Embed Size (px)
Citation preview
Primary Prevention of Cardiovascular Disease:
the role of aspirin and statins
Michael Pignone, MD, MPHProfessor of Medicine
UNC Division of General Internal Medicine
UCSF CVD prevention symposium Jan 30, 2012
Aspirin and statins
• Both effective for prevention of CVD events– Some uncertainty about sub-groups
• Different adverse effects
• Costs converging
• Challenge: which patients should receive either or both for primary CVD prevention?
• Modeling may provide insight
Challenges in interpreting models
• Examining different modeling approaches can offer insights and highlight areas of uncertainty– Framing of questions– Inputs– Model structure – Time horizon, discount rate– Expression of results
Pignone et al Ann Intern Med. 2005;142:1073-9
Risk-based treatment preferred• CVD prevention benefits increase with
increasing CVD risk
• Adverse effects increase with age but otherwise relatively unrelated to risk
• Thus, CVD risk can be used to guide cost-effective treatment
• Global risk-based treatment strategies generally outperform risk factor-based strategies in modeling
Lee et al Circulation 2010; 122:1478-
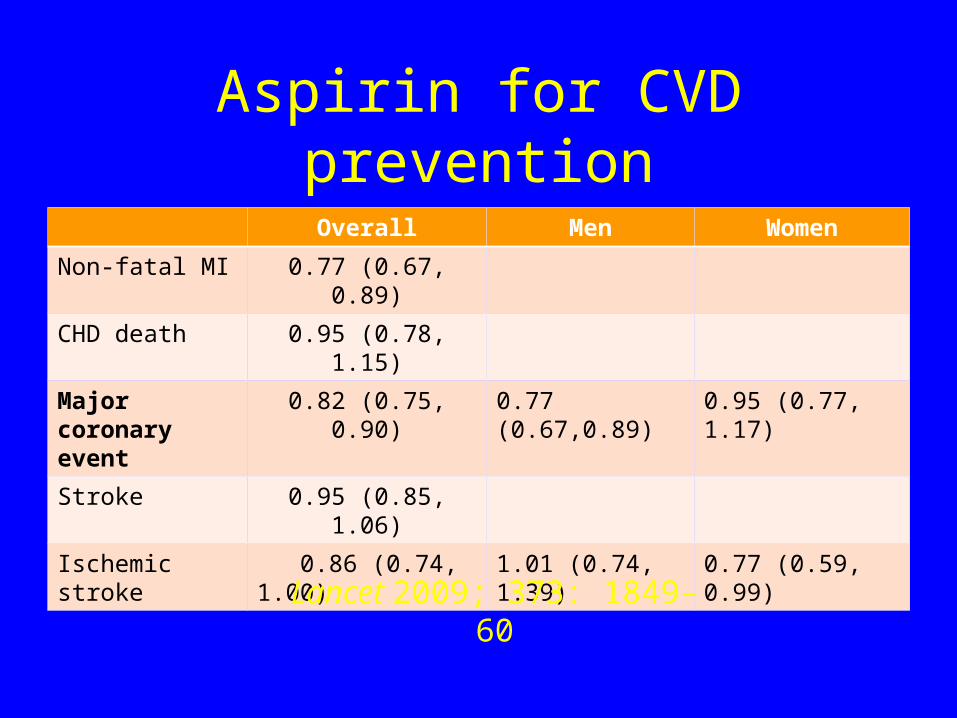
Aspirin for CVD prevention
Overall Men Women
Non-fatal MI 0.77 (0.67, 0.89)
CHD death 0.95 (0.78, 1.15)
Major coronary event
0.82 (0.75, 0.90) 0.77 (0.67,0.89) 0.95 (0.77, 1.17)
Stroke 0.95 (0.85, 1.06)
Ischemic stroke 0.86 (0.74, 1.00) 1.01 (0.74, 1.39) 0.77 (0.59, 0.99)
Lancet 2009; 373: 1849–60
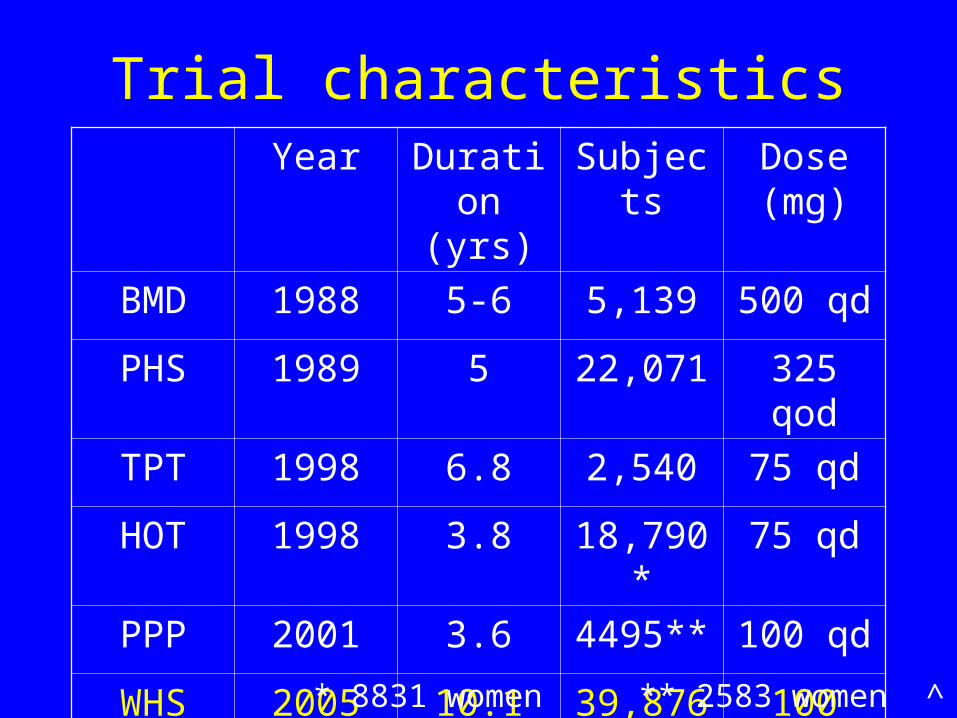
Trial characteristicsYear Duratio
n(yrs)
Subjects
Dose (mg)
BMD 1988 5-6 5,139 500 qd
PHS 1989 5 22,071 325 qod
TPT 1998 6.8 2,540 75 qd
HOT 1998 3.8 18,790*
75 qd
PPP 2001 3.6 4495** 100 qd
WHS 2005 10.1 39,876^
100 qod* 8831 women ** 2583 women ^ all women
Adverse effects of aspirin: GI bleeding
• RR 1.54 (1.30, 1.82): Lancet meta-analysis
• Excess risk ≈ 1 per 1000 users / year– Increases with age– RR higher in observational analyses (2.0)– No “safe” dosage– Enteric coating doesn’t prevent– PPI decreases risk, but routine use
not economical*
*Earnshaw et al Arch Intern Med. 2011; 171(3):218-25
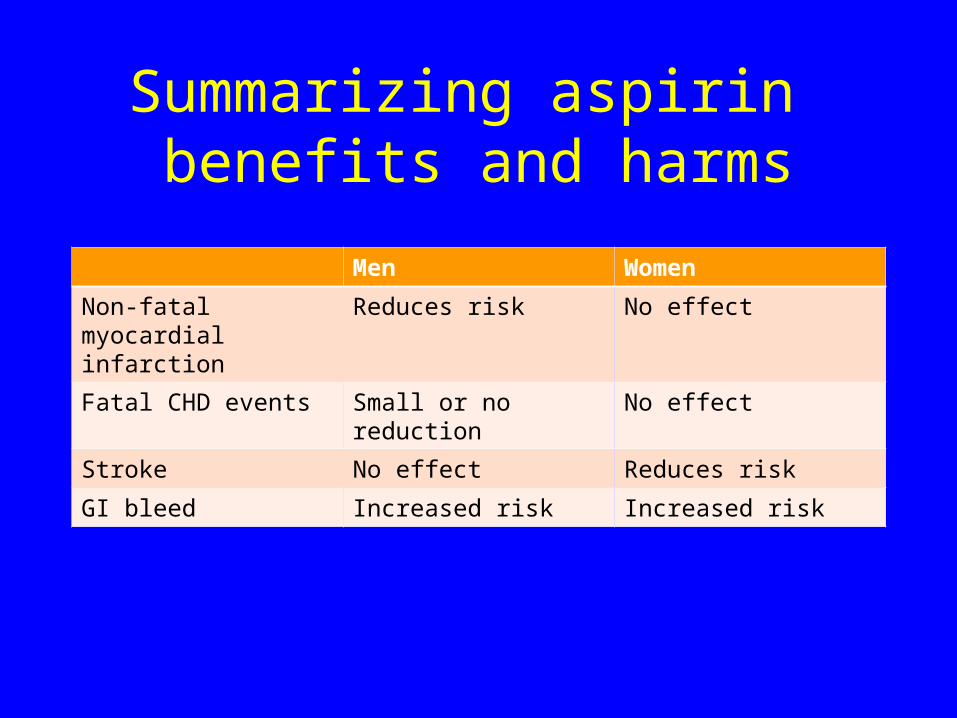
Summarizing aspirin benefits and harms
Men Women
Non-fatal myocardial infarction
Reduces risk No effect
Fatal CHD events Small or no reduction No effect
Stroke No effect Reduces risk
GI bleed Increased risk Increased risk
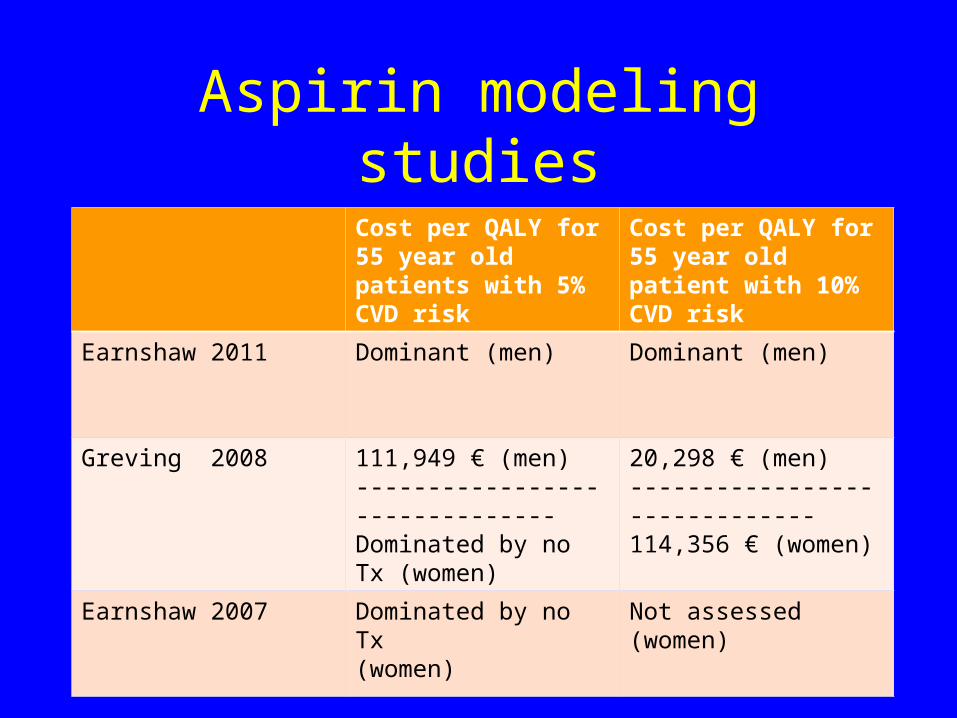
Aspirin modeling studies
Cost per QALY for 55 year old patients with 5% CVD risk
Cost per QALY for 55 year old patient with 10% CVD risk
Earnshaw 2011 Dominant (men) Dominant (men)
Greving 2008 111,949 € (men)-------------------------------Dominated by no Tx (women)
20,298 € (men)------------------------------114,356 € (women)
Earnshaw 2007 Dominated by no Tx(women)
Not assessed (women)
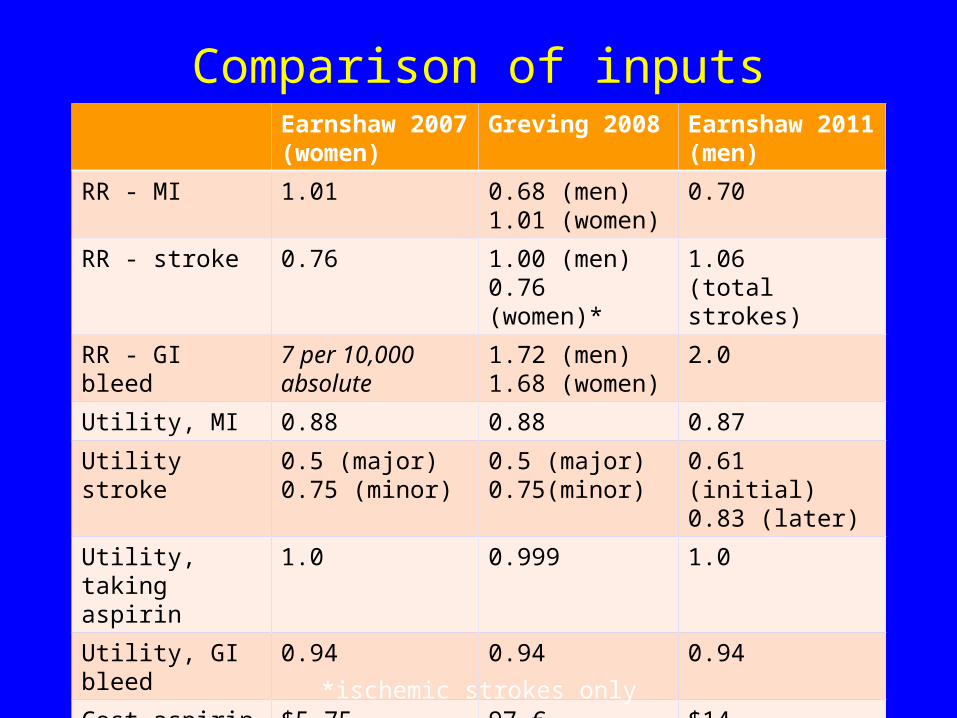
Comparison of inputsEarnshaw 2007 (women)
Greving 2008 Earnshaw 2011 (men)
RR - MI 1.01 0.68 (men) 1.01 (women)
0.70
RR - stroke 0.76 1.00 (men) 0.76 (women)*
1.06 (total strokes)
RR - GI bleed 7 per 10,000 absolute
1.72 (men) 1.68 (women)
2.0
Utility, MI 0.88 0.88 0.87
Utility stroke 0.5 (major)0.75 (minor)
0.5 (major) 0.75(minor)
0.61 (initial) 0.83 (later)
Utility, taking aspirin
1.0 0.999 1.0
Utility, GI bleed 0.94 0.94 0.94
Cost aspirin $5.75 97 € $14
Cost – GI bleed $7538 1625 € $13,342
*ischemic strokes only
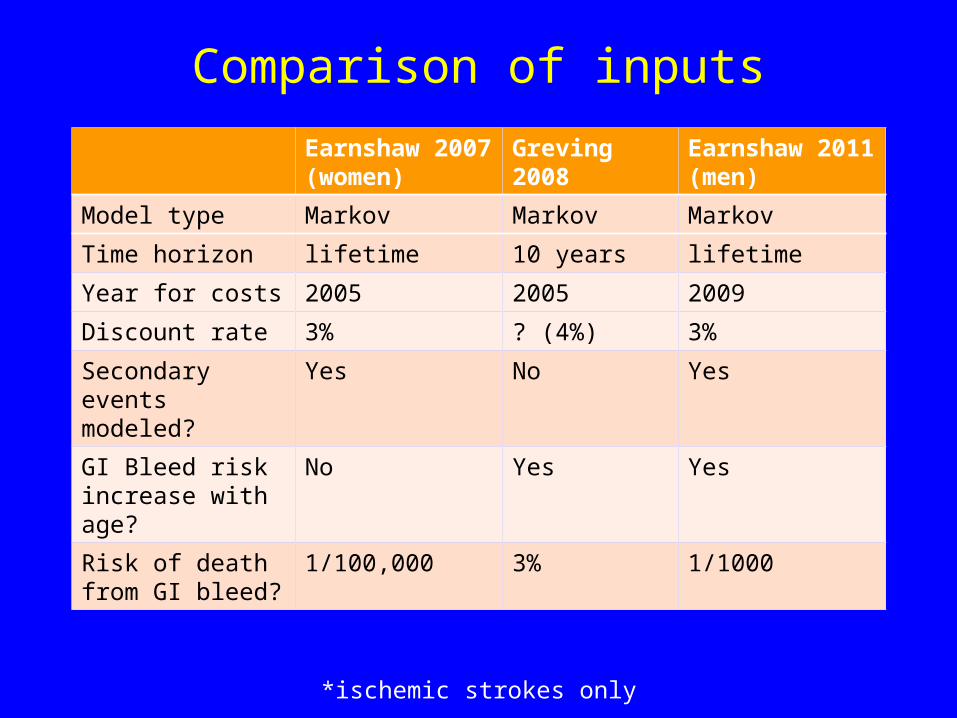
Comparison of inputs
Earnshaw 2007 (women)
Greving 2008 Earnshaw 2011 (men)
Model type Markov Markov Markov
Time horizon lifetime 10 years lifetime
Year for costs 2005 2005 2009
Discount rate 3% ? (4%) 3%
Secondary events modeled?
Yes No Yes
GI Bleed risk increase with age?
No Yes Yes
Risk of death from GI bleed?
1/100,000 3% 1/1000
*ischemic strokes only
Aspirin - conclusions• Aspirin appears cost-effective for men with
increased risk (>10% risk) in all models
• For women, aspirin is not cost-effective for younger women and those with low CVD risk (under 5%) but appears cost-effective for higher risk older women
• Cost-effectiveness for lower risk men (under 10%) unclear - depends on inputs and time horizon
Statins
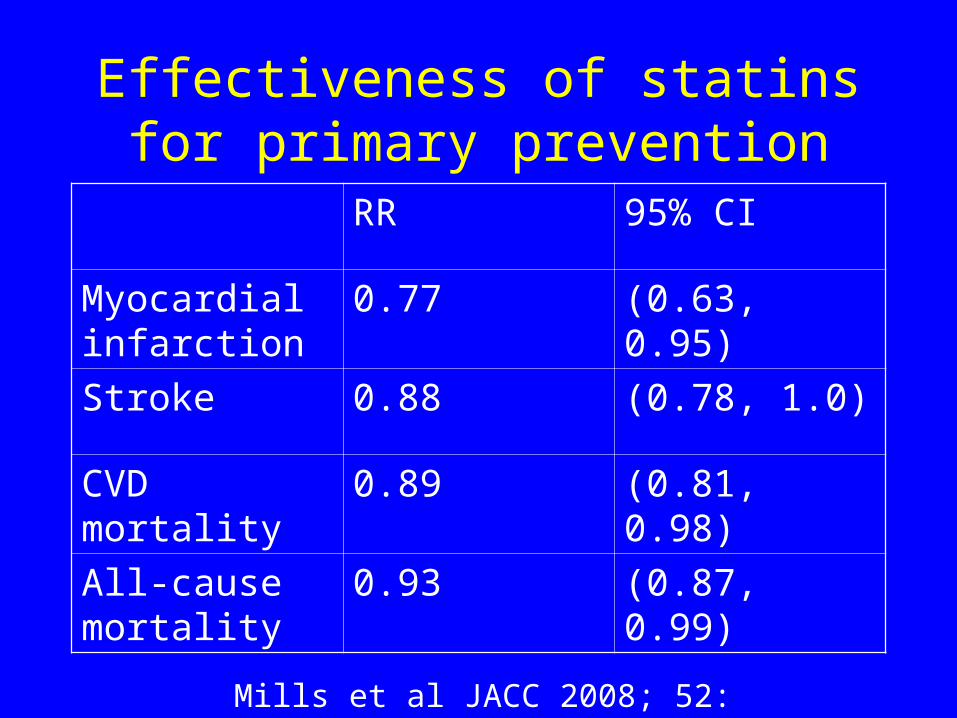
Effectiveness of statins for primary prevention
RR 95% CI
Myocardial infarction
0.77 (0.63, 0.95)
Stroke 0.88 (0.78, 1.0)
CVD mortality 0.89 (0.81, 0.98)
All-cause mortality
0.93 (0.87, 0.99)
Mills et al JACC 2008; 52: 1769-81
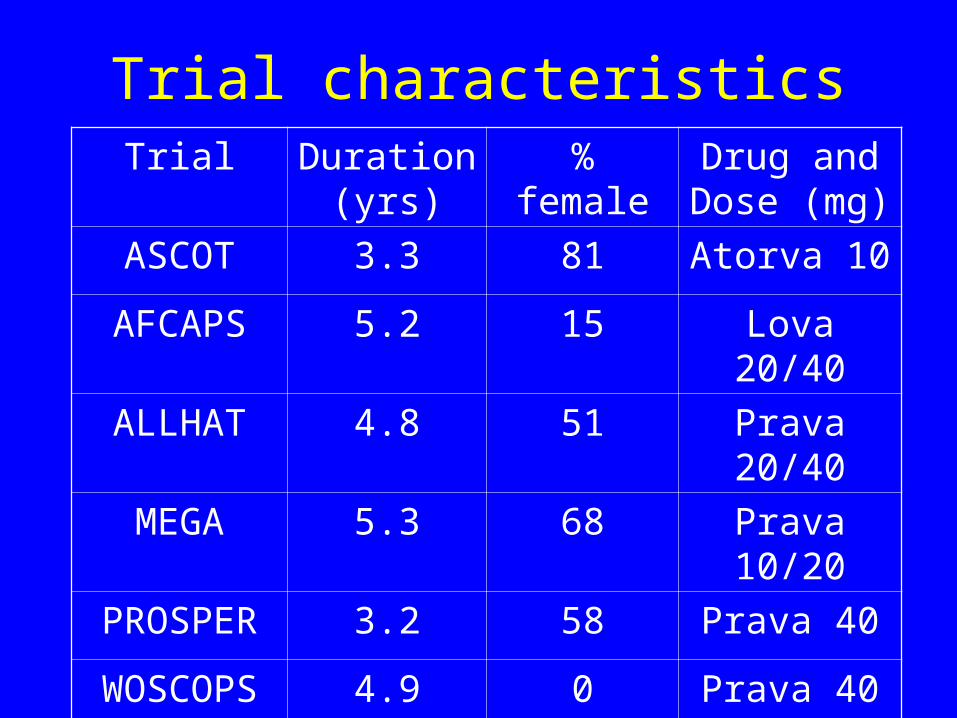
Trial characteristicsTrial Duration
(yrs)%
femaleDrug and Dose (mg)
ASCOT 3.3 81 Atorva 10
AFCAPS 5.2 15 Lova 20/40
ALLHAT 4.8 51 Prava 20/40
MEGA 5.3 68 Prava 10/20
PROSPER 3.2 58 Prava 40
WOSCOPS 4.9 0 Prava 40
Statin adverse effects
• Muscle pain- common (10%)
• Myopathy – rare (0.1%)
• Rhabdomyolysis – very rare (0.01%)
• ? Increased risk of diabetes
• Change in liver enzymes without failure
• Concerns about cancer risk and violence have not materialized
Jacobson Mayo Clin Proc 2008;83:687-700
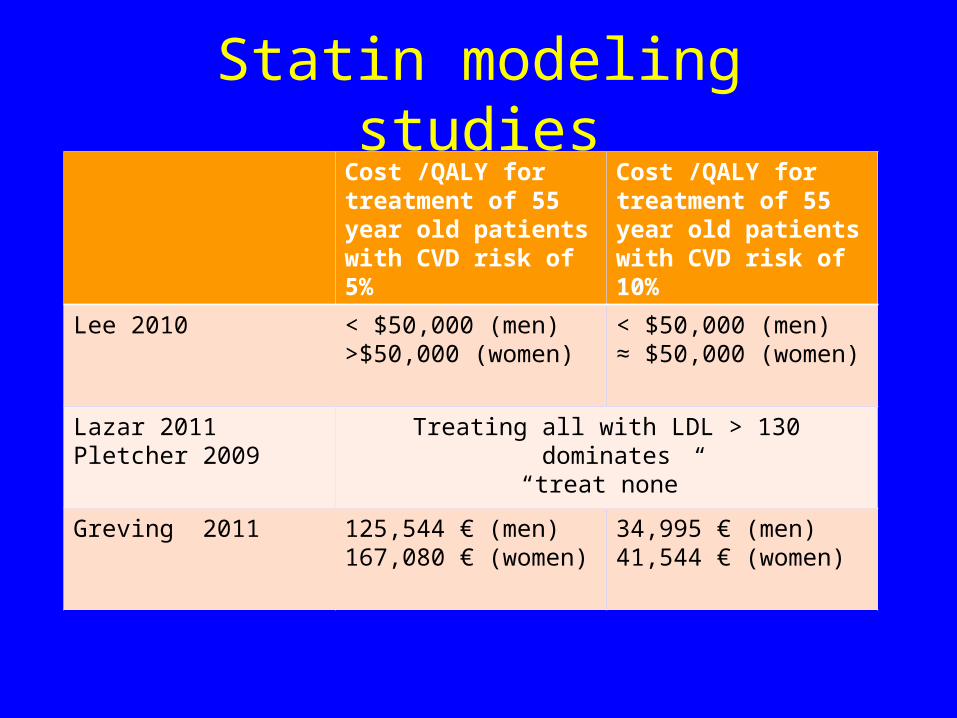
Statin modeling studiesCost /QALY for treatment of 55 year old patients with CVD risk of 5%
Cost /QALY for treatment of 55 year old patients with CVD risk of 10%
Lee 2010 < $50,000 (men)>$50,000 (women)
< $50,000 (men)≈ $50,000 (women)
Lazar 2011Pletcher 2009
Treating all with LDL > 130 dominates “treat none”
Greving 2011 125,544 € (men)167,080 € (women)
34,995 € (men)41,544 € (women)
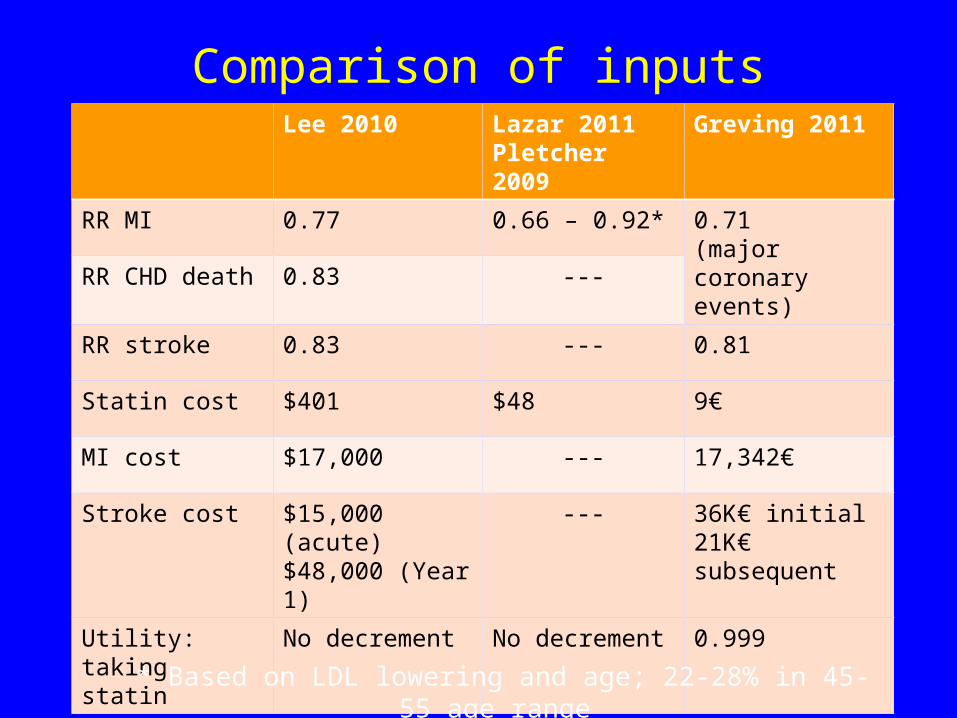
Comparison of inputsLee 2010 Lazar 2011
Pletcher 2009Greving 2011
RR MI 0.77 0.66 – 0.92* 0.71(major coronary events)RR CHD death 0.83 ---
RR stroke 0.83 --- 0.81
Statin cost $401 $48 9€
MI cost $17,000 --- 17,342€
Stroke cost $15,000 (acute)$48,000 (Year 1)
--- 36K€ initial21K€ subsequent
Utility: taking statin
No decrement No decrement 0.999
* Based on LDL lowering and age; 22-28% in 45-55 age range
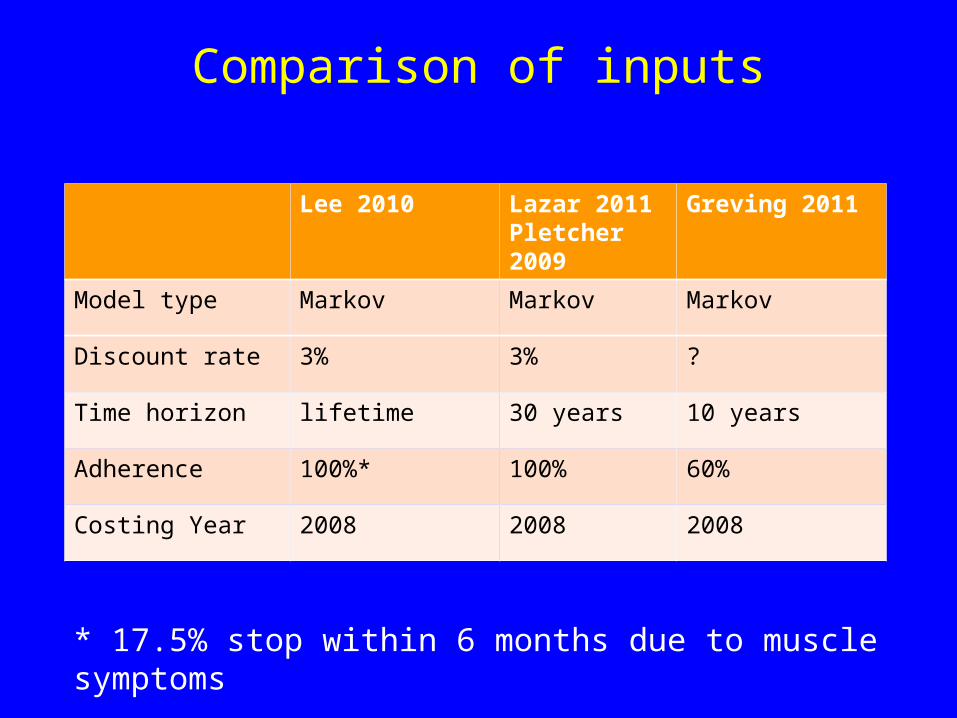
Comparison of inputs
Lee 2010 Lazar 2011Pletcher 2009
Greving 2011
Model type Markov Markov Markov
Discount rate 3% 3% ?
Time horizon lifetime 30 years 10 years
Adherence 100%* 100% 60%
Costing Year 2008 2008 2008
* 17.5% stop within 6 months due to muscle symptoms
Integrating aspirin and statin decision making
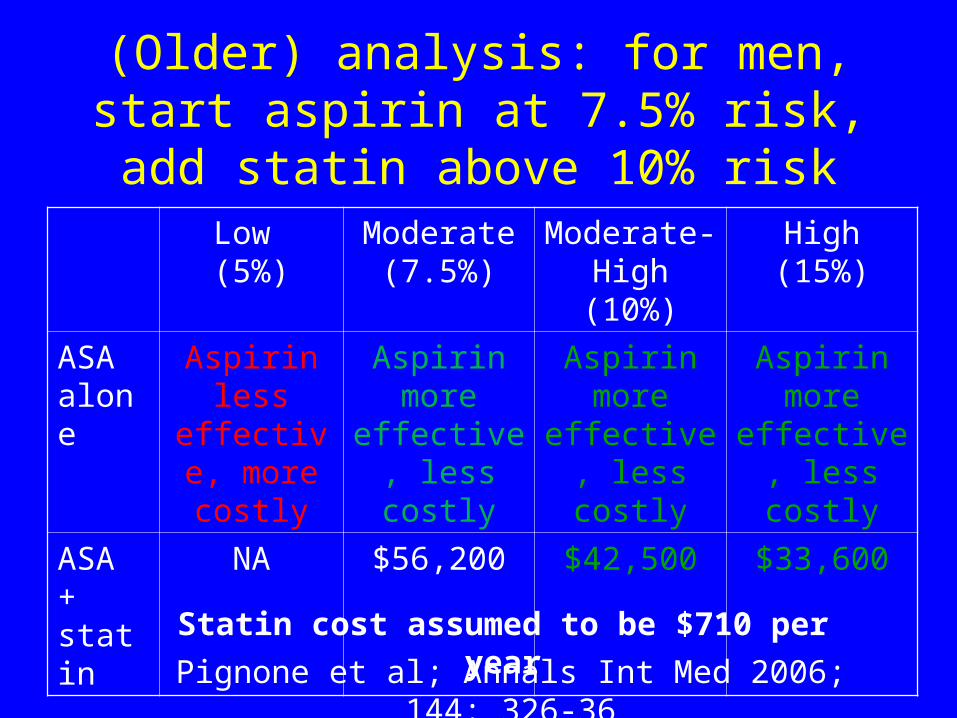
(Older) analysis: for men, start aspirin at 7.5% risk, add statin
above 10% riskLow (5%)
Moderate(7.5%)
Moderate-High (10%)
High(15%)
ASA alone
Aspirin less effective,
more costly
Aspirin more
effective, less costly
Aspirin more
effective, less costly
Aspirin more
effective, less costly
ASA + statin
NA $56,200 $42,500 $33,600
Statin cost assumed to be $710 per year
Pignone et al; Annals Int Med 2006; 144: 326-36
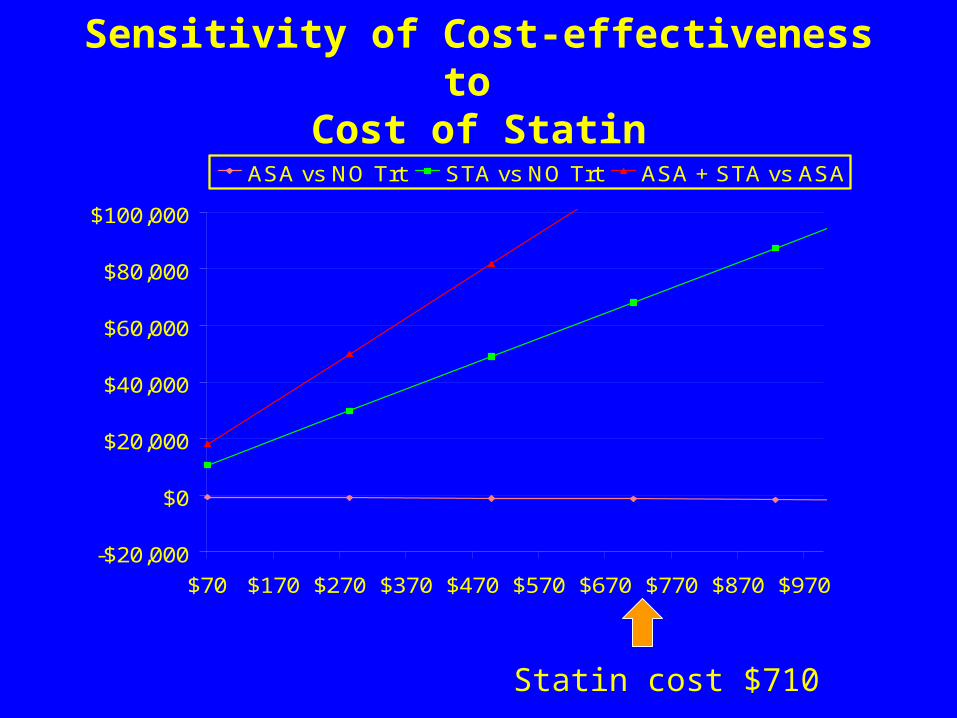
Sensitivity of Cost-effectiveness to
Cost of Statin
-$20,000
$0
$20,000
$40,000
$60,000
$80,000
$100,000
$70 $170 $270 $370 $470 $570 $670 $770 $870 $970
ASA vs NO Trt STA vs NO Trt ASA + STA vs ASA
Statin cost $710
Healthwarehouse.com
• Simvastatin 40mg Tablets• 30 Tablets $3.50• 90 Tablets $9.50• 360 Tablets $36.50
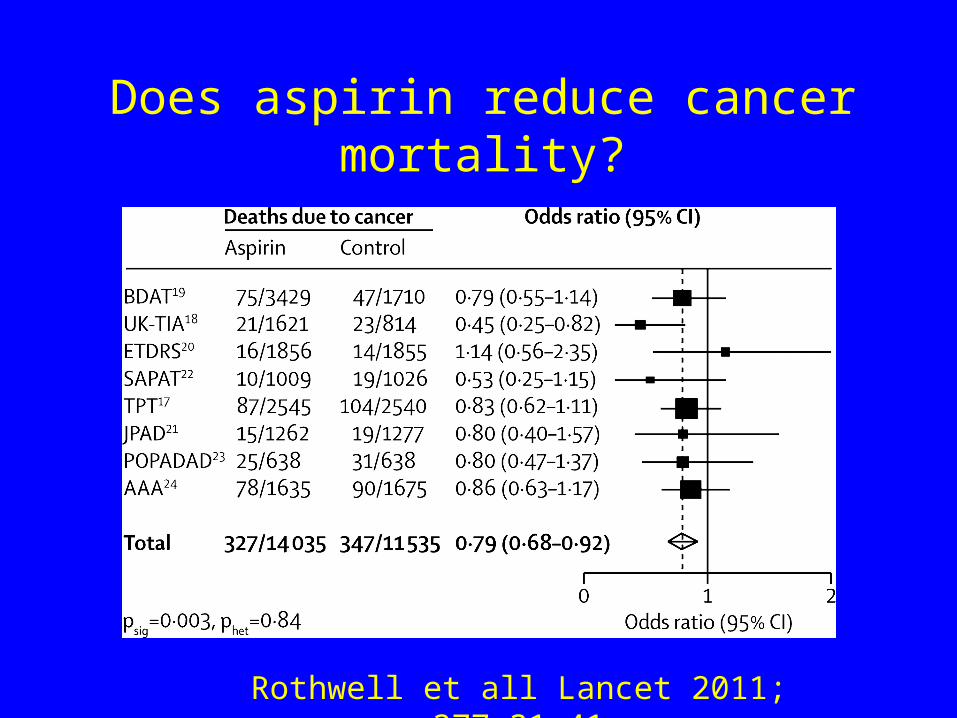
Does aspirin reduce cancer mortality?
Rothwell et all Lancet 2011; 377:31-41
Updated modeling
• Examines joint decision making: aspirin and statins
• Updated model parameters– Statin costs– GI bleeding risk– Other health care costs
• Examines the potential effect of aspirin-related cancer mortality reduction
Stephanie Earnshaw to describe current model
Research Priorities
• Cost-effective adherence promotion
• Disutility of daily medication use
• Does aspirin affect cancer mortality?
• Cost-effective methods for reducing adverse effects
• Appropriate time horizons for primary prevention analyses
















![Chapter 25 – HORMONES OF THE CARDIOVASCULAR SYSTEM · Chapter 25 – HORMONES OF THE CARDIOVASCULAR SYSTEM Michael E. Hall, MD, MS, ... [30], beta blockade [31], or the use of statins](https://img.pdfslide.us/doc/110x75/5ae211e17f8b9ae74a8bf464/chapter-25-hormones-of-the-cardiovascular-25-hormones-of-the-cardiovascular.jpg)












