Embed Size (px)
Citation preview

Anxiety in Children and Adolescents: How to Manage those Worries and Fears
Isabel Rodriguez-Duncan, LCSW, Ed.S.Clinician, CCF
Topics to Cover① Introduction to who we are
② Overview of child anxiety
③ Description of specific anxiety disorders
④ Treatment techniques
⑤ Reinforcing the coping child
⑥ Overview of outcomes
⑦ How to Participate

The CCF
o Provide clinical treatments based in strong evidence for children and adolescents with mental and behavioral health problems
o Conduct top research in all areas of child and adolescent typical development and mental health problems
o Educate upcoming clinicians and researchers in the field
Who We are at the CCF
Who We Are at the CCFTreatment for infants through 17yo◦ ADHD
◦ Aggression
◦ Anxiety, fears, worries
◦ Autism
◦ Mood problems
◦ Learning difficulties
◦ Families in Transition from divorce/Couples Counseling
◦ Based in Behavioral and Cognitive methods
Who We Are at the CCF for AnxietyTreatment for 3-17yo
Use Best Practice Treatments◦ Supported by research◦ 8-16 sessions of Cognitive-Behavioral Therapy (CBT)◦ Attention-Bias Modification Therapy◦ Parent training component to treatment, more for younger children
Clinicians: ◦ Ph.D. level, licensed psychologists, licensed clinicians◦ Highly trained doctoral and masters level graduate students
(supervised)
Overview of Child Anxiety
Normal Fear and Anxiety or an Anxiety Disorder?
For most children and adolescents, fear and anxiety are experienced without great interference in everyday life
Anxiety is:◦ A natural emotion
◦ An enjoyable emotion for many children (e.g., scary movies, stories)
For some children, fears persist and interfere in daily functioning or in family functioning and disrupt normal development

Normal Fears & Worries vs.Anxiety Disorders
o Children’s fears are usually mild, transitory, can be adaptive, and are very common and normal
o HOWEVER, some children experience fears that persist, interfere with daily functioning, and are not age appropriate.
o When these fears become excessive, persistent, and cause psychological distress, and are not associated with an actual threat, treatment is necessary
Prevalence and SignificancePediatric anxiety disorders are common◦ 10-20% of children in the general population report
clinical levels of anxiety
◦ Relatively stable over time
◦ Associated with depressed mood
Pediatric anxiety disorders are impairing◦ Academic and social problems
◦ Predict future emotional health problems (if untreated)
Description of Specific Anxiety Disorders
Anxiety Disorders: Children and Adolescents
o Separation Anxiety Disorder
o Specific Phobias
o Social Phobia
o Selective Mutism
oGeneralized Anxiety Disorder
oObsessive-Compulsive Disorder
o Panic Disorder with or without Agoraphobia
Separation Anxiety DisorderPersistent fear of separation from caregiver
Repeated somatic complaints such as stomachaches, headaches
Reluctance or refusal to go to school, play dates, sleepovers, camp, birthday parties, etc. without a parent present
Symptom trends:◦ Ages 5-8: fears of harm befalling attachment figures,
nightmares, school refusal◦ Ages 9-12:excessive distress at separation◦ Ages 13-16: somatic complaints and school refusal
Specific PhobiaMarked and persistent fear that is excessive or unreasonable
Examples: animals, the dark, heights, thunder/lightening, shots/blood tests, doctors/dentists, vomiting, choking, etc.
Exposure to the phobic stimulus almost invariably provokes an immediate anxiety response, which may provoke a panic attack

Social PhobiaMarked and persistent fear of one or more social or performance situations in which the person is exposed to unfamiliar people or to possible scrutiny by others
What you might see:◦ Keeps to self in class
◦ Reluctant to answer questions
◦ Shyness around unfamiliar people
◦ Difficulty initiating conversations with peers
◦ Isolation in unstructured settings (lunch, recess)
Age Trends in Social PhobiaoMay begin as inhibited temperament in
preschoolers
oAssociated with selective mutism in young school-aged children
oHigher prevalence in postpubertal adolescents
o Retrospective reports of adults place age of onset in adolescence
Selective Mutismo Consistent failure to speak in social situations where there
is an expectation of speaking
o Failure to speak is not due to lack of knowledge of language

Generalized Anxiety DisorderExcessive anxiety and worry occurring more days than not for at least 6 months, about a number of events or activities
The worrying…◦ Is difficult to control
◦ May be associated with restlessness, fatigue, irritability, muscle aches, and sleep disturbance
What you might see:◦ The “worry-wart” (worry about school, performance, health,
personal safety)
◦ Perfectionism (on-time, need to keep schedule)
◦ Excessive reassurance-seeking and the “What ifs?”
◦ Difficulty with transitions/new situations
Obsessive-Compulsive DisorderObsessions and/or compulsions:◦ Recurrent and persistent thoughts, impulses or images that are
intrusive and cause marked anxiety or distress (obsessions)
◦ Child attempts to suppress such thoughts, or to neutralize them with a thought or action (compulsion)
◦ Distressing and time consuming (at least 1 hour per day)
What you might see:◦ Ordering and arranging of items
◦ Repeated checking (did I lock the front door?)
◦ Erasing and rewriting multiple times
◦ Excessive hand-washing
◦ Counting things over and over or special number of times
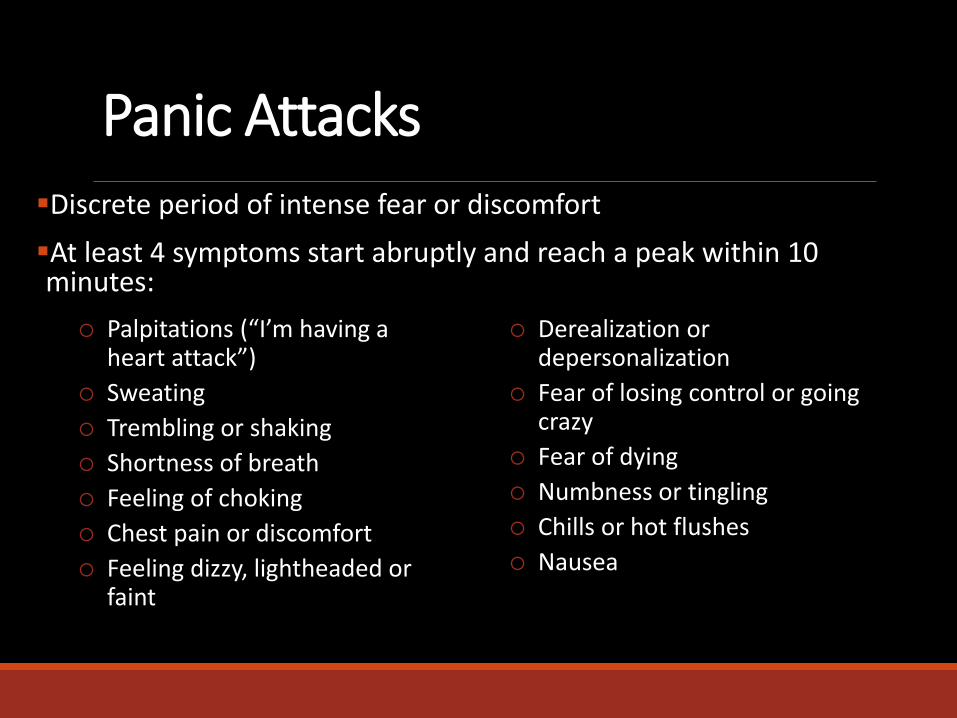
Discrete period of intense fear or discomfort
At least 4 symptoms start abruptly and reach a peak within 10 minutes:
Panic Attacks
Palpitations (“I’m having a heart attack”)
Sweating
Trembling or shaking
Shortness of breath
Feeling of choking
Chest pain or discomfort
Feeling dizzy, lightheaded or faint
Derealization or depersonalization
Fear of losing control or going crazy
Fear of dying
Numbness or tingling
Chills or hot flushes
Nausea
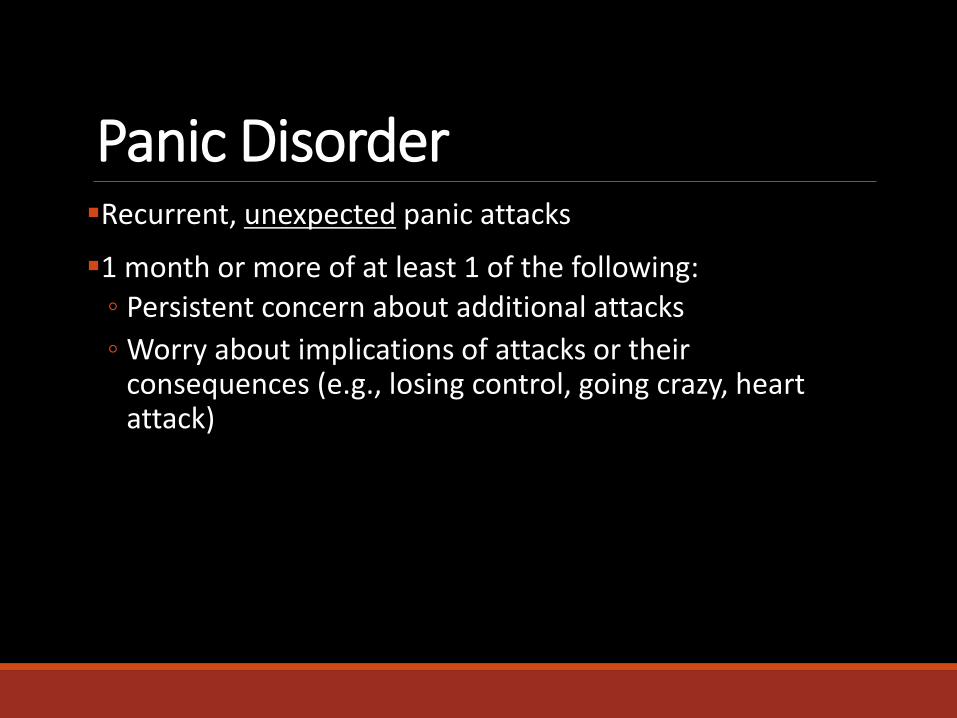
Panic DisorderRecurrent, unexpected panic attacks
1 month or more of at least 1 of the following:◦ Persistent concern about additional attacks
◦ Worry about implications of attacks or their consequences (e.g., losing control, going crazy, heart attack)
Rarely occurs in children <12

AgoraphobiaAnxiety about being in places/situations where, if an unexpected panic attack occurs:◦ Escape might be difficult or embarrassing◦ Help may not be available
These situations are:◦ Avoided or endured with marked distress or anxiety about
having an attack◦ Require the presence of a companion
Commonly Avoided Places◦ Classrooms, Crowded hallways, Cafeteria, Movie theater, Malls,
Open spaces

What to Do: Treatment Techniques
Cognitive-Behavioral Treatment

Cognitive-Behavioral Therapy is…oSkills-focused, goal-directive
oPresent and future-focused
oEmpirically supported (12-16 sessions)

Core Treatment ComponentsEducation about anxiety (fear, depression, etc.)
Relaxation (if applicable)
Cognitive Restructuring (“Detective Thinking”)
oExposure!!!
Situational Exposure

Education about Fear and AnxietyFear is…◦ Natural
◦ Necessary
◦ Harmless
Fear is designed to…◦ Draw our attention to an immediate threat
◦ Keep us safe by activating our fight-or-flight system
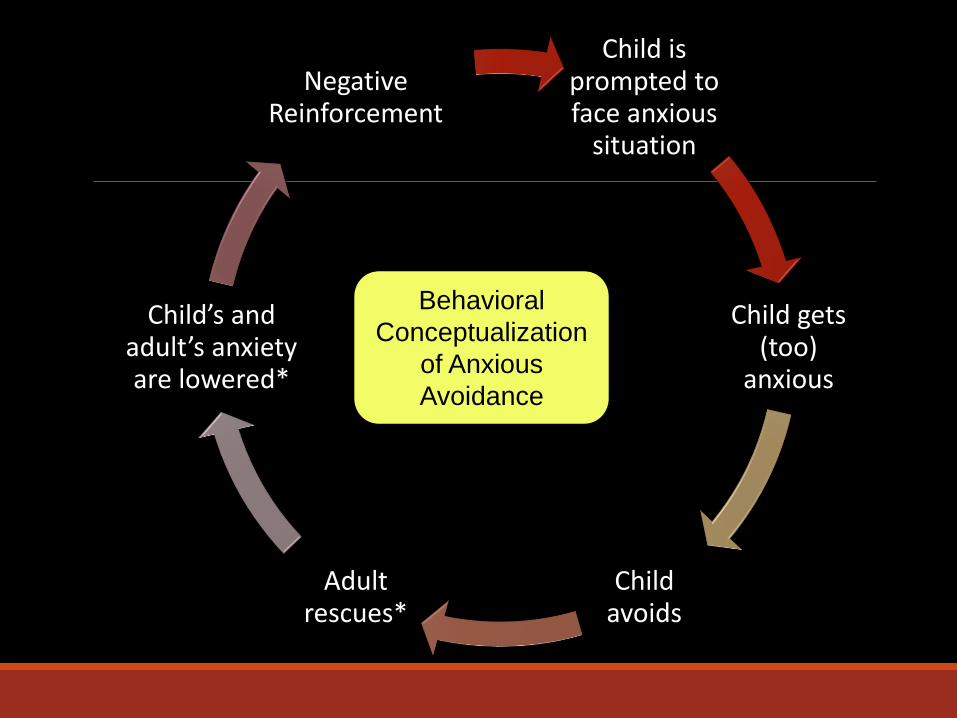
Child is prompted to face anxious
situation
Child gets (too)
anxious
Child avoids
Adult rescues*
Child’s and adult’s anxiety are lowered*
Negative Reinforcement
Behavioral
Conceptualization
of Anxious
Avoidance
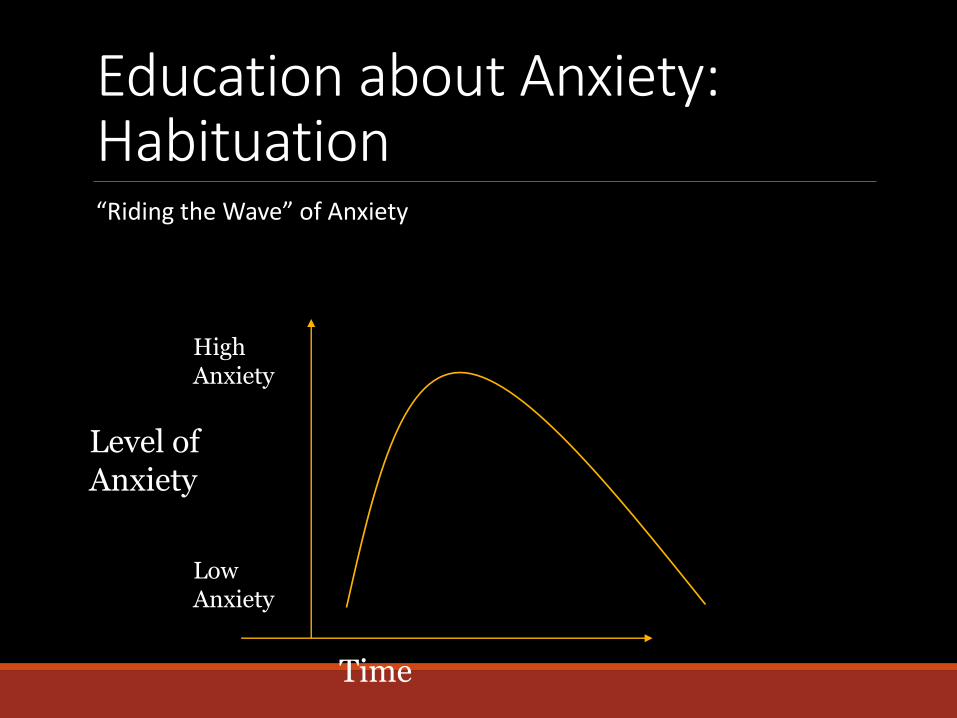
Education about Anxiety: Habituation“Riding the Wave” of Anxiety
Time
Level of Anxiety
Low Anxiety
High Anxiety
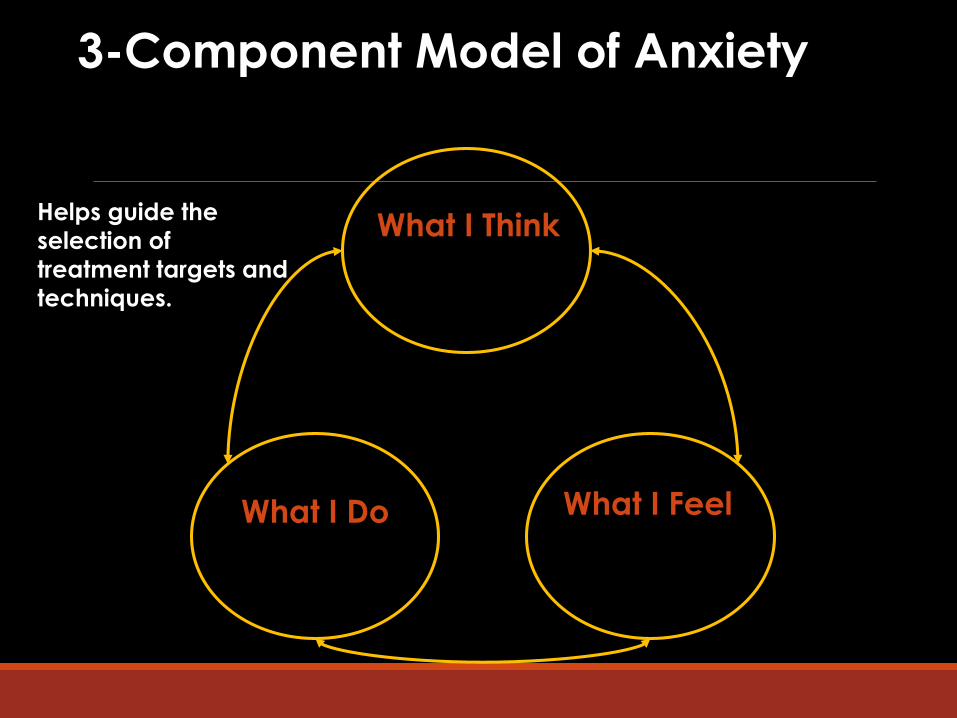
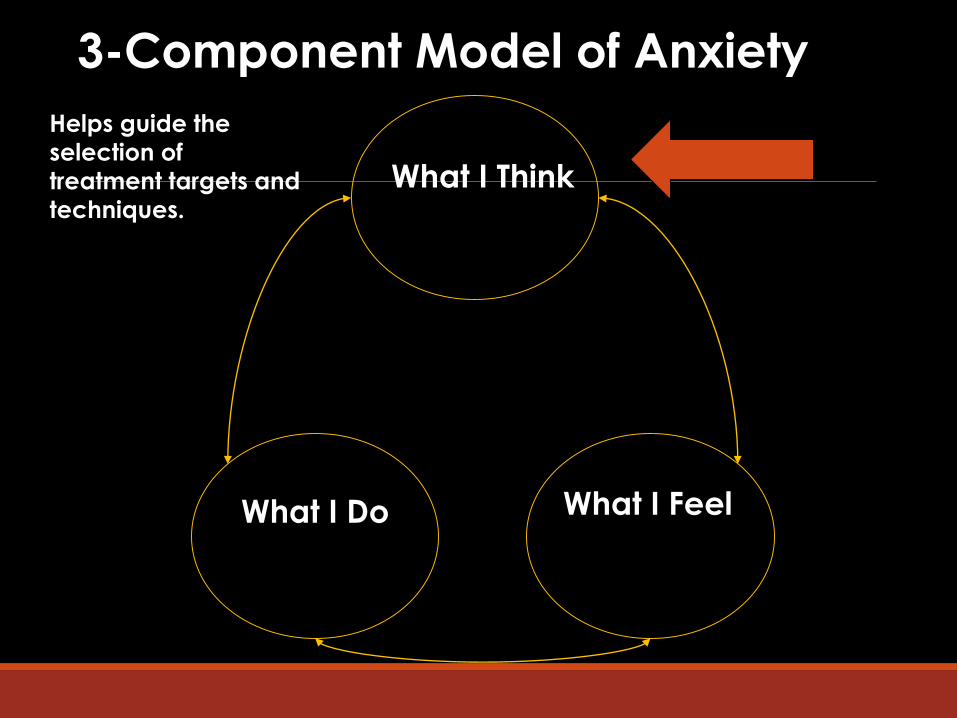
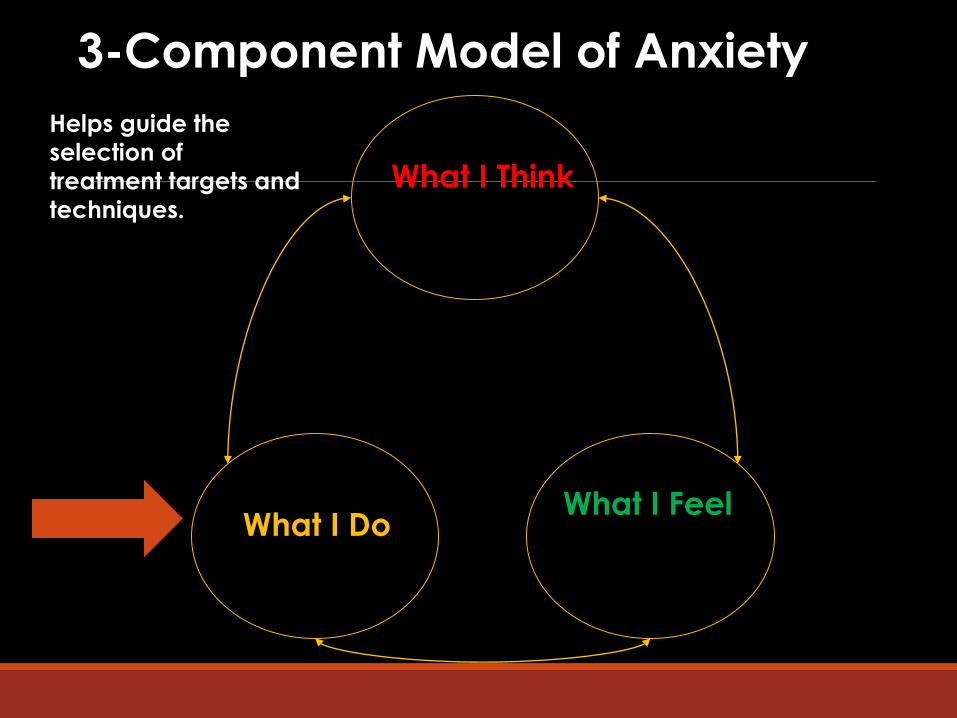
3-Component Model of Anxiety
What I Do What I Feel
What I ThinkHelps guide the
selection of
treatment targets and
techniques.
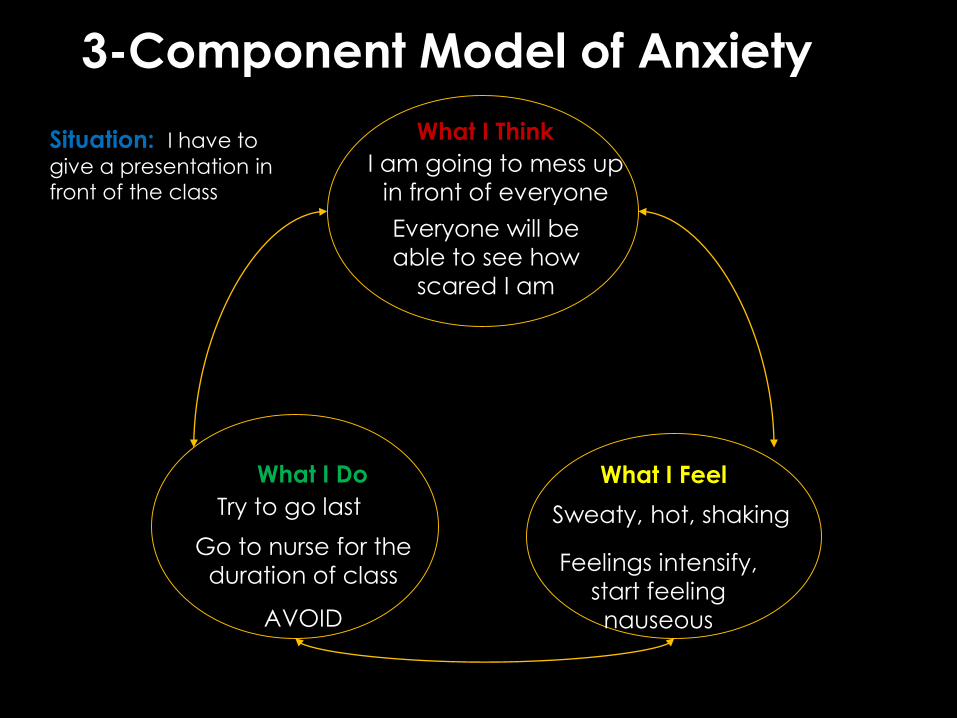
3-Component Model of Anxiety
What I FeelWhat I Do
What I Think
Sweaty, hot, shaking
Situation: I have to
give a presentation in
front of the class
I am going to mess up
in front of everyone
Everyone will be
able to see how
scared I am
Try to go last
Feelings intensify,
start feeling
nauseous
Go to nurse for the
duration of class
AVOID
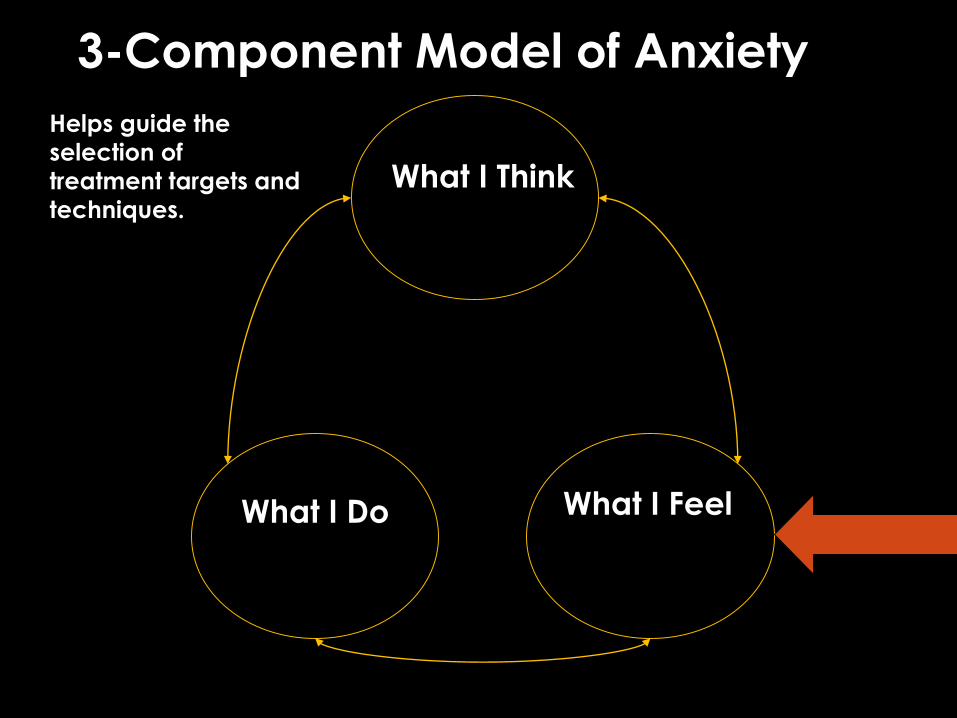
3-Component Model of Anxiety
What I Do What I Feel
What I Think
Helps guide the
selection of
treatment targets and
techniques.

Recognizing & Labeling Feelings
Child learns to recognize and label different emotions
Use body language, facial expression, and tone of voice
------------------
Magazines
Feelings Collage
Feelings Charades
Body Reactions to Anxiety
Trembling?
Butterflies?
Sweating?
Stomachache?
Headache?
Pounding Heart?
Coping modeling and role-plays Body Drawing
Fire Alarm and Detective Analogies
RelaxationMuscle Tension
Relaxation Training ◦ Progressive Muscle Relaxation (PMR)
◦ Secret Calming/Deep Breathing
Positive imagery exercises◦ A Peaceful Place
3-Component Model of Anxiety
What I Do What I Feel
What I Think
Helps guide the
selection of
treatment targets and
techniques.

What You Think: Anxious Self-TalkIn situations where we are experiencing strong emotions, like anxiety or fear, thoughts may be unrealistic.
◦ Thoughts about the situation, not the situation itself, are often what scare us.
◦ Consider thoughts to be “fact” and do not question how realistic they are.
◦ Anxious children tend to overestimate the likelihood that something bad will occur, and underestimate their ability to cope with it if it did.
Identifying Anxious Thoughts
If I talk, I’ll say
something stupid
and everyone will
laugh!
What if someone
steals me from
my bed?!?!
I’m not feeling
well! Maybe I have
a disease and I
might die!
I’m scared I’m gonna
do bad on this test
and then I won’t be
able to go to college
and get a good job!

Addressing Anxious ThoughtsThink like a detective! ◦ What trap did I fall into?
◦ Treat thoughts like guesses, not facts
◦ Look for evidence in support and against this thought
◦ Explore alternate interpretations
Three Most CommonThinking Traps
1. Jumping to ConclusionsoLeaping to a specific conclusion without evaluating how realistic
that outcome is.oExample?
2. Thinking the WorstoThinking that the worst possible outcome is going to happen.oExample?
3. Ignoring the PositiveoFocusing on the negative aspects of a situation, while ignoring
the positive.oExample?

Detective Thinking Imagine the worst thing actually happening
Critically evaluate its actual severity:◦ Would it be as bad as first thought?◦ Could you cope with it?◦ Have you handled anything like that before?
Typically, consequences of a situation are:◦ Time-limited◦ Manageable
Say to self: “So what if ‘it’ happens?”
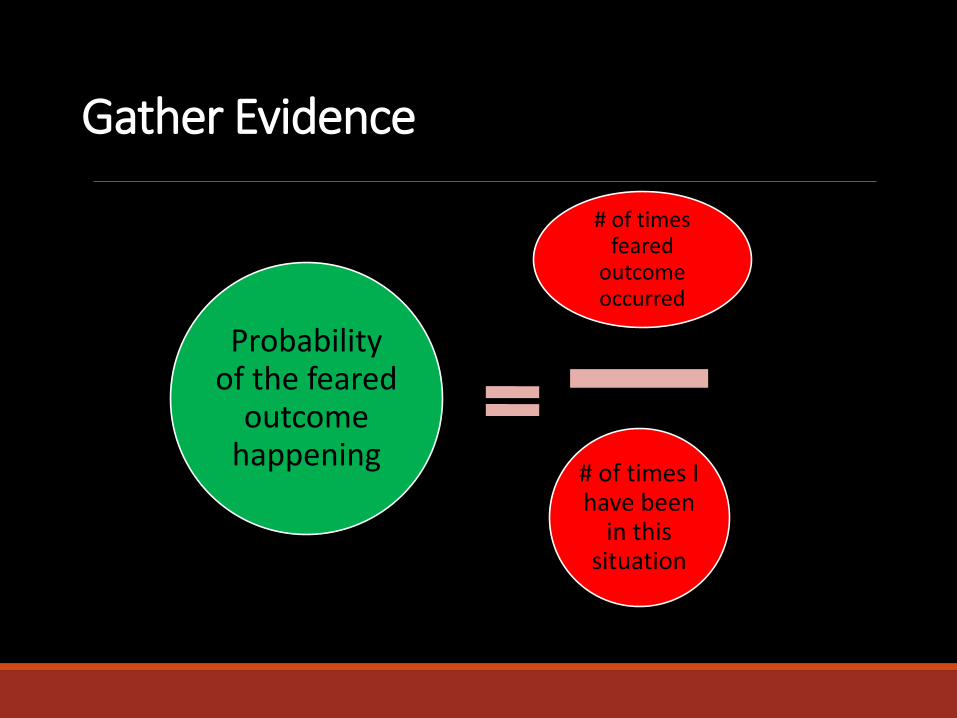
Gather Evidence
# of times feared
outcome occurred
# of times I have been
in this situation
Probability of the feared
outcome happening
**Focus on probability NOT possibility
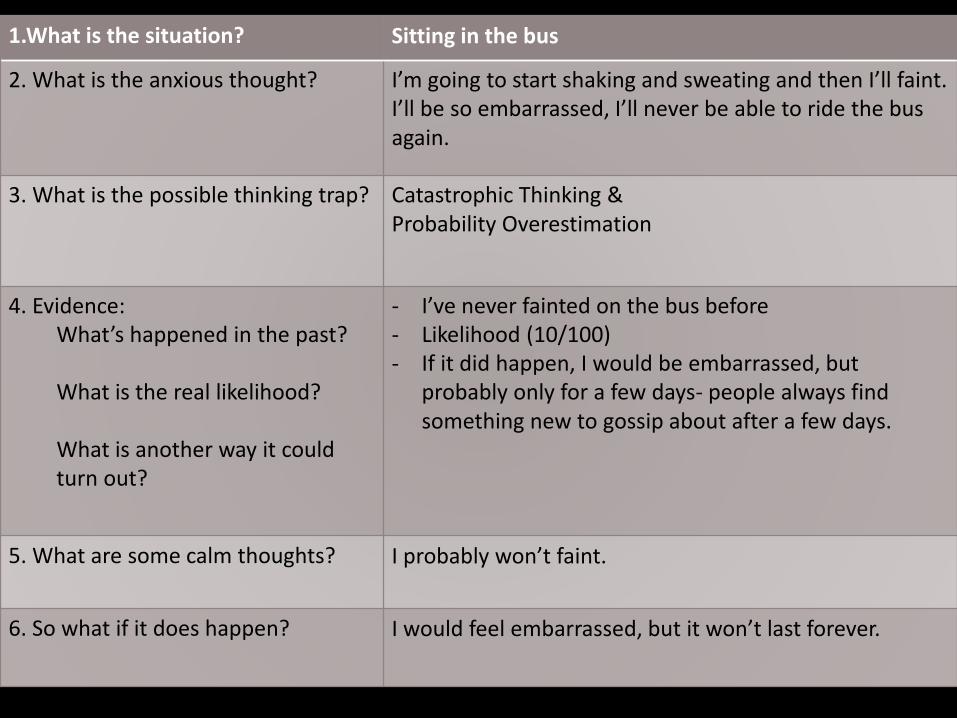
1.What is the situation? Sitting in the bus
2. What is the anxious thought? I’m going to start shaking and sweating and then I’ll faint. I’ll be so embarrassed, I’ll never be able to ride the bus again.
3. What is the possible thinking trap? Catastrophic Thinking & Probability Overestimation
4. Evidence:What’s happened in the past?
What is the real likelihood?
What is another way it could turn out?
- I’ve never fainted on the bus before - Likelihood (10/100) - If it did happen, I would be embarrassed, but
probably only for a few days- people always find something new to gossip about after a few days.
5. What are some calm thoughts? I probably won’t faint.
6. So what if it does happen? I would feel embarrassed, but it won’t last forever.
Targeting Thoughts: Cognitive Self-Statements
Some kids benefit from single coping self statements (especially if derived from detective thinking):
I am a brave girl (boy).
I can take care of myself when I am alone
There are no monsters under my bed!
I did it the last time, so I can do it again!
*These statements can be made into “coping cards”
*Should always be realistic for the child!*

Five STEPS to Problem Solving
S – Say what the problem is
T – Think of Solutions (even the silly ones)
E – Evaluate each Solutiono What is good about this?o What is bad about this?
P – Pick one and try it out
S – See if it workedo If it worked, great! If it did not, go back to your list of solutions and try another one
3-Component Model of Anxiety
What I DoWhat I Feel
What I Think
Helps guide the
selection of
treatment targets and
techniques.
Practice, Practice, Practice!EXPOSURES: “We’ll go places and do things!”
•Anxiety provoking situations
•Aim is not to remove anxiety, but to be able to manage it, so child should experience anxiety.
• Opportunity to practice
• Gradual (step-by-step)
• Repetition is key!
• Reward offered when completed!
Targeting Anxious Behavior: Situational Exposure
Facing Fears◦ Provides basis for more realistic thoughts about
situation◦ Not as scary/dangerous as thought◦ I was able to handle the situation/ feeling
scared
*Do not use relaxation techniques during exposure!*
FEAR
PYRAMID
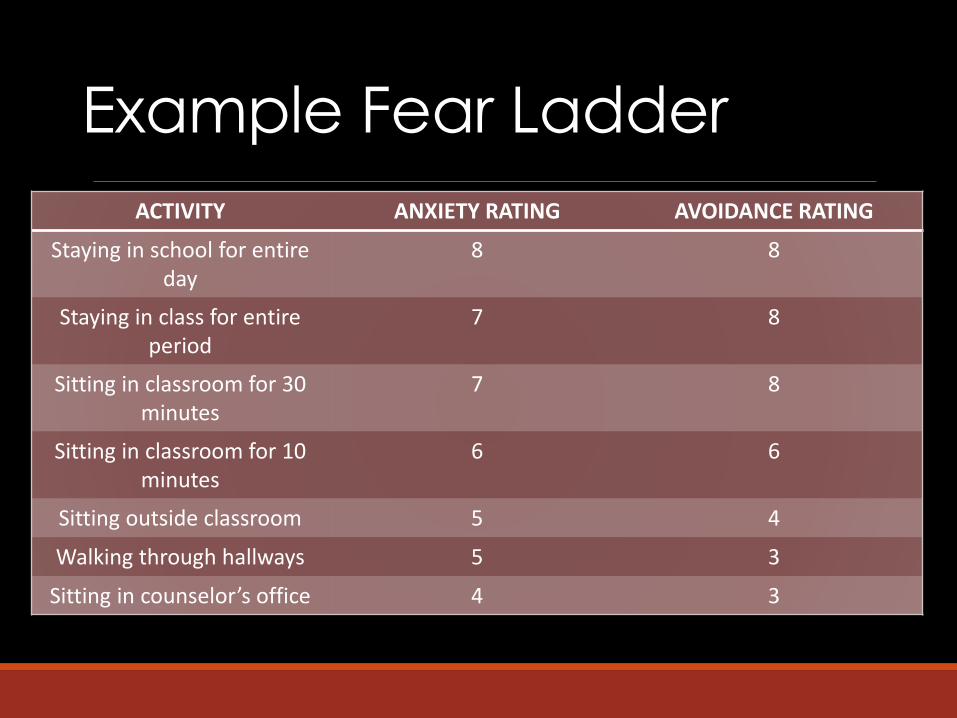
Example Fear Ladder
ACTIVITY ANXIETY RATING AVOIDANCE RATING
Staying in school for entire day
8 8
Staying in class for entireperiod
7 8
Sitting in classroom for 30 minutes
7 8
Sitting in classroom for 10 minutes
6 6
Sitting outside classroom 5 4
Walking through hallways 5 3
Sitting in counselor’s office 4 3
Reinforcing the Coping Child
Modeling Appropriate BehaviorA child can learn anxious behaviors by observing others
Model brave, calm behavior for the child – self-disclosure
Use appropriate coping skills in the face of anxiety
Reinforcement Techniques
Parents can inadvertently reinforce anxious behaviors◦ Providing excessive reassurance◦ Permitting avoidance
Using Reinforcement◦ Reward/praise non-anxious behavior◦ Active Ignoring of inappropriate behaviors (ex:
reassurance-seeking behaviors, tantrums)
Discouraging Avoidance Learn to support child, but not encourage avoidance
oEncourage child to utilize coping skills
oHelp child break down anxiety-provoking situations into manageable steps. Example: Child is nervous about being alone in the dark.
How would you break this down into manageable steps?
Provide praise when child faces their fears.oLabeled praise is more effective (Example: “Good job”
vs. “You did such a good job staying in your own bed last night.”)
Rewarding ChildrenSetting up a Reward systemoReward should be given immediately after completion of
task, if possible
oNon-monetary
oGive only if see the desired behavior
oSet clear expectations around how rewards can be earned
oBe consistent and follow through!
◦ Can be faded over time
Self-Evaluation and Self-RewardRating performance
Rewarding partial success and effort
Tangible vs. social rewardsExamples:
Toys Game-time with therapist
Stay awake later Choose favorite meal
Praise Movie night
REWARD MENU
5 things a parent or teacher can say to me to make me feel good
1. ___________________________________________________________
2. ___________________________________________________________
3. ___________________________________________________________
4. ___________________________________________________________
5. ___________________________________________________________
5 things I can do with family or friends for fun
1. ___________________________________________________________
2. ___________________________________________________________
3. ___________________________________________________________
4. ___________________________________________________________
5. ___________________________________________________________
5 things that cost less than $5
1. ___________________________________________________________
2. ___________________________________________________________
3. ___________________________________________________________
4. ___________________________________________________________
5. ___________________________________________________________

Overview of Outcomes

Pooled Analysis of CBT for Child Anxiety Disorders
% R
em
issi
on
Dia
gn
osi
s
12 Studies; ITT, p = 0.13, Cochrane Report, 2006
Pharmacological Intervention
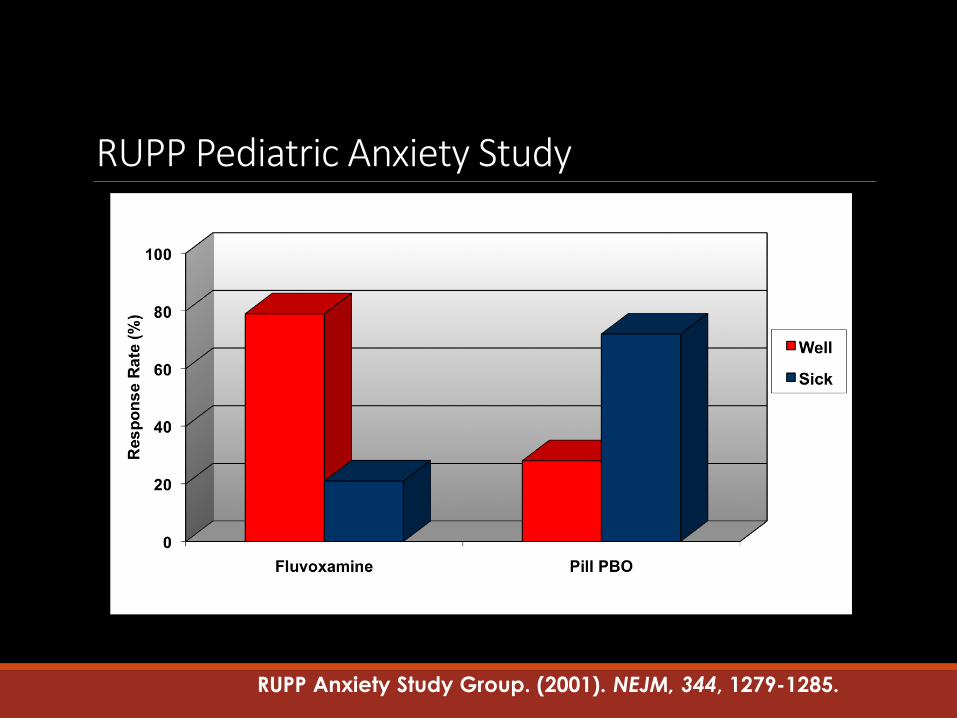
RUPP Pediatric Anxiety Study
RUPP Anxiety Study Group. (2001). NEJM, 344, 1279-1285.
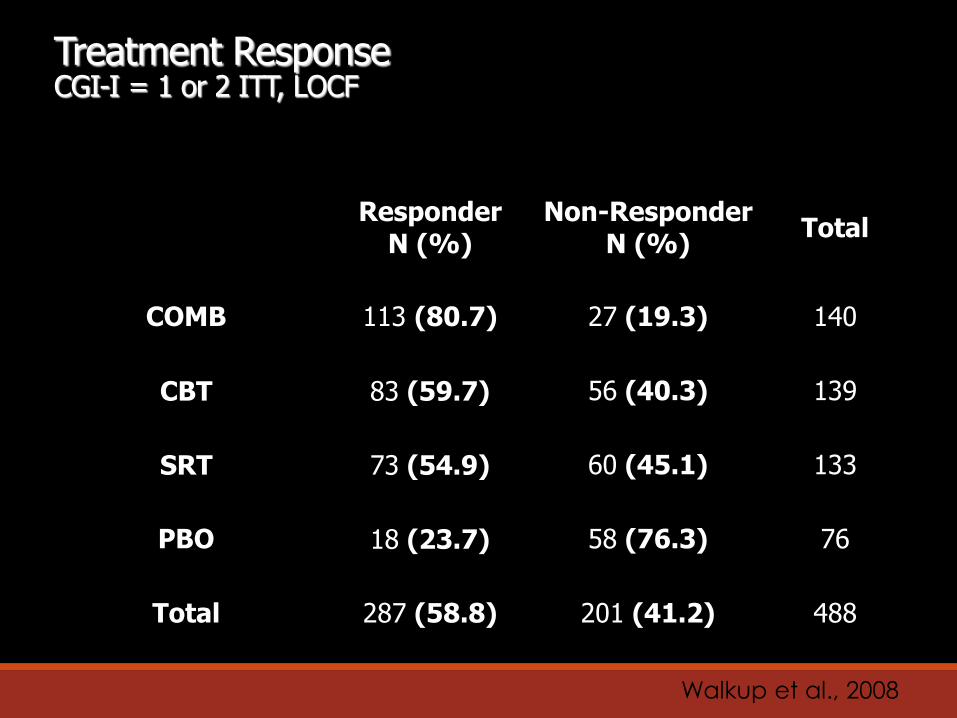
Treatment Response CGI-I = 1 or 2 ITT, LOCF
ResponderN (%)
Non-ResponderN (%)
Total
COMB 113 (80.7) 27 (19.3) 140
CBT 83 (59.7) 56 (40.3) 139
SRT 73 (54.9) 60 (45.1) 133
PBO 18 (23.7) 58 (76.3) 76
Total 287 (58.8) 201 (41.2) 488
Walkup et al., 2008

In Summaryo Ignore inappropriate or anxious behavior where possible, attend to
positive or “brave” behavior
o Facilitate at-home exposure practice
o Model confidence during exposure practice
o Remind child to use skills if anxiety expressed “ride the wave,” do “quick calming,” or use detective thinking
o Don’t solve the problem for your child
o Implement Reward System
For the younger ones…Use more concrete vs. abstract methods to engage
Create character for their anxiety
Simple relaxation strategies
More family-based coaching and parent training
CBT for Other Disorders
Obsessive-Compulsive Disorder
◦ Exposure and Response Prevention
◦ Bossing back OCD
Panic Disorder
◦ Interoceptive exposures
Tic Disorders, Tourettes, Trichotillomania
◦ Habit Reversal
Depression
- Focus on cognitions
- Interpersonal Therapy for Adolescents (IPT-A)
- Family-focused treatments
Intensive TreatmentsPanic Disorder with or without Agoraphobia
Specific Phobias
o One-session treatment (Ollendick, Ost, et al., 2009)
Separation Anxiety Disorder
Obsessive Compulsive Disorder
Selective Mutism-
A Clinically Significant Outcome
How to Participate

Clinical ServicesIndividual and group therapy offered for children ages 3-17◦ MINT
◦ CAPP
◦ General CCF
CALL 305-348-0477
Research ProgramsCHILD ANXIETY AND PHOBIA PROGRAM (CAPP)
Attention Bias Modification Training
Purpose: Evaluate a computer administered attention training program as a brief, low intensity intervention
Eligibility: ages 6-17, mild to moderate levels of anxiety, and do not meet criteria for anxiety disorder
Research ProgramsCHILD ANXIETY AND PHOBIA PROGRAM (CAPP)
“Brain training”◦ Research study of mild brain stimulation during an
attention training program for teenagers
(ages 13-17) with anxiety disorders
◦ Safe, noninvasive procedures used in over 1,000 published studies
◦ 4 weekly sessions
◦ Compensation provided for participation
◦ Call 305-348-1937 for more information!

Research ProgramsMENTAL HEALTH INTERVENTIONS AND TECHNOLOGY
PROGRAM (MINT)
Coaching program for young children with anxiety ages 3-7Trial for internet-based version of CBT for children ages 7-17
Saturday Treatment Program (SatTP)o If your child is ages 5-11 and struggling with behavior problems or
ADHD
o 8 Weeks
o Children participate in therapeutic recreational activities focused on social and sports skills
o Promotes positive peer relationships
Parenting Strategies Groupo If your child is ages 5-11 and struggling with behavior
problems or ADHDo 8 Weekly parenting classes o Provide interactive support for parents o Homework help available (extra cost)o School consultations available (extra cost)
T POWER Group – Teens Pursuing Opportunities with Evolving Relationships12-17 years old with interests in building social skills. Presenting socially awkward.
No formal diagnosis required – preliminary screening provided.
12 Sessions
6:00 PM - 7:30 PM Thursday Evenings.
Contact Information
Center for Children and Families
FIU, AHC 1 Room 140
11200 SW 8th St., Miami, FL 33199
(305) 348-0477
Email: [email protected]
Web: www.ccf.fiu.edu
Effectivechildtherapy.fiu.edu

Helpful Resources
Growing up Brave, Pincus
You and Your Anxious Child: Free Your Child from Fears and Worries and Create a Joyful Family Life, Albano
Helping your anxious child: A step-by-step guide for parents, Rapee, Spence, Cobhan & Wignall
Keys to parenting your anxious child, Manassis
Freeing your child from anxiety, Chansky
www.childanxiety.net