Embed Size (px)
Citation preview

Pulmonary Board ReviewPart 2
Lisa M. Zahn, MDMount Sinai School of MedicineDepartment of Emergency MedicineJanuary 23, 2008

Lecture 1
• Pneumonia: community acquired, immunocompromised host, aspiration, pediatric
• Pneumothorax• Mycobacterium tuberculosis• Miscellaneous: Pleural effusion, lung abscess, ARDS, acute
chest syndrome in Sickle Cell Anemia
Lecture 2
• Pulmonary Embolism / Fat Embolism• Asthma / COPD• Cancer• Peds Pulmonary: croup, FB, CF• Miscellaneous: cyanosis, hiccups
Pulmonary Embolism
Which of the following statements regarding the utility of a spiral CT angiogram of the chest for the dx of PE is correct?
a) a completely negative spiral CT lung scan is equivalent to a nl v/q lung scan
b) a high-probability v/q lung scan and a spiral CT angiogram of the chest have similar specificities for PEc) a spiral CT lung scan will most likely be non-diagnostic in patients with a hx of COPDd) the sensitivity and specificity of spiral CT for PE in central vessels are similar to those in peripheral vesselse) when used to dx PE, a spiral CT lung scan spares use of contrast material
Answer is B
Spiral (helical) CT angiography has replaced V-Q scanning
Spiral CT takes less than 30 seconds, and uses IV contrast material. It can image the main pulmonary arteries to the segmental ones. On CT it is hard to identify PE in the subsegmental vessels. Spiral CT has higher sensitivity and specificity for PE in central vs peripheral vessels
Subsegmental PE’s are a common source of false-negative spiral CT readings
Spiral CT has a similar specificity for PE when c/w high-prob v/q scan 93% and 98% respectively. And a similar sensitivity when c/w low-prob v/q scan 78% and 82% respectively. However, a negative spiral CT scan is not as sensitive as a normal v/q scan
Conditions that can result in non-dx v/q lung scan include: heavy smoking, COPD, parenchymal infiltrate
CT also affords the benefit of detecting alternative dx such as aortic dissection
Which of the following is part of the Wells criteria for the assessment of pretest probability for PE?
a) heart rate greater than 90 bpmb) immobilization or surgery in the previous 4
weeksc) nonproductive coughd) Pao2 less than 60 mmHge) pleuritic chest pain
Answer is D
There are many different ways to risk stratify pts with regard to likelihood of PE. Most group pts into low risk (<10% probability), moderate risk (11-60% probability) or high risk (>60% probability) by incorporating signs, symptoms and risk factors
The Wells et al., criteria for PE are:• Suspected DVT = 3 points• Alternative dx less likely than PE = 3 points• HR greater than 100 bpm = 1.5 points• Immobilization or surgery in the previous 4 weeks = 1.5 points• Previous hx of dvt/pe = 1.5 points• Hemoptysis = 1 point• Malignancy (i.e., active tx, tx in past 6 months or palliative) = 1 point
Low-risk pts (score <2; 40% of total pts) had a mean probability of 3.6% for PE
Intermediate-risk pts (score 2-6 points; 53% of total pts) had a mean probability of 20.5% for PE
High-risk pts (score > 6 points; 7% of total pts) had a mean probability of 66.7% for PE
PERC rule (Kline, et al 2004)
Use the following 8 clinical criteria to determine pretest probability:• age < 50 yo• HR < 100 bpm• RA sat > 94%• No prior DVT or PE• No recent trauma or surgery• No hemoptysis• No exogenous estrogen• No clinical signs suggestive of DVT
If pt with none of the above, pretest probability is less than 2% (in ED pts) and therefore pt will not benefit from eval for PE. This was derived from a large multicenter database and validated at 4 academic med centers.
Recall that the “good” d-dimer test is the ELISA or turbidimetric D-dimer

Varicose veinsSuperficial vein dilatation
Which of the following statements regarding fat embolism is correct?
a) heparin is a mainstay of therapy
b) most often occurs after sternal fx’s
c) petechial rash typically appears on the lower extremities
d) systemic arterial circulation is rarely affected
e) thrombocytopenia is often an early finding
Answer is E
Predisposing factors for fat embolism include hip fx and long bone (tibia, fibula, femur ) fx
Incidence increases with multiple fx’s (0.5% to 2% isolated vs 5 to 10% multiple)
c/w thromboemboli, fat emboli can pass through the pulmonary circulation into the systemic arterial circulation; any organ can be affected
Symptoms occur 1-3 days after an acute injury. And include: respiratory distress, CNS symptoms such as headache, irritability, AMS, convulsions and coma
Signs include: upper body (chest, axilla, neck, fundi, conjunctivae) petechiae
Thrombocytopenia occurs late in disease
Fat globulins can be seen in the urine in half of pts w/i 3 days of injury but are not diagnostic
Management is supportive, and most often self-resolving
Several trials have shown efficacy of IV steroids
Heparin is not a treatment modality
Asthma / COPD
Which of the following statements regarding the management of acute severe asthma is most accurate?
a) corticosteroids should be administered after completion of bronchodilator therapy
b) IV beta-agonists are more effective than nebulized beta-agonists
c) magnesium administration results in an improvement of approximately 10% of FEV1
d) patients require high-dose corticosteroid therapy
e) response to corticosteroids is age related
Answer is C
No evidence for IV beta-agonists. For severe exacerbations, use continuous nebulizations. But for mild to moderate attacks there appears to be no difference in continuous vs intermittent delivery.
Use corticosteroids early in the course of treatment of a severe acute asthma attack.
Studies have shown that early steroid use reduces admission rates.
No advantage for IV vs oral steroids. But use IV if cannot take po (emesis, extremely sob, etc…)
No need for high dose steroids, lower doses seem effective in most cases.
No age-related response to steroids.
Magnesium beneficial in severe asthma exacerbations (FEV1<25% predicted), resulting in an improvement of about 10% of predicted FEV1, which is clinically significant. Adverse effects of magnesium are: hypotension, fatigue.

Which of the following pts is at the highest risk for death from asthma?
a) 24 year old black male who has a hx of childhood asthma
b) 28 year old black woman who is currently using systemic corticosteroids
c) 36 year old Hispanic man who has been hospitalized once for asthma within the past year
d) 42 year old woman who has used an entire inhaled short-acting beta2-agonist canister this month
e) 50 year old white man who has a PMH of mild depression
Answer is B
Risk factors for death from asthma• past hx of sudden severe exacerbations• prior intubation for asthma• prior admission to an ICU• 2+ admissions for asthma in the past year• hospitalization or ED visit for asthma in past month• use of >2 canisters of albuterol q month• current use or recent w/d of corticosteroids• difficulty perceiving severity of airflow obstruction• comorbidities (e.g, cv dz)• serious psychiatric/psychosocial issues• drug abuse (especially inhaled cocaine and heroin)• low SES in urban residents• poor access to health care
Hx of just peds asthma not a RF for death
Most asthma deaths occur from 15 to 34 years old
Higher death rate in black pts
Non-hispanic black pts have higher asthma mortality when c/w non-Hispanic white pts and Hispanic pts
Prevalence of asthma is lower in Hispanics c/w white non-Hispanics or black non-hispanics
Females have a significantly higher death rates from asthma than men
Most asthma deaths occur at night, within 24 hours of symptom onset (these pts often don’t make it to the hospital)
Western countries have higher rates of asthma, especially among persons who live in inner-city areas
In an asthmatic pt who requires intubation:
a) inspiratory to expiratory ratio should be kept at 1:2
b) ketamine is the preferred paralytic agentc) nasotracheal intubation is preferred over
orotracheald) propofol can be used as a sedating
agente) tidal volume should be kept at 10 cc/kg
of ideal body weight
Answer is D
1% - 2% of pts with asthma exacerbation require endotracheal intubation
Indications include profound hypoxia, depressed mental status, exhaustion, respiratory failure
Orotracheal, RSI with induction / paralytic agents
Nasotracheal requires a smaller diameter ETT, resulting in greater airway resistance, which is not desirable in an asthmatic. Also, airway secretion can obstruct the tube, causing higher resistance
Ketamine is preferred for induction, because it has direct bronchodilating properties and stimulates the release of catecholamines
Succinylcholine or rocuronium for paralysis
Propofol has bronchodilating properties and is often used for continues sedation
Complications of mechanical ventilation include hypotension and barotrauma, which can be reduced by reducing mean airway pressure. Accomplish this by reducing minute ventilation (TV x RR), increasing inspiratory flow rates, and maintaining low plateau pressure
Set TV at 6-8 cc/kg (c/w 8 to 10 cc/kg of ideal body wt)
Set RR at 8-10 breaths/min (c/w 10-12 breath/min)
Prolong the expiration phase with an I to E ratio of 1:4 or 1:5. This allows for full expiration, thereby reducing air trapping
Inspiratory flow rate should be increased from the usual to 80 to 100 liter/min with a decelerating flow pattern (c/w 60 liter/min)
Plateau pressure should be maintained at less than 30 cm H2O
Predicted difficulties during intubation with a fiberoptic bronchoscope include:
a) bleeding in the airway
b) cervical spine injury
c) epiglottitis
d) limited mouth opening
e) protuberant teeth

Answer is A
Fiberoptic bronchoscope can be used on awake pts or following sedation and paralysis
It is much more difficult if there is bleeding in the airway or excessive oral secretions
The suction on the scope is usually inadequate. Sometimes attaching oxygen to blow away excess secretions can be helpful
Paradoxically, intubation using a scope in a supine anesthetized or comatose pt is more difficult c/w an awake upright pt. Following anesthesia, the soft tissues of the OP and hypopharynx can collapse in a supine pt. These problems can be corrected by using oral airways, or having an assistants provide jaw thrust or simultaneous DL
Ideal situation is to use scope on awake pts with a known or suspected difficult airway. C-spine injury or pts with limited mouth opening are ideal candidates for awake intubation with scope
For pts with epiglottitis, scope is preferential mode of intubation
Intubation is by nasal route
Protuberant teeth are not a contraindication. But if considering DL in these pts, Miller blade may provide a better view

Which of the following abnormalities is typically seen on the CXR of a pt with emphysema?
a) decreased retrosternal air space
b) elevated dome-shaped diaphragm
c) enlarge cardiac silhouette
d) hyperinflated lungs
e) increased vascular markings

Answer is D
COPD is characterized by progressive airflow obstruction that is not fully reversible and is associated with an unusual inflammatory response to noxious particles or gases
In the past, COPD was defined as 3 distinct processes (asthma, emphysema, bronchitis) but recent definitions of COPD have excluded the asthma component and have attempted to exclude the distinction between emphysema vs bronchitis
In asthma, unlike COPD, airflow obstruction is reversible
In bronchial washings of COPD pts, neutrophils, lymphocytes and macrophages predominate whereas in asthmatics, eosinophils do
Most important RF for COPD is cigarette smoking
CXR are important to obtain in pts with copd, presenting with presumed exacerbations in order to exclude PNA, PTX which can present similarly to an exacerbation.
COPD pts can have fairly NL CXR
CXR findings in pts with emphysema include : hyperinflated lung fields, decreased vascular markings, increased parenchymal lucency, small cardiac silhouette, flattened diaphragm, increased retrosternal air space and bullae
Which of the following statements regarding bronchiectasis is correct?
a) hemoptysis occurs in a minority of casesb) it involves small-sized airways often at
the level of the alveolic) Staphylococcus aureus lower respiratory
tract infection is an important caused) the associated cough is most often drye) viruses have not been shown to be
associated with its development
Answer is C
Bronchiectasis can occur from both infectious and noninfectious causes
Infection (by bacteria or virus) results in inflammation and epithelial injury in the walls of medium-sized airway (level of segmental or subsegmental bronchi). Damaged walls lose their ability to clear pulmonary secretions, resulting in microbe colonization, infection, more inflammation and bronchial injury. This cycle results in permanent dilation of bronchi, and replacement of the NL bronchial lining with fibrous tissue
Common viral infections are caused by adeno and influenza virus. Common bacteria include: S. aureus, Klebsiella, P. aeruginosa, H. flu and anaerobic flora. TB and Mycobacterium avium complex are possible also. Necrotizing fungal infections and Mycoplasma rarely result in bronchiectasis
Toxic inhaled substances (e.g., ammonia) can result in bronchiectasis
Symptoms include persistent or recurrent cough with purulent sputum
Hemoptysis occurs in the majority of pts (50%-70%)
Radiographic changes best visualized on high-res chest CT
Mngmnt: control infection with abx, and improve clearance of pulm secretions
Lung tx is an option

Cancer
Which of the following statements regarding lung cancer is correct?
a) cavitation is commonly seen in small cell cancersb) extrathoracic metastases are rarely seen with small
cell lung cancerc) large cell cancers of the lung tend to present as
peripheral massesd) small cell neoplasms are not a common cause of SVC
obstructione) squamous cell carcinoma is the most common type of
lung cancer in the US
The answer is C
Lung cancer describes tumors originating from the respiratory tract epithelium (bronchi, bronchioles, alveoli)
Lung cancer is the leading cause of CA death in the US in men and women
Peak incidence is 55 to 65 years
Primary lung cancer can be categorized into:- Squamous cell (epidermoid) carcinoma: central mass, cavitation,
SVC syndrome- Small cell (oat cell) carcinoma: central mass, SVC syndrome- Adenocarcinoma (including bronchioalveolar): peripheral mass- Large cell (large cell anaplastic) carcinoma: peripheral mass,
cavitation

In the US, adenocarcinoma is the most common type, then squamous cell then small cell then large cell
Tx decisions are based on small cell or non-small cell. C/w small cell, non-small cell cancers do not respond as well to chemo
Small cell ca: chemo +/- RT
90% of lung ca pts have a hx of cigarette smoking.
Active smoking increases the RR of lung ca by 13 fold
Long-term passive exposure increases the RR by 1.5 fold COPD is another RF
Mets, most commonly encountered in small cell cancer can occur in almost any organ system: brain, bone, BM, liver, LN, spinal cord, adrenal glands. (Adrenal mets are common but rarely result in adrenal insufficiency.)
Which of the following statements regarding asbestosis is correct?
a) early radiographic changes occur along the upper lung fields
b) it is a form of localized interstitial fibrosing lung disease
c) mesotheliomas rarely metastasized) small cell carcinoma is the most common
associated cancere) smoking and asbestosis exposure
increase the risk of lung cancer
Answer is E
Asbestos encompasses various mineral silicates (chrysolite, amosite, anthophyllite, crocidolite). B/c of their excellent thermal and electrical insulation properties, they were commonly used in building construction, fire-smothering blankets, cement and floor tiles, etc… Most manufacturing occurred between 1930-1960
Asbestos exposure can result in diffuse interstitial fibrosing lung dz (asbestosis), lung ca (squamous cell and adenocarcinoma) and mesotheliomas (pleural and peritoneal)
Usually, moderate to severe exposure has to occur for at least 10 years before dz becomes clinically apparent
Early CXR findings include bilateral, irregular, or linear opacities along the lung periphery and lower lobes. With dz progression, changes are noticeable w/I the middle and upper fields
Smoking along with asbestos exposure increases risk of developing lung ca
A 70 year old Jewish man presents with a chief complaint of left nipple retraction. He has had a painless left subareolar mass for the past 3 months. He has not noticed any nipple d/c, and there have been no signs of infection. He had a mammogram 1 month earlier that was read as negative. Which of the following statements regarding this pt’s condition is correct?
a) gynecomastia is a significant RF for breast cancer in menb) Jewish ancestry is associated with a lower risk for breast cancer in
menc) mammography is of no value when evaluating breast cancer in mend) most men with breast cancer present with a painful subareolar masse) workup should include bx despite the negative mammogram
Answer is E
Breast cancer in men is rare, comprising < 1% of all cases of cancer in men
Median age at dx is 68 yo
Associated with hormonal abnlities
RF in men: testicular abnlities, infertility, Klinefelter, positive FH, benign br conditions, radiation exposure, Jewish ancestry
90% of breast tumors in men are invasive carcinomas: infiltrating ductal carcinoma
Common presenting s/s: br mass, nipple retraction or ulceration or bleeding or d/c, localized pain. 85% present with a painless subareolar mass
Dx: mammography, fna vs core vs excisional bx
Pediatric Pulmonary
Which of the following statements regarding cystic fibrosis is correct?
a) Aspergillus fumigatus is commonly found in patients’ sputum
b) it is a contraindication to lung transplantationc) it is most commonly observed in African-
Americansd) Mycobacterium tuberculosis infection is
common in pts with CFe) Pseudomonas aeruginosa is commonly
recovered from lung secretions in newly dx’d CF pts
Answer is A
CF is autosomal recessive, gene on chromosome 7
Incidence highest within white populations of north America and northern Europe (1 in 3000 live births). Prevalence is 1 in 17,000 live births for African-Americans
Most dx’d during childhood, but 7% of cases dx’d in US after age 18
Initially, most common organisms isolated from lung secretions are S. aureus and H. flu. After repeat abx exposure, Pseudomonas aeruginosa becomes predominant in the lower respiratory tract. Aspergillus fumigatus is commonly found in sputum
TB rare, but 10%-20% have non-tuberculous mycobacteria
Earliest CXR abnlity is hyperinflation, sec to small airway obstruction
The most severe lung changes occur in the RUL. PTX and hemoptysis are other complications that can occur. Ultimately bronchiectasis and bronchiolectasis
Lung tx is done for pts with respiratory failure who have failed medical mngmnt
For a previously healthy toddler with mild croup, the administration of oral dexamethasone:
a) is indicated only for moderate-to-severe croup, because mild croup is self-limited
b) is indicated only if the parents are unable to provide cool mist at home
c) is precluded by an unacceptably high rate of uncontrollable vomiting after administration
d) leads to mild hyperactivity that interferes with normal sleep patterns
e) leads to quicker resolution of symptoms when compared with observation

Answer is E
Croup is a respiratory illness characterized by inspiratory stridor, barking cough, hoarseness. Children 3 months to 3 years of age are most commonly affected. Cause is parainfluenza virus.
Steroids and nebulized racemic epinephrine for medical management (since 1980’s). Which has decreased the number of hospital admissions (from 2.8 to 2.1 per 1000 in children <1 yo and 1.8 to 1.2 per 1000 for children 1-4yo when comparing the time periods 1979-1982 vs 1994 to 1997).
Dexamethasone dosing is 0.6 mg/kg to a maximum of 10 mg.
Geelhold et al. (1995), studied n=120 ed peds pts of a tertiary pediatric hospital in a double blind randomized control trial. They showed that there was no difference in duration of hospitalization, reduction in croup score or need for nebulized epinephrine in the 3 single dose dex groups (0.15 mg/kg, 0.3 mg/kg, or standard 0.6mg/kg). They concluded that dex 0.15 mg/kg was as effective as 0.3 or 0.6 mg/kg dex.
Racemic epinephrine dosing is: 0.05 ml/kg per dose, maximum of 0.5 ml of a 2.25% solution. Dilute the epi to a volume of 3 ml with NS, give over 15 minutes.
PEER VII notes 3 trials which are relevant:
Bjornson et al performed double-blind randomized placebo-controlled trial of single dose dex for mild croup. N= 720. Found that PO dex led to fewer returns for medical care, quicker res of croup symptoms, less lost sleep, less parental stress than placebo. Although croup is self-limited, this study showed that kids with mild croup benefited from dex
Donaldson et al compared IM dex to oral dex for tx of mod/severe croup n=96. Parental assessment of sx’s at 24 hours was similar in the 2 groups, suggesting that po vs im results were comparable
Emesis was not reported as an impediment to po dex in the above studies
Neto et al performed a randomized, controlled trial of cool mist vs none, n=71 in moderate croup pts in the ED. No clinically significant difference was noted. Although historically considered an important tx, cool mist is clinically ineffective and does not influence the decision to tx with dex
A 3 year old boy presents with an intermittent nonproductive cough for the past 2 days. The mother reports that the child has been afebrile, well appearing, playful, eating normally, and has no change in toileting habits. The mother requests a note to allow her son back into preschool. On PE, the boy is afebrile, smiling, well appearing, playful, and has just a hint of wheezing on the right that seems to clear with coughing. His room air oxygen saturation is 99%, and his respiratory rate and work of breathing are normal. Cxr is obtained.
Which of the following is the most appropriate management plan?
a) administer a beta-agonist by MDI and observe for 6 hoursb) arrange for bronchoscopy within the next 24 hours, even if transfer
is neededc) initiate immediate respiratory precautions and admit to the PICUd) insert a thoracostomy tube after providing sedation and admit to the
hospitale) write the note as requested, prescribe cough medicine, and d/c
home
Answer is B
Above presentation is typical for aspirated FB
Dramatic, life-threatening presentations of complete airway obstruction can occur, but more commonly children have more subtle signs/symptoms
Clues include: onset while eating, mild asymmetry of breath sounds, persistent cough, lack of fever. On CXR air-trapping may be seen (right is more common). With inspiration, symmetric expansion will be appreciated. But with exhalation, the affected side (usually right) will be relatively expanded when c/w unaffected side
85% of FB aspirations are radiolucent
Bronchoscopy is needed for definitive dx. Transfer pt if not available at your institution
Beta agonist will not help, b/c bronchospasm is not the problem
No respiratory isolation, no admission to PICU
Chest tube not indicated: no ptx, no hemothorax, etc...
Child at risk for post obstructive pna and fibrosis from reaction to FB which could lead to open thoracotomy and partial lobectomy
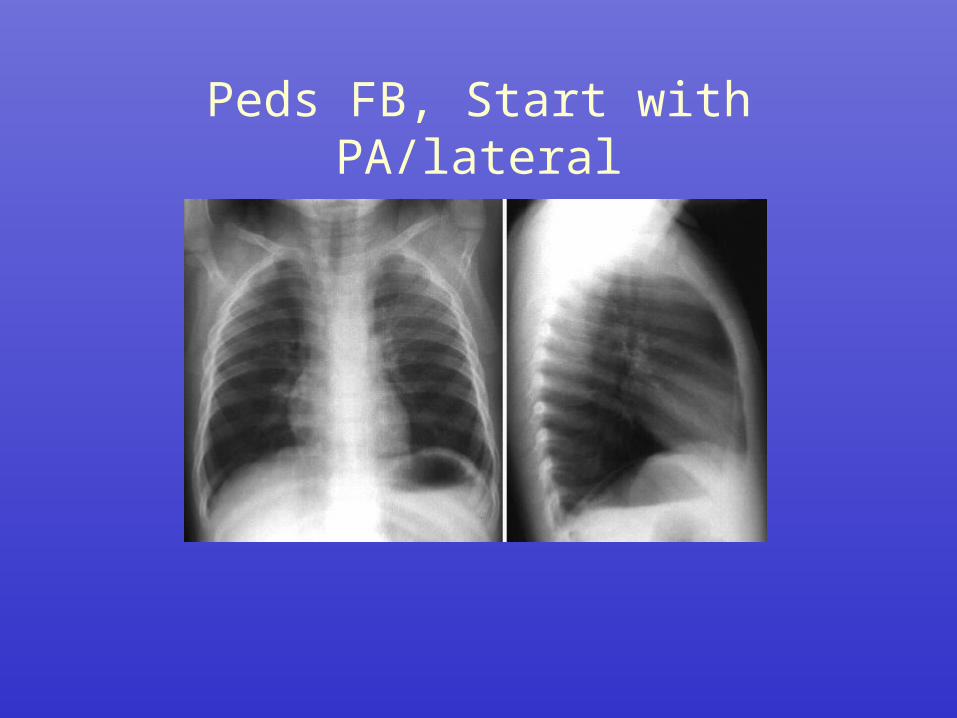
Peds FB, Start with PA/lateral
CXR is normal
Next step is to obtain an expiratory film, if patient is cooperative
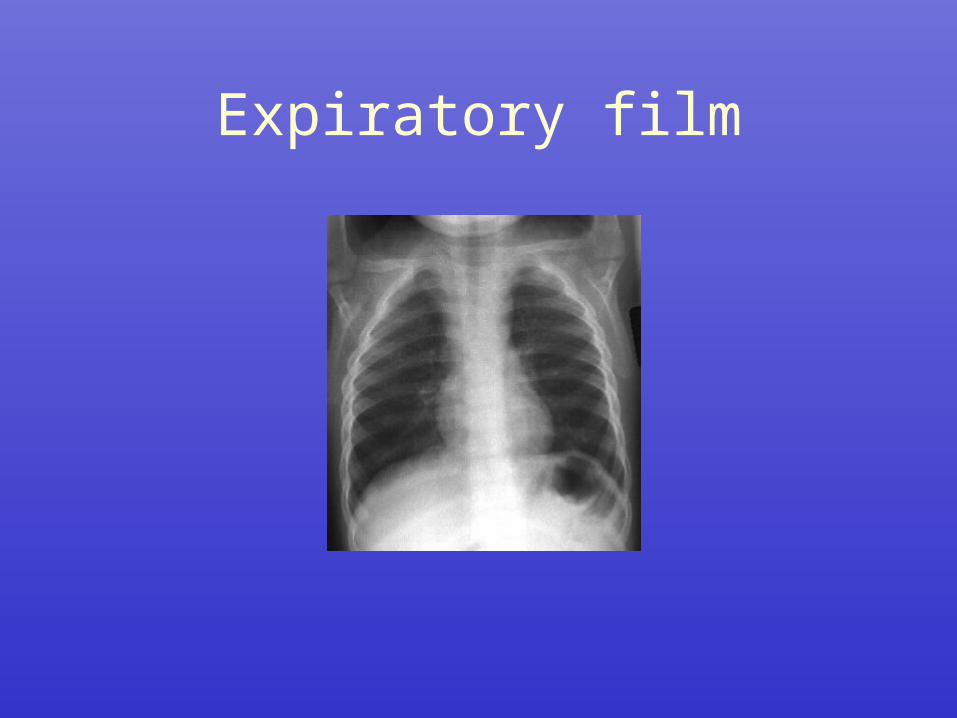
Expiratory film
This expiratory film is negative
Look for symmetry in the lung fields
Expect bilateral lower lung volumes (because of expiration)
If a FB is present, air trapping would occur and you would see air trapping on the side of the FB
A negative expiratory film does not r/o FB.
Next, obtain right and left lateral decubitus films
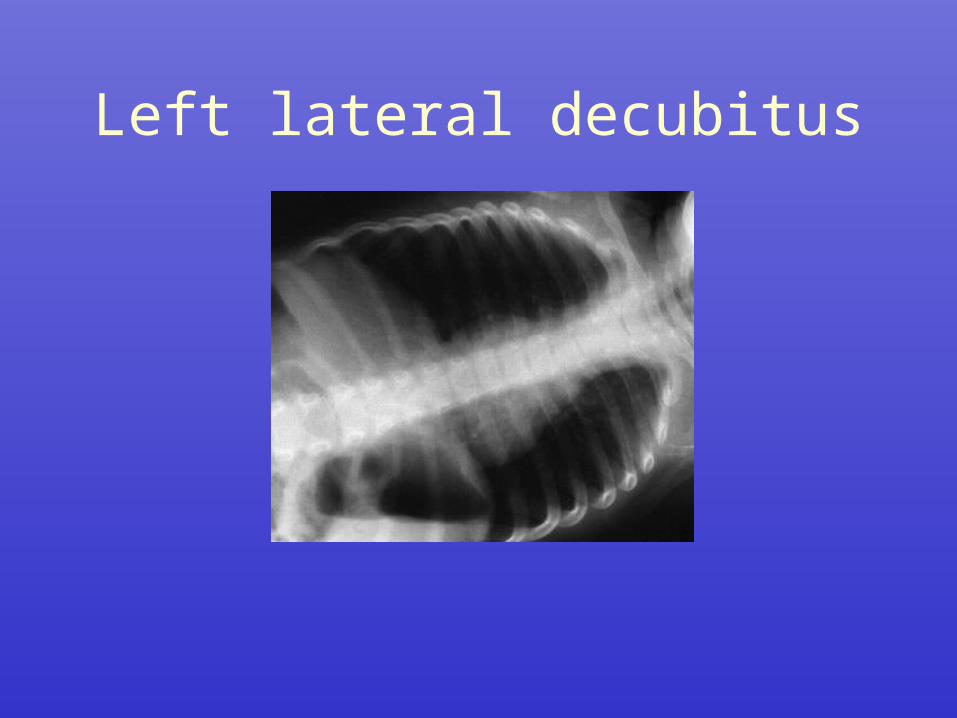
Left lateral decubitus
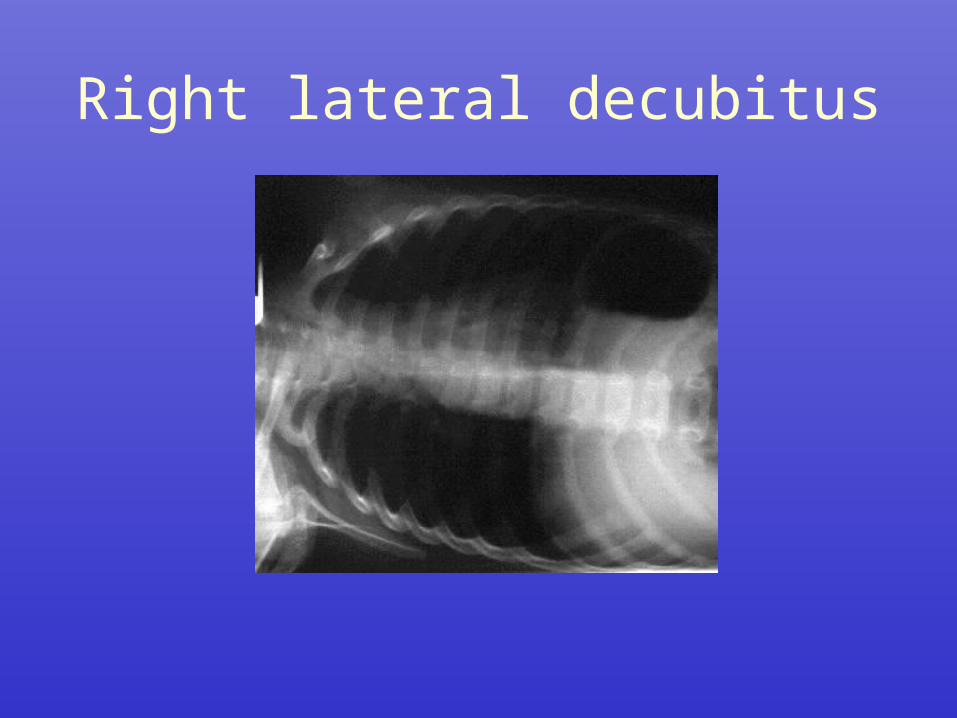
Right lateral decubitus
On decubitus films, the dependent lung should be less inflated c/w the other side
Although it is difficult to see, these films were interpreted as abnl. Both dependent lung fields were slightly more inflated than would be expected
And bilateral FB’s were found at bronchoscopy
If decubitus films are negative, next step is bronchoscopy
Transfer your patient to another hospital if unavailable at your institution

Miscellaneous

Which of the following drugs is FDA approved for the tx of intractable hiccups?
a) baclofen
b) chlorpromazine
c) metoclopramide
d) nifedipine
e) valproic acid
Answer if B
Hiccups are characterized as either acute (benign, self-limited) or chronic (persistent, intractable)
Acute causes: gastric distention (from food, drinking, air), etoh intoxication, excessive smoking, sudden change in environmental temperature, psychogenic events (stress)
Chronic hiccups: vagal or phrenic nerve irritation, CNS structural lesions, metabolic conditions (uremia, hyperglycemia), general anesthesia, surgical procedures (thoracic, abdominal, prostate, urinary tract, craniotomy)
FB, a hair within the external auditory canal pressing against the TM can also cause hiccups, via stim of the auricular branch of the vagus nerve
Steroids and bzd can induce hiccups
Chlorpromazine (thorazine) is the only drug with FDA approval for intractable hiccups, 30 min onset, a/e of extrapyramidal symptoms and hypotension
Metoclopramide (reglan) may be helpful, a/e of extrapyramidal symptoms
Nifedipine, valproic acid, and baclofen have also been advocated. Less a/e, slower onset
Which of the following conditions can result in pseudocyanosis?
a) cold exposure
b) hemochromatosis
c) methemoglobinemia
d) PE
e) Sulfhemoglobinemia
Answer is B
Cyanosis occurs when inadequately oxygenated blood perfuses peripheral tissues and end organs. It results in a blue or purple discoloration of the skin and mm.
The absolute amount of deoxygenated hgb is the determinant of cyanosis, not the amount of oxygenated hgb
Cyanosis: central or peripheral
Central: hypoxemia, anatomic shunts, or abnl hgb (e.g., high altitude, v/q mismatch, r to l shunt, methgbemia, sulfhgbemia)
Peripheral: vasoconstriction and reduced flow of normally oxygenated hgb. (e.g., low output states: shock, lv failure, cold exposure, arterial occlusion, pvd, venous obstruction
Pseudocyanosis: abnl skin pigmentation, no hgb abnlities (e.g., hemochromatosis, Ag, Au, Pb, As, or meds: phenothiazine, minocycline, amio, chloroquine). No blanching on physical exam
Chrysiasis, a/e gold tx. Permanent gray, blue or purple pigmentation of skin exposed to light
Argyria: from chronic ingestion or local application of silver salts or colloidal silver.
A 42 year old man involved in a MVC presents with severe SOB. He has ecchymosis over the left upper chest wall area. VS are BP 90/50, pulse rate 92, respiratory rate 28, temperature 36.7 c (98.1 f), and pulse oximetry 82% on RA. The nurse’s note says that the pt is cyanotic. Which of the following sites should be checked to confirm cyanosis?
a) conjunctivaeb) earlobesc) nail bedsd) tonguee) uvula
Answer is D
Greater than 4 to 5 g/dL of deoxygenated hgb in whole blood can cause visible cyanosis. Methgbemia and sulfhgbemia produce cyanosis at much lower concentrations 1.5 g/dL and 0.5 g/dL respectively
On exam, the tongue is considered one of the most sensitive sites for observing central cyanosis. Earlobes, conjunctivae, and nail beds are much less reliable
With ABG remember need co-oximetry b/c can get false high in certain states such as methgbemia, Conventional ABG analyzer calculates o2 sat from the dissolved o2 tension (pao2) which is normal in methgbemia. Co-ox can differentiate between oxy-, deoxy-, met- and carboxy- hgb molecules. Co-ox cannot differentiate between met- and sulf -hgbemia
Which of the following statement regarding ABG measurements is correct?
a) air bubbles with the syringe lower the pHb) co-oximetry allows identification of
sulfhemoglobinc) excess heparin within the syringe affects only
pH and Pco2d) the blood gas analyzer warms the blood to 37
c (98.6) prior to analyzinge) the conventional blood gas analyzer directly
measure the oxygen saturation
Answer is D
ABG syringe should be preflushed with heparin to allow a/c of 2-4 ml of blood. Too much heparin can distort pH, PO2, PCO2 and hgb
Syringe should be free of air bubbles, b/c they can result in lower PCO2 and elevated pH and PO2 levels
ABG on ice, read within 10 minutes
The ABG machine does warm the blood to 98.6 F. This process increases the partial pressure of dissolved gases and results in a falsely higher PO2 and PCO2 and lower pH.
O2 sat is calculated from measure PaO2.
Thank you for your attention.
Questions?