Embed Size (px)
Citation preview
Sponsored by
AAGLAdvancing Minimally Invasive Gynecology Worldwide
Excision of Endometriosis –
Laparoscopic and Robotic
MODERATOR
Mohamed Ibrahim, MD
FACULTY
Michelle Nisolle & Tamer A. Seckin, MD

Professional Education Information Target Audience This educational activity is developed to meet the needs of residents, fellows and new minimally invasive specialists in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 1.75 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME.
Table of Contents
Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 2 Excision of Endometriosis – Laparoscopic and Robotic M. Nisolle ...................................................................................................................................................... 3 Excision of Endometriosis – Laparoscopic and Robotic T.A. Seckin ................................................................................................................................................... 15 Cultural and Linguistics Competency ......................................................................................................... 36
Surgical Tutorial 9 Excision of Endometriosis – Laparoscopic and Robotic
Moderator: Mohamed Ibrahim
Michelle Nisolle & Tamer A. Seckin
Minimally invasive management of endometriosis has been the foundation for the advancement of minimally invasive surgery. When cases of the most severe endometriosis can be managed by operative laparoscopy, almost all other pathologies can be treated with a minimally invasive approach. The limiting factors are surgeon skill, which relies on knowledge of anatomy, and availability of proper instrumentation. In this course we will share treatment strategies for managing severe cases of endometriosis. These will include utilization of proper instruments, including robotics, in performing posterior cul-de-sac and pelvic side wall dissection. Alternative approaches to excision (ablation and fulguration) will be reviewed along with their indications in certain cases. Learning Objectives: At the conclusion of this course, the participant will be able to: 1) Recognize subtle and occult endometriosis in distorted anatomy; 2) select proper strategy in the management of severe endometriosis, including new techniques to improve the quality of excision surgery; 3) assess appropriate utilization of new technology; and 4) recognize potential complications and their prevention.
1
PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop and have no conflict of interest to disclose (in alphabetical order by last name). Art Arellano, Professional Education Manager, AAGL* Viviane F. Connor Consultant: Conceptus Incorporated Kimberly A. Kho* Frank D. Loffer, Executive Vice President/Medical Director, AAGL* Linda Michels, Executive Director, AAGL* M. Jonathan Solnik* Johnny Yi*
SCIENTIFIC PROGRAM COMMITTEE Ceana H. Nezhat Consultant: Ethicon Endo-Surgery, Lumenis, Karl Storz Other: Medical Advisor: Plasma Surgical Other: Scientific Advisory Board: SurgiQuest Arnold P. Advincula Consultant: Blue Endo, CooperSurgical, Covidien, Intuitive Surgical, SurgiQuest Other: Royalties: CooperSurgical Linda D. Bradley* Victor Gomel* Keith B. Isaacson* Grace M. Janik Grants/Research Support: Hologic Consultant: Karl Storz C.Y. Liu* Javier F. Magrina* Andrew I. Sokol* FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Mohamed Ibrahim* Michelle Nisolle* Tamer Seckin* Asterisk (*) denotes no financial relationships to disclose.
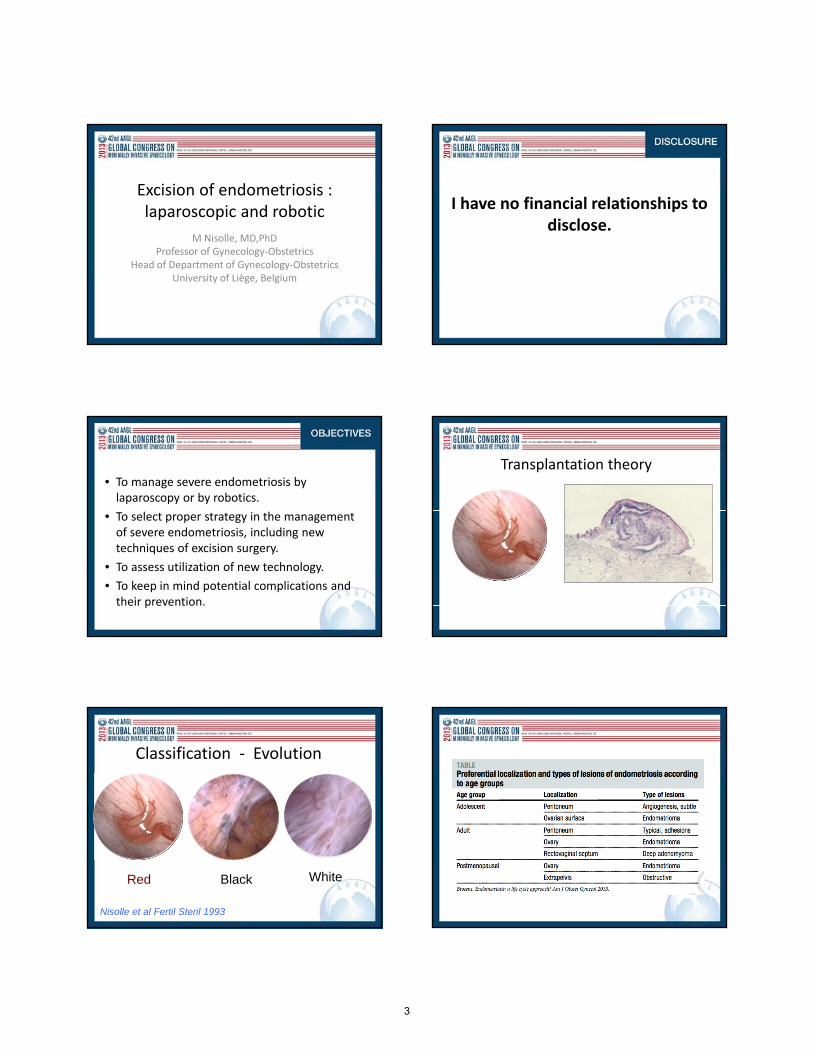
Excision of endometriosis : laparoscopic and robotic
M Nisolle, MD,PhDProfessor of Gynecology‐Obstetrics
Head of Department of Gynecology‐ObstetricsUniversity of Liège, Belgium
I have no financial relationships to disclose.
• To manage severe endometriosis by laparoscopy or by robotics.
• To select proper strategy in the management of severe endometriosis, including new techniques of excision surgery.
• To assess utilization of new technology.
• To keep in mind potential complications and their prevention.
Transplantation theory
Classification ‐ Evolution
Red
Nisolle et al Fertil Steril 1993
Black White
3
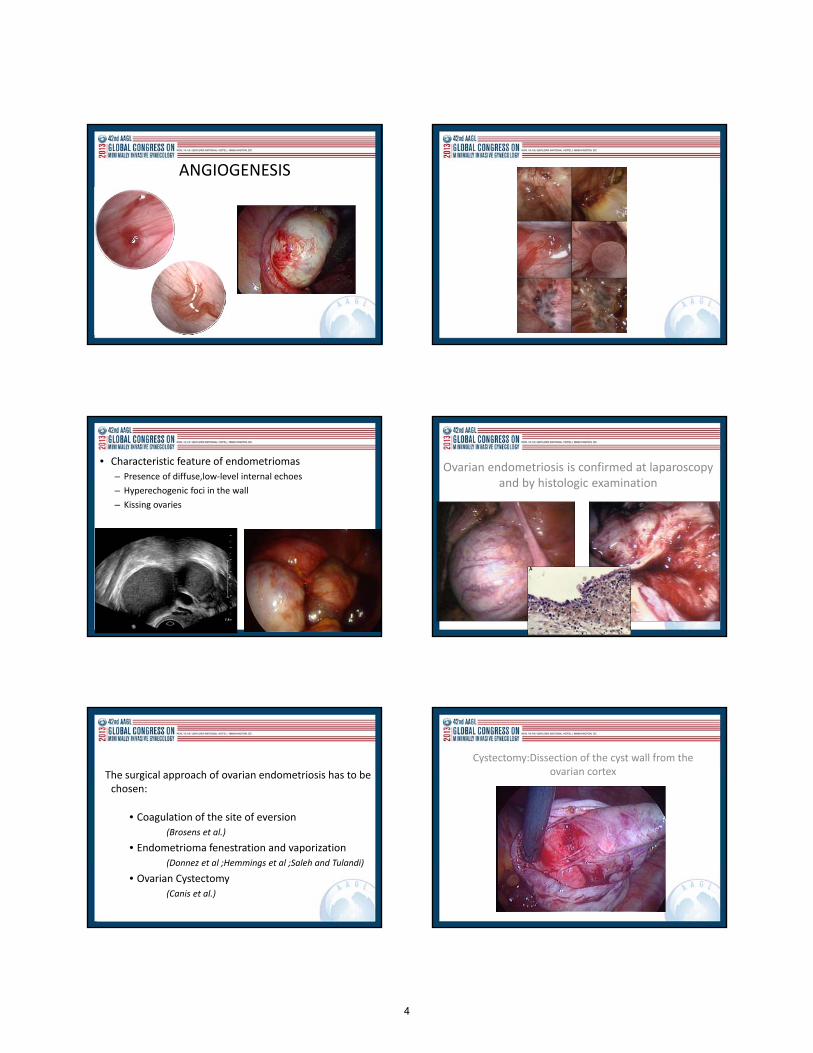
ANGIOGENESIS
• Characteristic feature of endometriomas
– Presence of diffuse,low‐level internal echoes
– Hyperechogenic foci in the wall
– Kissing ovaries
Ovarian endometriosis is confirmed at laparoscopy and by histologic examination
The surgical approach of ovarian endometriosis has to be chosen:
• Coagulation of the site of eversion(Brosens et al.)
• Endometrioma fenestration and vaporization
(Donnez et al ;Hemmings et al ;Saleh and Tulandi)
• Ovarian Cystectomy
(Canis et al.)
Cystectomy:Dissection of the cyst wall from the ovarian cortex
4

Large Endometrioma>3 cm in diameter
1/Adhesiolysis
2/Aspiration of chocolate fluid
3/Vaporization of peritoneal lesions
4/Cystectomy
or combined treatment:
4/Medical therapy and
Second look laparoscopy
Ovarian endometriosis: plasmajet
Risk of Recurrence at 1 year
EXCISION COAGULATION
Hemmings et al (Retro; 1998) 8 % 12 %
Berreta et al (RCT; 1998) 6 % 18 %
Saleh and Tulandi (Retro; 1999) 6.1 % 21.9 %
Alborzi et al (RCT; 2004) 5.8 % 22.9 %
Cochrane Review
Hart et al. Hum Reprod 2005 ; 11: 3000-7
There is some evidence that excisional surgery for endometriomata providesa more favourable outcome than drainage and ablation with regard to the
- recurrence of the endometrioma- recurrence of symptoms- subsequent spontaneous pregnancy
Cystectomy:
Risk of removal normal ovarian tissue and ovocytes
Residual ovarian volumeafter surgery
Exacoustos et al. Am J Obstet Gynecol, 2004
5
IVF : WHEN?
Barri et al 2010
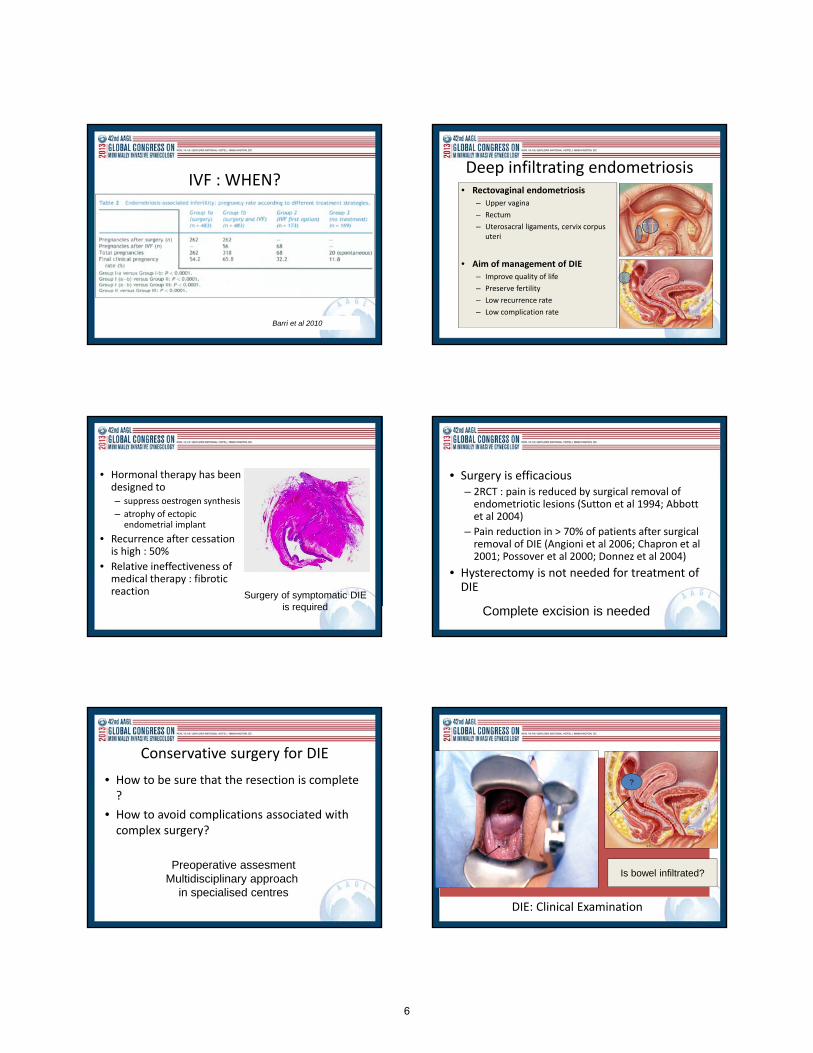
Deep infiltrating endometriosis• Rectovaginal endometriosis
– Upper vagina
– Rectum
– Uterosacral ligaments, cervix corpus uteri
• Aim of management of DIE – Improve quality of life
– Preserve fertility
– Low recurrence rate
– Low complication rate
• Hormonal therapy has been designed to – suppress oestrogen synthesis
– atrophy of ectopic endometrial implant
• Recurrence after cessation is high : 50%
• Relative ineffectiveness of medical therapy : fibrotic reaction Surgery of symptomatic DIE
is required
• Surgery is efficacious – 2RCT : pain is reduced by surgical removal of endometriotic lesions (Sutton et al 1994; Abbott et al 2004)
– Pain reduction in > 70% of patients after surgical removal of DIE (Angioni et al 2006; Chapron et al 2001; Possover et al 2000; Donnez et al 2004)
• Hysterectomy is not needed for treatment of DIE
Complete excision is needed
Conservative surgery for DIE
• How to be sure that the resection is complete ?
• How to avoid complications associated with complex surgery?
Preoperative assesmentMultidisciplinary approach
in specialised centresDIE: Clinical Examination
?
?
Is bowel infiltrated?
6

Rectal endoscopic MRI
Sonography
- Distinction between - Cartography
muscularis propria
submucosa-mucosa
Bazot et al Hum Reprod 2007Similar accuracy for diagnosis of rectal involvement when compared to MRI
Deep infiltrating endometriosis
a
Deep infiltrating endometriosis
a
Surgical Techniques
Redwine (1991) : Laparoscopic resection
Bailey (1994) : Laparotomy
Donnez (1994) : Laparoscopy without bowel resection
Possover(2000) : Vaginal dissection followed by laparoscopy and minilaparotomy
Chapron (2003) : Laparotomy if positive EER
Koninckx: Laparoscopy – discoid resection
Keckstein, Wattiez, Canis, Darai, Anaf : Laparoscopy and minilaparotomy
Possover(2005) : LANN technique
Landi (2006) : Laparoscopic nerve‐sparing complete excision of DIE
Nezhat (2010) : Robotic‐assisted laparoscopy
‐ Preoperative assessment
‐ Type of surgical treatment ?
‐ Excision of the nodular lesion‐ Without bowel resection : shaving technique
‐ Uterosacral ligaments infiltration
‐ Vaginal infiltration
‐ With bowel resection:
‐ discoid or segmental bowel resection
‐ laparoscopy ; laparotomy ; laparoscopically assisted technique
• « Check list » at the end of the surgery
– Treatment is complete
– Haemostasis is achieved
– Absence of rectal perforation
(Methylene blue rectal injection)
– Ureteral peristaltism
is satisfactory
7

‐ Preoperative assessment
‐ Type of surgical treatment ?
‐ Excision of the nodular lesion‐ Without bowel resection : shaving technique
‐ Uterosacral ligaments infiltration
‐ Vaginal infiltration
‐ With bowel resection:
‐ discoid or segmental bowel resection
‐ laparoscopy ; laparotomy ; laparoscopically assisted technique
• Baryum enema: irregularities of anterior rectal – sigmoid wall
BOWEL ENDOMETRIOSIS
Section of the distal part of the rectum (Endo GIA)Minilaparotomy for exteriorisation of the bowel
BOWEL ENDOMETRIOSIS
BOWEL ENDOMETRIOSIS Digestive complications of colorectal surgery
Authors Patients Rectovaginal fistula
Linkage of anastomosis
Secondary ileo-colost
Nezhat et al. (1992) 15 0 0 0
Jerby et al. (1999) 26 1 0 1
Possover et al. (2000) 34 0 2 0
Daraï et al. (2005) 40 4 0 4
Campagnacci et al. (2005) 7 0 0 0
Ribeiro et al. (2006) 125 2 0 NA
Panel et al. (2006) 21 2 0 2
Lyons et al. (2006) 7 0 0 0
Brouwer and Woods (2007) 213 2 1 NA
Wills et al. (2009) 167 2 3 2
Minelli et al. (2009) 357 14 4 12
TOTAL 1003 27 (2,7 %) 10 (1 %) 21(2,1%)
8
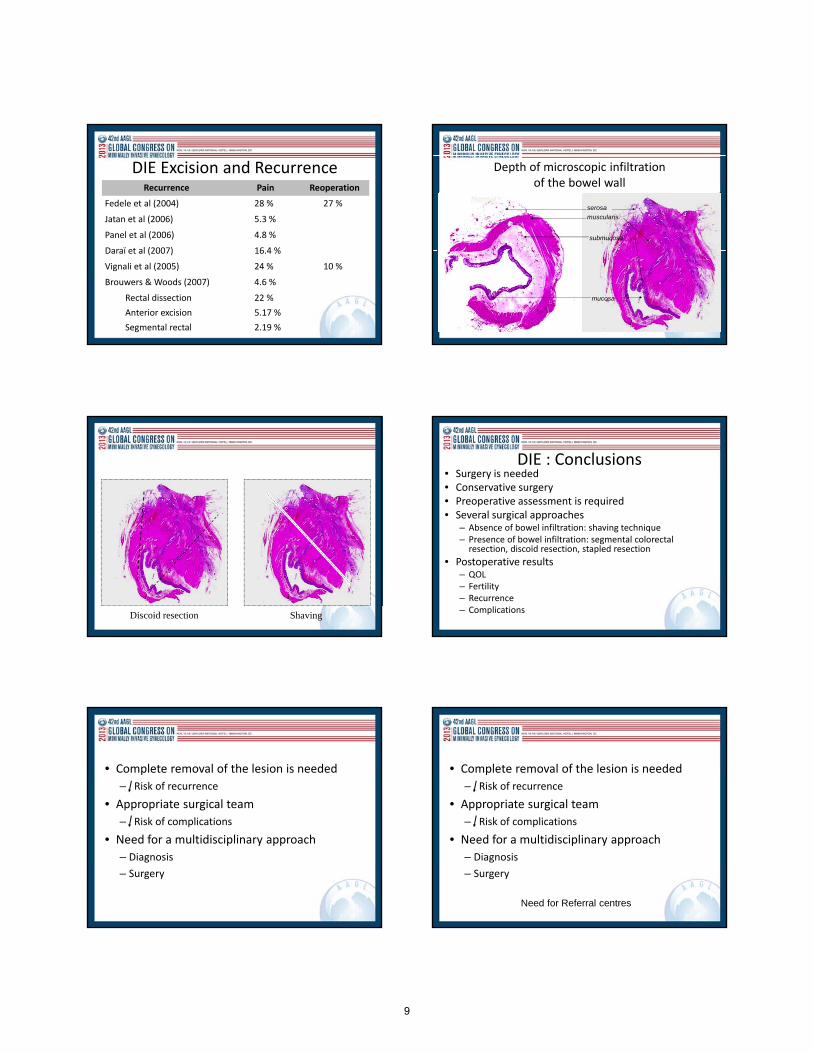
DIE Excision and RecurrenceRecurrence Pain Reoperation
Fedele et al (2004) 28 % 27 %
Jatan et al (2006) 5.3 %
Panel et al (2006) 4.8 %
Daraï et al (2007) 16.4 %
Vignali et al (2005) 24 % 10 %
Brouwers & Woods (2007) 4.6 %
Rectal dissection 22 %
Anterior excision 5.17 %
Segmental rectal 2.19 %
Depth of microscopic infiltrationof the bowel wall
Normal DIEserosa
muscularis
submucosa
mucosa
Discoid resection Shaving
DIE : Conclusions • Surgery is needed• Conservative surgery • Preoperative assessment is required• Several surgical approaches
– Absence of bowel infiltration: shaving technique– Presence of bowel infiltration: segmental colorectal resection, discoïd resection, stapled resection
• Postoperative results– QOL– Fertility– Recurrence– Complications
• Complete removal of the lesion is needed
– Risk of recurrence
• Appropriate surgical team
– Risk of complications
• Need for a multidisciplinary approach
– Diagnosis
– Surgery
• Complete removal of the lesion is needed
– Risk of recurrence
• Appropriate surgical team
– Risk of complications
• Need for a multidisciplinary approach
– Diagnosis
– Surgery
Need for Referral centres
9
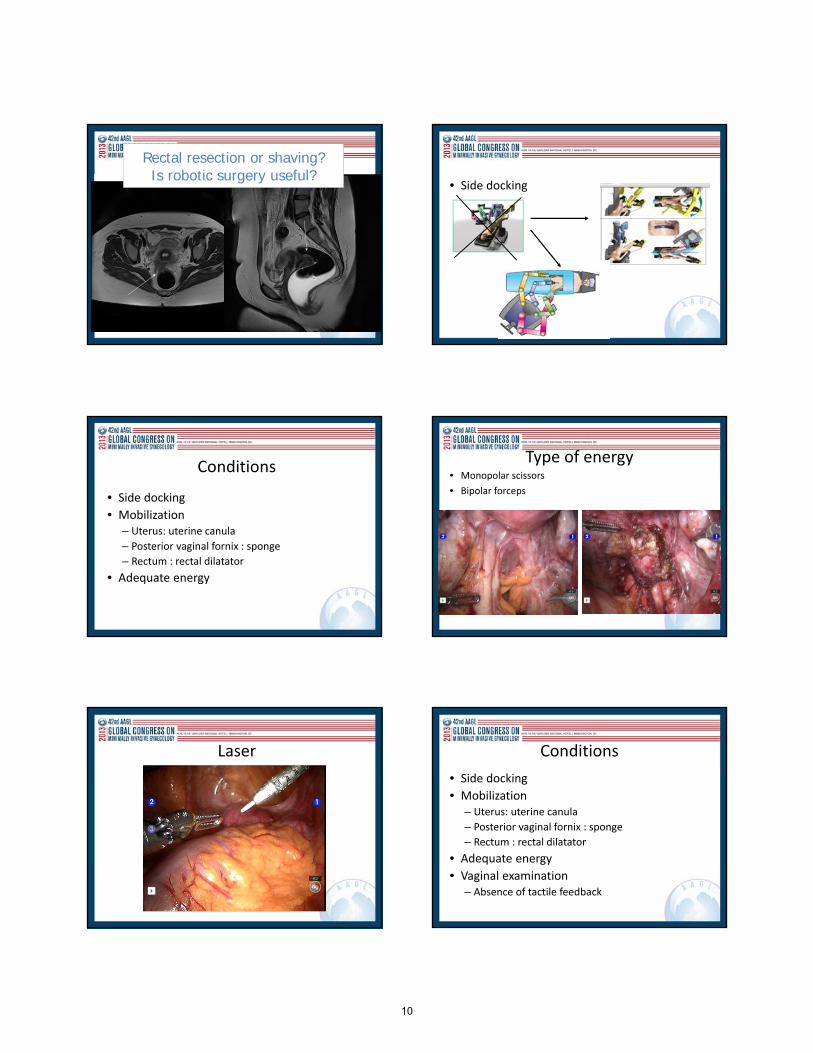
Rectal resection or shaving?Is robotic surgery useful?
• Side docking
Conditions
• Side docking
• Mobilization– Uterus: uterine canula
– Posterior vaginal fornix : sponge
– Rectum : rectal dilatator
• Adequate energy
Type of energy• Monopolar scissors
• Bipolar forceps
Laser Conditions
• Side docking
• Mobilization– Uterus: uterine canula
– Posterior vaginal fornix : sponge
– Rectum : rectal dilatator
• Adequate energy
• Vaginal examination– Absence of tactile feedback
10
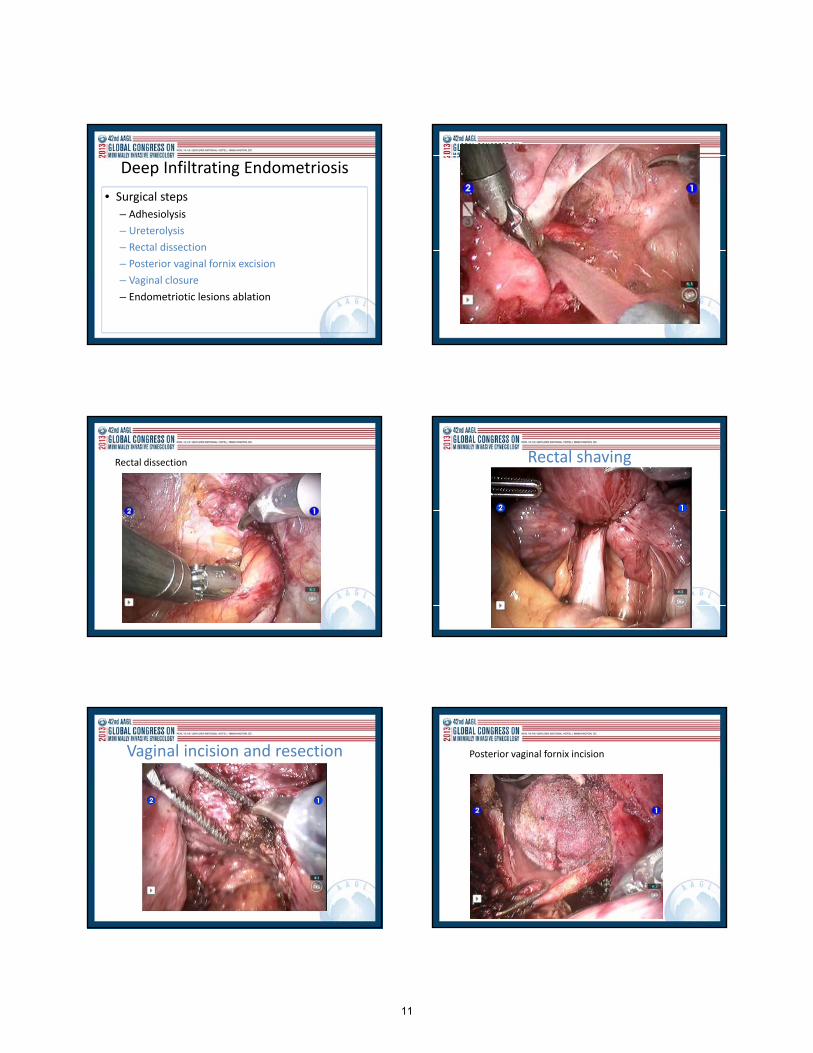
Deep Infiltrating Endometriosis
• Surgical steps
– Adhesiolysis
– Ureterolysis
– Rectal dissection
– Posterior vaginal fornix excision
– Vaginal closure
– Endometriotic lesions ablation
Rectal dissection Rectal shaving
Vaginal incision and resection Posterior vaginal fornix incision
11
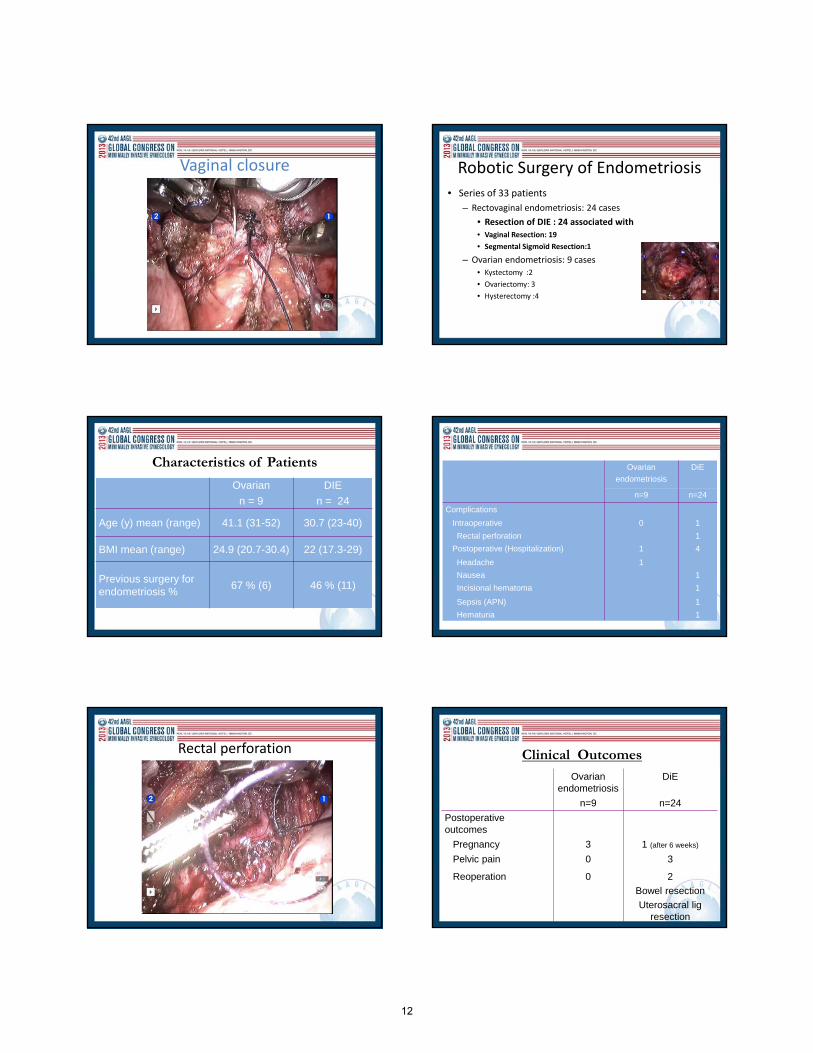
Vaginal closure Robotic Surgery of Endometriosis
• Series of 33 patients
– Rectovaginal endometriosis: 24 cases
• Resection of DIE : 24 associated with
• Vaginal Resection: 19
• Segmental Sigmoïd Resection:1
– Ovarian endometriosis: 9 cases• Kystectomy :2
• Ovariectomy: 3
• Hysterectomy :4
Characteristics of Patients
Ovarian DIE
n = 9 n = 24
Age (y) mean (range) 41.1 (31-52) 30.7 (23-40)
BMI mean (range) 24.9 (20.7-30.4) 22 (17.3-29)
Previous surgery for endometriosis %
67 % (6) 46 % (11)
Ovarian
endometriosis
DiE
n=9 n=24
Complications
Intraoperative 0 1
Rectal perforation 1
Postoperative (Hospitalization) 1 4
Headache 1
Nausea 1
Incisional hematoma 1
Sepsis (APN) 1
Hematuria 1
Rectal perforation Clinical Outcomes
Ovarian endometriosis
DiE
n=9 n=24
Postoperative outcomes
Pregnancy 3 1 (after 6 weeks)
Pelvic pain 0 3
Reoperation 0 2
Bowel resection
Uterosacral lig resection
12

Ercoli et al, 2012 Ercoli et al, 2012
JSLS 2013
JSLS 2013
13
Conclusions• Endometriosis surgery is complex
• RAL is safe and feasible
• Robotic platform : offered in patients withcomplex pelvic dissection
• Advantages for patients
– To offer complete removal of endometrioticlesions
– To decrease the recurrence rate and reoperation?
– To avoid bowel resection?
• Nisolle M, Casanas‐Roux F, Anaf V, Mine JM, Donnez J: Morphometric study of the stromal vascularizationin peitoneal endometriosis. Fertil Steril, (1993), 59: 681‐4.
• Brosens I, Puttermans P, Benagiano G: Endometriosis: a life cycle approach? Am J Obstet Gynecol, (2013), 209: 307‐16.
• Hemmings R, Biljan MM, Dean N, Tan SL: An ectopic pregnancy masked by follicular initiation of gonadotropin‐releasing hormone agonist for pituitary desensitization prior to in vitro fertilization., J AssistReprod Genet, (1998), 15: 161‐3.
• Saleh A, Tulandi T: Reoperation after laparoscopic treatment of ovarian endometriomas by excision and by fenestration, Fertil Steril (1999), 72: 322‐4.
• Canis M, Pouly JL, Tamburro S, Mage G, Wattiez A, Bruhat MA: Ovarian response during IVF‐embryotransfer cycles after laparoscopic ovarian cystectomy for endometriotic cysts of > 3 cm in diameter. Hum reprod (2001), 16: 2583‐6.
• Beretta P, Franchi M, Ghezzi F, Busacca M, Zuppi E, Bolis P: Randomized clinical trial of two laparoscopictreatments of endometriomas: cystectomy versus drainage and coagulation. Fertil Steril (1998), 70: 1176‐80.
• Alborzi S, Momtahan M, Parsanezhad ME, Dehbashi S, Zolghadri J, Alborzi S: A prospective, randomizedstudy comparing laparoscopic ovarian cystectomy versus fenestration and coagulation in patients withendometriomas. Fertil Steril (2004), 82: 1633‐7.
• Hart R, Hickey M, Maouris P, Buckett W, Garry R: Excisional surgery versus ablative surgery for ovarianendometriomata: a Cochrane Review. Hum Reprod (2005), 20: 3000‐7.
• Exacoustos C, Zupi E, Amadio A, Szabolcs B, De Vivo B, Marconi D, Elisabetta Romanini M, Arduini D: Laparoscopic removal of endometriomas: sonographic evaluation of residual functioning ovarian tissue. Am J Obstet Gynecol (2004), 191: 68‐72.
• Barri PN, Coroleu B, Tur R, Barri‐Soldevila PN, Rodriguez I: Endometriosis‐associated infertility: surgery and IVF, a comprehensive therapeutic approach. Reprod Biomed Online (2010), 21: 179‐85.
• Sutton CJ, Ewen SP, Whitelaw N, Haines P: Prospective, randomized, double‐blind, controlled trial of laser laparoscopy in the treatment of pelvic pain associated with minimal, mild, and moderate endometriosis. Fertil Steril (1994), 62: 696‐700.
• Abbott J, Hawe J, Hunter D, Holmes M, Finn P, Garry R: Laparoscopic excision of endometriosis: a randomized, placebo‐controlled trial. Fertil Steril (2004), 82: 878‐84.
• Angioni S, Peiretti M, ZironeM, Palomba M, Mais V, Gomel V, Melis GB: Laparoscopic excision of posteriorvaginal formix in the treatment of patients with deep endometriosis without rectum involvement: surgicaltreatment and long‐term follow‐up. Hum Reprod (2006), 21: 1629‐34.
• Possover M, Diebolder H, Plaul K, Schneider A: Laparoscopically assisted vaginal resection of rectovaginalendometriosis. Obstet Gynecol (2000), 96: 304‐7.
• Bazot M, Bornier C, Dubernard G, Roseau G, Cortez A, Daraï E: Accuracy of magnetic resonance imagingand rectal endoscopic sonography for the prediction of location of deep pelvic endometriosis. Hum Reprod(2007): 1457‐63.
• Bailey HR, Ott MT, Hartendorp P: Aggressive surgical management for advanced colorectal endometriosis. Dis Colon Rectum (1994), 37: 747‐53.
• Wattiez A, Puga M, Albornoz J, Faller E: Surgical strategy in endometriosis. Best Pract Res Clin ObstetGynaecol (2013), 27: 381‐92.
• Possover M, Quakernack J, Chiantera V: The LANN technique to reduce postoperative functional morbidityin laparoscopic radical pelvic surgery. J Am Coll Surg (2005), 201: 913‐7.
• Landi S, Ceccaroni M, Perutelli An allodi C, Barbieri F, Fiaccavento A, Ruffo G, McVeigh E, Zanolla L, MinelliL: Laparoscopic nerve‐sparing complete excision of deep endometriosis: is it feasible? Hum Reprod (2006), 21: 774‐81.
• Nezhat C, Lewis M, Kotikela S, Veeraswamy A, Saadat L, Hajhosseini B, Nezhat C: Robotic versus standard laparoscopy for treatment of endometriosis. Fertil Steril (2010), 94: 2758‐60.
• Nezhat C, Nezhat F, Pennington E: Laparoscopic treatment of infiltrative rectosigmoid colon and rectovaginal septum endometriosis by the technique of videolaparoscopy and the CO2 laser. Br J ObstetGynaecol (1992), 99: 664‐7.
• Redwine DB, Wright JT: Laparoscopic treatment of complete obliteration of the cul‐de‐sac associated withendometriosis: long‐term follow‐up of en bloc resection. Fertil Steril (2001), 76: 358‐65.
• Jerby BL, Kessler H, Falcone T, Milsom JW: Laparoscopic management of colorectal endometriosis. SurgEndosc (1999), 13: 1125‐8.
• Duepree HJ, Senagore AJ, Delaney CP, Marcello PW, Brady KM, Falcone T: Laparoscopic resection of deeppelvic endometriosis with rectosigmoid involvement. J Am Coll Surg (2002), 195: 754‐8.
• Daraï E, Thomassin I, Barranger E, Detchev R, Cortez A, Houry S, Bazot M: Feasibility and clinical outcomeof laparoscopic colorectal resection for endometriosis. Am J Obstet Gynecol (2005), 192: 394‐400.
• Campagnacci R, Perretta S, Guerrieri M, Paganini AM, De Sanctis A, Ciavattini A, Lezoche E: Laparoscopiccolorectal resection for endometriosis. Surg Endosc (2005), 19: 662‐4.
• Ribeiro PA, Rodriguez FC, Kehdi IP, Rossini L, Abdalla HS, Donadio N, Aoki T: Laparoscopic resection of intestinal endometriosis: a 5‐year experience. J Minim Invasive Gynecol (2006), 13: 442‐6.
• Panel P, Chis C, Gaudin S, Letohic A, Raynal P, Mikhayelyan M, Fraleu B, Sangana G, Almeras C, Dufour C, Boidart F: Laparoscopic surgery of deep endometriosis. About 118 cases. Gynecol Obstet Fertil (2006), 34: 583‐92.
• Jatan AK, SolomonMJ, Young J, Cooper M, Pathma‐Nathan N: Laparoscopic management of rectal endometriosis. Dis Colon Rectum (2006), 49: 169‐74.
• Lyons SD, Chew SS, Thomson AJ, Lenart M, Camaris C, Vancaillie TG, Abbott JA: Clinical and quality‐of‐life outcomes after fertility‐sparing laparoscopic surgery with bowel resection for severe endometriosis. J Minim Invasive Gynecol (2006), 13: 436‐41.
• Brouwer R, Woods RJ: Rectal endometriosis: results of radical excision and review of published work. ANZ J surg (2007), 77: 562‐71.
• Wills HJ, Reid GD, Cooper MJ, Tsaltas J, Morgan M, Woods RJ: Bowel resection for severe endometriosis: an Australian series of 177 cases. Aust NZJ Obstet Gynaecol (2009), 49: 415‐8.
• Minelli L, Fanfani F, Fagotti A, Ruffo G, Ceccaroni M, Mereu L, Landi S, Pomini P, Scambia G: Laparoscopiccolorectal resection for bowel endometriosis: feasibility, complications, and clinical outcome. Arch Surg(2009), 144: 234‐9.
• Fedele L, Bianchi S, Zanconato G, Bettoni G, Gotsch F: Long‐term folow‐up after conservative surgery for rectovaginal endometriosis. Am J Obstet Gynecol (2004), 4: 1020‐4.
• Daraï E, Bazot M, Rouzier R, Houry S, Dubernard G: Outcome of laparoscopic colorectal resection for endometriosis. Curr Opin Obstet Gynecol (2007), 19: 308‐13.
• Vignali M, bianchi S, Candiani M, Spadaccini G, Oggioni G, Busacca M: Surgical treatment of deependometriosis and risk recurrence. J Minim Invasive Gynecol (2005), 12: 508‐13.
• Ercoli A, D’asta M, Fagotti A, Fanfani F, Romano F, Baldazzi G, Salerno MG, Scambia G: Robotic treatmentof colorectal endometriosis: technique, feasibility and short‐term results. Hum Reprod (2012), 27: 722‐6.
• Neme RM, Schraibman V, Okazaki S, Maccapani G, Chen WJ, Domit CD, Kaufmann OG, Advicula AP: Deepinfiltrating colorectal endometriosis treated with robotic‐assisted rectosigmoidectomy. JSLS (2013)
• Bedaiwy M, Abdel Rahman MY, Chapman M, Frasure H, Mahajan S, von Gruenigen V, Hurd W, Zanotti C: Robotic‐assisted hysterectomy for the management of severe endometriosis: a retropsective review of short‐term surgical outcomes. JSLS 2013.
14

Tamer Seckin, MD [email protected]
Excision of Endometriosis:Laparoscopic & Robotic Approaches
Tamer Seckin, MD, FACOG, ACGENorth Shore LIJ Lenox Hill Hospital
Surgery Instructor, Division of Advanced Laparoscopy
Department of Obstetrics & Gynecology
Co‐Director, Minimally Invasive Gynecologic Surgery for Women Fellowship ProgramFounder & Medical Director, Endometriosis Foundation of America
Tamer Seckin, MD [email protected]
I have no financial relationships to disclose.
Tamer Seckin, MD [email protected]
• 1) Recognize subtle and occult endometriosis in normal and distorted anatomy
• 2) select proper strategy in the management of early and severe endometriosis, including new techniques to improve the quality of excision surgery;
• 3) assess appropriate utilization of new technology; and
• 4) recognize potential complications and their prevention.
Learning Objectives:
4
Tamer Seckin, MD [email protected]
Excision vs Fulguration/Ablation
4
Animations and Surgery Videos Of Excision Procedure
5
Tamer Seckin, MD [email protected]
Total Pelvic Excision Peritonectomy+ Bowel Resection3/15 positive for borderline Serous Carcinoma
6
Tamer Seckin, MD [email protected]
Understanding Endometriosis• Neonatal uterine bleeding as antecedent of pelvic endometriosis.
Brosens I, Brosens J, Benagiano G.
Source
Leuven Institute for Fertility and Embryology, Oud-Heverleestraat 83, 30001 Leuven, Belgium.
Abstract
We elaborate on a new theory to explain pelvic endometriosis, including endometriosis in premenarcheal girls, based on the finding that the neonatal endometrium can display secretory activity immediately after birth and, in some cases, changes analogous to those seen at menstruation in adults. The neonatal uterus is therefore capable of shedding its endometrium. Indeed, occult vaginal bleeding occurs in a majority of neonates, although overt bleeding is estimated to occur in only 5% of neonates. This may be due to functional plugging of the endocervical canal in the neonate, which in turn would promote retrograde flux of endometrial cells contained in menstrual debris. Ectopic endometrial implantation in a newborn with hydrometrocolpos has been documented. These data, coupled with the observation of a significantly increased risk of endometriosis in adolescents with cervical outflow obstruction and patent Fallopian tubes, indicate that endometriosis, especially in children and young adolescents, may originate from retrograde uterine bleeding soon after birth.
KEYWORDS:
cervical obstruction, fetal uterus, neonatal uterine bleeding, pelvic endometriosis, retrograde menstruation
15

7
Tamer Seckin, MD [email protected]
Inflammation and Stem Cell Theory
Endometriosis originates from the cellular debris of retrograde menstruation which contains progenitor stem cells of endo-myometrial junction
C.E. Gargett et al. Molecular and Cellular Endocrinology 288 (2008) 22–29
10
Text
micro menses
micro pre menses
10
Tamer Seckin, MD 872 5th Av NY, NY 10021 [email protected]
Seckin, MD
11
Seckin, MD
12
v
Seckin, MD
12
16
Seckin, MD
13
Seckin, MD
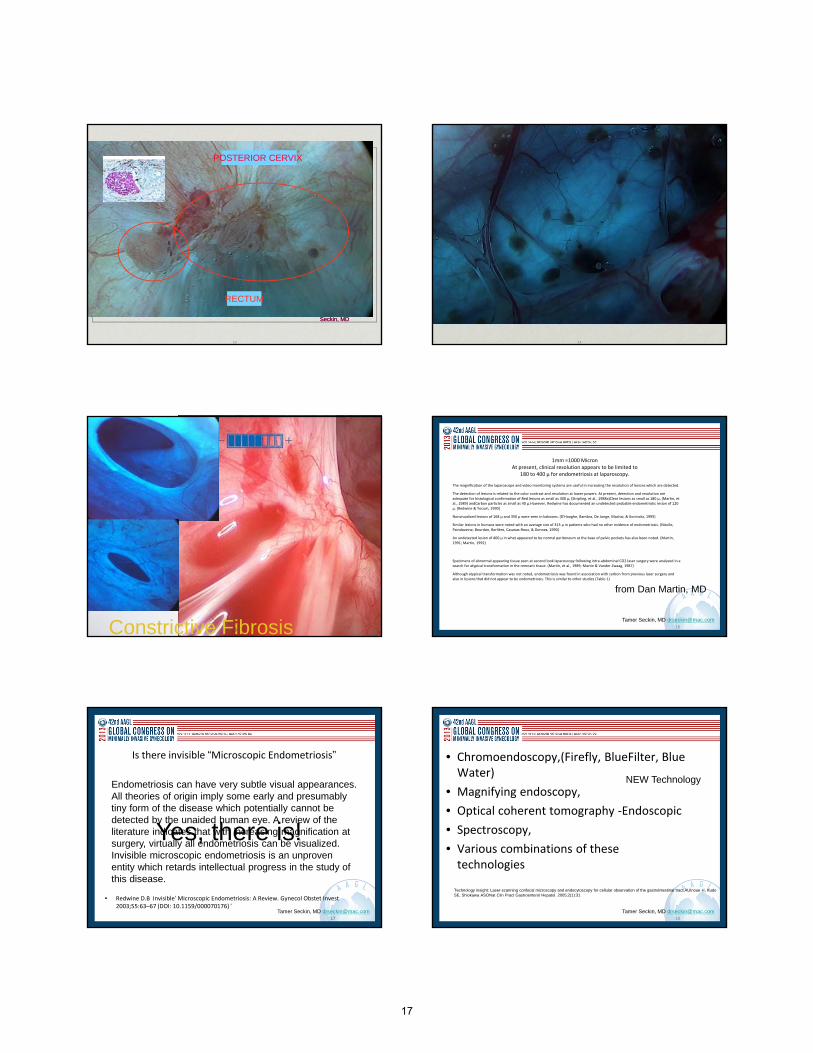
RECTUM
POSTERIOR CERVIX
Seckin, MD
14
15Constrictive Fibrosis1516
Tamer Seckin, MD [email protected]
1mm =1000 MicronAt present, clinical resolution appears to be limited to
180 to 400 µ for endometriosis at laparoscopy.
The magnification of the laparoscope and video monitoring systems are useful in increasing the resolution of lesions which are detected.
The detection of lesions is related to the color contrast and resolution at lower powers. At present, detection and resolution are adequate for histological confirmation of:Red lesions as small as 400 µ, (Stripling, et al., 1988a)Clear lesions as small as 180 µ, (Martin, et al., 1989) andCarbon particles as small as 40 µ.However, Redwine has documented an undetected probable endometriotic lesion of 120 µ. (Redwine & Yocum, 1990)
Nonvisualized lesions of 168 µ and 350 µ were seen in baboons. (D'Hooghe, Bambra, De Jonge, Machai, & Koninckx, 1995)
Similar lesions in humans were noted with an average size of 313 µ in patients who had no other evidence of endometriosis. (Nisolle, Paindaveine, Bourdon, Berlière, Casanas‐Roux, & Donnez, 1990)
An undetected lesion of 400 µ in what appeared to be normal peritoneum at the base of pelvic pockets has also been noted. (Martin, 1991; Martin, 1992)
Specimens of abnormal appearing tissue seen at second look laparoscopy following intra‐abdominal CO2 laser surgery were analyzed in a search for atypical transformation in the remnant tissue. (Martin, et al., 1989; Martin & Vander Zwaag, 1987)
Although atypical transformation was not noted, endometriosis was found in association with carbon from previous laser surgery and also in lesions that did not appear to be endometriosis. This is similar to other studies (Table 1)
from Dan Martin, MD
17
Tamer Seckin, MD [email protected]
Is there invisible “Microscopic Endometriosis”
• Redwine D.B Invisible’ Microscopic Endometriosis: A Review. Gynecol Obstet Invest 2003;55:63–67 (DOI: 10.1159/000070176) ‘
17
Endometriosis can have very subtle visual appearances. All theories of origin imply some early and presumably tiny form of the disease which potentially cannot be detected by the unaided human eye. A review of the literature indicates that with increasing magnification at surgery, virtually all endometriosis can be visualized. Invisible microscopic endometriosis is an unproven entity which retards intellectual progress in the study of this disease.
Yes, there is!
18
Tamer Seckin, MD [email protected]
• Chromoendoscopy,(Firefly, BlueFilter, Blue Water)
• Magnifying endoscopy,
• Optical coherent tomography ‐Endoscopic
• Spectroscopy,
• Various combinations of these technologies
Technology insight: Laser-scanning confocal microscopy and endocytoscopy for cellular observation of the gastrointestinal tract.AUInoue H, Kudo SE, Shiokawa ASONat Clin Pract Gastroenterol Hepatol. 2005;2(1):31
NEW Technology
17

19
Tamer Seckin, MD [email protected]
Subtle and Occult endometriosis in non‐distorted and distorted anatomy
Subtle/Atypical
Classic‐Typical Lesions
Occult (due to their size and location)
20
Tamer Seckin, MD [email protected]
Classic‐Typical Lesions• puckered
– black,
– bluish
– red
The diagnosis of endometriosis has often been made by observation of puckered black or bluish "typical" lesions. (Buttram & Reiter, 1985; Dmowski, 1984; Haney, 1987; Hulka, 1985; Kirshon, Poindexter, & Fast, 1989)
21
Tamer Seckin, MD [email protected]
Classic‐Typical Lesions
• Obstet Gynecol Clin North Am. 2003 Mar;30(1):83-93, viii.
Typical and subtle atypical presentations of endometriosis.Donnez J, Squifflet J, Casanas-Roux F, Pirard C, Jadoul P, Van Langendonckt A.
Source
Department of Gynecology, St. Luc's Hospital, Université Catholique de Louvain, Avenue Hippocrate, 1200 Brussels, Belgium. [email protected]
Abstract
The diagnosis of peritoneal endometriosis at the time of laparoscopy is often made by the observation of typically puckered black or bluish lesions. There are also numerous subtle appearances of peritoneal endometriosis. The lesions are frequently non-pigmented. Red flame-like lesions, glandular excrescences, and subovarian adhesions must be considered as the most active lesions. Sometimes, however, subtle endometriotic lesions can be the only lesions seen at laparoscopy.
21 22
Tamer Seckin, MD [email protected]
Subtle Endometriosis• The lesions are frequently non‐pigmented.
– Red flame‐like lesions,
– glandular excrescences, and
– subovarian adhesions
22
Subtle forms are more common. (Davis & Brooks, 1988; Martin, et al., 1989; Redwine, 1987a)Subtle forms may be more active than dark lesions.(Vernon, Beard, Graves, & Wilson, 1986; Wild & Wilson, 1987)
23
Tamer Seckin, MD [email protected]
Subtle and Occult endometriosis in distorted anatomy
• Classic‐Typical Lesions
• Atypical Lesions Lesions
• Fibrotic non infiltrative Nodules
• Infiltrative Nodules
Hidden(Occult) retroperitoneal disease is active. (Koninckx, Ruttinen, Seppala, & Cornillie, 1992)
24
Tamer Seckin, MD [email protected]
Occult Disease‐Surface
18
25
Tamer Seckin, MD [email protected]
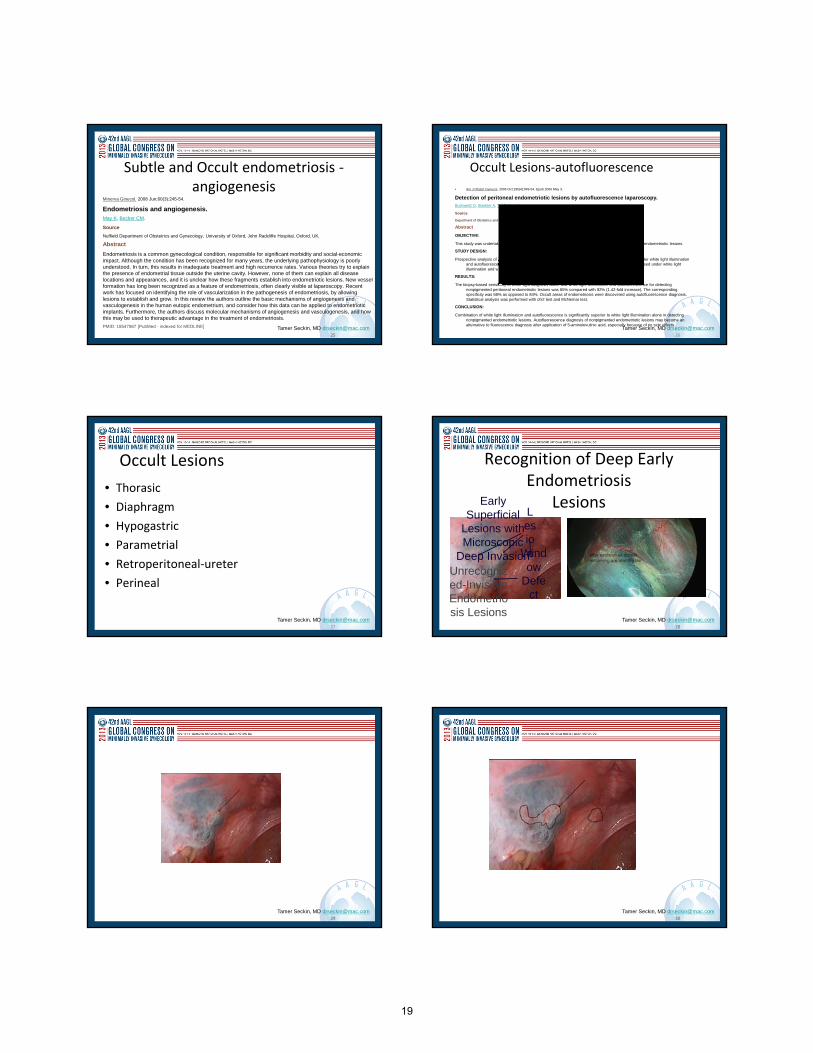
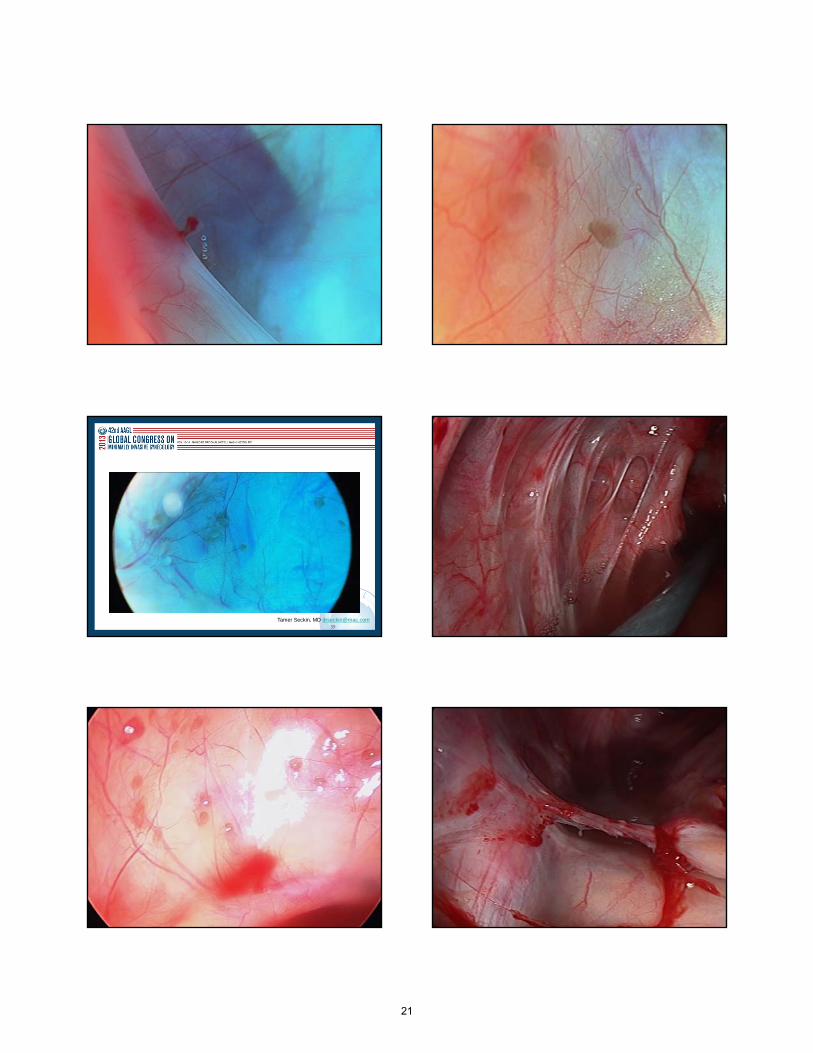
Subtle and Occult endometriosis ‐angiogenesis
Minerva Ginecol. 2008 Jun;60(3):245-54.
Endometriosis and angiogenesis.May K, Becker CM.
Source
Nuffield Department of Obstetrics and Gynecology, University of Oxford, John Radcliffe Hospital, Oxford, UK.
Abstract
Endometriosis is a common gynecological condition, responsible for significant morbidity and social-economic impact. Although the condition has been recognized for many years, the underlying pathophysiology is poorly understood. In turn, this results in inadequate treatment and high recurrence rates. Various theories try to explain the presence of endometrial tissue outside the uterine cavity. However, none of them can explain all disease locations and appearances, and it is unclear how these fragments establish into endometriotic lesions. New vessel formation has long been recognized as a feature of endometriosis, often clearly visible at laparoscopy. Recent work has focused on identifying the role of vascularization in the pathogenesis of endometriosis, by allowing lesions to establish and grow. In this review the authors outline the basic mechanisms of angiogenesis and vasculogenesis in the human eutopic endometrium, and consider how this data can be applied to endometriotic implants. Furthermore, the authors discuss molecular mechanisms of angiogenesis and vasculogenesis, and how this may be used to therapeutic advantage in the treatment of endometriosis.
PMID: 18547987 [PubMed - indexed for MEDLINE]
25 26
Tamer Seckin, MD [email protected]
Occult Lesions‐autofluorescence
• Am J Obstet Gynecol. 2006 Oct;195(4):949-54. Epub 2006 May 3.
Detection of peritoneal endometriotic lesions by autofluorescence laparoscopy.Buchweitz O, Staebler A, Tio J, Kiesel L.
Source
Department of Obstetrics and Gynaecology, University of Münster, Germany.
Abstract
OBJECTIVE:
This study was undertaken to evaluate the feasibility of autofluorescence laparoscopy in the diagnosis of endometriotic lesions.
STUDY DESIGN:
Prospective analysis of 83 consecutive patients undergoing laparoscopy for suspected endometriosis under white light illumination and autofluorescence diagnosis. The study measured total number of endometriotic lesions diagnosed under white light illumination and with autofluorescence diagnosis.
RESULTS:
The biopsy-based sensitivity of white light diagnosis alone and white light illumination and autofluorescence for detecting nonpigmented peritoneal endometriotic lesions was 65% compared with 92% (1.42-fold increase). The corresponding specificity was 68% as opposed to 84%. Occult areas of endometriosis were discovered using autofluorescence diagnosis. Statistical analysis was performed with chi2 test and McNemar test.
CONCLUSION:
Combination of white light illumination and autofluorescence is significantly superior to white light illumination alone in detecting nonpigmented endometriotic lesions. Autofluorescence diagnosis of nonpigmented endometriotic lesions may become an alternative to fluorescence diagnosis after application of 5-aminolevulinic acid, especially because of no side effects.
27
Tamer Seckin, MD [email protected]
Occult Lesions
• Thorasic
• Diaphragm
• Hypogastric
• Parametrial
• Retroperitoneal‐ureter
• Perineal
28
Tamer Seckin, MD [email protected]
Recognition of Deep Early Endometriosis
Lesions
28
Early Superficial
Lesions with Microscopic
Deep InvasionWindow
Defect
Lesion
Unrecognized-Invisible Endometriosis Lesions
29
Tamer Seckin, MD [email protected] 30
Tamer Seckin, MD [email protected]
19
31
Tamer Seckin, MD [email protected] 32
Tamer Seckin, MD [email protected]
33
Tamer Seckin, MD [email protected] 34
Tamer Seckin, MD [email protected]
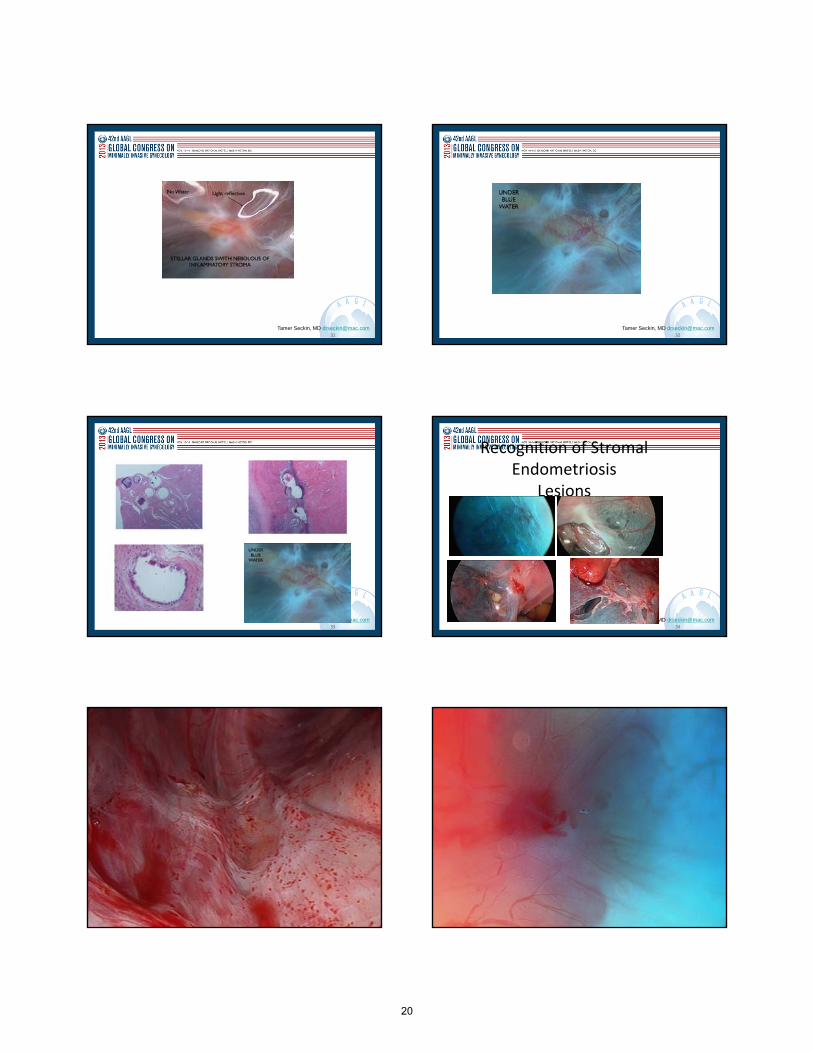
Recognition of Stromal Endometriosis
Lesions
34
35
Tamer Seckin, MD [email protected] 36
Tamer Seckin, MD [email protected]
20
37
Tamer Seckin, MD [email protected] 38
Tamer Seckin, MD [email protected]
39
Tamer Seckin, MD [email protected] 40
Tamer Seckin, MD [email protected]
41
Tamer Seckin, MD [email protected] 42
Tamer Seckin, MD [email protected]
21
43
Tamer Seckin, MD [email protected]
Seckin, MD
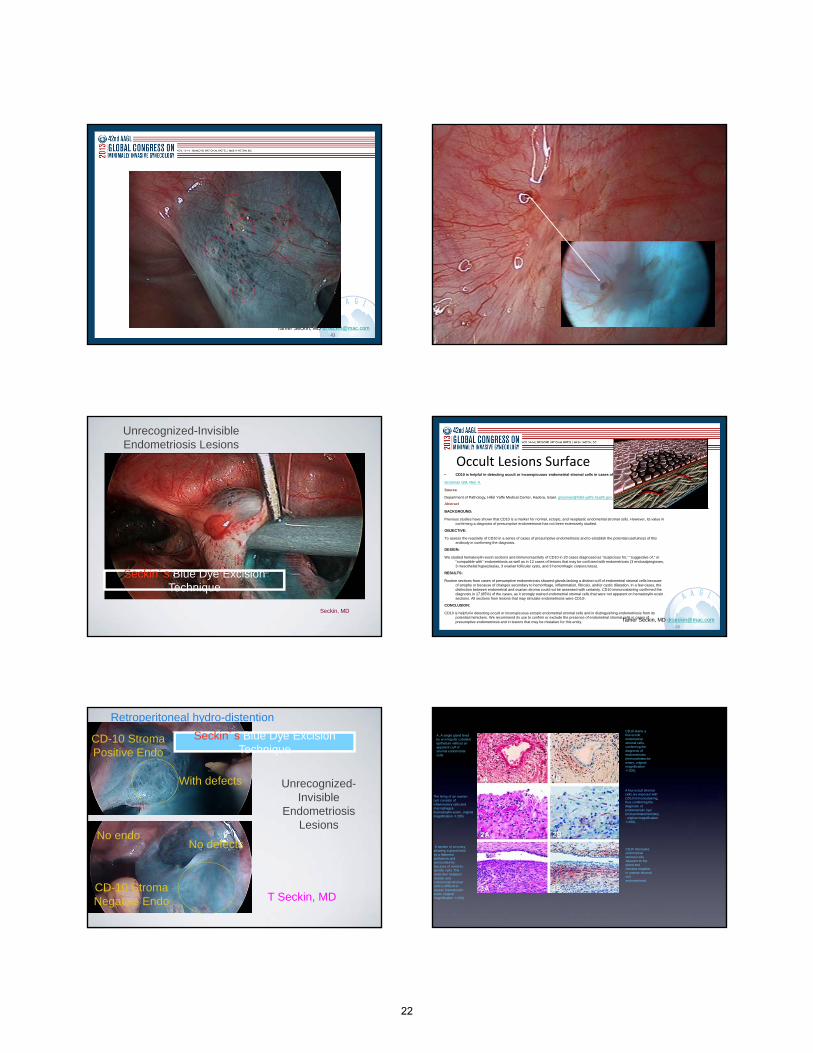
Unrecognized-Invisible Endometriosis Lesions
Seckin’s Blue Dye Excision Technique
46
Tamer Seckin, MD [email protected]
• CD10 is helpful in detecting occult or inconspicuous endometrial stromal cells in cases of presumptive endometriosis.
Groisman GM, Meir A.
Source
Department of Pathology, Hillel Yaffe Medical Center, Hadera, Israel. [email protected]
Abstract
BACKGROUND:
Previous studies have shown that CD10 is a marker for normal, ectopic, and neoplastic endometrial stromal cells. However, its value in confirming a diagnosis of presumptive endometriosis has not been extensively studied.
OBJECTIVE:
To assess the reactivity of CD10 in a series of cases of presumptive endometriosis and to establish the potential usefulness of this antibody in confirming the diagnosis.
DESIGN:
We studied hematoxylin-eosin sections and immunoreactivity of CD10 in 20 cases diagnosed as "suspicious for," "suggestive of," or "compatible with" endometriosis as well as in 12 cases of lesions that may be confused with endometriosis (3 endosalpingioses, 3 mesothelial hyperplasias, 3 ovarian follicular cysts, and 3 hemorrhagic corpora lutea).
RESULTS:
Routine sections from cases of presumptive endometriosis showed glands lacking a distinct cuff of endometrial stromal cells because of atrophy or because of changes secondary to hemorrhage, inflammation, fibrosis, and/or cystic dilatation. In a few cases, the distinction between endometrial and ovarian stroma could not be assessed with certainty. CD10 immunostaining confirmed the diagnosis in 17 (85%) of the cases, as it strongly stained endometrial stromal cells that were not apparent on hematoxylin-eosin sections. All sections from lesions that may simulate endometriosis were CD10-.
CONCLUSION:
CD10 is helpful in detecting occult or inconspicuous ectopic endometrial stromal cells and in distinguishing endometriosis from its potential mimickers. We recommend its use to confirm or exclude the presence of endometrial stromal cells in cases of presumptive endometriosis and in lesions that may be mistaken for this entity.
Occult Lesions Surface
T Seckin, MD
No endo
CD-10 Stroma Positive Endo
Retroperitoneal hydro-distention
With defects
CD-10 Stroma Negative Endo
No defects
Unrecognized-Invisible
Endometriosis Lesions
Seckin’s Blue Dye Excision Technique
A, A single gland lined by an irregular cuboidal epithelium without an apparent cuff of stromal endometrial cells.
CD10 stains a few occult endometrial stromal cells, confirming the diagnosis of endometriosis (immunohistochemistry, original magnification ×200).
The lining of an ovarian cyst consists of inflammatory cells and macrophages (hematoxylin-eosin, original magnification ×200).
A few occult stromal cells are exposed with CD10 immunostaining, thus confirming the diagnosis of endometriotic cyst (immunohistochemistry, original magnification ×200).
A section of an ovary showing a gland lined by a flattened epithelium and surrounded by fascicles of ovoid-to-spindle cells. The distinction between ovarian and endometrial stromal cells is difficult to assess (hematoxylin-eosin, original magnification ×100).
CD10 decorates endometrial stromal cells adjacent to the gland and remains negative in ovarian stromal cell endometriosis.
22

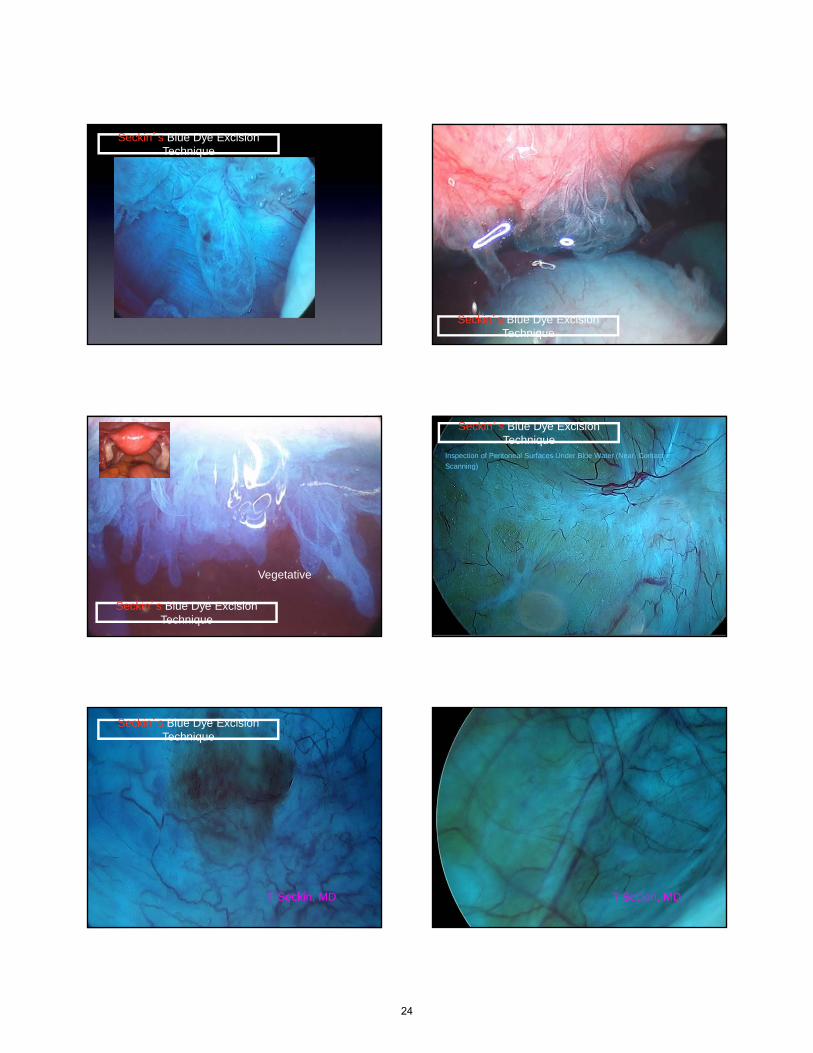
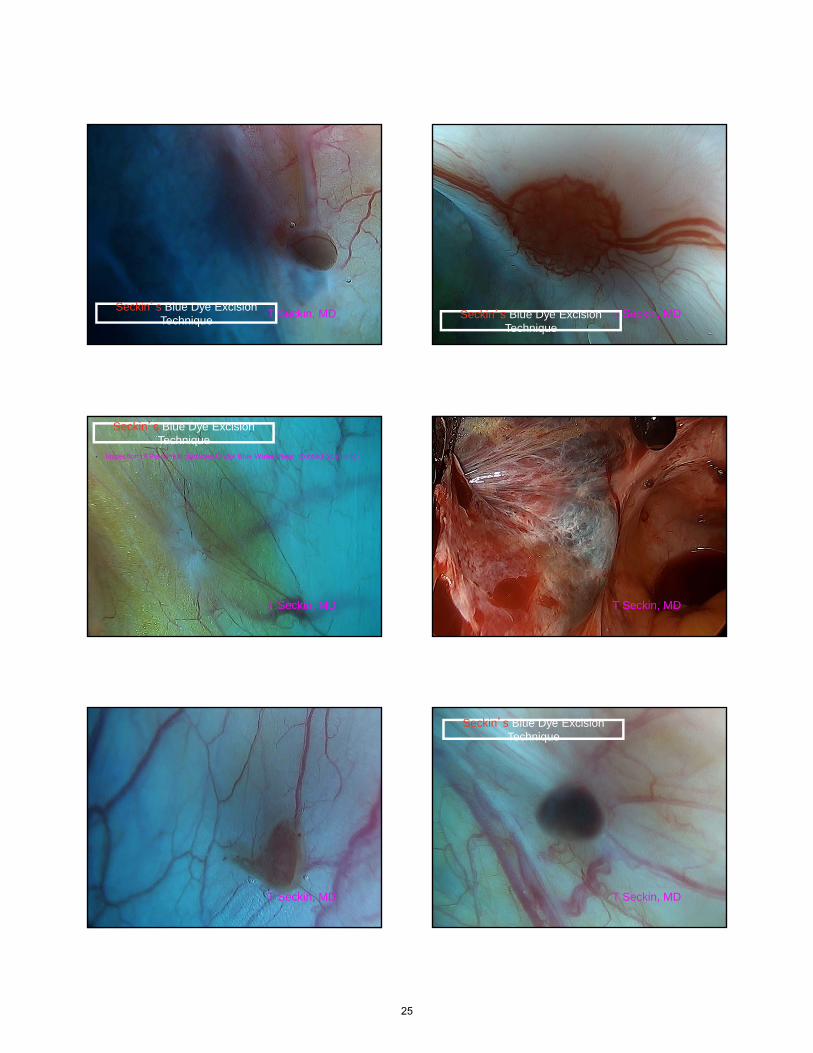
Seckin’s Blue Dye Excision Technique
Retroperitoneal distention with Blue water and creationcontrast under peritoneal membrane
Inspection for Superficial collateral pathology- Leopard Spots -Inspection for Retroperitoneal fibrosis Inspection for micro endometriosis implants
Cold excision with back up micro bipolar coagulation
Step Two
Step One
A near contact examination (Scanning) of the Peritoneal Surface Under Blue Water-Hydro floatationElimination of light reflection
Red and Yellow Elimination of direct gas pressure on the peritoneal surfaces- surface lesions(projectile, vegetative) lesions start to hydro float
Seckin’s Blue Dye Excision Technique
Seckin’s Blue Dye Excision Technique
Inspection of Peritoneal Surfaces Under Blue Water (Near Contact Scanning)
Hydro floatation
Step One
A near contact examination (Scanning) of the Peritoneal Surface Under Blue Water-Elimination of light reflection
Red and Yellow Elimination of direct gas pressure on the peritoneal surfaces- surface lesions(projectile, vegetative) lesions start to hydro float
Step One
Seckin’s Blue Dye Excision Technique
T Seckin, MD
Seckin’s Blue Dye Excision Technique
23
Seckin’s Blue Dye Excision Technique
Seckin’s Blue Dye Excision Technique
Vegetative
Seckin’s Blue Dye Excision Technique
• Inspection of Peritoneal Surfaces Under Blue Water (Near Contact
Scanning)
•
Seckin’s Blue Dye Excision Technique
T Seckin, MDT Seckin, MD
Seckin’s Blue Dye Excision Technique
T Seckin, MDT Seckin, MD
24
T Seckin, MDT Seckin, MDSeckin’s Blue Dye Excision
Technique T Seckin, MDT Seckin, MDSeckin’s Blue Dye Excision
Technique
T Seckin, MDT Seckin, MD
• Inspection of Peritoneal Surfaces Under Blue Water (Near Contact Scanning)
Seckin’s Blue Dye Excision Technique
T Seckin, MDT Seckin, MD
T Seckin, MDT Seckin, MD T Seckin, MDT Seckin, MD
Seckin’s Blue Dye Excision Technique
25

67
Tamer Seckin, MD [email protected]
Distorted Anatomy‐Deep Disease
67 68
Tamer Seckin, MD [email protected]
69
Tamer Seckin, MD [email protected] 70
Tamer Seckin, MD [email protected]
Distorted Anatomy
70
72
Tamer Seckin, MD [email protected]
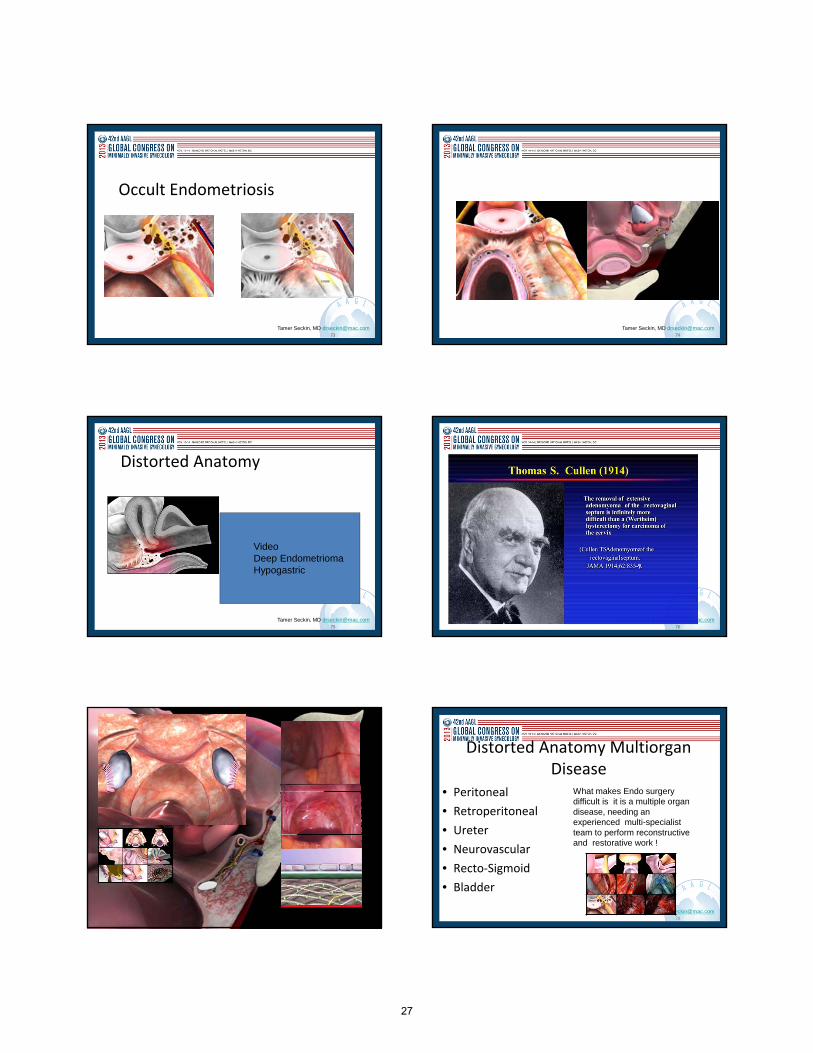
Occult Endometriosis‐Deep
Video DeepParametrial/Obtrator
26
73
Tamer Seckin, MD [email protected]
Occult Endometriosis
73 74
Tamer Seckin, MD [email protected]
75
Tamer Seckin, MD [email protected]
Distorted Anatomy
75
Video Deep EndometriomaHypogastric
76
Tamer Seckin, MD [email protected]
Tamer Seckin, MD [email protected]
gh
78
Tamer Seckin, MD [email protected]
Distorted Anatomy Multiorgan Disease
• Peritoneal
• Retroperitoneal
• Ureter
• Neurovascular
• Recto‐Sigmoid
• Bladder
What makes Endo surgery difficult is it is a multiple organ disease, needing an experienced multi-specialist team to perform reconstructive and restorative work !
27
79
Tamer Seckin, MD [email protected]
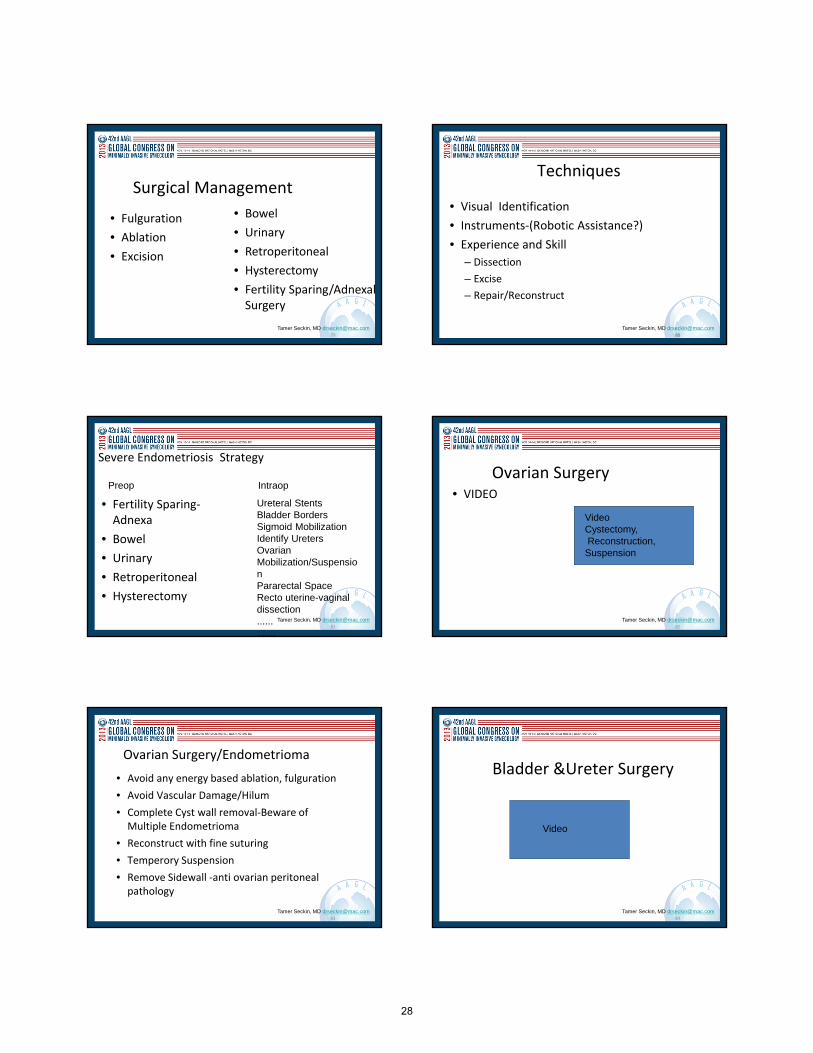
Surgical Management
• Fulguration
• Ablation
• Excision
• Bowel
• Urinary
• Retroperitoneal
• Hysterectomy
• Fertility Sparing/Adnexal Surgery
80
Tamer Seckin, MD [email protected]
Techniques
• Visual Identification
• Instruments‐(Robotic Assistance?)
• Experience and Skill
– Dissection
– Excise
– Repair/Reconstruct
80
81
Tamer Seckin, MD [email protected]
Severe Endometriosis Strategy
• Fertility Sparing‐Adnexa
• Bowel
• Urinary
• Retroperitoneal
• Hysterectomy
Ureteral StentsBladder BordersSigmoid MobilizationIdentify UretersOvarian Mobilization/Suspension Pararectal SpaceRecto uterine-vaginal dissection.............
Preop Intraop
82
Tamer Seckin, MD [email protected]
Ovarian Surgery• VIDEO
VideoCystectomy,Reconstruction, Suspension
83
Tamer Seckin, MD [email protected]
Ovarian Surgery/Endometrioma
• Avoid any energy based ablation, fulguration
• Avoid Vascular Damage/Hilum
• Complete Cyst wall removal‐Beware of Multiple Endometrioma
• Reconstruct with fine suturing
• Temperory Suspension
• Remove Sidewall ‐anti ovarian peritoneal pathology
84
Tamer Seckin, MD [email protected]
Bladder &Ureter Surgery
Video
28
85
Tamer Seckin, MD [email protected]
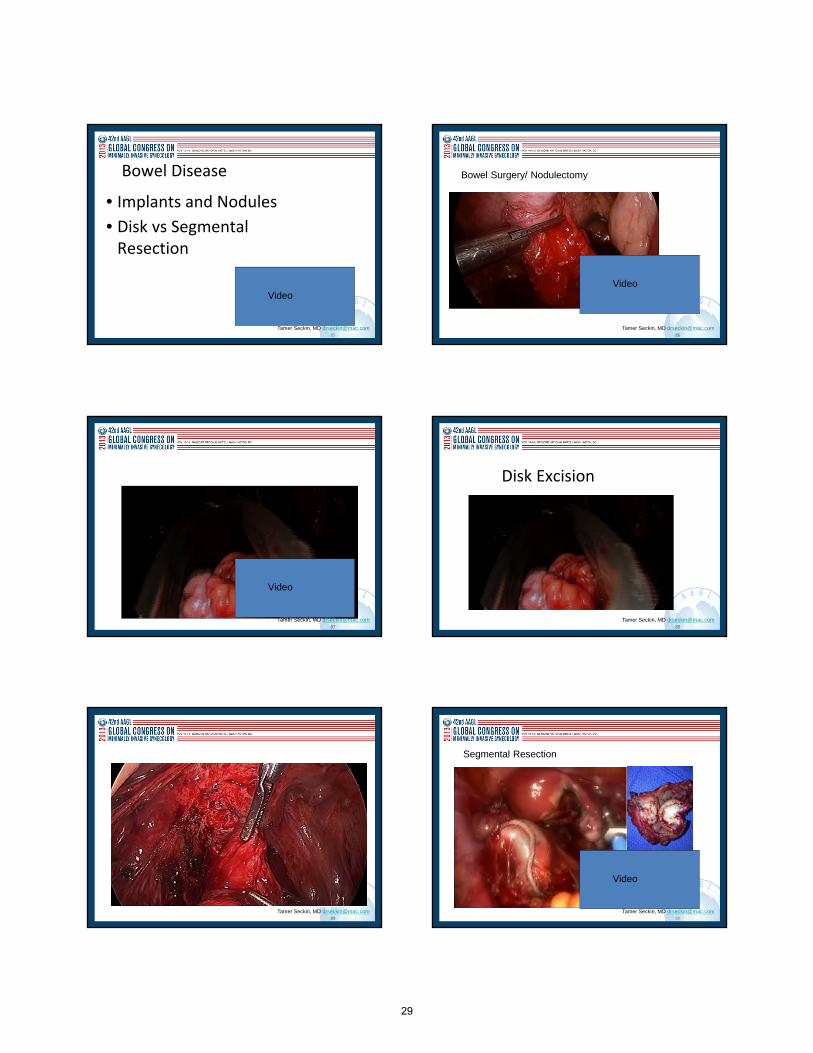
Bowel Disease
• Implants and Nodules
• Disk vs Segmental Resection
Video
86
Tamer Seckin, MD [email protected]
Bowel Surgery/ Nodulectomy
Video
87
Tamer Seckin, MD [email protected]
Video
88
Tamer Seckin, MD [email protected]
Disk Excision
88
89
Tamer Seckin, MD [email protected] 90
Tamer Seckin, MD [email protected]
Segmental Resection
Video
29
91
Tamer Seckin, MD [email protected]
Nodulectomy ending with Segmental Resection
92
Tamer Seckin, MD [email protected]
93
Tamer Seckin, MD [email protected]
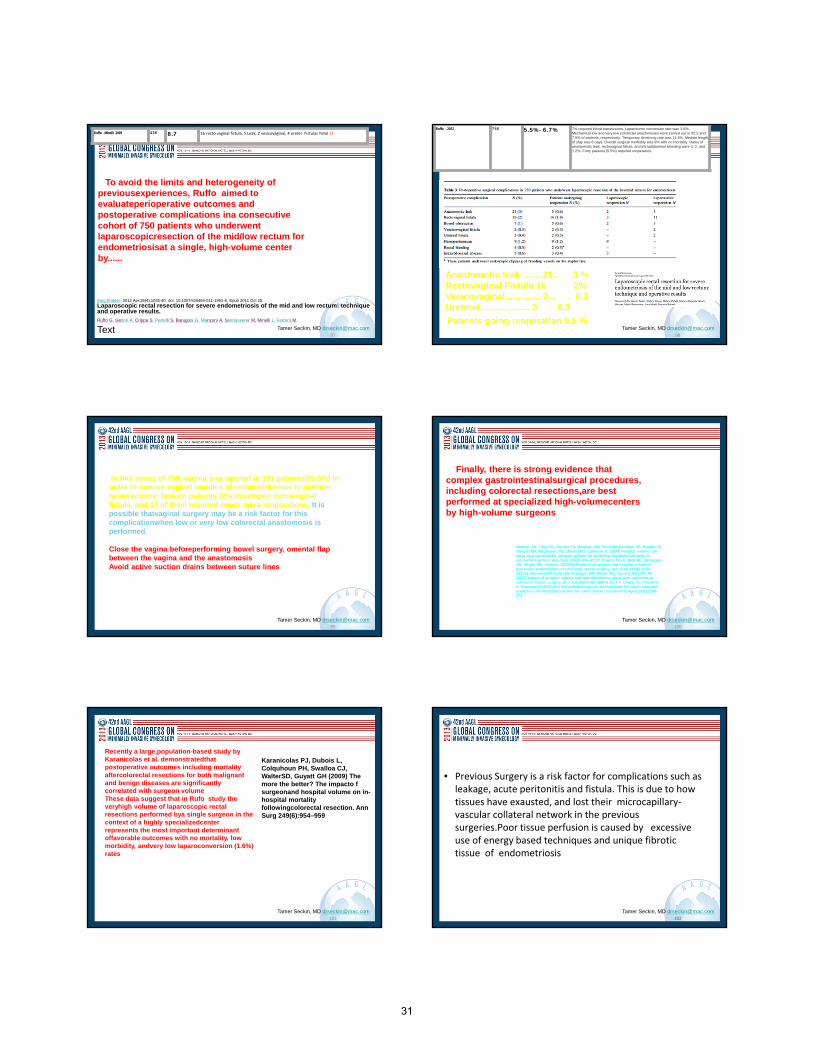
Bowel Nodules/Implants
• Multifocality
• Multicentricty
• Both
94
Tamer Seckin, MD [email protected]
• .Kavallaris A, Kohler C, Kuhne-Heid R, Schneider A (2003) Histopathological extent of rectal invasion by rectovaginal endometriosis. Hum Reprod 18: 1323-
Department of Obstetrics and Gynecology, Friedrich Schiller University, Bachstrasse 18, 07740 Jena, Germany.
Vaginal Invasion
95
Tamer Seckin, MD [email protected]
Rectovaginal 91
Rectal 224
Pararectal 287
Sigmoid 107
Ileo-cecal 19
Appendix 35
Ileum 1
Location of Bowel Endometriosis vs Number of Excisions
93 %
7 %
rectosigmoid colon is the most frequently affected site
13 %
Rectovaginal
91
Rectal 224
Sigmoid 107
42296
Tamer Seckin, MD [email protected]
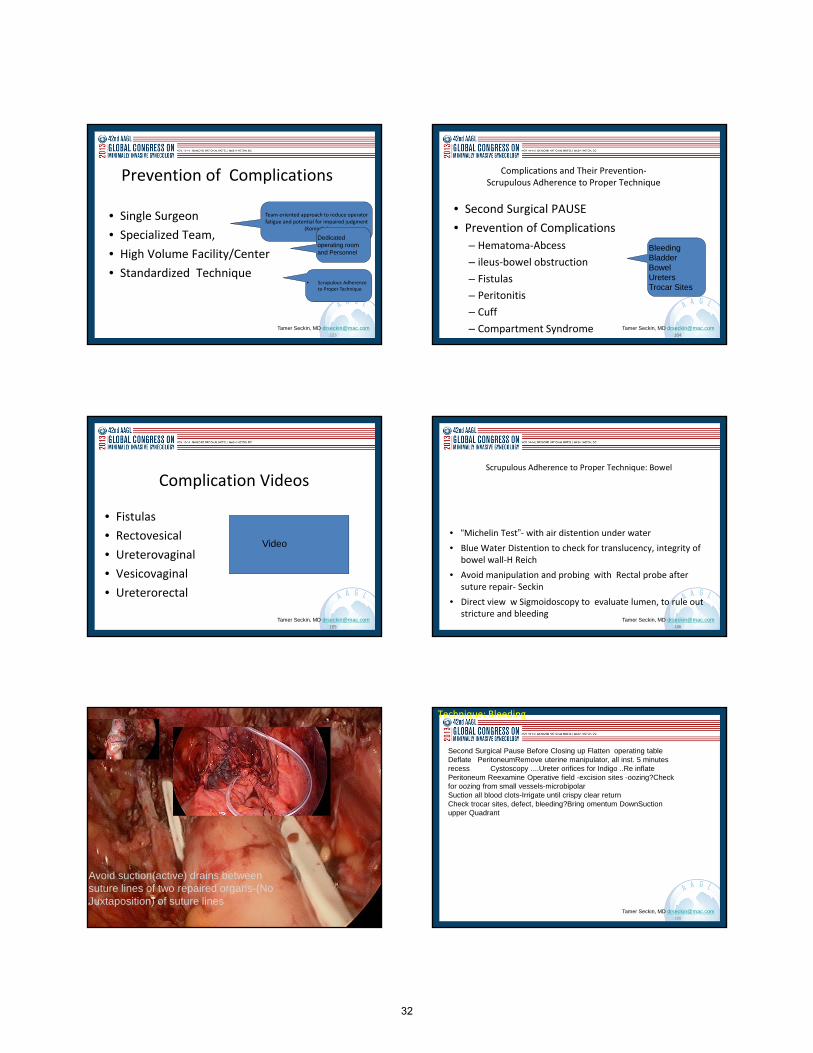
Ruffo G, Sartori A, Crippa S, et al. Laparoscopic rectal resectionfor severe endometriosis of the mid and low rectum: techniqueand operative results. Surg Endosc. 2012;26:1035–1040
The prospective database of bowel resections maintained atthe Department of Surgery of the Ospedale Sacro Cuore-Don Calabria was queried to identify patients who underwentlaparoscopic rectal resection for endometriosis of themid/low rectum between January 2002 and September2010
30
97
Tamer Seckin, MD [email protected]
To avoid the limits and heterogeneity of previousexperiences, Ruffo aimed to evaluateperioperative outcomes and postoperative complications ina consecutive cohort of 750 patients who underwent laparoscopicresection of the mid/low rectum for endometriosisat a single, high-volume center by......
Ruffo -Minelli 2009 436 8.7 16 recto vaginal fistula, 5 Leak, 2 vesicovaginal, 4 ureter Fistulas Total 24
Surg Endosc. 2012 Apr;26(4):1035-40. doi: 10.1007/s00464-011-1991-8. Epub 2011 Oct 25.
Laparoscopic rectal resection for severe endometriosis of the mid and low rectum: technique and operative results.Ruffo G, Sartori A, Crippa S, Partelli S, Barugola G, Manzoni A, Steinasserer M, Minelli L, Falconi M.
Text98
Tamer Seckin, MD [email protected]
Anastomotic leak .......21.. 3 %Rectovaginal Fistula 16 2%Vesicovaginal.............. 2... . 0.3Ureteral.................... 3 0.3
Patients going reoperation 5.5 %
Ruffo - 2012 750 5.5%- 6.7% 7% required blood transfusions. Laparotomic conversion rate was 1.6%. Mechanical low and very low colorectal anastomoses were carried out in 92.5 and 7.5% of patients, respectively. Temporary ileostomy rate was 14.5%. Median length of stay was 8 days. Overall surgical morbidity was 9% with no mortality. Rates of anastomotic leak, rectovaginal fistula, and intraabdominal bleeding were 3, 2, and 1.2%. Forty patients (5.5%) required reoperation.
99
Tamer Seckin, MD [email protected]
In this series of 750, vagina was opened in 191 patients(25.5%) in order to remove vaginal nodules of endometriosisor to perform hysterectomy. Sixteen patients (2%)developed rectovaginal fistula, and 14 of them required oneor more reoperations. It is possible thatvaginal surgery may be a risk factor for this complicationwhen low or very low colorectal anastomosis is performed.
Close the vagina beforeperforming bowel surgery, omental flap between the vagina and the anastomosisAvoid active suction drains between suture lines
100
Tamer Seckin, MD [email protected]
Finally, there is strong evidence that complex gastrointestinalsurgical procedures, including colorectal resections,are best performed at specialized high-volumecenters by high-volume surgeons
Harmon JW, Tang DG, Gordon TA, Bowman HM, Choti MA,Kaufman HS, Bender JS, Duncan MD, Magnuson TH, LillemoeKD, Cameron JL (1999) Hospital volume can serve as a surrogatefor surgeon volume for achieving excellent outcomes in colorectalresection. Ann Surg 230(3):404–41117. Rogers SO Jr, Wolf RE, Zaslavsky AM, Wright WE, Ayanian JZ(2006) Relation of surgeon and hospital volume to processes andoutcomes of colorectal cancer surgery. Ann Surg 244(6):1003–101118. Borowsi DW, Kelly SB, Bradburn DM, Wilson RG, Gunn A,Ratcliffe AA (2007) Impact of surgeon volume and specializationon short-term outcomes in colorectal cancer surgery. Br J Surg94(7):880–88919. Ko CY, Chang JT, Chaudhry S, Kominski G (2002) Are highvolumesurgeons and hospitals the most important predictors ofin-hospital outcome for colon cancer resection? Surgery132(2):268–273
101
Tamer Seckin, MD [email protected]
Recently a large,population-based study by Karanicolas et al. demonstratedthat postoperative outcomes including mortality aftercolorectal resections for both malignant and benign diseases are significantly correlated with surgeon volumeThese data suggest that in Rufo study the veryhigh volume of laparoscopic rectal resections performed bya single surgeon in the context of a highly specializedcenter represents the most important determinant offavorable outcomes with no mortality, low morbidity, andvery low laparoconversion (1.6%) rates
Karanicolas PJ, Dubois L, Colquhoun PH, Swalloa CJ, WalterSD, Guyatt GH (2009) The more the better? The impacto f surgeonand hospital volume on in-hospital mortality followingcolorectal resection. Ann Surg 249(6):954–959
102
Tamer Seckin, MD [email protected]
• Previous Surgery is a risk factor for complications such as leakage, acute peritonitis and fistula. This is due to how tissues have exausted, and lost their microcapillary‐vascular collateral network in the previous surgeries.Poor tissue perfusion is caused by excessive use of energy based techniques and unique fibrotic tissue of endometriosis
102
31
103
Tamer Seckin, MD [email protected]
Prevention of Complications
• Single Surgeon
• Specialized Team,
• High Volume Facility/Center
• Standardized Technique
Team‐oriented approach to reduce operator fatigue and potential for impaired judgment
(Koninckx)
Dedicated operating room and Personnel
• Scrupulous Adherence to Proper Technique
104
Tamer Seckin, MD [email protected]
Complications and Their Prevention‐Scrupulous Adherence to Proper Technique
• Second Surgical PAUSE
• Prevention of Complications
– Hematoma‐Abcess
– ileus‐bowel obstruction
– Fistulas
– Peritonitis
– Cuff
– Compartment Syndrome104
BleedingBladderBowelUretersTrocar Sites
105
Tamer Seckin, MD [email protected]
Complication Videos
• Fistulas
• Rectovesical
• Ureterovaginal
• Vesicovaginal
• Ureterorectal
105
Video
106
Tamer Seckin, MD [email protected]
Scrupulous Adherence to Proper Technique: Bowel
• “Michelin Test”‐ with air distention under water
• Blue Water Distention to check for translucency, integrity of bowel wall‐H Reich
• Avoid manipulation and probing with Rectal probe after suture repair‐ Seckin
• Direct view w Sigmoidoscopy to evaluate lumen, to rule out stricture and bleeding
106
Repair in layersIschemia free techniqueTension free anostomosis
Avoid suction(active) drains between suture lines of two repaired organs-(No Juxtaposition) of suture lines
108
Tamer Seckin, MD [email protected]
Second Surgical Pause Before Closing up Flatten operating table Deflate PeritoneumRemove uterine manipulator, all inst. 5 minutes recess Cystoscopy ....Ureter orifices for Indigo ..Re inflate Peritoneum Reexamine Operative field -excision sites -oozing?Checkfor oozing from small vessels-microbipolarSuction all blood clots-Irrigate until crispy clear returnCheck trocar sites, defect, bleeding?Bring omentum DownSuctionupper Quadrant
Technique: Bleeding
32

109
Tamer Seckin, MD [email protected]
Issues with Robotic Enabling/ Assistance
• Aggressive Marketing/
– Advertisement
• Misrepresentation
– Lack of Evidence
• Cost ‐Time
• Complications
109
Tamer Seckin, MD [email protected]
Injuries May, in fact, be Under-reported
• Researchers at Johns Hopkins found that 174 injuries and 71 deaths werereported to the FDA, but demonstrated other examples of “ botchedoperations ” that went unreported, concluding that “ robotic surgerycomplications are vastly under-reported.”16
• The true extent of complications and injuries which have occurred in actualpractice may be unknown
• Reports of suppressed complaints, complications and performance errors17
• Little to no oversight/incentives exist for reporting18
4
Tamer Seckin, MD [email protected]
• JAMA: of 260,000 hysterectomy patients, median hospital cost for robot-assisted surgery was $8,868 as compared to $6,679 for a laparoscopic hysterectomy19
• “It is feasible for robotic hysterectomy to be less expensive than abdominal hysterectomy, but unlikely for robotic hysterectomy to be less expensive than traditional laparoscopy.” [Shah et al.]20
• Present review of literature indicates robot-assisted surgery is consistently more expensive than video-laparoscopy, and in many cases open surgery.21
Mean complication rates generally do not vary significantly among minimally invasive methods of hysterectomy, but patient costs are significantly influenced by method.22
Data Consistently Demonstrates Increased Cost as Compared to Conventional Laparoscopic Approach in Gyn & GynOnc, yet Equal or Lesser Reimbursement Continues
Tamer Seckin, MD [email protected]
Cost Data, continued
• Hospital charges for robotic surgery vs. laparoscopic in endometrial cancerrevealed higher costs but no difference in surgeon reimbursement.23
• Cost is not limited only to the surgery itself; the initial cost, cost ofinstruments and cost of maintenance is exorbitant and limiting.24, 25
• “Given the high costs and small scientific evidence, the introduction ofrobotic surgery has been irresponsibly quick. Better scientific research ofrobotic surgery is needed before this technology can be broadly applied inclinical practice.” la Chapelle et al.26
Tamer Seckin, MD [email protected]
Known Disadvantages
• Bulkiness of equipment, inability to use certain tools, lack of tactile feedback, inability tomove surgical table, additional set up/breakdown time of robotic equipment27
• Significantly longer surgical and anesthesia time, as well as larger trocars arenecessary28
• Learning Curve – though not as steep as conventional laparoscopy, technology can neverreplace true skill
• No proven benefit over adhesion formation vs laparotomy or laparoscopy29
• Difficult to separate poor surgical skill from actual device-related injuries; increasedlikelihood of electrical arcing30
• Aesthetics/Port size:• 2 port: 5mm to ¼ inch; # of ports 2• Standard lap: 2 at 5mm, 1 at 10mm to ¼ inch, 1 at 12mm to 3/4 inch ; # of ports 3-4• Robotic: 3 at 8 mm, 2 at 12 mm; # of ports 5 (also increases risk of herniation)
Tamer Seckin, MD [email protected]
Too Much, Too Soon?
• Use of robotic surgery has grown substantially since 2007 by 400%, with littledata to support such growth; surgeons may feel pressured to adopt the techniquewithout adequate training or in the face of concerns that another procedure maybe a better option31
• Aggressive marketing lack counterbalance in adequate training; lack of long-termdata continues to be a significant issue32, 33
• Data implies that materials provided by hospitals regarding the robotoverestimate benefits, largely ignore risks and are strongly influenced by themanufacturer34
33

Tamer Seckin, MD [email protected]
Evidence of Advantages Lacking?
• Advantages do exist, particularly where the inexperienced laparoscopic surgeon isconcerned during complex procedures; however, further randomized trials are needed35
• May be argued that endometriosis can be equally well visualized with traditional 2Dsystems via improved HD optics and magnification; new technology may be on par withrobotic symptoms while reducing learning curve and preserving tactile feedback 36, 37, 38
• Complex, multidisciplinary surgery for advanced endometriosis is feasible by laparoscopyin expert hands39
• Paucity of quality data addressing the superiority of robotic surgery over laparoscopicsurgery; early evidence shows robotic surgery did not actually benefit women with benigngynacological disease in effectiveness or safety40
• Literature on robotics for endometriosis is very sparse; no guidelines about benefits;41
may be limited to value in advanced cases that may otherwise be converted42
• Use of robotic surgery may not be result of evidence-based benefits but driven by themanufacturers, patients and enthusiastic surgeons.”43
Tamer Seckin, MD [email protected]
Reimbursement/Healthcare Legislation
• Currently no differences in reimbursement to the surgeon between the two operative approaches44
•Speculation implies that the Affordable Care Act will limit the amount paid for procedures and doctors' ability to recommend them45
• Experts note that although hospitals have been willing to absorb higher costs associated with robotic surgery, healthcare overhaul provisions may change such practices46, 47
Tamer Seckin, MD [email protected]
“…Robotic-assisted laparoscopic surgery should not replace conventional laparoscopic or vaginal procedures for women who couldotherwise undergo conventional laparoscopic or vaginal surgery for benign gynecologic diseases…Additional research comparingconventional laparoscopic and robotic-assisted laparoscopic surgery is needed to help characterize the advantages anddisadvantages of robotic-assisted surgery and concurrently determine patient groups who would benefit from robotic-assistedlaparoscopy over other methods.” AAGL Position Statement, 201348
“…Many women today are hearing about the claimed advantages of robotic surgery for hysterectomy, thanks to widespread marketingand advertising. Robotic surgery is not the only or the best minimally invasive approach for hysterectomy. Nor is it the most cost-efficient. It is important to separate the marketing hype from the reality when considering the best surgical approach forhysterectomies. The outcome of any surgery is directly associated with the surgeon’s skill. …While there may be some advantages tothe use of robotics in complex hysterectomies, especially for cancer operations that require extensive surgery and removal of lymphnodes, studies have shown that adding this expensive technology for routine surgical care does not improve patient outcomes.Consequently, there is no good data proving that robotic hysterectomy is even as good as-let alone better-than existing, and far lesscostly, minimally invasive alternatives.”- ACOG Position Statement, 201349
“…As with any new technology, care should be taken that protocols are in place to ensure appropriate patient selection and the fullexplanation of risks and benefits for all surgical options. Education and guidelines for the perioperative and post-operative teams,particularly those personnel or units new to robotic surgery, are important steps for assuring that these surgeries are performed safely,and that there is prompt recognition and treatment of any patient complications.” Commonwealth of Massachusetts, Board ofRegistration in Medicine Position Statement, 201350
A Cautionary Tale
Tamer Seckin, MD [email protected]
Though the literature clearly lacks in the area of using robotics forendometriosis; additional studies will reveal benefits; e.g. LAROSEStudy
Should we be using the robot in endometriosis? “With appropriaterationale and indications for its use, proper training with subsequentcredentialing and privileging, and infrastructure to allow for safe andefficient use of the technology with outcomes tracking.”-Arnie ArnoldP. Advincula, MD51
A Look Ahead…
Tamer Seckin, MD [email protected]
THANK YOU!
120
Tamer Seckin, MD [email protected]
1. Cullen, T. S. (1896). Adeno‐myoma uteri diffusum benignum. Johns Hopkins Hosp Rep, 6, 133‐157.
2. Cullen, T. S. (1919). The distribution of adenomyomata containing uterine mucosa. Am J Obstet Gynecol, 80, 130‐138.
3. Fallon, J., Brosnan, J. T., Manning, J. J., Moran, W. G., Meyers, J., & Fletcher, M. E. (1950). Endometriosis: a report of 400 cases. Rhode Island Med J, 33, 15‐23.
4. Lockyer, C. (1913). Adenomyoma in the recto‐uterine and recto‐vaginal septa. Proc Royal Soc Med (Obstet), 6, 112‐120.
5. Martin, D. C., Hubert, G. D., Vander Zwaag, R., & El‐Zeky, F. A. (1989). Laparoscopic appearances of peritoneal endometriosis. Fertil Steril, 51, 63‐67.
6. Sampson, J. A. (1921). Perforating hemorrhagic (chocolate) cysts of the ovary. Their importance and especially their relation to pelvic adenomas of the endometrial type ("adenomyoma" of the uterus, rectovaginal septum,
sigmoid, etc.). Arch Surg, 3, 245‐323.
7. Sampson, J. A. (1922). Ovarian hematomas of endometrial type (perforating hemorrhagic cysts of the ovary) and implantation adenomas of endometrial type. Boston Med Surg J, 186, 445.
8. Sampson, J. A. (1924). Benign and malignant endometrial implants in the peritoneal cavity, and their relation to certain ovarian tumors. Surg Gynecol Obstet, 38, 287‐311.
9. Sampson, J. A. (1927a). Metastatic or embolic endometriosis, due to the menstrual dissemination of endometrial tissue into the venous circulation. Am J Pathol, 3, 93‐109.
10. Sampson, J. A. (1927b). Peritoneal endometriosis due to menstrual dissemination of endometrial tissue into the peritoneal cavity. Am J Obstet Gynecol, 14, 422‐469.
11. Sampson, J. A. (1940). The development of the implantation theory for the origin of peritoneal endometriosis. Am J Obstet Gynecol, 40, 549‐557.
12. Semm, K., & Friedrich, E. R. (1987). Operative Manual for Endoscopic Abdominal Surgery. Chicago: Yearbook Medical Publishers.
13. Martin DC (ed), Protean Appearance of Endometriosis. Adapted from "Recognition of Endometriosis" in Laparoscopic Appearance of Endometriosis, Lecture Supplement Resurge Press, Memphis, (c) 1991
14. Donnez J, Squifflet J, Casanas‐Roux F, Pirard C, Jadoul P, Van Langendonckt A. Typical and subtle atypical presentations of endometriosis. Obstet Gynecol Clin GM, Meir A., CD10 is helpful in detecting occult or
inconspicuous endometrial stromal cells in cases of presumptive endometriosis. Department of Pathology, Hillel Yaffe Medical Center, Hadera, Israel
15. Kavallaris A, Köhler C, Kühne‐Heid R, Schneider A (2003) Histopathological extent of rectal invasion by rectovaginal endometriosis. Hum Reprod. 2003;18:1323–1327. [PubMeKoninnky, Timmermans, Meuleman,
Penninckx. Complications of CO2‐laser endoscopic excision of deep endometriosis. Human Reproduction (impact factor: 4.47). 10/1996; 11(10):2263‐8
120
References
34

121
Tamer Seckin, MD [email protected]
33. Tusheva, Gargiulo, Einarsson. Application of Robotics in Adnexal Surgery. Rev Obstet Gynecol. 2013; 6(1): e28–e34
34. Mendez‐Probst, Vilos, Fuller, Fernandez, Borg, Galloway, Pautler. Stray electrical currents in laparoscopic instruments used in da Vinci® robot‐assisted surgery: an in vitro study. J Endourol. 2011 Sep;25(9):1513‐7
35. David Mittleman. “New Concerns Arise Over Robotic Surgery.” The Legal Examiner. September 11, 2013. Online: http://lansing.legalexaminer.com/defective‐dangerous‐products/new‐concerns‐arise‐over‐robotic‐surgery/. Last accessed
October 5, 2013
36. 1‐12‐CV‐237723: Zarick, et al. v. Intuitive Surgical, Inc. Case Documentation. Superior Court of California, County of Santa Clara
37. Patki, Patel. Anesthesia Concerns in da Vinci Robotic Laparoscopic Hysterectomy. J Anesth Clin Res 2012, 3:9
38. David Mittleman. “New Concerns Arise Over Robotic Surgery.” The Legal Examiner. September 11, 2013. Online: http://lansing.legalexaminer.com/defective‐dangerous‐products/new‐concerns‐arise‐over‐robotic‐surgery/. Last accessed
October 5, 2013
39. 1‐12‐CV‐237723: Zarick, et al. v. Intuitive Surgical, Inc. Case Documentation. Superior Court of California, County of Santa Clara
40. Cooper, Ibrahim, Lyu, Makary (2013). Underreporting of Robotic Surgery Complications. Journal for Healthcare Quality. doi: 10.1111/jhq.12036
41. Wright, Ananth, Lewin, Burke, Lu, Neugut, Herzog, Hershman. Robotically Assisted vs Laparoscopic Hysterectomy among Women with Benign Gynecologic Disease. JAMA. 2013;309(7):689‐698
42. Shah, Wright, Jonsdottir, Jorgensen, Einarsson, Muto. The Feasibility of Societal Cost Equivalence between Robotic Hysterectomy and Alternate Hysterectomy Methods for Endometrial Cancer.Obstet Gynecol Int. 2011;2011:570464
43. van Dam, Hauspy, Verkinderen, Trinh, van Dam, Van Looy Dirix. Are costs of robot‐assisted surgery warranted for gynecological procedures? Obstet Gynecol Int. 2011;2011:973830
44. Wright, Jonsdottir, Jorgensen, Shah, Einarsson. Costs and outcomes of abdominal, vaginal, laparoscopic and robotic hysterectomies. JSLS. 2012 Oct‐Dec;16(4):519‐24
45. Venkat, Chen, Young‐Lin, Kiet, Young, Amatori, Dasverma, Yu, Kapp, Chan. An economic analysis of robotic versus laparoscopic surgery for endometrial cancer: costs, charges and reimbursements to hospitals and professionals. Gynecol
Oncol. 2012 Apr;125(1):237‐40
46. Kelly Wright, MD. “Why Isn’t Everyone Excited about Robotic Assisted Surgery?”MedPage Today, KevinMD.com. Online: http://www.kevinmd.com/blog/2012/03/isnt‐excited‐robotic‐assisted‐surgery.html. Last accessed October 5,
2013
47. Ladaique, Lambaudie, Collinet, Houvenaeghel. Robot‐assisted laparoscopy in gynecologic surgery Journal of Visceral Surgery.Volume 148, Issue 5, Supplement, October 2011, Pages e30–e39
48. la Chapelle CF, Jansen FW, Pelger RC, Mol BW. Robotic surgery in the Netherlands: lack of high‐quality proof of efficacy. Ned Tijdschr Geneeskd. 2013;157(28):A5145
121
References
122
Tamer Seckin, MD [email protected]
49. la Chapelle CF, Jansen FW, Pelger RC, Mol BW. Robotic surgery in the Netherlands: lack of high‐quality proof of efficacy. Ned Tijdschr Geneeskd. 2013;157(28):A5145
50. Tusheva, Gargiulo, Einarsson. Application of Robotics in Adnexal Surgery. Rev Obstet Gynecol. 2013; 6(1): e28–e34.
51. Nezhat, Lewis, Kotikela, Veeraswamy, Saadat, Hajhosseini, Nezhat. Robotic versus standard laparoscopy for the treatment of endometriosis. Fertil Steril. 2010 Dec;94(7):2758‐60
52. Somigliana, Benaglia, Vigano, Candiani, Vercellini, Fedele. Surgical measures for endometriosis‐related infertility: A plea for research. Placenta. Volume 32, Supplement 3, September 2011, Pages S238–
S242.
53. Cooper, Ibrahim, Lyu, Makary (2013). Underreporting of Robotic Surgery Complications. Journal for Healthcare Quality. doi: 10.1111/jhq.12036
54. David Mittleman. “New Concerns Arise Over Robotic Surgery.” The Legal Examiner. September 11, 2013. Online: http://lansing.legalexaminer.com/defective‐dangerous‐products/new‐concerns‐arise‐
over‐robotic‐surgery/. Last accessed October 5, 2013
33. 1‐12‐CV‐237723: Zarick, et al. v. Intuitive Surgical, Inc. Case Documentation. Superior Court of California, County of Santa Clara
55. Jin, Ibrahim, Newman, Makarov, Pronovost, Makary. Robotic surgery claims on United States hospital websites. J Healthc Qual. 2011 Nov;33(6):48‐52
56. Nezhat, Modest, King. The role of the robot in treating urinary tract endometriosis. Curr Opin Obstet Gynecol. 2013 Aug;25(4):308‐11.
57. Rakesh, Meenakshi, Shweta, Gayatri, Manju, Rushindra. 3D laparoscopy: technique and initial experience in 451 cases. Gynecological Surgery.May 2013, Volume 10, Issue 2, pp 123‐128
58. Viking manufacturer data; http://www.vikingsystems.com/medical/3d‐surgery/default.html
59. Casie Leiby. “Olympus Goes 3D.” MD Buyline. April 25, 2013. Online: http://www.mdbuyline.com/olympus‐goes‐3d#sthash.PnkHTmPN.0U4T17uN.dpbs. Last accessed October 5, 2013.
60. Cannone, Ladaique, Lambaudie, Collinet, Houvenaeghel. Robot‐assisted laparoscopy in gynecologic surgery Journal of Visceral Surgery. Volume 148, Issue 5, Supplement, October 2011, Pages e30–e39
61. Liu, Lu, Wang, Shi, Song, Clarke. Robotic surgery for benign gynaecological disease. Cochrane database. System Rev. 2012;2:CD00897
62. Tusheva, Gargiulo, Einarsson. Application of Robotics in Adnexal Surgery. Rev Obstet Gynecol. 2013; 6(1): e28–e34. This is only comparing those who need to open, not skilled endoscopists
122
References
123
Tamer Seckin, MD [email protected]
63. Van Dam, Hauspy, Verkinderen, Trinh, van Dam, Van Looy, Dirix. Are costs of robot‐assisted surgery warranted for gynecological procedures? Obstet Gynecol Int. 2011;2011:973830
64. Venkat, Chen, Young‐Lin, Kiet, Young, Amatori, Dasverma, Yu, Kapp, Chan. An economic analysis of robotic versus laparoscopic surgery for endometrial cancer: costs, charges and reimbursements to
hospitals and professionals. Gynecol Oncol. 2012 Apr;125(1):237‐40
65. Joseph Hogue. “Get 25% Upside With This 'Cyborg In The Operating Room.” StreetAuthority, LLC. September 18, 2013. Online: http://beta.streetauthority.com/growth-investing/get-25-upside-cyborg-
operating-room-478037. Last accessed October 4, 2013
66. Michelle Andrews. “Questions Arise About Robotic Surgery's Cost, Effectiveness.” Kaiser Health News. April 23, 2013. Online: http://www.kaiserhealthnews.org/features/insuring-your-
health/2013/042313-michelle-andrews-robotic-surgery.aspx. Last accessed October 5, 2013
67. AAGL Position Statement: Robotic‐Assisted Laparoscopic Surgery in Benign Gynecology. Journal of Minimally Invasive Gynecology Volume 20, Issue 1, January–February 2013, Pages 2–9
68. Statement on Robotic Surgery by ACOG President James T. Breeden, MD. American Congress of Obstetricians and Gynecologists, Washington, DC. March 14, 2013. Online.
http://www.acog.org/About_ACOG/News_Room/News_Releases/2013/Statement_on_Robotic_Surgery. Last accessed October 5, 2013.
69. Commonwealth of Massachusetts, Board of Registration in Medicine, Quality and Patient Safety Division. ADVISORY ON ROBOT‐ASSISTED SURGERY,March 2013. Online:
http://www.mass.gov/eohhs/docs/borim/physicians/pca-notifications/robot-assisted-surgery.pdf. Last accessed October 5, 2013.
70. Arnold P. Advincula MD; Cheryl B. Iglesia MD; Rosanne M. Kho MD; Jamal Mourad, DO; Marie Fidela R. Paraiso, MD; Jason D. Wright, MD. The robot is gaining ground in gynecologic surgery. Should you
be using it? Roundtable. OBGManagement. April 2013 Vol. 25, No. 4
123
References
Tamer Seckin, MD [email protected]
THANK YOU!
35

CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsian
Indo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
36















![[D.T] Digimon Adventure V-Tamer 01](https://img.pdfslide.us/doc/110x75/568befb01a28ab89338d0d26/dt-digimon-adventure-v-tamer-01.jpg)