Embed Size (px)
Citation preview

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 7 0 , N O . 9 , 2 0 1 7
ª 2 0 1 7 B Y T H E A M E R I C A N CO L L E G E O F C A R D I O L O G Y F O U N DA T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 7 . 0 6 . 0 5 8
Efficacy of Rosuvastatin inChildren With Homozygous FamilialHypercholesterolemia and AssociationWith Underlying Genetic Mutations
Evan A. Stein, MD, PHD,a Eldad J. Dann, MD,b Albert Wiegman, MD, PHD,c Flemming Skovby, MD,dDaniel Gaudet, MD, PHD,e Etienne Sokal, MD, PHD,f Min-Ji Charng, MD, PHD,g Mafauzy Mohamed, MM,h
Ilse Luirink, MD,c Joel S. Raichlen, MD,i Mattias Sundén, PHD,j Stefan C. Carlsson, MD, PHD,j Frederick J. Raal, PHD,k
John J.P. Kastelein, MD, PHDc
ABSTRACT
FrocD
Ne
Co
Un
en
Un
Ma
Sci
As
co
wh
BACKGROUND Homozygous familial hypercholesterolemia (HoFH), a rare genetic disorder, is characterized by
extremely elevated levels of low-density lipoprotein cholesterol (LDL-C) and accelerated atherosclerotic cardiovascular
disease. Statin treatment starts at diagnosis, but no statin has been formally evaluated in, or approved for, HoFH
children.
OBJECTIVES The authors sought to assess the LDL-C efficacy of rosuvastatin versus placebo in HoFH children, and the
relationship with underlying genetic mutations.
METHODS This was a randomized, double-blind, 12-week, crossover study of rosuvastatin 20 mg versus placebo,
followed by 12 weeks of open-label rosuvastatin. Patients discontinued all lipid-lowering treatment except ezetimibe
and/or apheresis. Clinical and laboratory assessments were performed every 6 weeks. The relationship between LDL-C
response and genetic mutations was assessed by adding children and adults from a prior HoFH rosuvastatin trial.
RESULTS Twenty patients were screened, 14 randomized, and 13 completed the study. The mean age was 10.9 years;
8 patients were on ezetimibe and 7 on apheresis. Mean LDL-C was 481 mg/dl (range: 229 to 742 mg/dl) on placebo and
396 mg/dl (range: 130 to 700 mg/dl) on rosuvastatin, producing a mean 85.4 mg/dl (22.3%) difference (p ¼ 0.005).
Efficacy was similar regardless of age or use of ezetimibe or apheresis, and was maintained for 12 weeks. Adverse events
were few and not serious. Patients with 2 defective versus 2 negative LDL receptor mutations had mean LDL-C
reductions of 23.5% (p ¼ 0.0044) and 14% (p ¼ 0.038), respectively.
CONCLUSIONS This first-ever pediatric HoFH statin trial demonstrated safe and effective LDL-C reduction with
rosuvastatin 20 mg alone or added to ezetimibe and/or apheresis. The LDL-C response in children and adults was
related to underlying genetic mutations. (A Study to Evaluate the Efficacy and Safety of Rosuvastatin in Children
and Adolescents With Homozygous Familial Hypercholesterolemia [HYDRA]; NCT02226198) (J Am Coll Cardiol
2017;70:1162–70) © 2017 by the American College of Cardiology Foundation.
m the aMetabolic and Atherosclerosis Research Center, Cincinnati, Ohio; bRambam Health Care Campus, Haifa, Israel;
epartment of Paediatrics and Vascular Medicine, Academic Medical Center, University of Amsterdam, Amsterdam, the
therlands; dDepartment of Clinical Genetics, University Hospital, and Institute of Clinical Medicine, University of Copenhagen,
penhagen, Denmark; eECOGENE-21 Clinical and Translational Research Center and Lipidology Unit, Department of Medicine,
iversité de Montréal, Chicoutimi, Quebec, Canada; fUniversité Catholique de Louvain, Cliniques St. Luc, Service de Gastro-
térologie et Hépatologie Pédiatrique, Brussels, Belgium; gTaipei Veterans General Hospital, Taipei, Taiwan, R.O.C.; hHospital
iversiti Sains Malaysia (HUSM), Clinical Trial Unit, Level 2, Kelantan, Malaysia; iAstraZeneca Pharmaceuticals LP, Gaithersburg,
ryland; jAstraZeneca Gothenburg, Mölndal, Sweden; and kCarbohydrate and Lipid Metabolism Research Unit, Faculty of Health
ences, University of Witwatersrand, Johannesburg, South Africa. The study was funded by AstraZeneca Pharmaceuticals LP.
traZeneca was responsible for study conduct, data collection, and analysis. The study was designed by AstraZeneca in
njunction with Drs. Stein and Kastelein. The initial drafts of the manuscript were done by Dr. Stein, Prof. Raal, and Dr. Kastelein,
o had full access to the study data. All authors reviewed and had input to the final draft. The academic authors vouch for the

AB BR E V I A T I O N S
AND ACRONYM S
apo B = apolipoprotein B
ARH = autosomal recessive
hypercholesterolemia
CVD = cardiovascular disease
HeFH = heterozygous familial
hypercholesterolemia
HoFH = homozygous familial
hypercholesterolemia
LDL-C = low-density
lipoprotein cholesterol
LDLR = low-density
lipoprotein receptor
PCSK9 = proprotein
convertase subtilisin/kexin
type 9
J A C C V O L . 7 0 , N O . 9 , 2 0 1 7 Stein et al.A U G U S T 2 9 , 2 0 1 7 : 1 1 6 2 – 7 0 Rosuvastatin in Children With Homozygous FH
1163
H omozygous familial hypercholesterolemia(HoFH) is a rare, but severe, genetic disor-der with an estimated frequency of 1 in
300,000 to 1,000,000 (1). It is caused by mutationsthat occur in either the low-density lipoprotein recep-tor (LDLR), apolipoprotein B (apo B), proprotein con-vertase subtilisin/kexin type 9 (PCSK9), or the LDLRadaptor protein1 (LDLRAP1, also known as ARH)genes, which all significantly impair low-density lipo-protein cholesterol (LDL-C) clearance (2). This in turnresults in a phenotype with severely elevated LDL-C,skin and tendon xanthoma, and premature and oftenfatal cardiovascular disease (CVD) in childhood orearly adulthood (1,2). Statins, when used as mono-therapy at their highest doses, are modestly effectivein HoFH, reducing LDL-C by 25%. The addition of eze-timibe reduces LDL-C an additional 15% to 20% (2).Due to the very high baseline LDL-C levels, theapproximately 40% reduction with statin–ezetimibecombination therapy results in large absolute de-creases in LDL-C and appears to contribute to thereduction in CVD morbidity and mortality in HoFHpatients reported in observational studies (3,4). How-ever, very few, if any, patients achieve anywhere nearoptimal LDL-C levels with these conventional drugtherapies, and LDL apheresis is required; if available,apheresis is usually performed weekly or biweekly (1).
SEE PAGE 1171
Numerous trials in HoFH, predominantly withadults, have been carried out with various statinsover the past 30 years (5–7). Rosuvastatin, the mostefficacious statin, has been shown to significantlyreduce LDL-C levels in adult HoFH patients, but aswith all statins, data in pediatric patients are limitedand almost nonexistent in children younger than 12years (7). No controlled trials of apheresis in youngHoFH children have been reported. Among neweragents approved for HoFH, lomitapide is approved inadults, and mipomersen and evolocumab areapproved, but not for use in HoFH children younger
validity of the data in the final manuscript. Dr. Stein has received consultant
statins. Dr. Gaudet has served as a consultant or advisor for AstraZeneca, Reg
Novartis, Ionis, Cymabay, Uniqure, and Catabasis; and has received researc
consultant and expert witness fees from AstraZeneca regarding statins and
Shire not related to statins; and is chief science officer of Promethera Bios
advisor fees from AstraZeneca. Drs. Raichlen, Sundén, and Carlsson are
research grants and consultant or lecture fees from AstraZeneca, Merck, Pfiz
received grant support from AstraZeneca, Pfizer, Roche, Novartis, Merck, M
lecture fees from AstraZeneca, GlaxoSmithKline, Pfizer, Novartis, Merck/Sc
heim; and consulting fees from AstraZeneca, Abbott, Pfizer, Ionis, Genzyme,
Sanofi. All other authors have reported that they have no relationships rele
Manuscript received May 2, 2017; revised manuscript received June 16, 2017
than 12 years (8,9). Although recent studieswith a PCSK9 inhibitor have shown that theLDL-C response is related to residual LDLRactivity in HoFH, similar data are lacking withstatins, especially in a pediatric population(9). We now report the first HoFH trial spe-cifically in children and adolescents, 6 to <18years of age, with a statin, rosuvastatin.Because the LDL-C response to statin therapyvaries considerably in HoFH, we also exam-ined the association between underlying ge-notype and rosuvastatin 20 mg treatment in abroader HoFH population of both childrenand adults.
METHODS
STUDY DESIGN AND PATIENTS. The HYDRA study(A Study to Evaluate the Efficacy and Safety ofRosuvastatin in Children and Adolescents with Ho-mozygous Familial Hypercholesterolemia) was aglobal trial in 7 countries in Asia, Europe, the MiddleEast, and North America. The study was reviewed andapproved by local human ethics committees. Parentsor legal guardians and, where applicable, the patient,signed an informed consent form before any study-related procedures being performed.
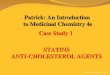
The trial involved HoFH children and adolescents,6 to <18 years of age, randomized to a double-blind,12-week crossover period of rosuvastatin 20 mgdaily versus placebo, followed by a 12-week, open-label rosuvastatin 20 mg maintenance phase. Thestudy design (Figure 1) consisted of a lead-in phase inwhich eligible patients discontinued all lipid-lowering therapy except ezetimibe and/or apheresis,which were continued throughout the study, andreceived rosuvastatin 10 mg daily in addition to di-etary advice for 4 weeks. Patients already stable onrosuvastatin 20 mg proceeded directly to therandomization period. Eligible patients were thenrandomized 1:1 to rosuvastatin 20 mg daily for
and expert witness fees from AstraZeneca regarding
eneron, Sanofi, Amgen, Aegerion, Chiesi, Gemphire,
h funding from AstraZeneca. Dr. Sokal has received
from Promethera Biosciences, Abbvie, Alexion, and
ciences. Dr. Mohamed has received consultant and
employees of AstraZeneca. Prof. Raal has received
er, Regeneron, Sanofi, and Amgen. Dr. Kastelein has
erck/Schering-Plough, Ionis, Genzyme, and Sanofi;
hering-Plough, Roche, Ionis, and Boehringer Ingel-
Roche, Novartis, Merck, Merck/Schering-Plough, and
vant to the contents of this paper to disclose.
, accepted June 29, 2017.

FIGURE 1 Study Design
Screening1–2 weeks
Visit 1screening
Week –5 to –6
Visit 2eligibilityWeek –4
Visit 4efficacysafety
Visit 5efficacysafety
Visit 6efficacysafety
Visit 7efficacysafety
Visit 3randomization
Week 0
Lead-in phase4 weeks
Rosuvastatin10 mg
Rosuvastatin20 mg
Rosuvastatin20 mg
Rosuvastatin20 mg
Placebo
Placebo
Randomized cross-over phase12 weeks (6 weeks + 6 weeks)
Maintenance phase12 weeks
After screening, the study included lead-in, randomized crossover, and maintenance phases.
Stein et al. J A C C V O L . 7 0 , N O . 9 , 2 0 1 7
Rosuvastatin in Children With Homozygous FH A U G U S T 2 9 , 2 0 1 7 : 1 1 6 2 – 7 0
1164
6 weeks either preceded or followed by 6 weeks ofplacebo in a 12-week crossover phase. Patients whosuccessfully completed the double-blind phaseentered the 12-week maintenance phase.
Eligibility criteria included male and female pa-tients with at least 1 of the following: genetic confir-mation of 2 mutated alleles of either the LDLR, apo B,or PCSK9 genes; or phenotype with untreated LDL-C>500 mg/dl and triglycerides <400 mg/dl; plus 1 ormore of the following: tendon or cutaneous xanthomabefore the age of 10 years or heterozygous familialhypercholesterolemia (HeFH) diagnosed by genetic orclinical criteria in both parents.
Fasting blood samples were analyzed for lipid andsafety parameters every 6 weeks after randomizationby a central laboratory (Medpace Reference Labora-tories, Cincinnati, Ohio, or Leuven, Belgium) thatmaintained Centers for Disease Control and Preven-tion part III lipid standardization and certification bythe College of American Pathologists throughout thetrial. Fasting LDL-C was determined by the Friede-wald equation (10).
Genotyping was performed either by a centrallaboratory (Laboratory for Molecular DiagnosticsExperimental Vascular Medicine, Academic MedicalCenter, Amsterdam, the Netherlands) if patientsprovided consent or obtained from the investigator ifit had been performed previously. LDLR functionalitywas characterized as either defective (2% to 25%) ornegative (<2%) if in vitro assessment of residual ac-tivity had been reported. Patients with differentmutations in both LDLR alleles were classified ac-cording to their estimated receptor activity. Patientswith an LDLR mutation combined with a mutation inapo B or PCSK9, or with 2 non-LDLR mutations, wereanalyzed separately.
To more robustly assess the LDL-C response on thebasis of underlying genetic mutations, we expandedthe patient population by combining data from the 13children in the HYDRA trial with 7 children ages 8 to17 years from a prior trial of HoFH patients who weretreated with diet alone for 4 weeks followed by6-weeks of rosuvastatin 20 mg daily (7). To assess theresponse in both children and adults, we furtherexpanded the analysis to include 33 adult patientsfrom the prior trial (7).
OBJECTIVES. The primary objective was to assessthe efficacy of rosuvastatin 20 mg daily on LDL-Ccompared with placebo. Secondary objectives wereto assess the efficacy of rosuvastatin 20 mg on otherlipids, lipoproteins, and apolipoproteins comparedwith placebo; the maintenance of efficacy over anadditional 12 weeks; and in a post hoc analysis, toexamine the association between HoFH genotypesand the LDL-C response to rosuvastatin. Additionalobjectives were to assess the short-term safety andtolerability of rosuvastatin compared with placebo.
STATISTICAL ANALYSIS. In the HYDRA study, theefficacy of rosuvastatin was analyzed in the log scaleusing a linear mixed-effects model with terms fortreatment and period as fixed effects, and patient as arandom effect. A similar model with an added cross-over period and treatment interaction term was usedto assess potential carryover effects between therosuvastatin and placebo treatment periods of thecrossover phase (an effect of the treatment sequence).Safety assessments were conducted during thescreening period and at 6-week intervals during thecrossover and maintenance phases. Analysis of rosu-vastatin efficacy with respect to genetic mutationsutilized Student t tests applied to the change

TABLE 1 Baseline Characteristics of Pediatric Patients
Randomized PediatricPatients (N ¼ 14)
Age, yrs 10.9 (7–15)
6 to <10 yrs 4 (29)
10 to <18 yrs 10 (71)
Male 7 (50)
Ethnicity
White 10 (71)
Black 1 (7)
Asian 3 (21)
On apheresis 7 (50)
On ezetimibe 8 (57)
Values are mean (range) or n (%).
TABLE 2 Changes in LDL-C and Other Lipids and Lipoproteins: Crossover Phase
Parameter(n ¼ 13) Treatment
Mean � SD*(mg/dl)
AbsoluteDifference(mg/dl)
MeanPercentChange 95% CI
pValue
LDL-C RSV 20 mg 396 � 196 �85.4 �22.3 �33.5 to �9.1 0.005
Placebo 481 � 185
TC RSV 20 mg 448 � 195 �91.4 �20.1 �29.7 to �9.1 0.003
Placebo 539 � 185
Non–HDL-C RSV 20 mg 412 � 199 �93.2 �22.9 �33.7 to �10.3 0.003
Placebo 505 � 186
Apo B RSV 20 mg 235 � 107 �33.0 �17.1 �29.2 to �2.9 0.024
Placebo 268 � 86
HDL-C RSV 20 mg 36 � 7 1.8 7.4 �7.4 to 24.5 0.314
Placebo 34 � 8
TG RSV 20 mg 80 � 24 �39.6 �30.4 �44.2 to �13.3 0.004
Placebo 120 � 53
*Following 6 weeks of treatment with either rosuvastatin or placebo.
Apo B ¼ apolipoprotein B; CI ¼ confidence interval; HDL-C ¼ high-density lipoprotein cholesterol;LDL-C ¼ low-density lipoprotein cholesterol; RSV ¼ rosuvastatin; TC ¼ total cholesterol; TG ¼ triglycerides.
J A C C V O L . 7 0 , N O . 9 , 2 0 1 7 Stein et al.A U G U S T 2 9 , 2 0 1 7 : 1 1 6 2 – 7 0 Rosuvastatin in Children With Homozygous FH
1165
from baseline data. To assess a potential trend inrosuvastatin efficacy between genetic mutations(LDLR defective/LDLR defective, LDLR defective/LDLR negative, and LDLR negative/LDLR negative), aheteroscedasticity adjusted linear regression wasused.
RESULTS
Twenty patients were enrolled in the screening periodof the HYDRA study, 14 of whommet eligibility criteriaand were randomized; 13 completed the 24-weekstudy (Online Figure 1). Of the 6 patients not ran-domized, 3 patients withdrew consent, and 3 did notfulfill eligibility criteria. The 1 patient who dis-continued therapy during the crossover phase did sodue to repeated difficulty with venous access duringblood collection. The baseline characteristics (Table 1)included amean age of 10.9 years (range: 7 to 15 years),one-half were male, 71% were Caucasian, one-halfwere on apheresis, and 57% were on ezetimibe. Thir-teen patients had confirmed genetic mutationsconsistent with HoFH, whereas the 1 patient withoutgenetic testing met clinical eligibility criteria and hadan LDL-C of 768 mg/dl on entry into the study.
EFFICACY. Due to pre-randomization therapy thatallowed continuation of ezetimibe and/or apheresis,and during which rosuvastatin treatment was insti-tuted or maintained, LDL-C values at the end of the6-week placebo phase were used as the baseline forcomparison to the 6-week rosuvastatin 20 mg phase(Table 2). The mean � SD LDL-C level on placebo was481 � 185 mg/dl. This compared to a mean LDL-C onrosuvastatin 20 mg of 396 � 196 mg/dl, representing amean absolute reduction in LDL-C of 85.4 mg/dl and aleast-squares mean relative difference versus placeboof �22.3% (95% confidence interval: �33.5% to �9.1%;p ¼ 0.005). No carryover effect was seen on the basis
of the treatment sequence (p ¼ 0.869). Efficacyobserved in patient subgroups on ezetimibe, onapheresis, by age, and by sex is shown in Figure 2.During the maintenance period, the least-squaresmean reduction in LDL-C was 19.3% (p ¼ 0.009)(Figure 3). Reductions in apo B, and other apo B-containing lipoproteins, paralleled those for LDL-C,with mean absolute reductions of 33 mg/dl (17.1%)in apo B (p ¼ 0.024) and 93.2 mg/dl (22.9%) in non–HDL-C (p ¼ 0.003) (Table 2, Figure 3). Mean absolutereductions in triglycerides of 39.6 mg/dl (30.4%;p ¼ 0.004) were seen with rosuvastatin 20 mgcompared with placebo (Table 2). Nonstatisticallysignificant increases in HDL-C of 1.8 mg/dl (7.4%;p ¼ 0.314) occurred with rosuvastatin 20 mg versusplacebo during the crossover phase together with anominally significant 11.2% increase during themaintenance phase (p ¼ 0.026).
LDL-C RESPONSE ASSOCIATED WITH GENETIC
MUTATIONS. The LDL-C response based on geneticmutations was evaluated in 19 of 20 pediatric pa-tients, because 1 patient was not genotyped, and in 33adults. The LDL-C reductions based on LDLR sub-groups and other mutations in children are shown inTable 3 and in the combined 53 pediatric and adultpatients in Table 4. Of the pediatric patients, 18 wereconfirmed as having $2 mutant alleles in the LDLR,apo B gene, or combinations thereof, and 1 patienthad mutations in both LDLR adaptor protein alleles(autosomal recessive hypercholesterolemia [ARH]).Of the 33 adults, 32 had $2 mutant alleles in theLDLR, apolipoprotein B gene, or combinationsthereof, and 1 patient had ARH. The remaining adult

FIGURE 2 LDL-C Response by Subgroups
–60
Favors RSV
Overall (n = 13)Apheresis (n = 7)
No apheresis (n = 6)Lead-in rosuvastatin 10 mg (n = 9)
Ezetimbe (n = 8)2 LDL receptor mutations (n = 11)
Age group 10–17 years (n = 9)Male (n = 7)
Female (n = 6)Favors PBO
–40 –20
LDL-C
0 20LS Mean % Change and 95% CI
Least-squares (LS) mean (�95% confidence interval [CI]) percentage change in low-density lipoprotein cholesterol (LDL-C) from baseline to
week 12 is shown with rosuvastatin (RSV) relative to placebo (PBO) by baseline characteristics. LDL ¼ low-density lipoprotein.
FIGURE 3 Change
0
–20
–15
–10
–5
Rela
tive
Bene
fit o
f Ros
uvas
tatin
20
mg
Vers
us P
lace
bo (%
)
–25
L
–22.p = 0.0
Significant difference
cholesterol, non–hig
(Apo) B between ros
LS mean during the
Stein et al. J A C C V O L . 7 0 , N O . 9 , 2 0 1 7
Rosuvastatin in Children With Homozygous FH A U G U S T 2 9 , 2 0 1 7 : 1 1 6 2 – 7 0
1166
patient who met eligibility for the HoFH study byclinical criteria had only a single identifiable LDLRmutation and achieved a 43.2% reduction in LDL-Cwith rosuvastatin 20 mg. In children with 2 negativeLDLR mutations, the mean LDL-C on diet alone orplacebo was 427.8 � 81.5 mg/dl, which was lower thananticipated; however, all 5 patients were also onapheresis, which is known to reduce LDL-C by about30% from pre-treatment levels (1,2). For comparison,the baseline/placebo mean LDL-C was 507.6 �184.6 mg/dl and 565.7 � 211.5 mg/dl for the 9 patientswith 2 defective LDLR mutations and the 3 patientswith 1 defective and 1 negative LDLR mutation,
in LDL-C and Other Lipid Parameters
DL-C Non-HDL-CTotalCholesterol
Apo B
305
–19.3p = 0.009 –20.1
p = 0.003
–16.9p = 0.009
–22.9p = 0.003
–19.5p = 0.007
–17.1p = 0.024
–14.4p = 0.039
Cross-Over (n = 13) Maintenance (n = 11)*
s were seen in the LS mean relative difference in LDL-C, total
h-density lipoprotein cholesterol (non–HDL-C), and apolipoprotein
uvastatin and placebo during the crossover double-blind phase and
open-label maintenance phase. Abbreviations as in Figure 2.
respectively. Only 3 of these 12 patients were onapheresis (Table 3).
Similar differences in baseline and placebo LDL-Cbetween the LDLR genotypes were seen in the com-bined group of adults and children (Table 4), where all8 patients with 2 negative LDLR mutations were onapheresis. The largest mean reductions in LDL-C withrosuvastatin were seen in the subgroup with the mostresidual LDLR activity; that is, in those with 2defective LDLR mutations: 23.5% (p ¼ 0.0044) and21.3% (p < 0.0001) in the children and all patients,respectively (Tables 3 and 4). In the 3 children with 1LDLR negative mutation, the reductions were lessand not statistically significant, but when pooled withthe adults to provide more robust numbers, the sub-group with 1 defective and 1 negative mutation in theLDLR demonstrated a mean reduction in LDL-C of17.0% (p ¼ 0.014). The lowest reductions in LDL-Cwere seen in the subgroup with 2 negative LDLRmutations: 12.9% (p ¼ 0.022) and 14.0% (p ¼ 0.038) inthe children and all patients, respectively. Amongthe patients with 2 LDLR mutations, a trendof �27.8 mg/dl in absolute LDL-C reduction(p ¼ 0.008) was found as the number of negativeLDLR mutations increased from 0 to 1 to 2. Compari-sons of the responses in adult and pediatric patientswith these LDLR mutation combinations are shown inthe Central Illustration. The child and adult with ARHexperienced LDL-C reductions of 40.3% and 26.6%,respectively, while the single patient with an apo Band an LDLR defect had an LDL-C reduction of 43.2%.
SAFETY. Rosuvastatin 20 mg daily was well toler-ated, with no patient terminating the trial or experi-encing drug discontinuations or dose interruptionsdue to treatment-related adverse events. The onlypatient terminating prematurely did so due to

TABLE 3 Response to Rosuvastatin in Pediatric HoFH Patients*
LDLR Status Based on Genetic Mutations PatientsPatients onApheresis
Baseline LDL-C†(mg/dl)
Absolute LDL-CReduction (mg/dl)
LDL-CReduction (%) p Value
All HoFH patients 20 8 (40.0) 503.5 � 177.3 89.7 � 77.2 20.2 � 16.4 <0.0001
LDLR defective/LDLR defective mutations 9 2 (22.2) 507.6 � 184.6 106.7 � 71.5 23.5 � 17.9 0.0044
LDLR defective/LDLR negative mutations 3 1 (33.3) 565.7 � 211.5 25.7 � 66.0 8.0 � 14.2 0.43
LDLR negative/LDLR negative mutations 5 5 (100.0) 427.8 � 81.5 54.0 � 35.6 14.0 � 10.2 0.038
LDLR defective/apo B mutations 1 0 (0.0) 229 122 43.2 N/A
Autosomal recessive hypercholesterolemia 1 0 (0.0) 699 282 40.3 N/A
Values are n, n (%), or mean � SD. *Data are combined from this and a prior HoFH trial that included 7 children with efficacy data on rosuvastatin 20 mg (8). †LDL-C after 6 weeks of blindedplacebo or after 4 weeks of dietary therapy.
HoFH ¼ homozygous familial hypercholesterolemia; LDLR ¼ low-density lipoprotein receptor; other abbreviations as in Table 2.
J A C C V O L . 7 0 , N O . 9 , 2 0 1 7 Stein et al.A U G U S T 2 9 , 2 0 1 7 : 1 1 6 2 – 7 0 Rosuvastatin in Children With Homozygous FH
1167
repeated problems with venous access during bloodcollection. There were no serious adverse events, andthe overall frequency of adverse events was low(Table 5). The only adverse event considered by theinvestigators to be related to the study drug was a lowserum bicarbonate at a single visit, not confirmed onretesting, during the maintenance period. The resultsof laboratory parameters for hepatic, renal, andmuscle tests are shown in Online Table 1. There wereno elevations in hepatic transaminases or creatinekinase $2 times the upper reference range. In termsof renal function, all quantitative urine protein mea-sures were within normal limits at all visits, with theexception of 1 patient who had a history of protein-uria. Glomerular filtration rate and serum creatininewere within the normal range at all visits for allpatients.
DISCUSSION
The HYDRA study, the first randomized, placebocontrolled trial of any statin in pediatric HoFH pa-tients as young as 7 years of age, demonstrated sig-nificant and sustained reductions in LDL-C withrosuvastatin 20 mg daily of 85.4 mg/dl (22.3%)
TABLE 4 Response to Rosuvastatin in All Pediatric and Adult HoFH P
LDLR Status Based on Genetic Mutations PatientsPatients onApheresis
All HoFH patients 53 14 (26.4)
LDLR defective/LDLR defective mutations 32 5 (15.6)
LDLR defective/LDLR negative mutations 8 1 (12.5)
LDLR negative/LDLR negative mutations 8 8 (100.0)
LDLR defective/apo B mutations 1 0 (0.0)
1 LDLR defective mutation 1 0 (0.0)
Autosomal recessive hypercholesterolemia 2 0 (0.0)
Values are n, n (%), or mean � SD. *Combined data from this and a prior HoFH trial thaplacebo or after 4 weeks of dietary therapy.
Abbreviations as in Tables 2 and 3.
compared with placebo. Although no children in thisstudy had clinical evidence of CVD, atheroscleroticcardiovascular events in children under age 10 yearsare not uncommon (4,11), highlighting the increasedrisk of death or serious morbidity in children withHoFH. As reduction in CVD risk is related to absoluterather than percent decrease in LDL-C, the mean ab-solute decrease of 85.4 mg/dl seen with rosuvastatincould be anticipated from trials in non-FH and HeFHpatients to result in a clinically important reductionor delay in long-term cardiovascular morbidity andmortality (12,13). This would also be consistent withregistry data in HoFH and represents a benefit thatmay be even greater when LDL-C reduction is startedas early as 7 years of age, as in this trial (1,4).
The study also demonstrated that despite a meanreduction of 85.4 mg/dl with rosuvastatin, includingin those already receiving ezetimibe, apheresis, orboth, children with HoFH were unable to approachanywhere near optimal LDL-C levels. However,rosuvastatin did provide a good foundation on whichto add further LDL-C reducing agents such as ezeti-mibe, apheresis, and the PCSK9 inhibitor evolocu-mab, which, when added to stable statin therapy, hasbeen shown to be effective, well tolerated, and
atients*
BaselineLDL-C† (mg/dl)
Absolute LDL-CReduction (mg/dl)
LDL-CReduction (%) p Value
507.5 � 135.2 99.5 � 71.6 20.3 � 13.6 <0.0001
519.4 � 119.0 107.7 � 65.3 21.3 � 13.1 <0.0001
570.1 � 149.2 91.0 � 95.6 17.0 � 14.8 0.014
401.8 � 81.2 48.4 � 43.2 12.9 � 12.5 0.022
229 99 43.2 N/A
437 122 27.9 N/A
548.5 � 212.8 194.0 � 124.5 33.5 � 9.7 N/A
t included 7 children with efficacy data on rosuvastatin 20 mg (8). †LDL-C after 6 weeks of blinded

CENTRAL ILLUSTRATION Individual LDL-C Responses Related to Underlying Genetic Defects
Stein, E.A. et al. J Am Coll Cardiol. 2017;70(9):1162–70.
This study sought to assess the low-density lipoprotein cholesterol (LDL-C) efficacy of rosuvastatin in children with homozygous familial hypercholesterolemia (HoFH)
and the relationship with underlying genetic mutations. The latter was accomplished by adding children and adults ($18 years of age) from a previous HoFH study.
Low-density lipoprotein receptor (LDLR) functionality was characterized as either defective (2% to 25%) or negative (<2%) if in vitro assessment of residual activity
had been reported; classification of patients with different mutations in both LDLR alleles was based on their estimated receptor activity. Use of rosuvastatin was
found to be safe and effective in a pediatric HoFH population with the LDL-C response in children and adults related to underlying genetic mutations.
Stein et al. J A C C V O L . 7 0 , N O . 9 , 2 0 1 7
Rosuvastatin in Children With Homozygous FH A U G U S T 2 9 , 2 0 1 7 : 1 1 6 2 – 7 0
1168

TABLE 5 AE Frequency
Any AE
Rosuvastatin20 mg (n ¼ 13)
Placebo(n ¼ 14)
Overall(N ¼ 14)
Patients AEs Patients AEs Patients AEs
Lead-in phase (RSV 10 mg) 3 (27.3) 4 – – 3 (27.3) 4
Crossover phase 1 (7.7) 1 4 (28.6) 4 4 (28.6) 5
Maintenance phase* 1 (7.7) 1 – – 1 (7.7) 1
Values are n (%) or n. *Only the 1 AE, an isolated low bicarbonate, in the maintenance phase wasassessed by the investigator to be causally related to study drug.
AE ¼ adverse event; RSV ¼ rosuvastatin.
PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE:
Patients with HoFH have extremely elevated LDL-C levels from
conception, and are at very high risk of accelerated atheroscle-
rotic CVD. Treatment with
statins should start at diagnosis; however, no statin has been
formally evaluated for use in HoFH children.
TRANSLATIONAL OUTLOOK: Rosuvastatin 20 mg alone or in
combination with ezetimibe and/or apheresis demonstrated
effective LDL-C reduction in children and adolescents with HoFH.
J A C C V O L . 7 0 , N O . 9 , 2 0 1 7 Stein et al.A U G U S T 2 9 , 2 0 1 7 : 1 1 6 2 – 7 0 Rosuvastatin in Children With Homozygous FH
1169
approved for children with HoFH 13 years of age orolder (9). Of the 2 orphan drugs approved for HoFH,the microsomal triglyceride transfer protein inhibitorlomitapide has not been studied or approved in apediatric population, and mipomersen, an apo Bsynthesis inhibitor, is not approved for use inchildren <12 years. In addition, both drugs are notwell tolerated, and have significant side effects andsubstantial monitoring requirements (8).
The combination of the 13 children in the HYDRAstudy, together with the 7 children from a previousHoFH trial (7), allowed, for the first time, a broaderassessment of rosuvastatin response in a pediatricHoFH population as it relates to underlying geneticdefects. The larger group of children also enabled acomparison with the response in adults. Overall, itconfirmed that HoFH children, like adults, with moreresidual LDLR activity respond with greater LDL-Creduction. However, unlike PCSK9 inhibition, whichresults in no LDL-C decrease in receptor-negativepatients (9), rosuvastatin produced a nearly 13%, or50 mg/dl, reduction in these patients, which wouldstill be anticipated to result in a long-term CVDbenefit. This supported the beneficial additionalmechanism of 3-hydroxy-3-methylglutaryl coenzymeA reductase inhibition, not only by up-regulatingLDLR activity through increased LDLR synthesis,but also by decreasing hepatic cholesterol and lipo-protein production (6,7).
Rosuvastatin 20 mg daily was well tolerated, andno safety signals were seen in HoFH children asyoung as 7 years of age. The safety and tolerabilitywere consistent with, and confirmatory of, 2 largerand longer-term rosuvastatin trials in 375 HeFH pe-diatric patients ages 6 to 17 years (14,15). In both tri-als, children received rosuvastatin 5, 10, or 20 mgdaily for periods up to 2 years. Rosuvastatin at alldoses was well tolerated with no hepatic, skeletalmuscle, or renal adverse events resulting in perma-nent treatment discontinuation. In neither of thesepediatric trials were there clinically importantchanges in renal function or signs of adverse effectson growth or sexual maturation.
On the basis of the efficacy and safety from thistrial, the U.S. Food and Drug Administration hasapproved rosuvastatin for the treatment of HoFHpediatric patients 7 to 17 years of age (16).
STUDY LIMITATIONS. Limitations of the studyincluded the short duration of rosuvastatin treat-ment, which might not reflect either longer-term ef-ficacy or safety for a disorder where lifetime therapyis needed. However, the similar response in adultswith HoFH indicate that increasing age, diet, or
lifestyle does not alter LDL-C efficacy. Second,despite that this pediatric-specific HoFH trial was thelargest to evaluate children, it was still relativelysmall. Lastly, it did not provide any information as tothe ultimate impact on cardiovascular events in thisvery high-risk population.
CONCLUSIONS
The HYDRA study, the first-ever pediatric HoFH trialwith a statin, demonstrated effective LDL-C reductionwith rosuvastatin 20 mg alone or in combination withezetimibe and/or apheresis, and resulted in U.S. Foodand Drug Administration approval of rosuvastatin forthe treatment of HoFH pediatric patients 7 to 17 yearsof age. Combined with additional pediatric HoFHpatients from a prior trial, the LDL-C response torosuvastatin was related to the underlying FH-causing mutations and was consistent with thatseen in adults.
ACKNOWLEDGMENT The authors thank KerrenDavenport at Prime-Medica for editorial support.
ADDRESS FOR CORRESPONDENCE: Dr. Evan A.Stein, Metabolic and Atherosclerosis Research Center,5355 Medpace Way, Cincinnati, Ohio 45227. E-mail:[email protected].

Stein et al. J A C C V O L . 7 0 , N O . 9 , 2 0 1 7
Rosuvastatin in Children With Homozygous FH A U G U S T 2 9 , 2 0 1 7 : 1 1 6 2 – 7 0
1170
RE F E RENCE S
1. Cuchel M, Bruckert E, Ginsberg HN, et al.Homozygous familial hypercholesterolaemia: newinsights and guidance for clinicians to improvedetection and clinical management. A positionpaper from the Consensus Panel on FamilialHypercholesterolaemia of the European Athero-sclerosis Society. Eur Heart J 2014;35:2146–57.
2. Sjouke B, Kusters DM, Kindt I, et al. Homozy-gous autosomal dominant hypercholesterolaemiain the Netherlands: prevalence, genotype-phenotype relationship, and clinical outcome. EurHeart J 2015;36:560–5.
3. Raal FJ, Santos RD. Homozygous familial hy-percholesterolemia: current perspectives on diag-nosis and treatment. Atherosclerosis 2012;223:262–8.
4. Raal FJ, Pilcher GJ, Panz VR, et al. Reduction inmortality in subjects with homozygous familialhypercholesterolemia associated with advances inlipid-lowering therapy. Circulation 2011;124:2202–7.
5. Raal FJ, Pappu AS, Illingworth DR, et al. Inhi-bition of cholesterol synthesis by atorvastatin inhomozygous familial hypercholesterolaemia.Atherosclerosis 2000;150:421–8.
6. Raal FJ, Pilcher GJ, Illingworth DR, et al.Expanded-dose simvastatin is effective in homo-zygous familial hypercholesterolaemia. Athero-sclerosis 1997;135:249–56.
7. Marais AD, Raal FJ, Stein EA, et al. A dose-titration and comparative study of rosuvastatinand atorvastatin in patients with homozygous fa-milial hypercholesterolaemia. Atherosclerosis2008;197:400–6.
8. Rader DJ, Kastelein JJ. Lomitapide and mipo-mersen: two first-in-class drugs for reducing low-density lipoprotein cholesterol in patients withhomozygous familial hypercholesterolemia. Cir-culation 2014;129:1022–32.
9. Raal FJ, Honarpour N, Blom DJ, et al., TESLAInvestigators, for the TESLA investigators. Inhibi-tion of PCSK9 with evolocumab in homozygousfamilial hypercholesterolaemia (TESLA Part B): arandomised, double-blind, placebo-controlledtrial. Lancet 2015;385:341–50.
10. Friedewald WT, Levy RI, Fredrickson DS. Esti-mation of the concentration of low-density lipo-protein cholesterol in plasma, without use of thepreparative ultracentrifuge. Clin Chem 1972;18:499–502.
11. Goldstein JL, Hobbs HH, Brown MS. Familialhypercholesterolemia. In: Scriver CR, Beaudet AL,Sly WS, Valle D, editors. The Metabolic and Mo-lecular Bases of Inherited Disease. New York, NY:McGraw-Hill; 2001:2863–913.
12. Cholesterol Treatment Trialists Collaboration,Baigent C, Blackwell L, Emberson J, et al. Efficacyand safety of more intensive lowering of LDLcholesterol: a meta-analysis of data from 170,000
participants in 26 randomised trials. Lancet 2010;376:1670–81.
13. Neil A, Cooper J, Betteridge J, et al. Re-ductions in all-cause, cancer, and coronarymortality in statin-treated patients with hetero-zygous familial hypercholesterolaemia: a pro-spective registry study. Eur Heart J 2008;29:2625–33.
14. Avis HJ, Hutten BA, Gagne C, Langslet G, et al.Efficacy and safety of rosuvastatin therapy forchildren with familial hypercholesterolemia. J AmColl Cardiol 2010;55:1121–6.
15. Braamskamp MJ, Langslet G, McCrindle BW,et al. Efficacy and safety of rosuvastatin therapy inchildren and adolescents with familial hypercho-lesterolemia: Results from the CHARON study.J Clin Lipidol 2015;9:741–50.
16. AstraZeneca. Crestor prescribing information.2016. Available at: http://www1.astrazeneca-us.com/pi/crestor.pdf. Accessed February 15, 2017.
KEY WORDS apheresis, low-densitylipoprotein cholesterol, low-densitylipoprotein receptor, pediatrics, statins
APPENDIX For a supplemental figure andtable, please see the online version of thispaper.