Embed Size (px)
Citation preview

Ala’a Al-johani
Tufol Al-zaid
Peptic ulcer disease
(PUD)

objectives:
Definition and pathophysiology.
Causes and risk factors.
Site.
Clinical picture.
Differential Diagnoses
Investigation.
Treatment.
Complication.

Case:
45 year Saudi female complain of Rhumatoid
Arthritis for 10 years ,she is on
methotrexate, naproxen came to Dr.Tufol
complain of recurrent epigastric pain 3-4 hs
after eat and weight gain.

Peptic ulcer disease (PUD) is a common disorder that affects
.millions of individuals worldwide
In the United States, PUD affects approximately 4.5 million
people annually. Approximately 10% of the US population
has evidence of a duodenal ulcer at some time.
The frequency of PUD in other countries is variable and is
determined primarily by association with the major causes of
PUD: H pylori and NSAIDs

Peptic Ulcer
An ulcer of the alimentary tract mucosa, usually
in the stomach or duodenum, & rarely in the
lower esophagus, where the mucosa is exposed to
the acid gastric secretion

Pathophysiology:

Causes:
The two most common causes of PUD are:
Helicobacter pylori infection ( 70-80%)
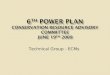
Non-steroidal anti-inflammatory drugs
(NSAIDS)
Other uncommon causes include:
• Gastrinoma (Zollinger-Ellison
syndrome) (Gastrin secreting tumor)
•Stress ulceration (trauma, burns,
critical illness)
•Viral infection.
•Chemotherapy -Radiotherapy

:Effect of NSAID on GI mucosa


Is there any genetic role in peptic ulcer?
More than 20% of patients have a family history of duodenal
ulcers, compared with only 5-10% in the control groups. In
addition, weak associations have been observed between
duodenal ulcers and blood type O.
A rare genetic association exists between familial
hyperpepsinogenemia type I (a genetic phenotype leading to
enhanced secretion of pepsin) and duodenal ulcers.

risk factors:
Age > 65 years (3.5-fold increased risk)
Alcoholic
Smoking
Past history of peptic ulcer
concomitant corticosteroid use
High dose or multiple NSAID
Medical diagnosis and management (short text book)
Mohmmad inaam danish
2009

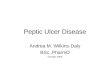
Site:
90-95% of duodenal ulcer occure
in the first portion of dudenum
in the anterior wall
duodenum
More than 90% of gastric ulcer
occur in the lesser curvature
Stomach
In reflux oesopgagitis esophagus
In Zollinger-Elison syndrome jejunum
Which contains ectopic gastric
mucosa
Meckle’s diverticulum

Case simulation

• Investigation
I
• observation
O
• Prevention
P
• Advice
A
• Prescription p
• referral
R
• clarification
C
• reassurance
R

Clinical picture

Clinical picture
Epigastric pain
The most common symptom of both gastric and duodenal ulcers.
It is characterized by burning sensation. Pain with radiation to the back is suggestive of a
posterior penetrating gastric ulcer . Abdominal pain is absent in 30% of older patient
with PUD.
2013 , 22 dateNov Upto
2007,01 octAFP

Clinical picture
epigastric pain
Food and antacid provide minimal
relief of pain.
Occurs shortly after meals
Pain not increase at nght.
Gastric ulcer
Food and antacid relief the pain.
Occurs 3-4 hours afterward
Pain awaken patient at night.
Duodenal ulcer
2013 , 22 dateNov Upto
2007,01 octAFP

Clinical picture
Other symptoms of PUD
Dyspepsia , bloating and distention.
Heartburn.
Chest discomfort.
Vomiting.
Fatty food intolerance.
Weight loss due to fear of food is a characteristic
of gastric ulcer.
2013 , 22 dateNov Upto
2007,01 octAFP

Clinical picture
(red flags):
Alarm features that warrant prompt gastroenterology referral:
Hematemesis or melena
hematochezia.
anemia .
Sudden onset of symptoms witch may indicate perforation.
Early satiety.
Recurrent vomiting
Unexplained weight loss
Family history of gastric ulcer.
Medscape Jun 7, 2012

Differential Diagnoses

Differential Diagnoses
Abdominal Aneurysm.
Cholangitis.
Cholecystitis.
Cholelithiasis.
Diverticular Disease.
Esophageal Perforation, Rupture and Tears.
Esophagitis.
Gastritis.
Gastroenteritis.
Gastroesophageal Reflux Disease.
Inflammatory Bowel Disease.
Viral Hepatitis.
Medscape Jun 7, 2012

investigations

Investigation
There are two major considerations in diagnosis of
peptic ulcer disease (PUD):
1. Investigations needed to establish diagnosis of
PUD.
2. Investigation needed to diagnose a cause (
H.pylori infection).
Uptodate Dec 03, 2013

Investigation
FIRST, diagnostic studies in patients who may have a peptic ulcer:
blood tests.
endoscopy (EGD):
1. Detection of ulcer disease ("gold" standard test )
2. Differentiation of benign gastric ulcers from cancer :
Benign ulcers have smooth, regular, rounded edges, with a flat, smooth ulcer
base often filled with exudate
Benign ulcer The ulcerated mass protrudes into
the lumen
The folds surrounding the ulcer crater are nodular
The margins are overhanging, irregular, or thickened
Malignant ulcer
Uptodate Dec 03, 2013

Investigation
Cont. Endoscopy:
3. Follow-up endoscopy to exclude malignant GU.
barium radiography:
1. Detection of ulcer disease
2. differentiation of benign versus malignant lesions:
Uptodate Dec 03, 2013

Investigation
SECOND, HELICOBACTER PYLORI TESTING:
Serology: serum antibody detection, it
is useful only for initial testing ,cannot be
used to confirm eradication because test can
be positive for years even if the infection is
cured.
Urea breath test: can be used to confirm
eradication ( PPI therapy should be stopped
for two weeks before test).
Uptodate Dec 03, 2013

SECOND, HELICOBACTER PYLORI TESTING:
Stool antigen test:
This test can be used to
diagnose the infection
and confirm that it has
been cured after
treatment.
Endoscopic biopsy.
Uptodate Dec 03, 2013

Treatment

treatment First, Eradication of Helicobacter pylori :
Triple therapy:
Omeprazole (20 mg twice daily).
amoxicillin (1 g tewice daily) or metronidazole (500 mg twice daily) -if allergic to penicillin-.
clarithromycin (500 mg twice daily).
quadruple therapy:
Ranitidine bismuth citrate (400 mg twice daily ).
tetracycline (500 mg twice daily) .
metronidazole ( 250 mg four times daily) .
Omeprazole (20 mg twice daily) .
Uptodate april 25,2014

treatment
Second, Cytoprotective agents:
Misoprostol : it is a prostaglandin analog that can be
used to decrease the incidence of peptic ulcers and
complications in long-term NSAID users at high risk.
Sucralfate : it binds with positively charged proteins in
exudates and forms a viscous adhesive substance that
protects the GI lining against pepsin, peptic acid, and bile
salts. It is used for short-term management of ulcers.
Uptodate april 25,2014
Medscape jun 07,2012

treatment
Third, health education:
Not taking (NSAIDs), These include aspirin and ibuprofen .
Avoid steroids.
Quitting smoking.
No special diet is needed, avoid any food or beverages that may aggravate symptoms.
Fourth, surgery: Duodenal ulcer: truncal vagotomy, selective vagotomy, highly
selective vagotomy, partial gastrectomy
Gastric ulcer: partial gastrectomy with gastroduodenal or gastrojejunal anastomosis.
Uptodate april 25,2014
Medscape jun 07,2012

complication

complication
Perforation: more common in DU than GU, and
usually ulcer site is on anterior duodenal bulb.
Bleeding: more common in posterior ulcer (presence
of gastroduodenal artery).
Gastric outlet obstruction.
Malignancy: gastric ulcer have 2-4% risk of
malignancy, multiple biopsies are required at time of
endoscopy.
Uptodate april 25,2014
Medscape jun 07,2012

References…