Embed Size (px)
Citation preview

Principles of Anesthesia
Prepared by: Dr. Othman Ismat Abdulmajeed
Cardiac Anesthetic Hawler Medical College
2015-2016 [email protected]
1

Types of Anesthesia
2
General Anesthesia
Local Anesthesia

General Anesthesia
• The word Anesthesia means absence of sensation, and general anesthesia therefore implies unconsciousness.
• General Anesthetics include any agents capable of producing total insensibility in a reversible manner, it can be inhalational, intravenous or combined.
3

What is Surgical anesthesia?
• Its a state of harmless and reversible insensibility which allows operations of considerable magnitude to be carried out without hindrance to the surgeon or detriment to the patient.
• It is convenient to consider this anesthetic state as consisting of a triad of SLEEP, ANALGESIA and MUSCLE RELAXATION.
4

Preparations for GA
• Before giving anesthesia, considerations should be given to the induction of anesthesia, the position of the patient on the operating table, monitoring, the use of intravenous fluids or blood transfusion, postoperative care and recovery facilities which will be required.
• The availability and function of all anesthetic equipment should be checked before starting.
5

Induction of GA
A. Inhalational induction.
• Can be done by one of the inhalational anesthetic agents which are: Halothane, Isoflurane, Enflurane, Desflurane and Sevoflurane.
• If spontaneous ventilation is to be maintained throughout the procedure, the mask is applied more firmly as consciousness is lost and the airway can be supported by guedel airway or by laryngeal mask or by endotracheal tube.
6

Induction of GA cont.
• Indications for Inhalational induction are:1. Young children.2. Upper airway obstruction.3. Lower airway obstruction with foreign body.4. Bronchopleural fistula.. Difficulties and Complications:1. Slow induction of anesthesia.2. Airway obstruction, bronchospasm.3. Laryngeal spasm.4. Environmental pollution.
7

Induction cont..
B. Intravenous Induction.
Monitoring should be started on the patient including Spo2, Blood pressure, ECG, Temperature.
Preoxygenation should be started using facemask with delivering of 100% oxygen.
Induction can be done by one of the IV induction agents: Thiopentone, Etomidate, Propofol, Ketamine.
8

Induction cont..
• Complications of IV induction:1. Regurgitation and vomiting.2. Intra-arterial injection.3. Peri-venous injection.4. Cardiovascular depression.5. Respiratory depression.6. Histamine release.7. Porphyria.8. others, like pain on injection.
9

Positioning
• After induction, the patient is placed on the operating table in a position appropriate for the proposed surgery.
• When positioning the patient, the anesthetist should take into account surgical access, patient safety, anesthetic technique, monitoring and position of i.v. lines.
10

Positioning cont..
• Here is the commonly used positions, each may have adverse effects on skeletal, ventilatory, circulatory and neurological.
1. The lithotomy position may result in nerve damage
2. The lateral position may cause asymmetrical lung ventilation.
3. The prone position may cause abdominal compression.
4. The trendelenburg position may cause pressure on the diaphragm.
5. The sitting position needs good support of the head.
6. The supine position may cause supine hypotensive syndrome during pregnancy.
11

Maintenance of GA
• Maintenance means continuation of anesthesia.
• Maintenance can be achieved by :
A. Inhalational + spontaneous ventilation.
B. Inhalational + controlled ventilation.
C. Intravenous + spontaneous ventilation.
D. Intravenous + controlled ventilation.
12

Inhalational Anesthesia
• Its suitable for superficial operations, minor procedures and small operations that don't require muscle relaxants.
• MAC is the minimum alveolar concentration of an inhaled anesthetic agent which prevents reflex movement in response to surgical incision in 50% of subjects.
• The main advantage of inhalational anesthesia is rapid control to deep anesthesia.
• The signs of inadequate depth of anesthesia are: Tachypnea, Tachycardia, Hypertension and sweating.
13

Complications of Inhalational
1. Airway obstruction.2. Laryngeal spasm.3. Bronchospasm.4. Malignant hyperthermia.5. Raised intracranial pressure.6. Atmospheric pollution.
14

Maintenance cont..
• Inhalational anesthesia can be delivered by face mask, laryngeal mask airway (LMA) or by endotracheal tube (ETT).
• USE OF FACE MASK:
The face mask has many variants of type and size, the selection of the correct fit is important to provide a gas-tight seal.
A mask with excessive dead space should be avoided in pediatric age group.
Maintenance of the airway may be assisted further by the use of Guedel airway.
15

Maintenance cont..
• Use of the laryngeal mask airway: Indications:1. To provide a clear airway with hands free
anesthetist.2. To avoid intubation during spontaneous ventilation.3. To assist intubation in case of difficulties. Contraindications:1. Full stomach patient.2. Any possibilities of regurgitations like hiatus hernia.3. surgery in the pharynx
16

Maintenance cont..
• Use of endotracheal intubation: Indications:1. secure clear airway.2. Can be used in unusual positions.3. Naso-tracheal tube can be used for head&neck
surgery.4. Protect the respiratory system from blood.5. Help suction of the respiratory system.6. For thoracic surgeries.
17

Relaxant Anesthesia
• Is an alternative to deep anesthesia with spontaneous ventilation and volatile agents leading to multisystem depression, the triad of sleep, suppression of reflexes and muscle relaxation may be provided separately with specific agents.
• Relaxant anesthesia provides muscle relaxation with light level of anesthesia with less risk of cardiovascular depression.
• Its appropriate for major abdominal, intraperitoneal, thoracic or intracranial operations.
18

Assessment of Relaxant Anesthesia
A. Adequacy of Anesthesia.Autonomic reflex activity with lacrimation, sweating, tachycardia, hypertension or reflex movement in response to surgery indicate “light anesthesia”.B. Awareness during anesthesia.The anesthetist should ensure that this possibility is avoided by constant observation of the patient for clinical signs of light anesthesia and by the use of Bispectral Index (BIS) monitoring.
19

Assessment of Relaxant Anesthesia cont..C. Adequacy of muscle relaxation.We should observe return of muscle tone, any abdominal movement or diaphragmatic or facial movement.An increase in airway pressure may indicate an increase in muscle tone.Small increments about 25-35% of the initial dose of the muscle relaxant.D. Adequacy of ventilation.The clinical signs of inadequacy are tachycardia, hypertension and increase in PaCo2.
20

Reversal of Relaxation
• At the end of operation, residual neuromuscular blockade is antagonized and spontaneous ventilation established before the tracheal tube is removed and the patient awakened.
• Reversal drug composed of ( Neostigmine 2.5 mg + Atropine 1.2 mg) for adults.
• Resumption of spontaneous ventilation should occur if normocapnic ventilation has been employed and assured by monitoring on end tidal Co2.
21

Reversal of Relaxation cont.
• In patients at risk of regurgitation and potential aspiration, the lateral position is preferred.
• Return of respiratory reflexes is significant by coughing and resistance to the presence of the tracheal tube.
• Tracheobroncheal suction via the tracheal tube is carried out using suction catheter.
• Pharyngeal suction is performed best under direct vision, avoiding trauma to the pharyngeal mucosa, uvula or epiglottis.
• After extubation, the patient’s ability to maintain the airway is ensured; Administration of oxygen is continued by face mask.
22

Complications of Extubation
• Laryngeal spasm:This may follow stimulation from extubation. Local anesthetic spray to the larynx may block the reflex and pharyngeal suction before extubation removes secretions which may cause stimulation.• Regurgitation / inhalation:If case of emergency surgery the patient’s stomach may be full, So aspiration by the nasogastric tube should be performed before tracheal extubation to remove gastric liquid.
23


Local Anesthesia
• Local anesthetic drugs act by producing a reversible block to the transmission of peripheral nerve impulse.
• A reversible block may be produced also by physical factors including pressure and cold.
• Many types of drug have local anesthetic actions (e.g. B-blocker and anti-histamines). But all those known and used as local anesthetics have originated from cocaine.
25

Mode of Action• When the nerve is stimulated, the potential difference
alters so that the inside becomes positive and the outside negative for a very brief period. In this state the nerve is said to be polarized and this is due to the rapid influx of sodium ions followed by an efflux of potassium.
• If a local anesthetic solution is applied to the nerve, then the action potential becomes smaller and if the concentration is sufficiently high, is completely abolished. If the trans-membrane potential is measured in this state it shows the normal resting potential.
26

Mode of Action cont..
• These substances are believed to block the sodium channels from the inside.
• Small nerve fibers are more sensitive than large nerve fibers.
• Myelinated fibers are blocked before non-myelinated fibers of the same diameter.
27

Mode of Action cont..
• Nerve fibers also differ in their susceptibility to local anesthetics. Thus it is the fine C fibers that are blocked first, followed by the A sigma fibers, both these groups subserving pain and temperature. Increasing the the concentration results in loss of touch and vibration sense, while the highest concentrations used clinically are needed to block motor function and proprioception.
28

Properties of Ideal LA
• Potent. • Non-irritant.• No allergic reaction.• No systemic toxicity.• Reversible action.• Rapid onset of action.• Sufficient duration of action.• Stable in solutions.• Not expensive.
29

Indications
• For local Anesthesia.
• Treatment of ventricular arrhythmia.
• To decrease hemodynamic response to tracheal intubation.
• Treatment of convulsions.
30

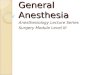
Structural classification of LA
31

32
Drugs Toxicity ESTERS Cocaine Very high Benzocaine Low Procaine Low Chloroprocaine Low Tetracain High AMIDES Lidocain Medium Mepivacain Medium Prilocain Low Bupivacain Medium Levobupivacain Low Ropivacain Low
Classification

Esters and Amides Differences• Esters result from the combination of para-
aminobenzoic acid and an amino-alcohol, while the amides result from the combination of aniline and amino acid.
• Esters have short half lives, while amides have longer.
• pKa values of the esters are higher than that of the amides.
• Amides are more stable in solution and are more diffusible in tissue.
33

Chemistry• The aromatic ring & hydrogen chain length determines
lipid solubility.
• The more lipid solubility, more easily penetrates cell membrane, more effect.
• The length of intermediate chain determines the duration of action. (long chain causes long duration).
• The duration of action increases with increasing protein binding. for example: protein binding of prilocain is 55% with medium duration compared with bupivacaine 96% protein binding and long duration.
34

Absorption
• Some of the drug will be absorbed into the systemic circulation.
• The degree of absorption depends on the vascularity of the area to which the drug has been applied.
• The rate of absorption can be decreased by adding vasoconstrictors.
35

Distribution
• The distribution of the drug is influenced by the degree of tissue and plasma protein binding of the drug.
• The more protein binding, the longer duration of action as free drug is slowly be available for metabolism.
36

Metabolism & Excretion• Esters (except cocaine) are broken down rapidly by
plasma esterases to inactive compounds and consequently have a short half life.
• Cocaine as exception is hydrolyzed in the liver.
• Ester metabolite excretion is renal.
• Amides are metabolized hepatically by amidases. This is a slower process, hence their half-life is longer and they can accumulate if given in repeated doses or by infusion.
37

Blood Levels of LA
• Systemic toxic reactions are directly related to the blood level of the drug, this is influenced by a number of factors. Following injection into tissues, the resultant blood level is a balance between absorption of the drug and distribution and metabolism, both of the latter acting to reduce its blood levels.
38

Blood Levels cont..Factors that determine the blood level are:1. Dose of the drug.2. Rate of administration.3. Site of injection.4. Presence or absence of vasoconstrictors.
The LA.s posses properties that will have some effect on their absorption. These include:
• Degree of protein binding.• Fat solubility.• Vasoactivity.• pKa.
39

Toxicity
• Why toxicity happens ?
• What are the signs and symptoms ?
• How we treat toxicity ?
40

Causes of Toxicity
• Toxicity occurs when a large dose has been injected into a very vascular area or when a normal dose is inadvertently injected intravenously; it may also result from premature release of the tourniquet during intra-venous regional anesthesia.
41

Signs & Symptoms of ToxicityA variety of signs and symptoms occur depending on the blood level and its rate of rise
Central Nervous System
Sedation, circumoral paraesthesia, pallor,fear, dizziness, excitement, tinnitus,anxiety and convulsion.
signs and symptoms appear in this sequence if the blood level increases gradually. If blood level inceases suddenly then convulsion may be the first sign to appear.
42

Signs & Symptoms cont..
Cardiovascular System
Increase refractory period, prolonged conduction, decrease contractility, finally ventricular fibrillation may occur.
With bupivacaine overdose ventricular fibrillation occurs immediately.
43

Treatment of Toxicity
• For convulsion we give benzodiazepine
• For respiratory failure we administer oxygen and control respiration.
• For circulatory failure we give vasopressor drugs, if not sufficient we give noradrenaline infusion.
44

Thank you