Embed Size (px)
Citation preview

Case presentation
By Dr. Muhammad Rashid
PGR WMW

Bio-data
• Patient, Mohammad Raza, 14 years male resident of Gujranwala and student of 7 class.
• Presented on 5th June, 2014 in nephrology OPD.

PATIENT PICTURE

Presenting complaints
• Sore throat for 10 days• Cola coloured urine for 1 day• Decrease urine output for 1 day

History of present illness
• My patient non-smoker, non-hypertensive and non-diabetic was in his usual state of health when he developed pain and irritation in throat. It was associated with fever, low grade not associated with rigors or chills and relieved by panadol from local doctor. Patient did not use any other medication except panadol. It improved in 3 days.

History of present illness• One day back patient started having cola coloured urine. It was sudden in onset not
associated with pain or shivering but associated with decreased output of urine. Patient noted that urine also contains some froth. Patient never had such episode before. Urine was never containing fresh blood or blood clots.
• Patient also noted mild swelling of the feet up to ankles only.

Systemic review
• Patient had decreased appetite and generalized weakness and he had to give support to take him to the washroom.
• History of decrease sleep.• No h/o vomiting or nausea.• No h/o bruising on skin or petechiae or rash.• No history of weight loss, vomiting, diarrhoea, nausea or
constipation.• No history of fits, neck rigidity, limb weakness or gait
abnormality.• No history shortness of breath, wheezing etc.

Past history
• Patient has never been admitted to hospital before in his life.

Personal and socio-economic history
• Patient is not a smoker• He is student and good in studies.• He has two siblings.• He belongs to a low socio-economic class.

Drug history
• No history of hakeem medication.• No history of any drug allergy.• No history of any medication except panadol
for this illness.

Family History
• No h/o such disease in the family

Differential diagnosis
• Post-streptococcal GN• IgA nephropathy• Drug induced GN• myoglobinurea

EXAMINATION

A young boy ill looking lying in bed, well cooperative with branula on his right forearm
• Pulse: 78/min• Bp: 160/100mm of Hg• Temp: 99 F• RR:• Pallor +ve• Pedal edema:+ve• Cyanosis: -ve• Jaundice: -ve• Koilonychia: -ve• Clubbing : -ve• Lymph nodes: not palpable• Thyroid gland : not enlarged• Petechia: not seen• Purpura: not seen

Abdominal & Genito urinary examination
• Flat abdomen, no scar mark, no striae, Genitalia normal on inspection, abdomen moving with breathing.
• Non tender in all quadrants, liver span is normal, spleen not palpable.
• Kidneys not palpable.• Shifting dullness –ve• Fluid thrill –ve• Bowel sounds normal.

RESPIRATORY SYSTEM
• Normal chest shape, no scar mark, striae, bruising, petichiae.
• Apex beat in 5th ICS• Trachea is central• Chest movements are bilateral equal and chest
expansion is 6cm.• Vocal fremitus is equal on both sides• On percussion, it is resonant and comparable bilaterally.• On auscultation, NVB with no added sounds.• Vocal resonance is equal on both sides.

CARDIO VASCULAR STSTEM
• Apex beat in 5th intercostal space. normal in character. Just medial to midclavicular line
• No parasternal heave• On auscultation, S1+ S2+ 0.

CENTRAL NERVOUS SYSTEM
• GCS 15/15• PERLA +• Higher mental functions intact• Sensory and motor system normal• No signs of meningeal irritation• Cerebellar system is intact• All Cranial nerves are intact

Investigations• WBC 9*103
• HB 8.0g/dl• Plt 422*103
• Blood urea 40• S.creatinine 1.0• Na +:138 K+:3.7• ALT 27• AST 32• Serum albumin 3.4• Urine C/E• Protein ++• Blood +++• Pus cells 4-5• aso titre >200

investigations
• Complement levels : Low complement levels• Anti-hcv : non reactive• HBsAg : non reactive• RA: -VE• ANA: -VE

Diagnosis after investigations
• POST STREPTOCCOCAL GN

TREATMENT STARTED
• Conservative treatment planned for POST-STREPTOCCOCAL GLOMERULONEPHRITIS Main aims were >BP control, >Salt and water restriction, >anemia correction, and >fluid and electrolytes replacement

• Patients RFTs rapidly worsen over 3 to 5 days• Repeated RFTs urea 110, s. creatinine 6.0• Urine output further deteriorated and patient
become anuric• Renal biopsy was planned to rule out rapidly
progressive glomerulonephritis.

• Patient started having uremic symptoms and he had to undergo 4 sessions of dialysis in next 10 days.

Renal biopsy
• Immunofluorescent staining demonstrates nonspecific granular immune deposits
• Confirming type II RPGN

What are the various uremic symptoms that you will see in your patient?

• Anorexia, Nausea, vomiting and diarrhoea• Shortness of breath• Muscle weakness• Restless leg syndrome• Encephalopathy• Uremic Froth• Platelet dysfunction leading to bleeding• Anemia• Pericarditis

What will be the length of first dialysis session?
a. 1 hrb. 2 hrsc. 3 hrsd. 4 hrse. 5 hrs

Why patient has deteriorated ?
What will be the findings you are expecting in renal biopsy report?

• His renal biopsy showed type II rapidly progressive glomerulonephritis
• CRESCENT formation between the bowman s capsule and glomerular tuft
• Immune complex deposition in basement membrane

What treatment options you will have now?
1. Keep patient on dialysis for lifetime2. Patient will recover spontaneously and stop
further dialysis immediately.3. Give anti-streptoccocal antibiotics and stop
dialysis.4. Give immunosuppressant and bridge up gap
with corticosteroids and dialysis

• Pt was put on deltacortril and on pulse therapy of cyclophosphamide.

What will be the possible side effects of cyclophosphamide and how to prevent the side effects

• Haemorrhagic cystitis• Hair loss• Vomitin,diarhea• Mouth sores • Weight loss• Leukopenia,anemia,thrombocytopenia• Suppress immune system leading to fatal
infections• Allergic reactions• Nephrotocicity• Male infertility,female premature menupause

> Adequate fluid intake,Avoidance of nighttime dosage,Mesna (sodium 2-mercaptoethane sulfonate),
a sulfhydryl donor which binds and detoxifies acrolein.
LEUPROLIDE used to prevent premature menopause in females

What will be the dose and how to give cyclophosphamide?

MANAGEMENT OF RPGN2 phases of treatment 1. INDUCTION THERAPY >IV METHYL PREDNIDOLONE IG for 3 days >followed by prednisolone 1mg/kg for 10-14
days. >then pulsed cyclophosphamide 1 g every
month for 6 months

• 2. MAINTANANCE PHASELow dose steriod and azathioprine are
continued for further 12-18 months

• Patient’s uremic symptoms improved with dialysis sessions and urine output also improved after 10 days of treatment.
• Patient was transfused twice during this stay• At 11th PAD, patient’s attendant noticed that
patient is not moving his right half of body.• It was then confirmed on clinical examination
that power in right leg is 3/5 and right arm is 2/5. Right planter is upgoing.

• As patient was already on prophylactic anticoagulant, so it was stopped immediately and CT scan is planned.

Why patient suffered weakness?

Why patient was getting prophylactic anti-coagulation?

Why anti-coagulation was stopped immediately?

What will be the differential diagnosis regarding weakness at this point in time?

• Thromboembolic phenomenon causing Ischemic stroke
• Haemorrhagic CVA d/t anticoagulation• Cyclophosphamide induced neutropenia
leading to brain Infections• SOL

• CT scan came out to be normal.• Showing no hemorrhage or ischemic infarct.

• Anti-coagulation is restarted and MRI is planned.

• Weakness was static and did not fluctuate or improved.
• Patient is also drowsy and GCS is 13/15.

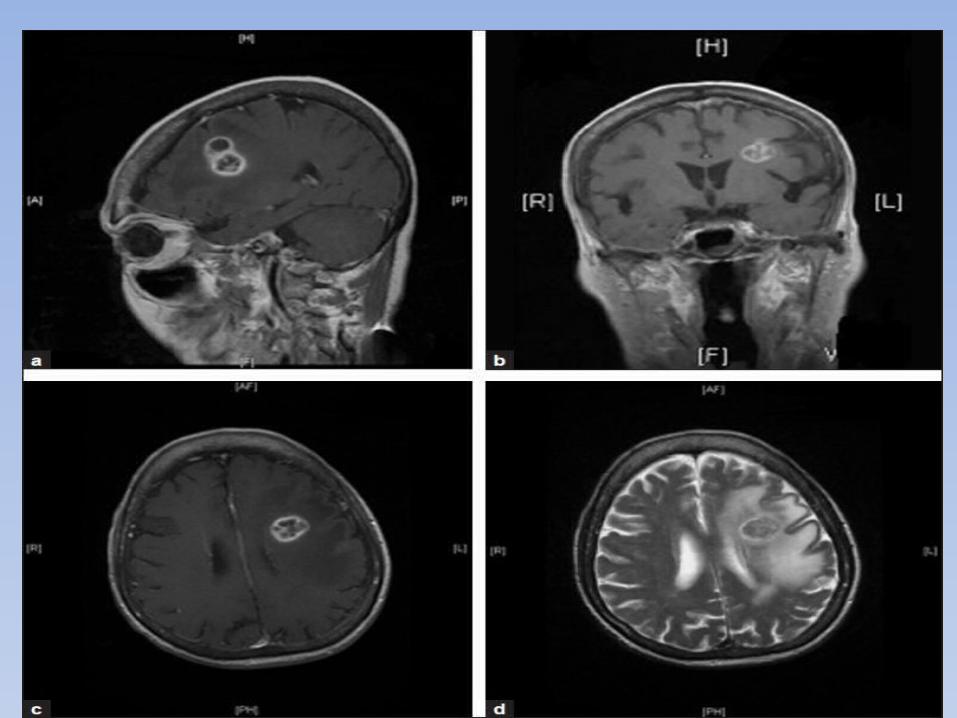
• MRI brain was done after 3 days and its reporting came after 2 days.
• MRI showed two contrast enhancing lesions in left sided hemisphere and which are reported as aspergiloma.

Why patient suffered from aspergiloma?

Was it related to our treatment?

How to manage now?

• Amphotericin B• Test dose 1mg IV infused over 20-30 min• Load 0.25-0.5mg/kgIV over 2-6 hours• Maintenance 0.25-1mg/kg iv

What are possible side effects of amphotericin B?

• Anorexia• Headache• Hypokalemia, hypomagnesemia• Hypotension• Nephrotoxicity• Flushing• Leukocytosis• Bone marrow suppression

Follow up
• Amphotericin B was started and immunosuppressant therapy was continued.
• After 10 days patients RFTs returned to the normal value and double lumen was removed as no further dialysis was required.
• Adequate urine ouput and normal urine complete was achieved.
• With further 15 days of amphotericin B therapy, conscious level and weakness improved.

Type Percentage of RPGN Cases CausesType 1: Anti-GBM antibody–mediated ≤ 10% Anti-GBM GN (without lung
hemorrhage*)Goodpasture syndrome (with lung hemorrhage)
Type 2: Immune complex ≤ 40% Postinfectious causes:•Antistreptococcal antibodies (eg, poststreptococcal GN) •Infective endocarditis•Vascular prosthetic nephritis•Viral hepatitis B infection•Visceral abscess or sepsisConnective tissue disorders:•Anti-DNA autoantibodies (eg, lupus nephritis)•IgA immune complexes (eg, immunoglobulin A–associated vasculitis GN, formerly Henoch-Schönlein purpura GN)•Mixed IgG-IgM cryoglobulins (eg, cryoglobulinemic GN)Other glomerulopathies:•IgA nephropathy•Membranoproliferative GN
Type 3: Pauci-immune ≤ 50% Eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome)Pulmonary necrotizing granulomas (eg, granulomatosis with polyangiitis)Renal-limited disease (eg, idiopathic crescentic GN)Systemic necrotizing arteritis (eg, polyarteritis nodosa)
Type 4: Double-antibody positive Rare Same as for as types 1 and 3Idiopathic Rare No clear cause

Go Nawaz Go





























