Pleural fluid showed:Cell count/differential: 150,000 RBCs, 980 WBCs (20% neutrophils, 55% lymphocytes, 10% mesothelial cells, and 15% eosinophils)Total Protein: 4.5 g/dLLDH 1200 U/LGlucose 45 mg/dLpH: 7.2
Pleural fluid gram stain is negative. Cytology is pending.
Which of the following is the most likely diagnosis?A. Transudative pleural effusionB. Malignant pleural effusionC. Parapneumonic effusionD. Rheumatoid pleural effusionE. Pleural effusion associated with esophageal rupture

[81] A 40-year-old man is evaluated for shortness of breath and left-sided chest discomfort without cough, fever, or hemoptysis. He had a contusion to the left side of his chest and back 1 week ago as a result of an automobile accident. CXR immediately after the accident showed no fracture of the spine or ribs, but he had severe contusions on his back and on the left side of his chest. PE shows contusions on the back and chest, and dullness on percussion and decreased breath sounds on the left side. CXR shows a moderate-sized left-sided pleura effusion without a pneumothorax. Pleural fluid aspiration yields 500cc of pleural fluid. Serum protein is 5.8 g/L, cholesterol 200mg/dL, and triglycerides 100mg/dL. Pleural fluid analysis shows:Cell count/differential: 300 RBCs, 890 WBCs (22% neutrophils, 65% lymphocytes, 4% mesothelial cells, and 4% eosinophils)Total Protein: 3.5 g/dLLDH 250 U/LAmylase 25U/LTriglycerides 145 mg/dLCholesterol 38 mg/dLpH: 7.5Cytology, gram stain, AFB, and culture all negative
Which of the following is the most likely diagnosis?A. ChylothoraxB. Parapneumonic effusionC. PseudochylothoraxD. Malignant pleural effusionE. Tuberculous pleural effusion

[81] A 40-year-old man is evaluated for shortness of breath and left-sided chest discomfort without cough, fever, or hemoptysis. He had a contusion to the left side of his chest and back 1 week ago as a result of an automobile accident. CXR immediately after the accident showed no fracture of the spine or ribs, but he had severe contusions on his back and on the left side of his chest. PE shows contusions on the back and chest, and dullness on percussion and decreased breath sounds on the left side. CXR shows a moderate-sized left-sided pleura effusion without a pneumothorax. Pleural fluid aspiration yields 500cc of pleural fluid. Serum protein is 5.8 g/L, cholesterol 200mg/dL, and triglycerides 100mg/dL. Pleural fluid analysis shows:Cell count/differential: 300 RBCs, 890 WBCs (22% neutrophils, 65% lymphocytes, 4% mesothelial cells, and 4% eosinophils)Total Protein: 3.5 g/dLLDH 250 U/LAmylase 25U/LTriglycerides 145 mg/dLCholesterol 38 mg/dLpH: 7.5Cytology, gram stain, AFB, and culture all negative
Which of the following is the most likely diagnosis?A. ChylothoraxB. Parapneumonic effusionC. PseudochylothoraxD. Malignant pleural effusionE. Tuberculous pleural effusion

Effusions
Chylothorax– Cloudy, white appearance (even after centrifuge)
– Pleural fluid triglycerides > 110 mg/dl– Chylomicrons (look with lipoprotein analysis if TG
50-110 mg/dL)– Acute (trauma, lymphoma, LAM)
Pseudochylothorax– Cholesterol crystals, fluid cholesterol usually >200– Chronic, thickened pleura (chyliform effusion)– Generally triglycerides < 50

[66] A 45-year-old man is evaluated in the emergency department for acute shortness of breath with right-sided chest pain. He also has a dry cough with scanty bloody streaking of his phlegm. He is a non-smoker and has no other past medical illnesses. He just returned by airplane from Japan. PE shows T 37.4C, BP 102/76, HR 98, RR 32/min. Breath sounds are marginally decreased on the right side with vocal fremitus. The pulmonary component of the second heart sounds is accentuated. He feels soreness in the left calf and has trace L ankle edema. Peripheral pulses are intact. LE compression US is positive for DVT. Spiral chest CT confirms the presence of pulmonary emboli and a small right-sided pleural effusion. The patient is hospitalized and therapy with heparin is started. On day 3, the PT is 14.7, INR: 1.6. CXR shows stable R effusion occupying about ¼ of the right hemithorax. US guided thoracentesis is performed showing: Cell count/differential: 100,000 RBCs, 465 WBCs (70% neutrophils, 25% lymphocytes, 2% mesothelial cells, and 3% eosinophils)Total Protein: 3.5 g/dLLDH 400 U/LGlucose 75 mg/dLpH: 7.45
Gram stain shows no organisms.
Which of the following is the most appropriate next step in management?A. Discontinue heparin, continue warfarinB. Discontinue warfarinC. Continue heparin and warfarin until INR is therapeutic, and then discontinue heparinD. Discontinue both heparin and warfarinE. Place and inferior vena cava filter

[66] A 45-year-old man is evaluated in the emergency department for acute shortness of breath with right-sided chest pain. He also has a dry cough with scanty bloody streaking of his phlegm. He is a non-smoker and has no other past medical illnesses. He just returned by airplane from Japan. PE shows T 37.4C, BP 102/76, HR 98, RR 32/min. Breath sounds are marginally decreased on the right side with vocal fremitus. The pulmonary component of the second heart sounds is accentuated. He feels soreness in the left calf and has trace L ankle edema. Peripheral pulses are intact. LE compression US is positive for DVT. Spiral chest CT confirms the presence of pulmonary emboli and a small right-sided pleural effusion. The patient is hospitalized and therapy with heparin is started. On day 3, the PT is 14.7, INR: 1.6. CXR shows stable R effusion occupying about ¼ of the right hemithorax. US guided thoracentesis is performed showing: Cell count/differential: 100,000 RBCs, 465 WBCs (70% neutrophils, 25% lymphocytes, 2% mesothelial cells, and 3% eosinophils)Total Protein: 3.5 g/dLLDH 400 U/LGlucose 75 mg/dLpH: 7.45
Gram stain shows no organisms.
Which of the following is the most appropriate next step in management?A. Discontinue heparin, continue warfarinB. Discontinue warfarinC. Continue heparin and warfarin until INR is therapeutic, and then discontinue heparinD. Discontinue both heparin and warfarinE. Place and inferior vena cava filter


65 yo admitted for CAP with pleural effusion. What is the next step for each thoracentesis result?
• G+ cocci in pairs on gram stain
• pH 7.15, glu 60 no organisms
• pH 7.3, LDH 300
• pH <7.1, glucose 30, loculations on cxr

65 yo admitted for CAP with pleural effusion. What is the next step for each thoracentesis result?
• G+ cocci in pairs on gram stain– Chest tube
• pH 7.15, glu 60 no organisms– Abx and repeat tap in 12-24 hrs
• pH 7.3, LDH 300– Abx
• pH <7.1, glucose 30, loculations on cxr– Chest tube, consider early VATS

Pulmonary Function Testing

Laryngoscopy


Epidemiology - Asthma
• Common - 7% of adults in US
• >1 million ER visits annually
• 3rd leading cause of preventable hospitalizations in US
• >5000 deaths/year– Rate of death nearly doubled in 1980s– Patients requiring MV 13% mortality

Theophylline
Murphy DG Arch Intern Med 1993;153:1784• 44 pts, acute asthma, b-agonist + steroids• Aminophylline v. placebo• No change in PEFR at 1-5 hours, toxicity
Huang D Ann Intern Med 1993;119:1155• 21 pts, acute asthma, b-agonist + steroids• Aminophylline v. placebo• Improved FEV1 at 3 hours, 48 hours
Not recommended by NHLBI for routine use

Magnesium
• 48 pts, limited response to b-agonist
• 3 groups– 2gms bolus, then 2gm/h– 2gm/h infusion– Placebo
• No change in FEV1 or PEFR
Tiffany BR et al Chest 1993;104:831