Embed Size (px)
Citation preview
An Overview of
STREPTOCOCCAL INFECTIONS
By
Dr. Basil, B. C – MBBS (Nig),Department of Chemical Pathology/Metabolic Medicine,
(Microbiology Postings)
Benue State University Teaching Hospital, Makurdi.
February 2016. 1
INTRODUCTION:
• STREPTOCOCCI are widely distributed in nature and some are members of the normal flora while others are pathogenic• Pathogenicity can be attributed in part to• Infection by the organism, and • Sensitization to them
• They elaborate a variety of extracellular substances and enzymes• They are a large and heterogeneous group of bacteria impossible to
classify into one system• Classification by various properties is key to understanding their
medical importance.
2
IDENTIFICATION:• Gram positive spheres (cocci) like staphylococci• But unlike staphylococci that appear in clusters, streptococci appear
in strips (chains) on gram stain – determined by their planes of division• 1µm in diameter and usually capsulated• Facultative anaerobes (some species – microaerophilic)• Some – Capnophilic• For most – growth and hemolysis are aided by incubation in 10% CO2
• They are catalase negative• Non-sporing bacteria and non-motile.• Growth requires enriched media containing blood or serum.
3
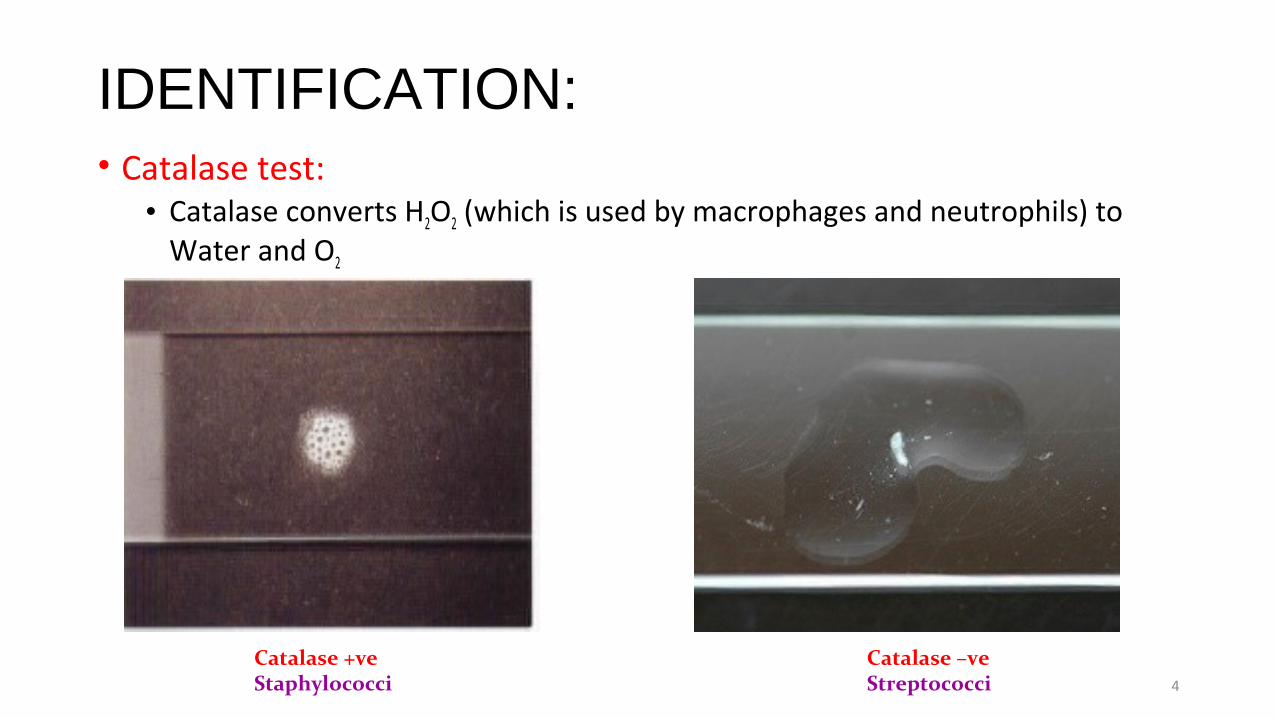
IDENTIFICATION:• Catalase test: • Catalase converts H2O2 (which is used by macrophages and neutrophils) to
Water and O2
4
Catalase +veStaphylococci
Catalase –veStreptococci
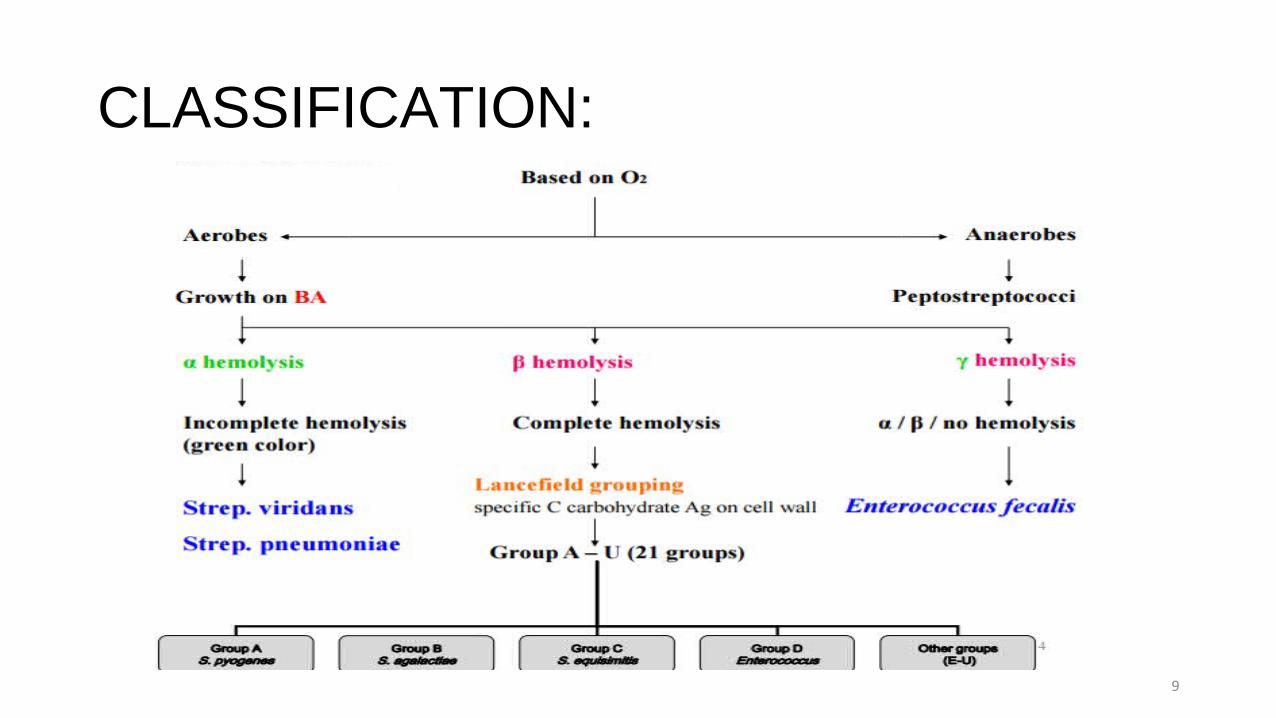
CLASSIFICATION:• Based on the hemolytic properties:
Beta-hemolytic: - clear zone of hemolysis around the colony Alpha-hemolytic: - greenish discolouration of the culture medium around the
colony (partial hemolysis) Gamma-hemolytic: - no hemolysis of RBCs (Non-hemolytic streptococci)
• Based on antigenic characteristics of cell wall CHO (C – carbohydrate) – Lancefield Antigens (Serologic Classification from A to V):
Out of over 30 species of streptococci, only 5 are significant human pathogens
3 have Lancefield Antigens: Group A – (S. pyogenes), Group B – (S. agalactiae), and Group D – (Enteroccoci + Non-enterococci)
2 have no Lancefield antigens – Lancefield Non-groupable: S. pnuemoiae, and Viridans group Streptoccoci
5
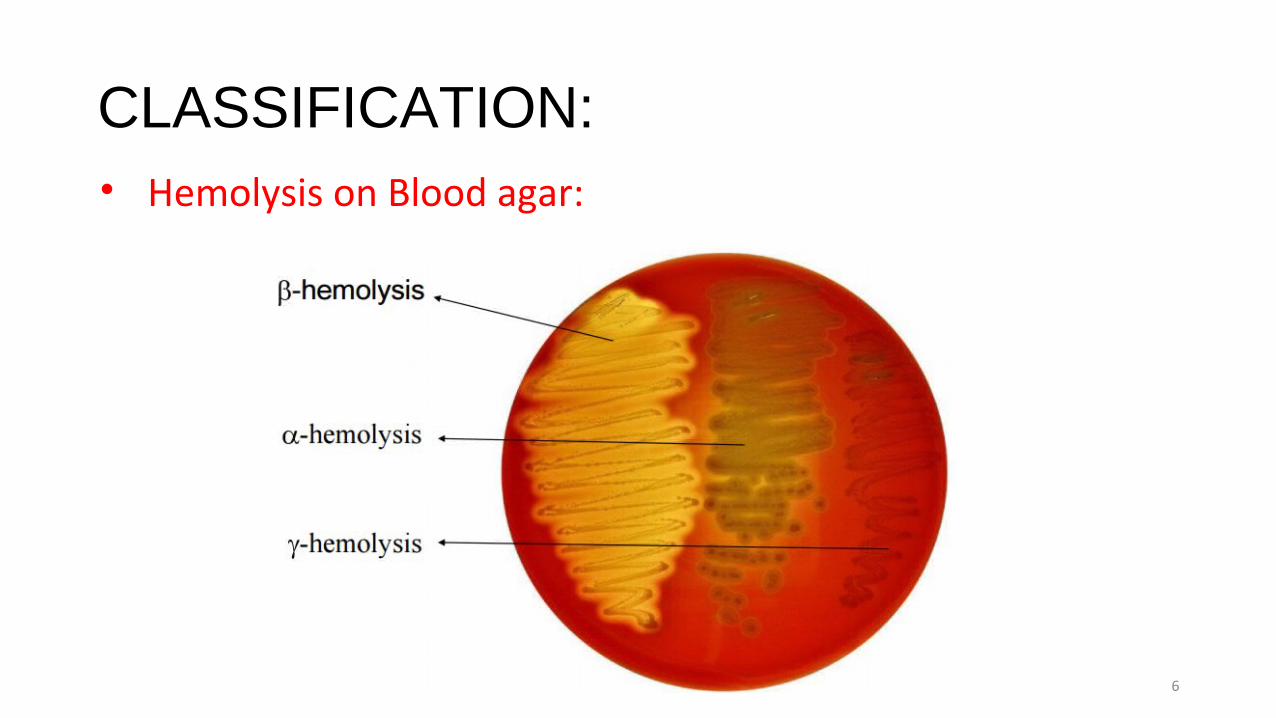
CLASSIFICATION:• Hemolysis on Blood agar:
6
CLASSIFICATION:
• Historically, Lancefield antigens have been used as a major way of differentiating the many streptococci though not applicable to a number of organisms including some pathogenic species• Identification of Streptococcal organisms require a combination of
several characteristics including:• Antigenic composition including Lancefield antigens,• Patterns of hemolysis,• Biochemical reactions,• Growth characteristics, and• Genetic studies
7
CLASSIFICATION:
8
CLASSIFICATION:
9
BIOCHEMICAL REACTIONS:Differentiation between beta-hemolytic streptococci:
10
• Bacitracin susceptibility test• CAMP test• Bile Esculin Test
BIOCHEMICAL REACTIONS:Bacitracin Test -
11
• Bacitracin susceptibility Test:• Specific for S. pyogenes (Group A) – for its presumptive identification
• Principle:• To distinguish between S. pyogenes (susceptible to B) & non group A such as S.
agalactiae (resistant to B)• Bacitracin will inhibit the growth of Group A – S. pyogenes giving zone of inhibition
around the disk
• Procedure:• Inoculate BAP with heavy suspension of tested organism• Bacitracin disk (0.04 U) is applied to inoculated BAP• After incubation, any zone of inhibition around the disk is considered as susceptible
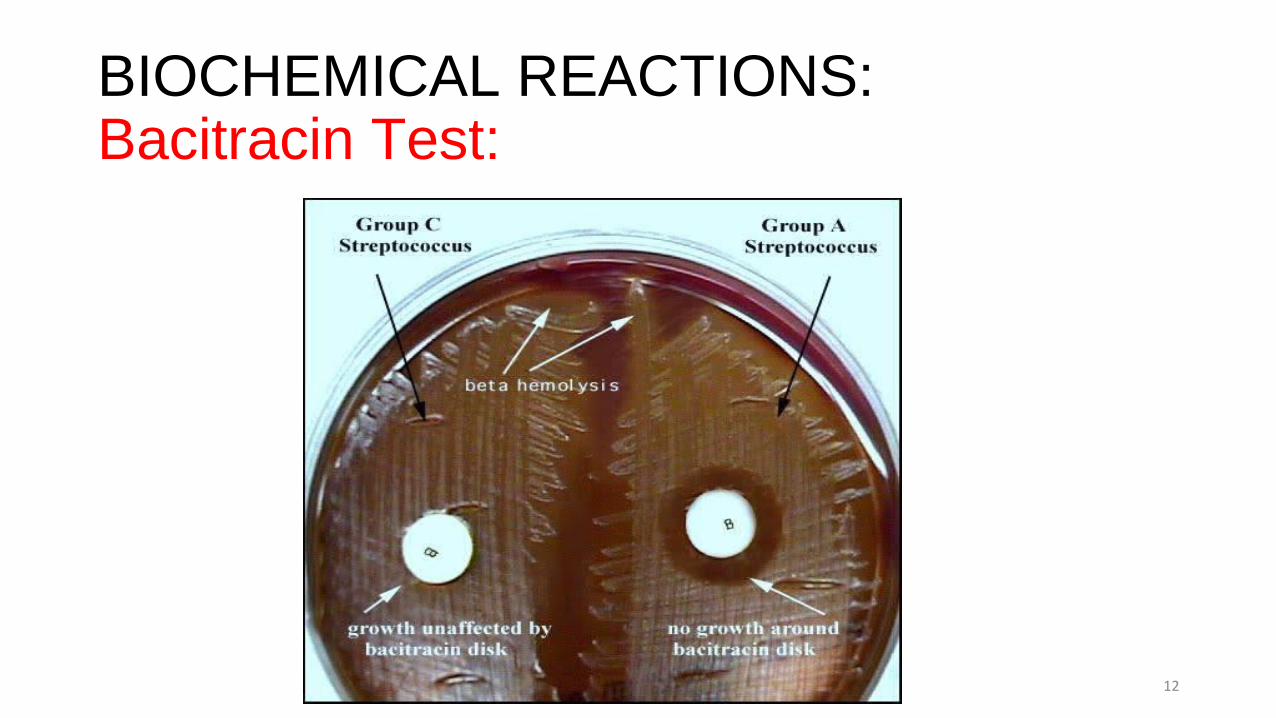
BIOCHEMICAL REACTIONS:Bacitracin Test:
12
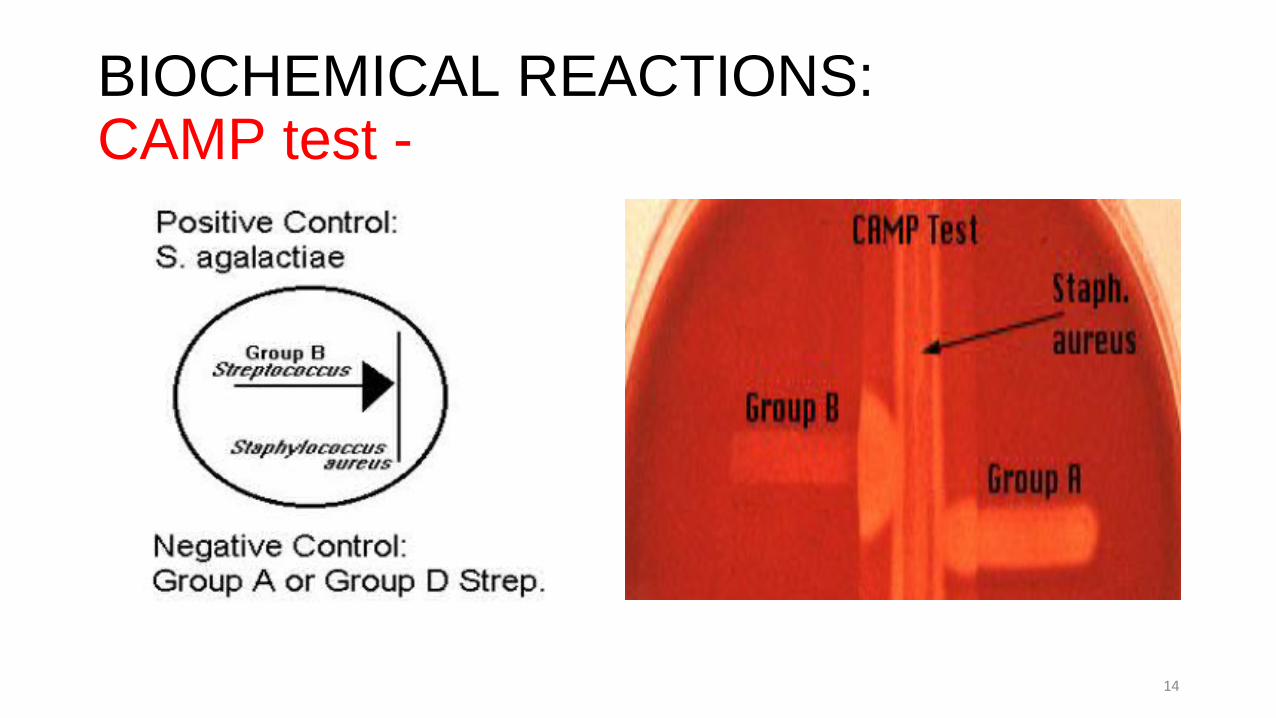
BIOCHEMICAL REACTIONS:CAMP test – (Christie Atkins Munch-Petersen)
• Principle:• Group B streptococci produce extracellular protein (CAMP factor)• CAMP act synergistically with staph. beta-lysin to cause lysis of RBCs
• Procedure:• Single streak of streptococci to be tested and staph. aureus are made
perpendicular to each other• 3 – 5mm distance was left between two streaks• After incubation, a positive result appear as an arrowhead shaped zone of
complete hemolysis
• S. agalactiae is CAMP test positive while non-group B streptococci are negative
13
BIOCHEMICAL REACTIONS:CAMP test -
14
BIOCHEMICAL REACTIONS:Bile Esculin Test - • Differential agar (BEA) used to isolate and identify Enterococcus (group D
streptococci) and differentiate it from other streptococci• Bile salts are the selective component, while Esculin is the differential
component• Must be interpreted in conjunction with gram stain morphology• Principle:
• Enterococcus hydrolyze Esculin liberating glucose (which is used up) and Esculetin. • Esculetin react with ferric citrate in the medium to produce insoluble iron salts,
resulting in the blackening of the medium• Many bacteria can hydrolyze Esculin, but only few can do so in the presence of bile.
15
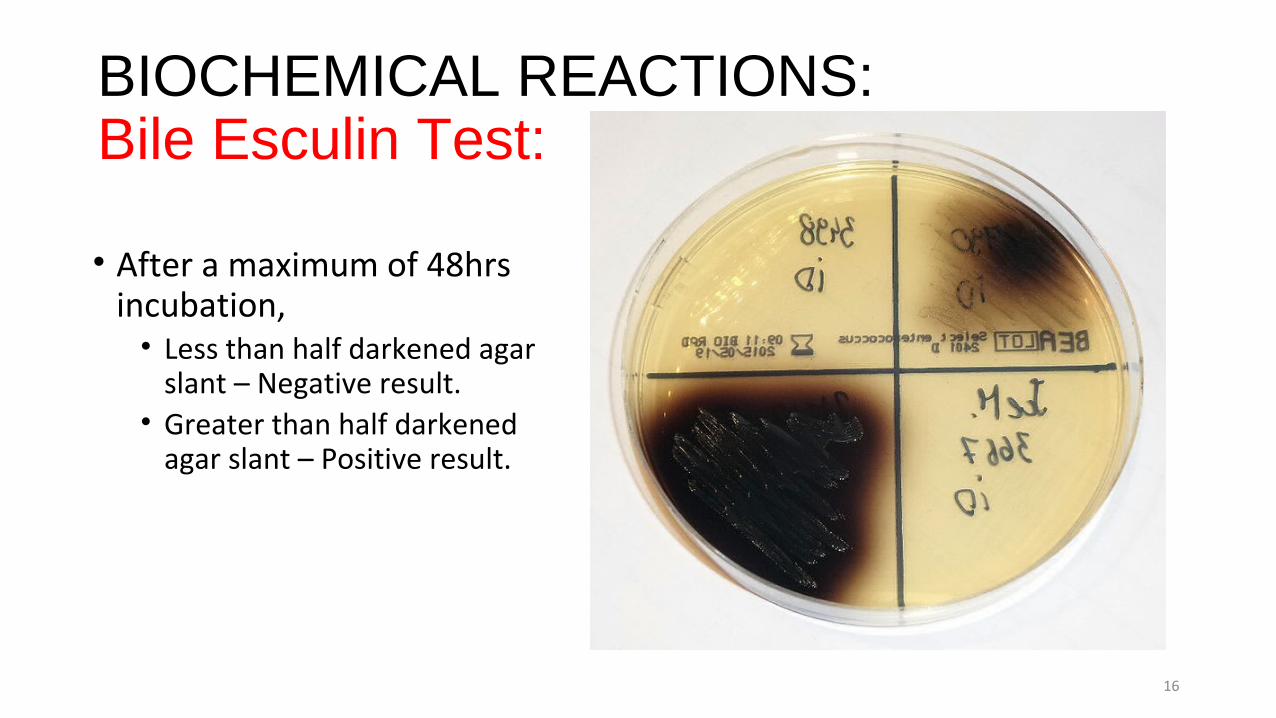
BIOCHEMICAL REACTIONS:Bile Esculin Test:
• After a maximum of 48hrs incubation,• Less than half darkened agar
slant – Negative result.• Greater than half darkened
agar slant – Positive result.
16
BIOCHEMICAL REACTIONS:Differentiation between alpha-hemolytic Streptococci
• Optochin test• Bile solubility test• Inulin fermentation
17
BIOCHEMICAL REACTIONS:Optochin test - • Principle:• S. pneumonia is inhibited by Optochin reagent (<5 μg/mL) giving an inhibition
zone of ≥14mm in diameter.
• Procedure:• BAP is inoculated with the organism to be tested and an Optochin disc placed
in the center of the plate• After incubation at 37oC for 18hrs, carefully measure the diameter of the
inhibition zone with a ruler• ≥14mm is positive; ≤ 13mm is negative
• S. pneumonia is positive (S); S. viridans is negative (R)
18
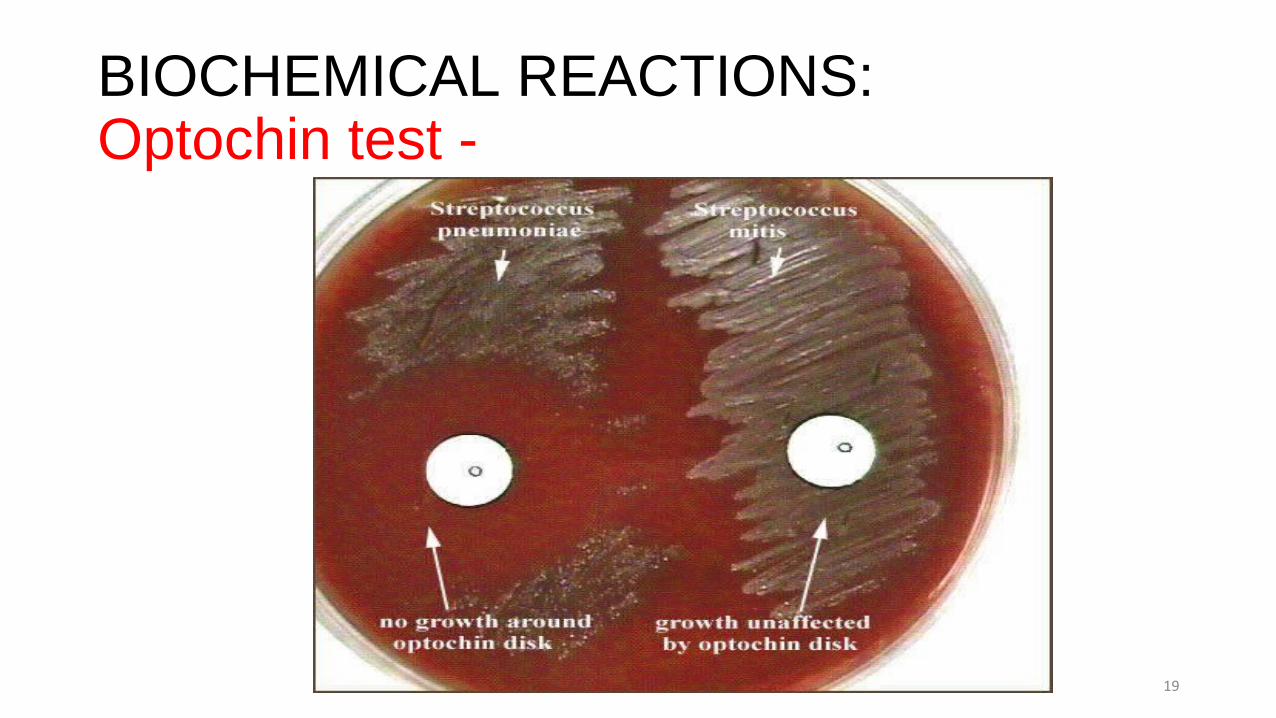
BIOCHEMICAL REACTIONS:Optochin test -
19
BIOCHEMICAL REACTIONS:Bile solubility test -• Principle:• S. pneumonia produce a self-lysing enzyme capable of inhibiting its growth
and this is accelerated in the presence of bile.
• Procedure:• Add 10 parts of the broth culture of the organism to be tested to one part of
2% Na-deoxycholate (bile) in a test-tube• Negative control is made by adding saline instead of bile to the culture• Incubate at 37oC for 15mins• Observe and record your findings.
20
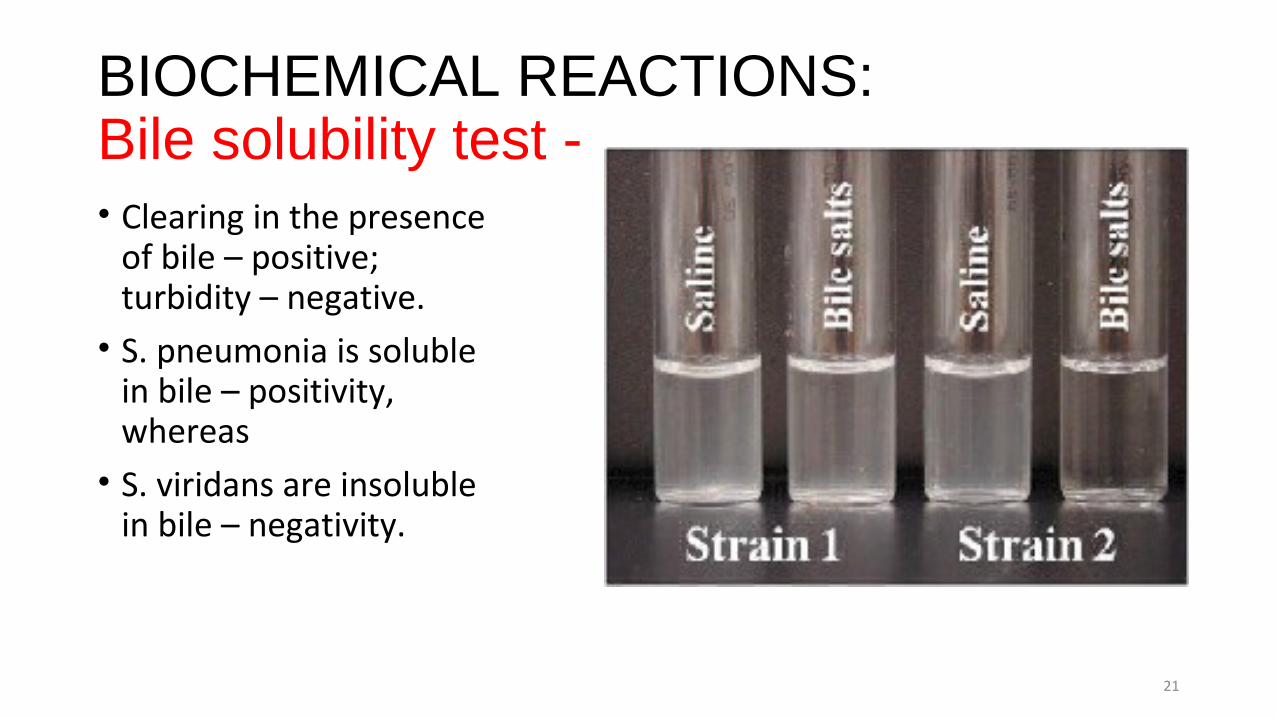
BIOCHEMICAL REACTIONS:Bile solubility test -• Clearing in the presence
of bile – positive; turbidity – negative.• S. pneumonia is soluble
in bile – positivity, whereas• S. viridans are insoluble
in bile – negativity.
21
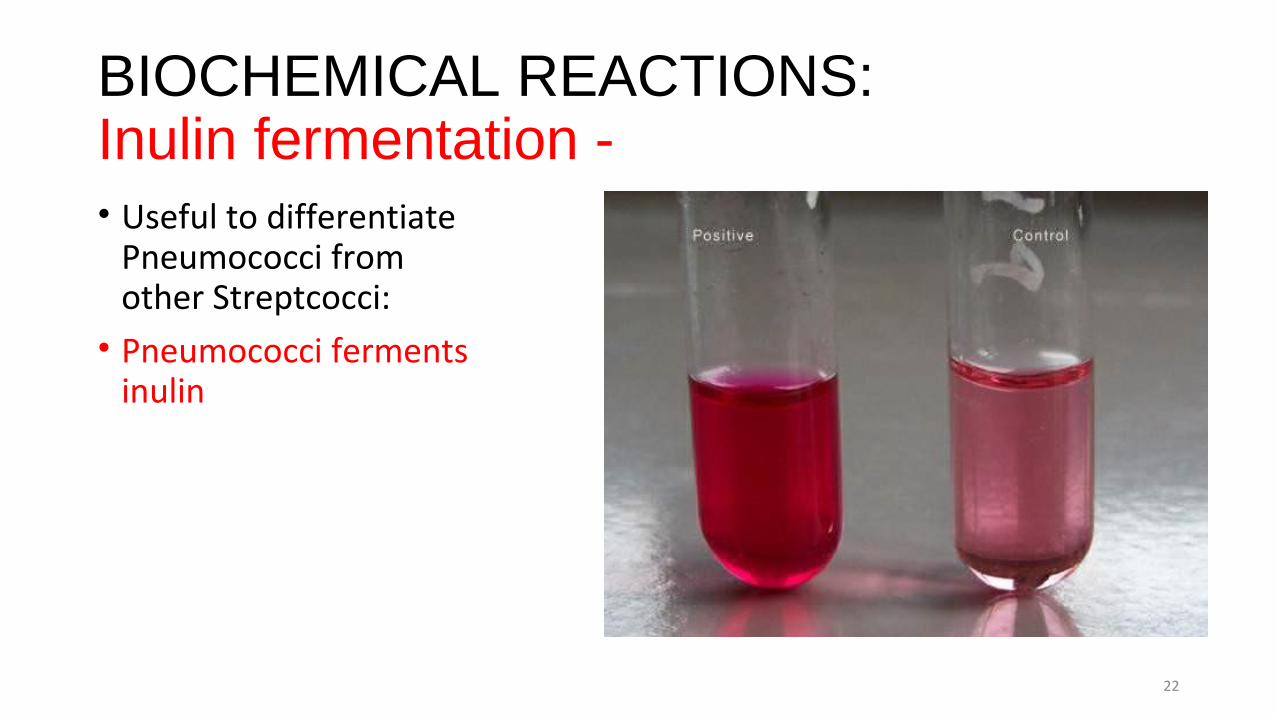
BIOCHEMICAL REACTIONS:Inulin fermentation - • Useful to differentiate
Pneumococci from other Streptcocci:• Pneumococci ferments
inulin
22
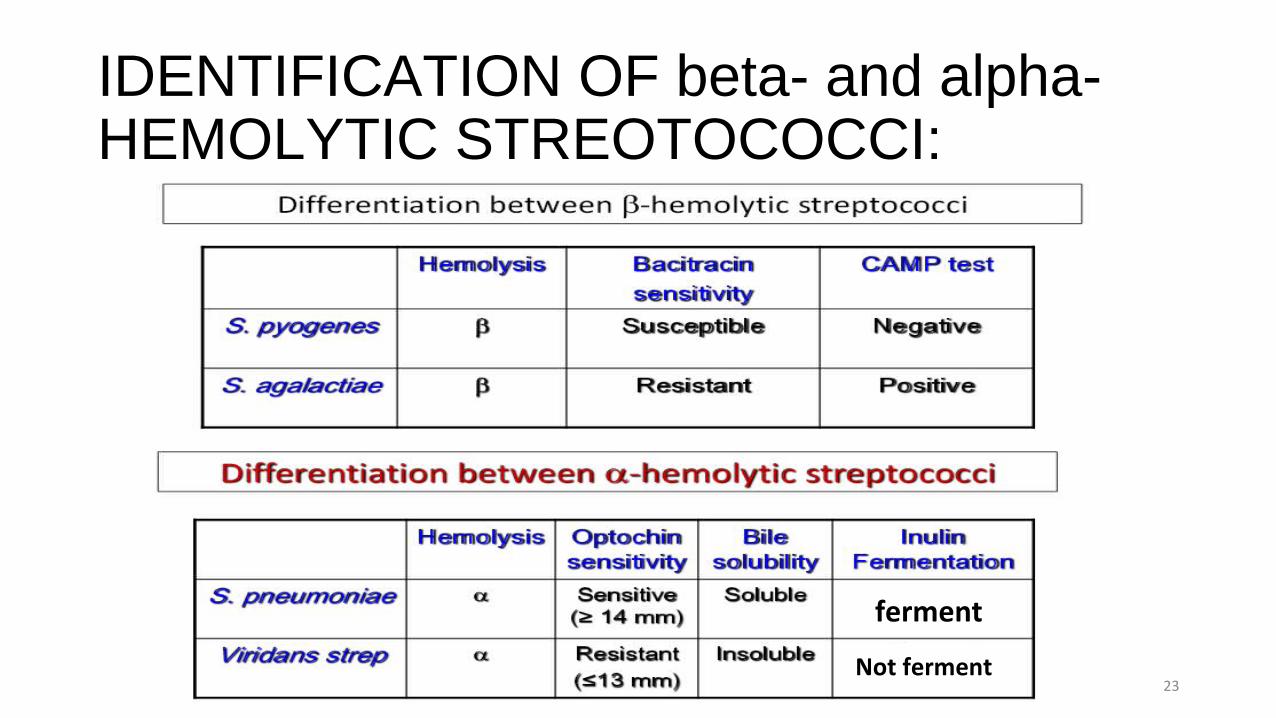
IDENTIFICATION OF beta- and alpha-HEMOLYTIC STREOTOCOCCI:
23
ferment
Not ferment
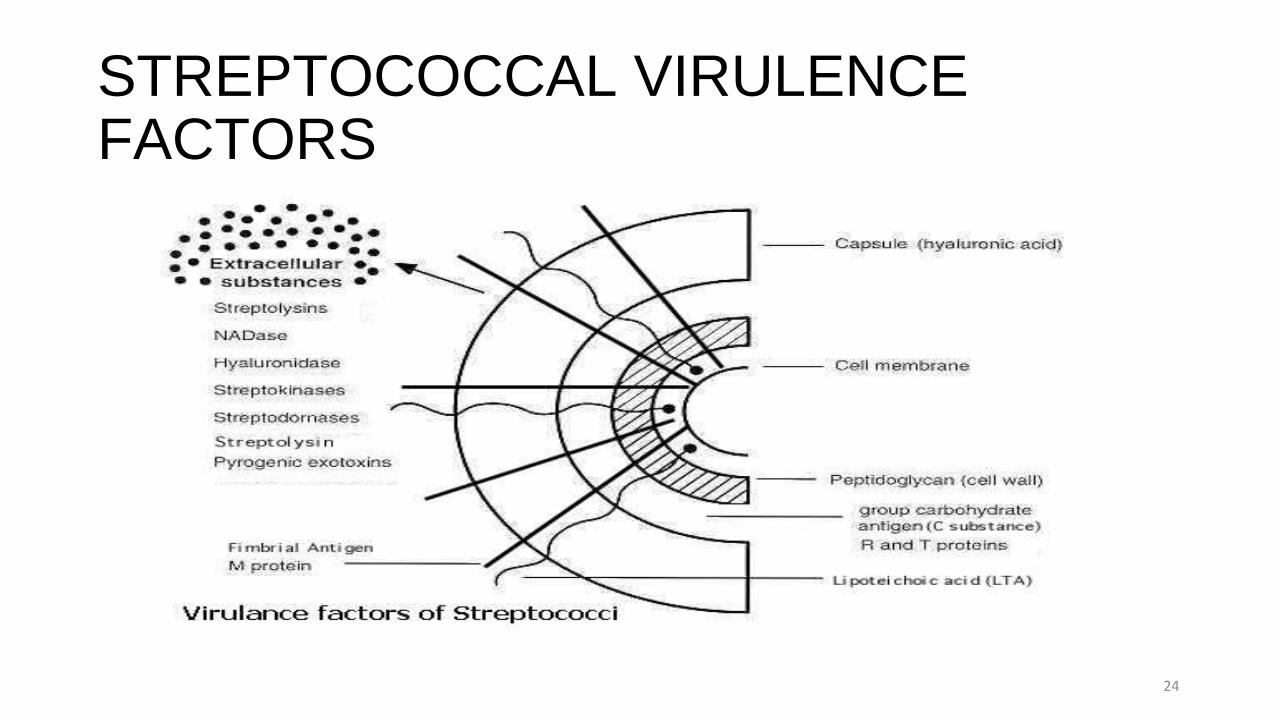
STREPTOCOCCAL VIRULENCE FACTORS
24
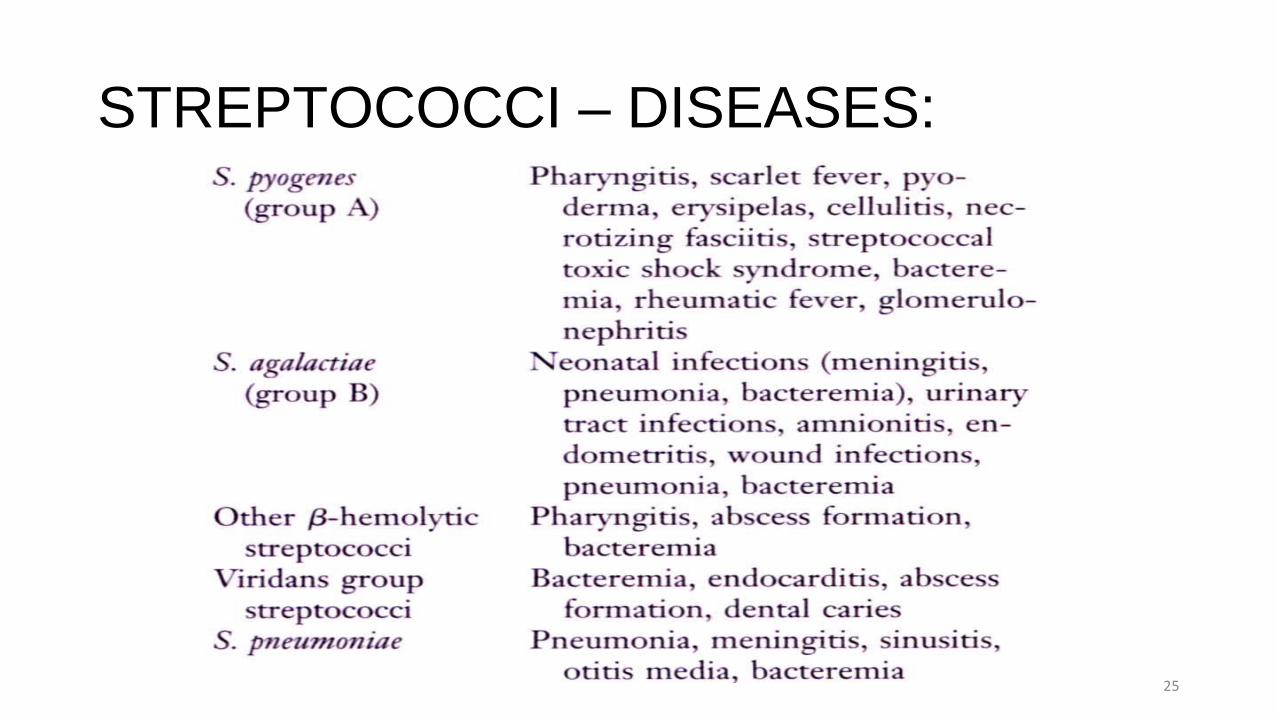
STREPTOCOCCI – DISEASES:
25
GROUP A: Streptococcus pyogenesMETABOLISM:• Catalase – negative • Microaerophilic• Beta-hemolytic – due to enzymes that destroy blood cells• Streptolysin-O:
• Oxygen labile• Antigenic
• Streptolysin-S:• Oxygen stable• Non-antigenic
26
VIRULENCE:
• M-protein (70 types) – major virulence factor• Adherence factor• Antiphagocytic• Antigenic: induces antibodies which can lead to phagocytosis
• Lipoteichoic acid:• Adherence factor
• Streptokinase - FIBRINOLYSIN• Hyaluronidase – destroys CT and aids spread of the organism• DNAase (Streptodornase)• Anti-C5a peptidase – prevents C5a mediated phagocytic activity• Protein F - • Streptolysin O – also antigenic; (but Streptolysin S – not antigenic)
• Hence Anti-Streptolysin O (ASO) antibody titer rises in recent infections• Skin infection does not induce ASO
27
TOXINS:
• Erythrogenic or pyrogenic toxin (produced only by lysogenized Group A Streptococci): responsible for scarlet fever• More than 4 serologically distinct toxins (Spe - A, B, C and F).• Dick Test: once commonly used to confirm Scarlet Fever diagnosis.• Some strains produce pyrogenic exotoxins which act as superantigens that
superstimulate T cell leading to release of cytokine which cause the Toxic shock syndrome.
• Toxic shock syndrome toxin (similar to, but different from the staph exotoxin TSST-1)
28
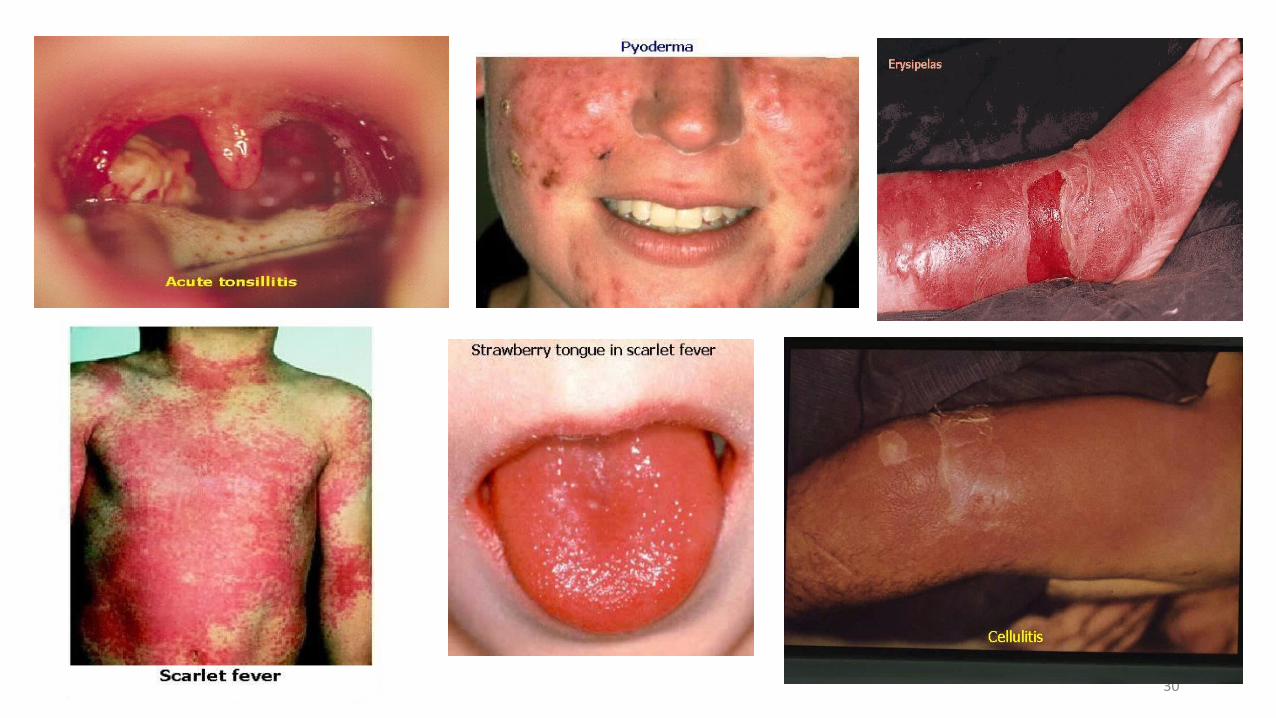
PATHOLOGY:DIRECT INVASION/TOXIN:•Pharyngitis:
• Red, Swollen tonsils and pharynx• Purulent exudate on tonsils• Fever• Swollen lymph nodes
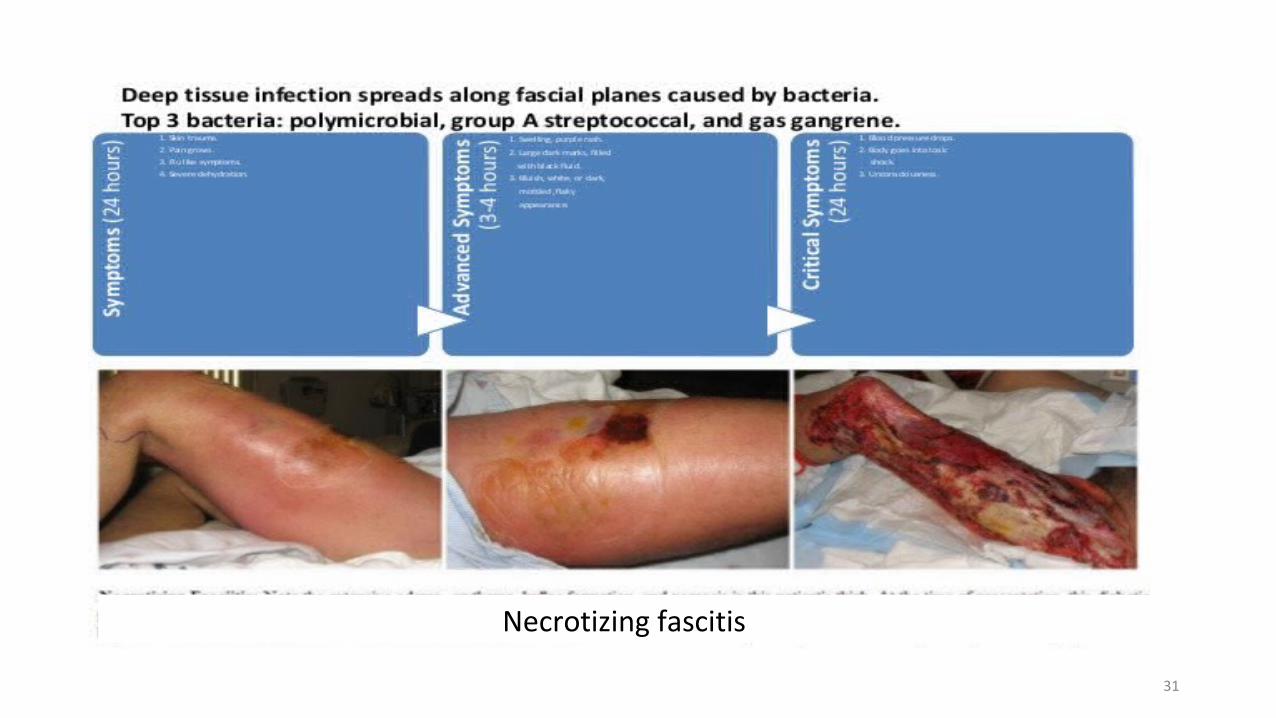
•Skin infections:• Folliculitis, Erysipelas, pyoderma• Cellulitis• Impetigo• Necrotizing fasciitis
•Scarlet fever: - fever and scarlet red rash on body•Toxic shock syndrome
29
30
31
Necrotizing fascitis
PATHOLOGY:ANTIBODY MEDIATED (Delayed):•Rheumatic fever (may follow streptococcal pharyngitis):
• Fever• Myocarditis: heart inflammation >> Rhuematic valvular heart disease many years
later.• Arthritis: migratory polyarthritis• Chorea (Sydenham’s chorea or St. Vitus dance)• Rash: Erythema marginatum• Subcutaneous nodules: 10 – 20 yrs after infection, may develop permanent heart
valve damage
•Acute post-streptococcal Glomerulonephritits:• Tea or coca cola coloured urine, following streptococcal skin or pharynx infection• Follows skin or throat infection by Nephritogenic strains
32
DIAGNOSIS:
• Gram stain: - gram positive cocci in chains• Culture on standard laboratory media: - Growth is inhibited by
bacitracin• S. pyogenes is the only beta-hemolytic strep which is sensitive to bacitracin
• Pharyngitis: - Throat swab rapid antigen detection test (RADT) is specific for S. pyogenes and immunologically detects group A carbohydrate antigen.• In children, RADT should be backed up by a throat culture due to the high
incidence of “strep throat” and moderate sensitivity to RADT.
33
TREATMENT:
• Penicillin G• Penicillin V• Penicillinase-resistant penicillin e.g Dicloxacillin: in skin infections,
where staphylococci could be the responsible organism Following rheumatic fever:
Patients are placed on continuous prophylactic antibiotics to prevent repeat strep throat infection that could potentially lead to repeat case of rheumatic fever
For invasive S. pyogenes infections, such as necrotizing fasciitis or streptococcal toxic shock syndrome, consider adding Clindamycin.
34
GROUP B: Streptococcus agalactiaeMETABOLISM:• Catalase – negative• Facultative anaerobe• Beta-hemolytic
• Part of normal flora:• 25% of pregnant women carry Group B streptococci in their vagina.• Can be transmitted to neonates during birth
35
PATHOLOGY:
• Neonatal meningitis• Neonatal pneumonia• Neonatal sepsis• Sepsis in pregnant women (with secondary infection of fetus)• Increasing incidence of infections in elderly >65yrs of age and patients
with diabetes or neurological disease: causes sepsis and pneumonia
36
DIAGNOSIS:
• Gram stain of CSF or Urine: - positive cocci in chains• Culture of CSF, Urine or Blood
37
TREATMENT:
• Penicillin G
38
GROUP C and G Streptococcus:
• Beta-hemolytic• S. equi, S. canis• Associated diseases:• Pharyngitis, pneumonia, cellulitis, pyoderma, erysipelas, impetigo, wound
infections, puerperal sepsis, neonatal sepsis, endocarditis, septic arthritis
• Treatment:• Penicillin, vancomycin, cephalosporins, macrolides (variable susceptibility)
39
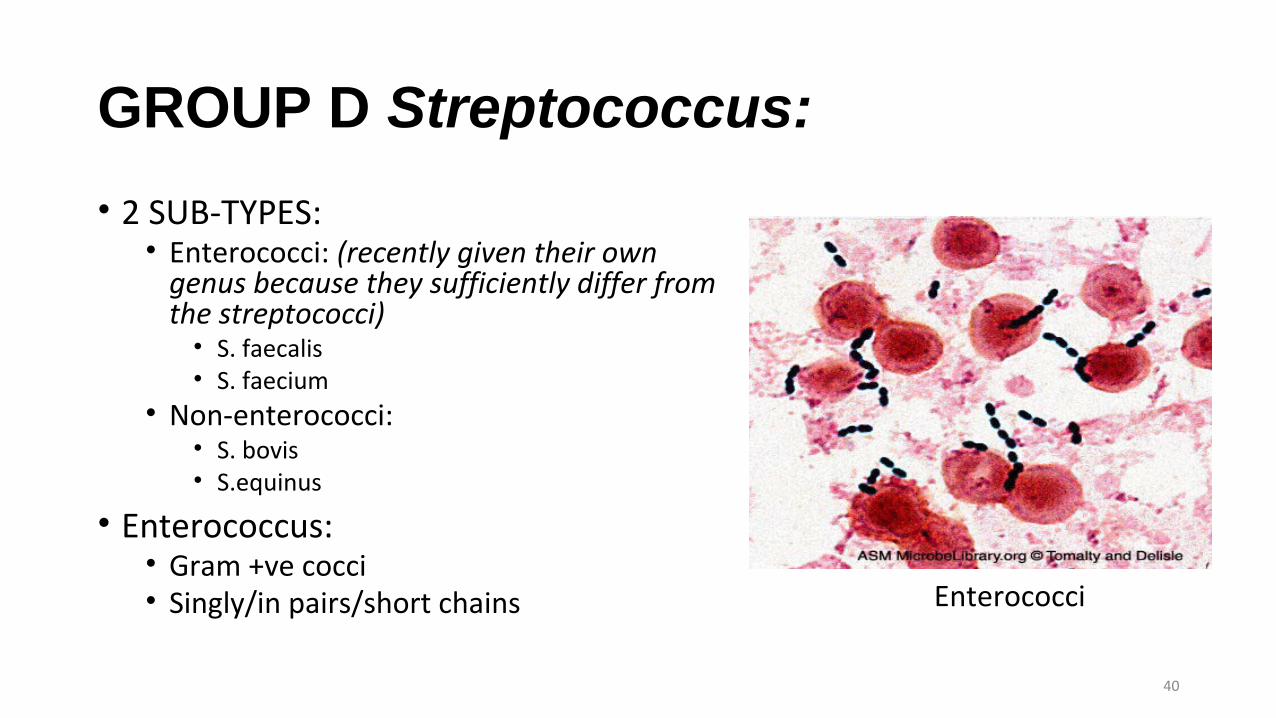
GROUP D Streptococcus:
• 2 SUB-TYPES:• Enterococci: (recently given their own
genus because they sufficiently differ from the streptococci)• S. faecalis• S. faecium
• Non-enterococci:• S. bovis• S.equinus
• Enterococcus:• Gram +ve cocci • Singly/in pairs/short chains
40
Enterococci
METABOLISM:
• Catalase – Negative• Facultative anaerobes• Usually Gamma-hemolytic, but maybe alpha-hemolytic• Positive bile esculin test
41
VIRULENCE:
• Extracellular dextran helps them bind to heart valves
42
PATHOLOGY:
• Sub-acute bacterial endocarditis• Biliary tract infections• Urinary tract infections (especially the Enterococci)• S. bovis is associated with colonic malignancies
43
DIAGNOSIS:
• Gram stain – positive cocci in chains• Culture:• Enterococci can be cultured in:
• 40% bile• 6.5% Sodium chloride
• Non-enterococci can only grow in bile
44
TREATMENT:
• Ampicillin, sometimes combined with an aminoglycoside• Resistant to Penicillin G• Emerging resistance to vancomycin• For vancomycin resistant organisms (VRE), consider Linezolid,
Daptomycin and Nitrofurantoin.
45
VIRIDANS GROUP Streptococci:
• Part of normal oral flora,• Found in the nasopharynx and gingivial crevices• GI tract
• Members:• Mitis group: S. mitis, S. sanguis, S. parasanguis, S. gordonii, S. crista, S.
infantis, S. oralis, S. peroris• Salavarius group: S. salavarius, S. vestibularis, S. thermophiles• Mutans group: S. mutans, S. sobrinus, S. criceti, S. rattus, S. downeii, S.
macacae• Angionosus group: S. angionosus, S. constellatus, S. intermedius
46
METABOLISM:
• Catalase – negative• Facultative anaerobes• Mostly alpha-hemolytic; some beta- and gamma• Resistant to Optochin• Bile solubility - Negative
47
VIRULENCE:
• Extracellular dextran – helps them bind to heart valves
48
PATHOLOGY:
• Sub-acute bacterial endocarditis: caused by S. mitis group• Dental caries (cavities): caused by S. mutans group• Brain or Liver abscesses: caused by S. angionosus group• Microaerophilic• Found alone in pure cultures or in mixed cultures with anaerobes
49
DIAGNOSIS:
• Gram stain• Culture – antibiotics may be added to inhibit growth of
contaminating bacteria• Resistant to optochin• Detection of group A streptococci by molecular methods:
PCR assay for pharyngeal specimens• Antibody detection• ASO titration for respiratory infections.• Anti-DNAase B and Antihyaluronidase titration for skin
infections.• Anti-streptokinase; Anti-M type-specific antibodies
50
TREATMENT:
• Penicillin G• Effective doses of penicillin or erythromycin for 10 days can prevent
post-streptococcal diseases.• Drainage and aggressive surgical debridement must be promptly
initiated in patients with serious soft tissue infections.• Antibiotic sensitivity test is helpful for treatment of bacterial
endocarditis.
51
Streptococci Pneumoniae (Pnuemococcus):METABOLISM:• Gram-positive lancet-shaped diplococci.• Alpha-hemolytic (Pneumolysin is similar to streptolysin O).• Form small round colonies on the plate, at first dome-shaped and
later developing a central plateau with an elevated rim.• Facultative anaerobe• Autolysis is enhanced in bile salt.• Growth is enhanced by 5-10% CO2 – capnophilic.
52
VIRULENCE:
• Polysaccharide Capsule (90 serotypes):• Protects the organism from phagocytosis• Highly antigenic – opsonized by antibodies specific to it• Due to the variable serotypes, surviving an infection from one serotype does
not confer immunity over the others
• Cell wall polysaccharide• Phosphocholine• Pneumolysin• IgA protease, etc.
53
TOXINS:• Pneumolysin: binds to cholesterol in host-cell membranes (but its
actual effect is unknown)• MAJOR HOST DEFENCE MECHANISM: - Ciliated Cells of the Resp tract
and Spleen• Loss of natural resistance may be due to:• Abnormalities of the respiratory tract (e.g. viral RT infections).• Alcohol or drug intoxication; abnormal circulatory dynamics.• Patients undergone renal transplant; chronic renal diseases.• Malnutrition, general debility, sickle cell anemia, hyposplenism or
splenectomy, nephrosis or complement deficiency• Young children and the elderly
54
PATHOLOGY:
• Pnuemonia – pneumococcus is the most common cause of pneumonia in adults• Meningitis – most common cause of bacterial meningitis in adults• Sepsis• Otitis media (most common cause in children)
55
DIAGNOSIS:• Gram stain: - reveals gram-positive
diplococcic• Culture: does not grow in presence of:
• Optochin• Bile
• Capsular polysaccharide antigen detection• DNA probe specific to S. pneumonia• Virulence to mice
56
Pneumococcus Specific DNA probe
DIAGNOSIS:
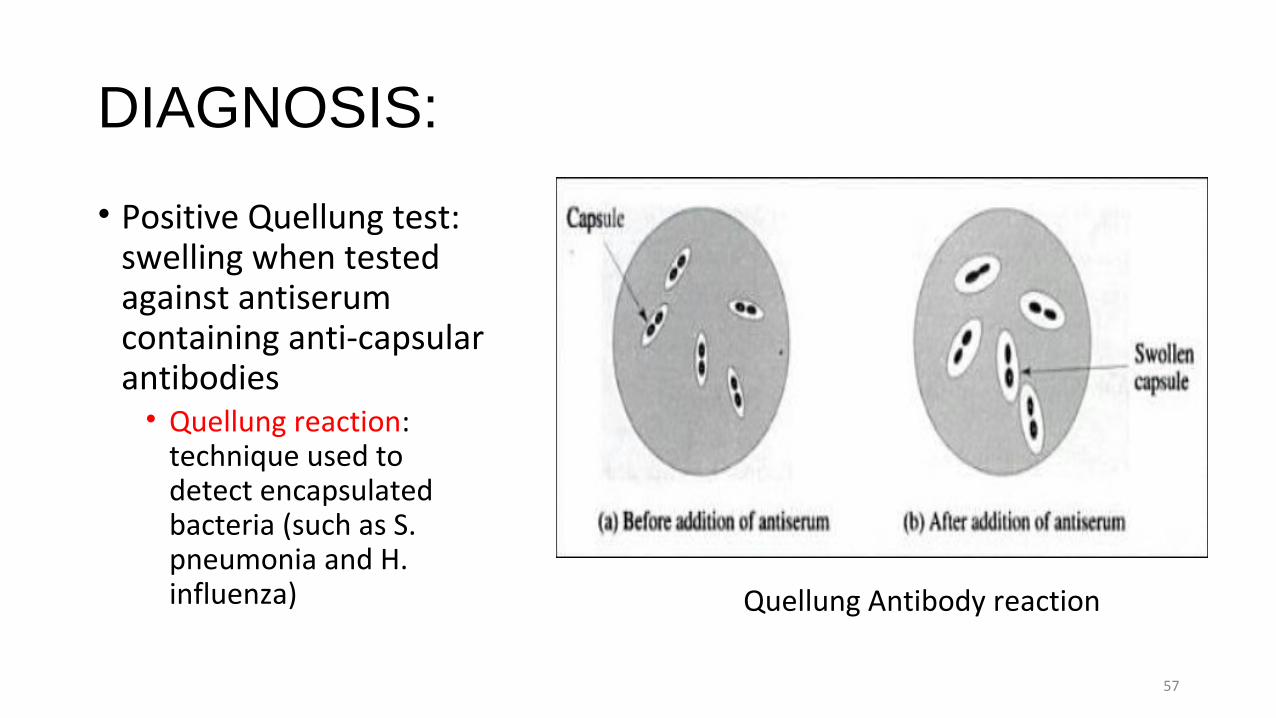
• Positive Quellung test: swelling when tested against antiserum containing anti-capsular antibodies• Quellung reaction:
technique used to detect encapsulated bacteria (such as S. pneumonia and H. influenza)
57
Quellung Antibody reaction
TREATMENT:
• Penicillin G (IM)• Erythromycin• Ceftriaxone• Vaccine: made against 23 most common capsular antigens.• Vaccinate individuals who are susceptible such as elderly or asplenic
individuals (including being functionally asplenic due to sickle cell anaemia)• Pnuemococcal conjugate vaccine - Capsular polysaccharide + Protein Carrier• Below 2yrs
• Heptavalent and the newer 13 valent conjugated vaccines are effective at preventing otitis media and pneumonia.
58
CONCLUSION:
• STREPTOCOCCI are widely distributed in nature and some are members of the normal flora while others are pathogenic• Pathogenicity can be attributed in part to• Infection by the organism, and • Sensitization to them
• They elaborate a variety of extracellular substances and enzymes• They are a large and heterogeneous group of bacteria impossible to
classify into one system• Classification by various properties is key to understanding their
medical importance.
59





























