Embed Size (px)
Citation preview

PREOPERATIVE ASSESMENT IN COCHLEAR IMPLANTATION
Dr. D.Sunil Kumar

Objectives of Imaging
• To review the findings that influence surgeon on the accurate patient selection, type of device and surgical approach.
• To detect any absolute contraindication, and incidental anatomical abnormalities.

Imaging Techniques
• HRCT Temporal Bone:– detailed evaluation of the osseous anatomy of the inner
and middle ear– assessment of mastoid pneumatization– degree of middle-ear aeration.
Disadvantages:Ionising RadiationDoes not directly depict the cochlear nerve,shows only
the bone channel that contains it.

• Magnetic resonance (MR) imaging
• High-resolution heavily T2-weighted 3D imaging techniques– direct visualization of the cisternal
and intracanalicular vestibulocochlear nerve bundles.
– detailed information about the fluid-filled labyrinth.
• Oblique sagittal images obtained perpendicular to VIIth-VIIIth nerve complexes through the internal auditory canal help distinguish the cochlear division of the eighth nerve.

Normal anatomy• Inner Ear• The inner ear consists of the fluid-
filled membranous labyrinth, which is enclosed by the bone of the osseous labyrinth.
• The cochlea is the primary organ of hearing.It is a spiral structure having 2.5–2.75 turns around a central column of bone (the modiolus).
• A spiral osseous lamina projects from the modiolus and divides the cochlear canal into upper (scala vestibuli) and lower (scala tympani) compartments; the scala tympani is the implantation destination.

• The vestibular system, which is located posterolateral to the cochlea, is formed by the vestibule and three semicircular canals: superior, posterior, and lateral .
• These structures play a minor role in hearing, but abnormalities often occur in conjunction with cochlear malformations.




Technique for Cochlear Implantation • The standard surgical technique for electrode placement
is – Mastoidectomy– opening of the facial recess to gain access to the middle-ear
cavity in the vicinity of the round window niche– Traditionally, a cochleostomy was created that was anterior-
inferior to the round window membrane, with the electrode array then inserted into the scala tympani of the basal turn through the cochleostomy .
• However, round window insertion is becoming more common in patients with substantial residual hearing, and the occurrence of fewer traumas to the cochlea is thought to be advantageous in preserving existing function.

• Mastoid and Middle Ear Anatomy
• Access to the cochlea from the mastoid by partial mastoidectomy. is central to placing the cochlear implant.
• Important bone landmarks, such as the facial nerve recess and round window niche, are used by the surgeon to gain access to the cochlea for placement of the cochlear implant electrode array.

VIII th nerve complex• The anatomy of the facial and vestibulocochlear nerve varies
on their way through the cerebellopontine angle (CPA) and IAM.
• In the CPA the facial nerve has an anterior and slightly superior put (which remains in this position in its entire length) and the vestibulocochlear nerve has a posteroinferior position.
• At the middle third of internal auditory canal, the arrangement of the facial, cochlear, and superior and inferior vestibular nerves is in the following manner:anterosuperior, anteroinferior, posterosuperior, posteroinferior.
• Cochlear nerve is larger than either the superior or inferior vestibular nerves in 90% of normal cases and it is of almost the same size or larger than the facial nerve in 64% of cases.


• Are There Cochleovestibular Anomalies that Preclude Implantation?
• Is There Evidence of Luminal Obstruction?• Are There Additional Findings that May
Complicate the Surgery or Subsequent Patient Management?

• Are There Cochleovestibular Anomalies that Preclude Implantation?

IAC and Cochlear Nerve Anomalies• IAC – Normal – 2-8mm
Average – 4mm Stenotic – 2 mm
• The IAC may also be atretic or may have a bony septum that partitions it into two or more separate canals.
• The morphologic characteristics and size of the IAC are not reliable indicators of the integrity of the cochlear nerve.
• High-resolution MR imaging is the preferred modality for accurate assessment of the cochlear nerve
• Sagittal oblique images obtained in a plane perpendicular to the long axis of the IAC provide the best depiction of the four major nerves of the IAC

Axial 0.8-mm-thick SSFP MR image shows the parallel courses of the facial(black arrowheads) and superior vestibular (white arrowheads) nerves as they cross the cerebellopontine angle to enter the internal auditory canal through the porus acusticus (double arrow).

Sagittal image shows the four nerves within the IAC: the facial nerve (straight arrow), cochlear nerve (curved arrow), and superior and inferior vestibular nerves (arrowheads).

• Three types of cochlear nerve anomalies have been described
• Type 1 cochlear nerve anomaly - stenotic IAC is seen with an absent eighth nerve.

• Type 2 anomaly, a common vestibulocochlear nerve is found, with hypoplasia or aplasia of its cochlear branch. – Type 2a – associated innerear malformations– Type 2b - isolated

Cochlear nerve aplasia in a 4-year-old girl with congenital hearing loss who wasunder consideration for cochlear implantation. left (a) and right (b) internal auditory canals, show the main branches of the facial and vestibulocochlear nerves in cross section. The anterior (A), posterior (P), superior (S), and inferior (I) aspects of the canals are labeled for ease of orientation. Absent cochlear nerve noted on right side

• At CT, stenosis of cochlear aperture(small canal at the fundus of the IAC, through which the cochlear nerve passes to enter the cochlea) indirectly indicates hypoplasia or absence of the cochlear nerve.
• Although the criteria for a normal aperture size are not well defined in the literature, an aperture with a diameter smaller than 2 mm is usually considered abnormal.

• Implications for Cochlear implantation:• A small nerve is only a relative contraindication to cochlear
implantation. An appreciably thin cochlear nerve, may still effectively transmit impulses to allow hearing.
• At one time, evidence of an absent or severely dysplastic cochlear nerve was considered an absolute contraindication to cochlear implantation in any patient.
• More recently, implantation in children with an absent or deficient eighth nerve was performed with varying results.
• Outcomes are more difficult to predict and poorer than expected compared with those in patients with normal nerve anatomy but some young children have achieved substantial word recognition and spoken language skills .(Young NM, Kim FM, Ryan ME, Tournis E, Yaras S. Pediatric cochlear implantation of children with eighth nerve deficiency. Int J Pediatr Otorhinolaryngol 2012;76(10):1442–1448. )

• A potential alternative treatment for children with cochlear nerve deficiency is auditory brainstem implantation.
• Auditory brainstem implantation is currently approved by the FDA only for use in individuals who are deafened by neurofibromatosis type II and are aged 12 years and older.

Cochleovestibular Abnormalities • Jackler et al. hypothesised that dysplasias result
from a developmental arrest during varying stages of inner ear organogenesis and identified the following groups: – labyrinthine aplasia– cochlear aplasia– cochlear hypoplasia– common cavity malformation– incomplete partitioning• cystic cochleovestibular dysplasia (incomplete partitioning
type I)• incomplete partitioning type II (true Mondini malformation)

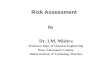
• Michel aplasiaMichel aplasia, also known as complete labyrinthine aplasia characterised by complete absence of cochlea and vestibular structures, is a rare congenital inner ear abnormality, accounting for approximately 1% of cochlear bony malformations. The internal auditory canals (IACs) may be small in size or absent.Cochlear nerve deficiency will be seen.

Complete labyrinthine aplasia. (a) Axial high-resolution CT image shows the absence of inner ear structures. Note the flat medial wall of the middle ear cavity (arrow) and the hypoplastic petrous bone (*). (b) Coronal CT image shows an atretic IAC (arrow). (c) Sagittal MR image obtained in a plane perpendicular to the IAC depicts a single nerve (arrow) within the small IAC. Combined with the findings in a and b, this feature is suggestive of absence of the eighth cranial nerve.

• Cochlear aplasia– Cochlea – absent with dense otic bone at the site of cochlea.– Vestibular system- normal,dilated or hypoplastic

• Implications for cochlear implantation:• Complete labyrinthine and cochlear aplasia
are rare, constituting less than 1% and 3%, respectively, of cochlear bone abnormalities.
• Cochlear and labyrinthine aplasia, are considered to be absolute contraindications; in spite of reports questioning it.

• Common cavity– single cavity that represents the undifferentiated
cochlea and vestibule with no internal archictecture– The semicircular canals are frequently malformed but
occasionally normal

• The modiolus is absent, and the opening of the internal auditory canal into the common cavity malformation is abnormal, which may account for the increased presence of CSF in these malformations (in contrast to perilymph fluid in a normal labyrinth)
• Hence there is increased incidence of spontaneous CSF leakage into the middle ear and recurrent meningitis in these anomalies

• A cochlear implant can be successfully placed into a common cavity malformation, but the procedure may be technically challenging.
• If CSF is already present within the cochlea, a brisk leak of CSF may be encountered after cochleostomy is performed.
• The leak must be effectively sealed to minimize the risk for meningitis.
• Even if there is initially no CSF within the common cavity malformation, the electrode array may be wrongly positioned into the internal auditory canal, resulting in a CSF leak
• CSF leakage may be avoided by controlling the tip of the array at the time of insertion; thus, identifying this type of malformation may influence the choice of electrode array and cochleostomy technique.

• Cochlear aplasia vs Common cavity:• Look beneath the cochlear promontry!!• cochlear aplasia - dense sclerotic bone• Common cavity – deformed cavity beneath
promontry

Incomplete partition I(cystic cochleovestibular Malformation)vestibule is distinguishable from the cochlea• Cochlea – no bony modiolus, resulting in an empty
cystic cochlea• Vestibule – cystic dilatation• Figure of 8 appearance• The cribriform area between the cochlea and IAC is
often defective, and all patients have a large IAC, predisposing them to increased risks for meningitis and for a perilymphatic gusher in the event of surgery

Type I incomplete partition. (a) Axial CT image shows a cystic cochlea without any internal architecture, accompanied by a dilated vestibule that forms a figure eight (straight arrow). Note the coexistent mucosal disease in the mastoid air cells and middle ear (curved arrow). (b, c) Axial CT (b) and MR (c) images obtained in another patient show a cystic cochlea (white arrowhead) that is separated from a dilated IAC (curved arrow) by a partially dehiscent cribriform plate (black arrowhead). Straight arrow in b = opacification of the middle ear and mastoid air cells.

• Cochlear Hypoplasia• The cochlea and vestibule can be
differentiated from each other but the size of the cochlea is smaller than normal.
• Cochlea – small with one or partial turn• Vestibule and semicircular canals –
malformed, may be normal• IAC - small



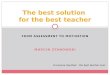
• Incomplete partition II (Mondini deformity) :
• most common type more than 50% of all cochlear deformities.
• Cochlea – Basal turn normal, middle and apical turns coalesce to form a cystic apex.
• Modiolus present in basal turn associated with a large endolymphatic duct and sac and an enlarged vestibular aqueduct
• Vestibule – dilated with normal semicircular canals.

Type II incomplete partition. (a) Axial CT image shows the absence of the modiolus from a cystic cochlear apex (straight arrow) formed by coalescent apical and middle turns. Dilatation of the vestibular aqueduct (arrowhead) and vestibule (curved arrow) and a coexistent middle ear effusion (*) also are seen. (b) Axial CT image obtained at a slightly lower level shows a normal basal turn of the cochlea (arrow). (c) Coronal CT image shows the cystic cochlear apex (arrow).

• In incomplete partition and cochlear hypoplasia, the cochlea is present but does not form the normal basal, middle, and apical turns.
• The surgical importance of these abnormalities is primarily determined by the degree of cochlear malformation and the potential for communication with CSF.
• Malformations with a dysplastic or absent modiolus are more likely to have CSF present in the cochlea, although an intact modiolus does not exclude the possibility of a fistula.

Enlarged Vestibular Aqueduct• The vestibular aqueduct is a bony canal that
extends from the medial wall of the vestibule, to the endocraneal surface of the posterior part of the petrous portion.
• It contains the endolymphatic duct, as an extension of the membranous labyrinth, which ends in cul-de-sac between the layers of the duramater
• An enlarged vestibular aqueduct, either by itself or in association with mild cystic cochlear dysplasia, has been reported to be the most common inner-ear malformation associated with SNHL
• Enlarged vestibular aqueduct (EVA) is commonly defined as having a width larger than 1.5 mm, measured at the midpoint of the common crus and external aperture


• Clinically, children with an enlarged vestibular aqueduct have hearing that ranges from normal to profoundly lost.
• The natural history is that of progressive but unpredictable hearing loss.
• Although the cause is unknown, one theory is that trauma may affect it by causing hemorrhage into the endolymphatic sac.
• To minimize the risk for a sudden decline in hearing, patients are generally counseled to wear a helmet and refraining from activities in which high-impact and unprotected head trauma are likely to occur.
• Once individuals with an enlarged vestibular aqueduct lose hearing to the degree that hearing aids are no longer sufficient, cochlear implantation is the only effective treatment option.

Vestibule and Semi- circular Canal Abnormalities
• Isolated anomalies of the vestibule or semicircular canal typically do not affect surgical planning.
• However absence of the semicircular canals is strongly associated with CHARGE syndrome.
• CHARGE syndrome is associated with cochlear dysplasias, dysplastic middle-ear cavity and an anomalous facial nerve course, which may complicate the surgical approach and cochleostomy

• Is There Evidence of Luminal Obstruction?

Cochlear Patency
• One of the most important causes of postnatal acquired SNHL is bacterial meningitis, which may have profound effects on cochlear patency that limit or preclude cochlear implantation.
• Deafness secondary to bacterial meningitis is often associated with labyrinthitis ossificans, a progressive process that may obstruct the cochlea.

• Labyrinthitis ossificans• Progressive condition characterised by fibrosis
of membranous labyrinth progressing to ossification.
• due to complication of meningitis, otosclerosis and trauma.
• commonly bilateral but may be asymmetrical. • Changes typically begin at the basal cochlear
turn and proceed apically

• Early implantation before the onset of substantial obstruction is necessary to achieve optimal electrode insertion and avoid the need for complex alternative surgical approaches, which have more variable outcomes.
• Early fibrotic changes of labyrinthitis ossificans are seen at MR imaging as a loss of the normal hyperintensity of fluid on T2-weighted images of the membranous labyrinth
• Labyrinthine enhancement may also accompany or precede fibrotic changes at contrast material–enhanced MR imaging

• In later stages ossification of membranous labyrinth are better depicted in CT than MRI.
• A completely mineralized labyrinth may mimic congenital absence of the cochlea and vestibule; however, in contrast to patients with hypoplasia, those with labyrinthitis ossificans should have a normal-sized internal auditory canal, petrous apex, and cochlear aperture.

• Cochlear ossification does not contraindicate the placement of cochlear implant, but it might complicate the surgical procedure.
• Preoperatively, is important to know the presence and extent of pathology to select the surgical approach and type of electrode

• Are There Additional Findings that May Complicate the Surgery or Subsequent Patient Management?

Other Anatomic Considerations
• Facial Nerve Anomalies– hypoplastic or
dehiscent facial nerve canal

• Vascular Anomalies– high-riding or dehiscent
jugular bulb– large occipital
transosseous veins may affect the placement of the postauricular incision
– an aberrant carotid artery

• Middle-Ear and Mastoid Variants
• Absence or dysplasia of the round window niche, which typically serves as a bone landmark for cochleostomy, necessitates the use of other structures to guide entry into the basal cochlear turn
• Assessing the configuration and pneumatization of mastoid air cells and the middle-ear cavity may also aid surgical planning
• Middle-ear opacification also limits visualization during surgery, and acute otomastoiditis requires treatment before implantation to decrease the risk for infection and meningitis.

Conclusions• Cochlear implantation is the first medical treatment
to enable deaf children to learn to talk and develop age-appropriate language and literacy.
• Imaging is an important part of the preoperative workup in these children.
• A greater understanding of the process for evaluating patients who are eligible for cochlear implantation, the surgical procedure, and the implant device itself enables the radiologist to provide more useful information to referring clinicians and ultimately improves the quality of care these children receive.