Embed Size (px)
Citation preview

PSO TRAINING
ANXIETY & HOW TO MANAGE IT
BY PIP WALKERPOLICE PSYCHOLOGIST
S/HSO
JULY 2015

OUTLINE OF WORKSHOP1. Demystifying anxiety2. “Normal” Vs “Pathological” Anxiety3. The development of Anxiety Disorders4. Different types of anxiety disorders5. Theoretical models to understand anxiety disorders6. Signs & symptoms of anxiety disorders to look out for7. Treatment/Interventions for managing anxiety
disorders8. Resources on anxiety disorders

Videos about the Impact of Anxiety on people’s lives
ACTIVITY: Discuss thoughts/reflections from videos

QUIZ:
UNCOVERING THE MYTHS OF ANXIETY!

WHAT IS “NORMAL” ANXIETY?
Psychological & physiological state characterised by physical, emotional, cognitive & behavioural components
Normal, adaptive response to perceived or actual threat – everyone gets anxious occasionally
Time limited, transient Can be beneficial Doesn’t usually interfere with daily functioning or
achievement of goals
Anxiety Vs Fear
Fear – concrete danger occurring at present time
Anxiety – perceived or actual threat that is occurring in future; usually a FALSE ALARM
Fight or flight response is the inborn, primitive, automatic, survival FEAR response to a perceived or actual threat, or the absence of people or objects that signify safety

WHEN “NORMAL” ANXIETY DEVELOPS INTO AN ANXIETY
DISORDER
Anxiety becomes “pathological” or “abnormal” and can turn into an Anxiety Disorder when it: Increases in excessive rates of:
Duration Intensity Frequency
Causes significant distress Impairs daily functioning & decreases quality of life Is disproportionate to the situation that elicited the anxious response Leads to irrational, illogical thinking & behaviour Is associated with maladaptive coping (e.g., avoidance, withdrawal)

ANXIETY DISORDERS
Often have an early onset - teens or early twenties
Show 2:1 female predominance
Have a waxing and waning course over lifetime

TYPES OF ANXIETY DISORDERS

THEORETICAL MODELS TO UNDERSTAND ANXIETY
Biopsychosocial Model
Multiple, inter-related causes of pathological anxiety: Biological Psychological Social (environmental)

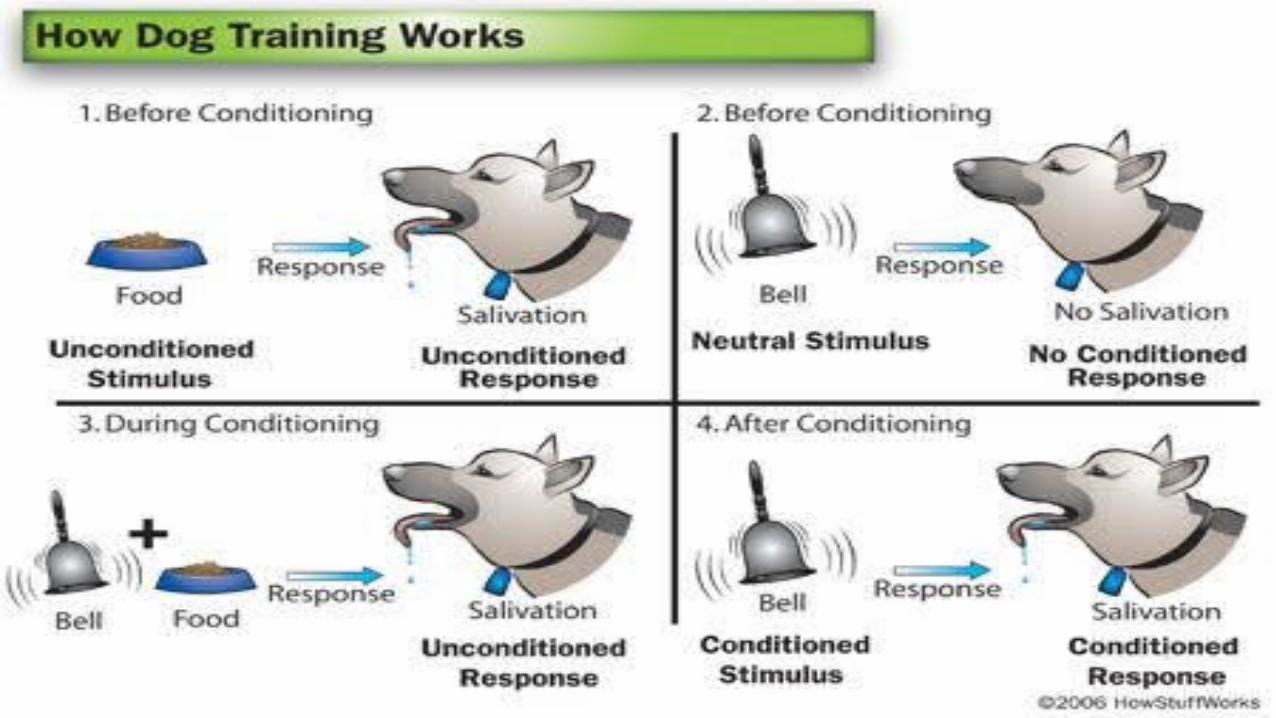
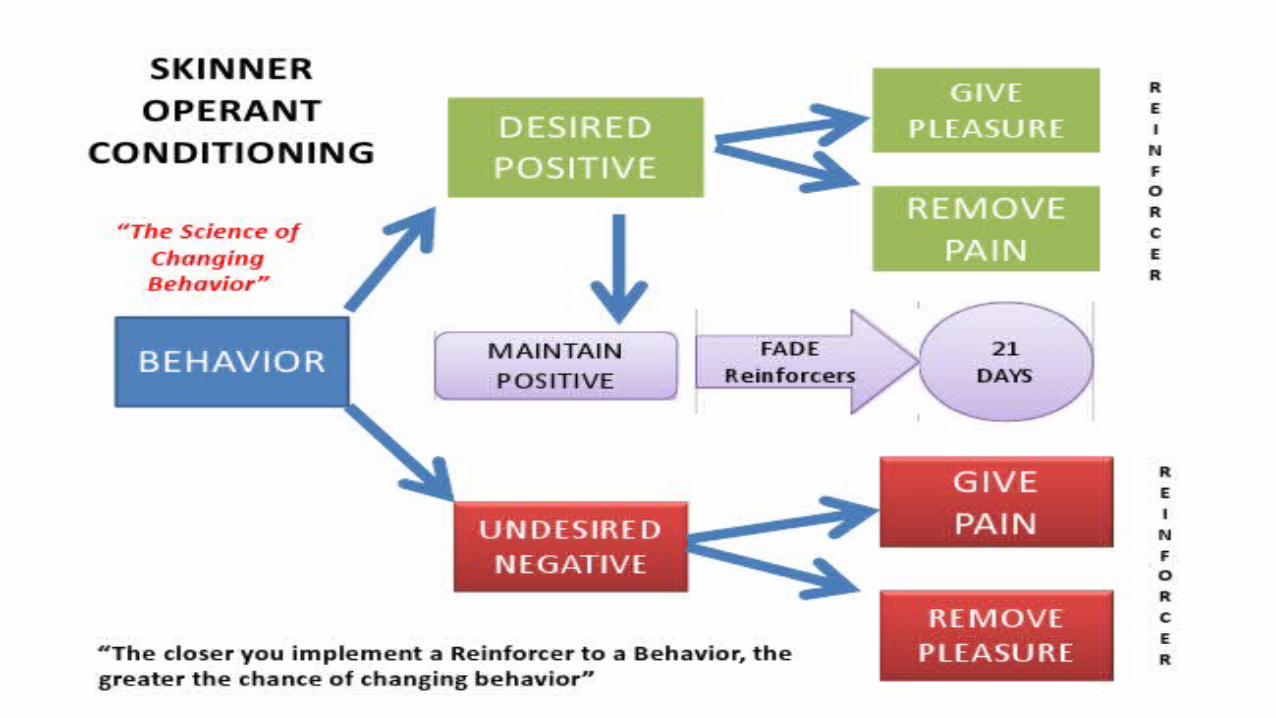
Behaviourism – Learning Theory Model
Focuses on observable behaviours
Behaviours linked to anxiety and/or phobias are learned through classical conditioning and maintained through operant conditioning.
Pavlov’s Dog Experiment – Classical Conditioning
Skinner – Operant Conditioning


Biological/Neuroscience model

1st Brain: Reptilian
Reptiles Reflex/Instinct Low level control Motor control (breathing, heartbeat & motor skills)
2nd Brain: Limbic system
Mammalian Emotions Reactionary (Fight/Flight, Pleasure/Reward & pain)

3rd Brain: Thinking
Human Foresight High level control / Executive Functioning
(Thinking - Reasoning, judgment, perception, motivation, memory & learning)

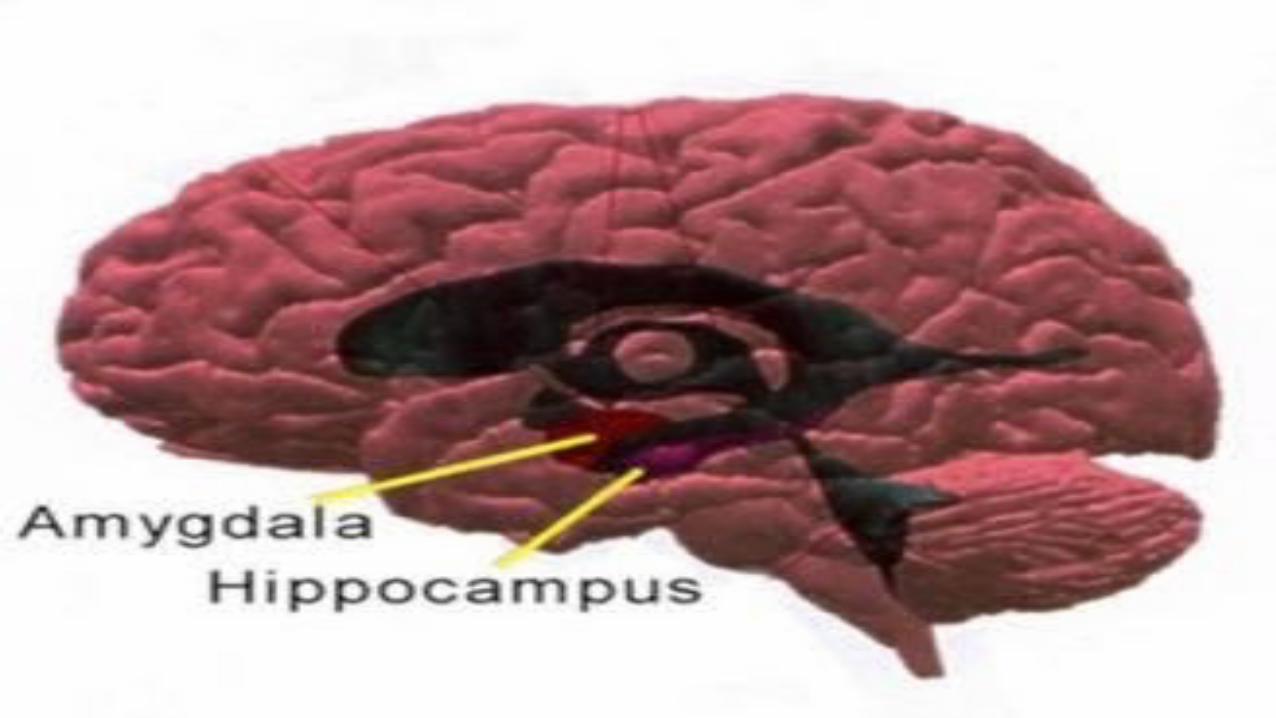
Amygdala & Hippocampus are the two main parts of the brain involved in anxiety.
Amygdala Almond-shaped structure that begins functioning before
birth. If something is perceived as a threat, the amygdala
activates the Fight or Flight Response
Hippocampus Assesses the accuracy of the threat after the fight or flight.
Our brains are wired to “shoot first, ask questions later!” Records and stores memories


Fight, Flight or Freeze Response We are wired to avoid fear/pain/discomfort more than we are to
seek pleasure. The neo-cortex is usually aware that there is no real threat, but the
deeper, primitive parts of the brain respond as if survival is at stake. “Fight” is about destroying the threat. “Flight” is about getting out of the way, running away or avoiding the
threat. “Freeze” is an optional third response: remaining still. It takes 15-30 minutes to reduce heightened threat arousal back to
‘normal’/homeostasis, if the process isn’t short circuited by the relaxation response (e.g., deep breathing).




WHAT CAUSES ANXIETY DISORDERS
Often a combination of factors lead to a person developing an anxiety disorder: Genetics Ongoing stressful events e.g.:
Job stress or job change Change in living arrangements Pregnancy and giving birth Family and relationship problems Major emotional shock following a stressful or traumatic event Verbal, sexual, physical or emotional abuse or trauma Death or loss of a loved one.

Physical health problems Hormonal problems (e.g. overactive thyroid) Diabetes Asthma Heart disease.
Substance use Personality factors
- Perfectionists, - Unrealistic expectations - Low self-esteem - Lack of assertiveness - Pessimism - Low tolerance of ambiguity or uncertainty, - External locus of control

SIGNS & SYMPTOMS OF ANXIETY DISORDERS
See Handout for details

TREATMENT/INTERVENTIONS FOR ANXIETY DISORDERS
Early intervention is essential - recognise the signs and symptoms and encourage people to seek support early
The sooner a person seeks help, the sooner they can recover Anxiety disorders are unlikely to go away on their own. If
ignored and left untreated, anxiety disorders can last for months, or years, and have far reaching negative effects on a person’s life and their loved ones.
Encourage the person to seek support from their family, friends and local community.

1. Physiological – Symptom Control Medication (Anti-depressants, PRN Benzodiazepines), if necessary –
refer to GP or Psychiatrist Self-monitoring of anxiety symptoms (e.g., symptom diary) Self-care/Stress Management:Minimum of 20 mins exercise per day (natural anti-depressant/anti-
anxiety drug - alters levels of chemicals in the brain, such as endorphins and stress hormones).
Balanced DietAdequate Sleep HygieneReduce or avoid stimulants (e.g., coffee, tea, alcohol)Delay making major life changes or decisions, if possibleSchedule pleasurable activitiesRelaxation training



Relaxation Training Diaphragmatic breathing – Using the diaphragm to slow down & deepen
the breath, relax the autonomic, sympathetic nervous system & prevent hyperventilation. Excellent for managing anxiety and panic attacks. Requires lots of practise.
Progressive Muscle Relaxation (PMR) - Learn to monitor & distinguish between relaxed & tense muscles in the body. Good for managing muscle tension and headaches. Simple & easy.
Guided visual imagery – Utilises visualisation & the remaining senses to imagine being in a relaxed place – a powerful way to enter a relaxed state. Similar to self-hypnosis & visualisation.
Grounding/mindfulness – Learn to manage difficult and distressing thoughts, focus on the present moment in a non-judgmental manner, the mind-body connection. Excellent for managing overwhelming anxiety/distress/panic. e.g., 5 senses mindfulness meditation, mindfulness of the breath, body scan. Requires practise.

2. COGNITIVE BEHAVIOURAL – ALTERING BEHAVIOUR & PERCEPTION

BEHAVIOURAL THERAPY
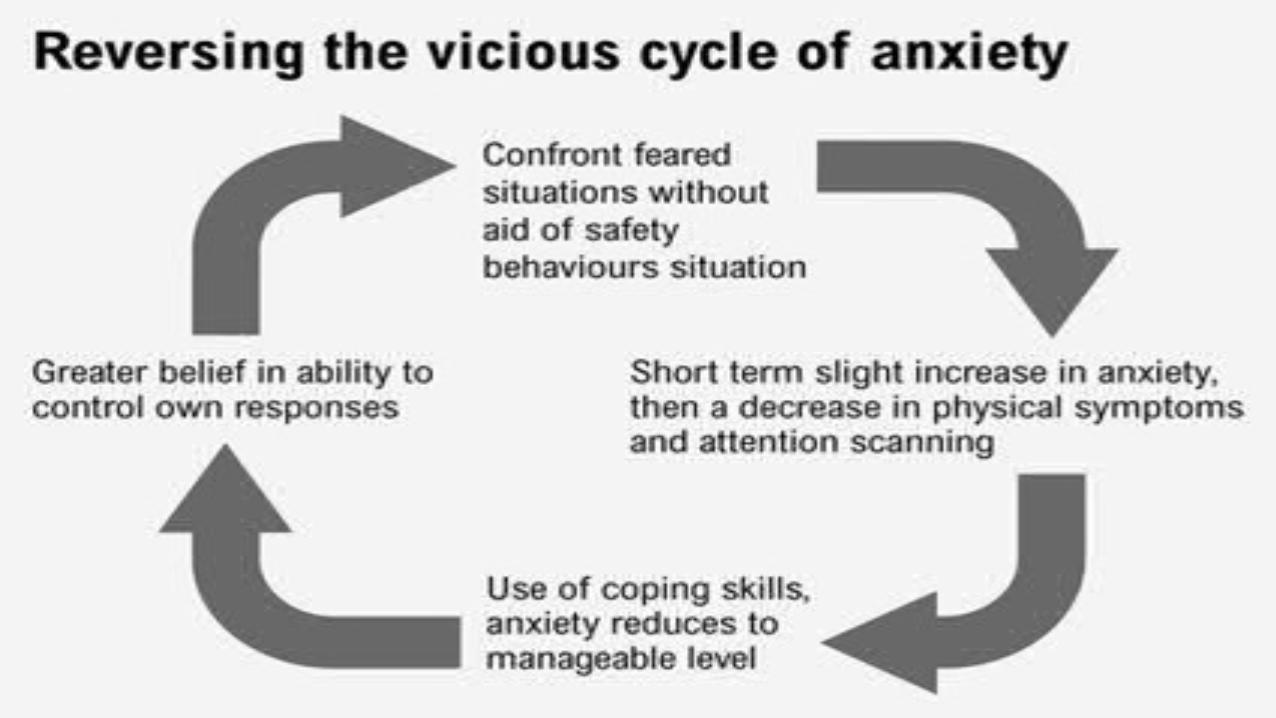
Exposure & Response Prevention: Anxiety should subside after gradually exposing
person to their fears until their behavioural and sensory response diminishes over time, after repeated exposure to feared stimulus (Habituation).
Refraining from undesirable behaviour (e.g., compulsions/rituals, avoidance, escape, safety behaviours).
Excellent for OCD, Panic Disorder with or without Agoraphobia, PTSD, Social Anxiety





CBT FOR ANXIETY IN A NUTSHELL Psychoeducation Behavioural therapy (e.g., Exposure & Response Prevention) Listen to, identify and challenge Negative Automatic Thoughts and self-defeating
core beliefs; Use Socratic questioning and reality testing to reframe perception of threat and appraisal of situations
Positive self-talk and coping statements Designated worry time Assertiveness training/Limit setting Incorporating mindfulness – focusing on the present moment, being non-
judgmental about thoughts and emotions, living an authentic life aligned with one’s true values

GENERAL TIPS ON HOW YOU CAN HELP STAFF WITH AN ANXIETY DISORDER
Have an RUOK conversation Let the person know if you’ve or their manager or colleague
has noticed a change in their behaviour. Spend time talking with the person about their experiences and
let them know that you’re there to be a support and listen without being judgmental.
Suggest the person see their GP or health professional (including HSO) and/or help them to make an appointment.
Offer to go with the person to the doctor or health professional. Help the person to find information about anxiety (e.g., library,
internet, HSO).

Encourage the person to try to get enough sleep, exercise and eat healthy food.
Discourage the person from using alcohol or other drugs to feel better. Encourage friends and family members to invite the person out and
keep in touch, but don’t pressure the person to participate in activities. Encourage the person to face their fears with support from their
doctor/psychologist. It would be unhelpful to:
- Put pressure on them by telling them to “snap out of it” or “get their act together”
- Stay away or avoid them - Tell them they just need to stay busy or get out more

VIDEO ACTIVITYhttp://learn.beyondblue-elearning.org.au/BeyondBlue/conversations/index.html
What symptoms of anxiety does Sarah seem to have?
If you were the PSO in this situation, what steps would you take to assist Sarah?
Reflections on approach that Sarah’s manager adopted

ANXIETY RESOURCES Websites: Beyond Blue Anxiety Australia Sane Mindspot Mental Health Online
Apps iCouch CBT Cognitive diary CBT Self-help Smiling Minds Self-help for Anxiety Management (SAM) eCBT Calm

Books:
The Anxiety and Phobia Workbook by Edmund Bourne Living with It: A Survivor’s Guide to Panic Attacks by Bev Bissett Overcoming Social Anxiety and Shyness: A Self-Help Guide Using
Cognitive Behavioral Techniques by Gillian Butler The Feeling Good Handbook by Dr David Burns The 10 best ever anxiety management techniques: Understanding How
Your Brain Makes You Anxious and What You Can Do to Change It by Margaret Wehrenberg
Get out of your mind and into your life by Steve Hayes
CDs:
Cancer Council Queensland Learning to Relax CD (FREE)