Embed Size (px)
Citation preview

Post Partum Hemorrhage
PPH
Primary PPH
Within 24 hours of birth
>500 mL vaginal birth or >1000 mL C section
** Or any amount that causes symptoms
Secondary PPH
Abnormal or excessive bleeding
24 hrs to 12 weeks postnatal
Often assoc with endometritis
** Can further subdivide PPH as minor (500-1000 mL) or major (>1000 mL)
PPH
One of leading causes of maternal mortality
1-5% of deliveries
#1 cause postpartum women admitted to ICU
Blood flow to uterus at term: >700 mL/min
Blood loss often under-estimated and bleeding not
always obvious… so what signs can we look for?
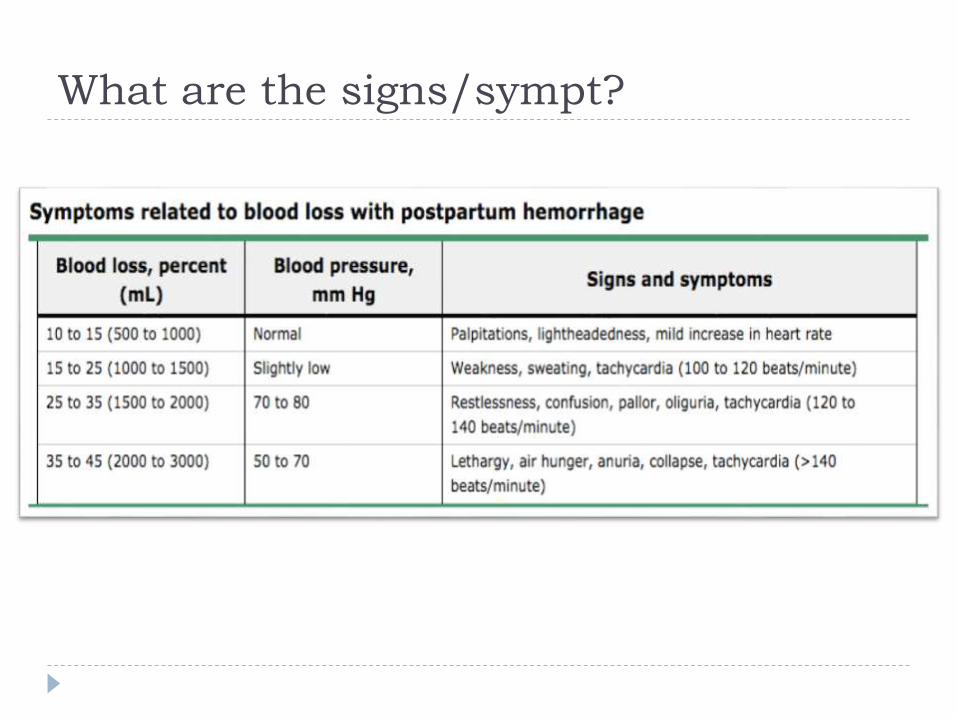
What are the signs/sympt?
Steps to managing PPH
Predict:
identify patients at risk
Prepare:
Multi-disiplinary approach, PPH protocol
Manage:
Timely, accurate diagnosis and appropriate interventions
Active management of 3rd stage of labour
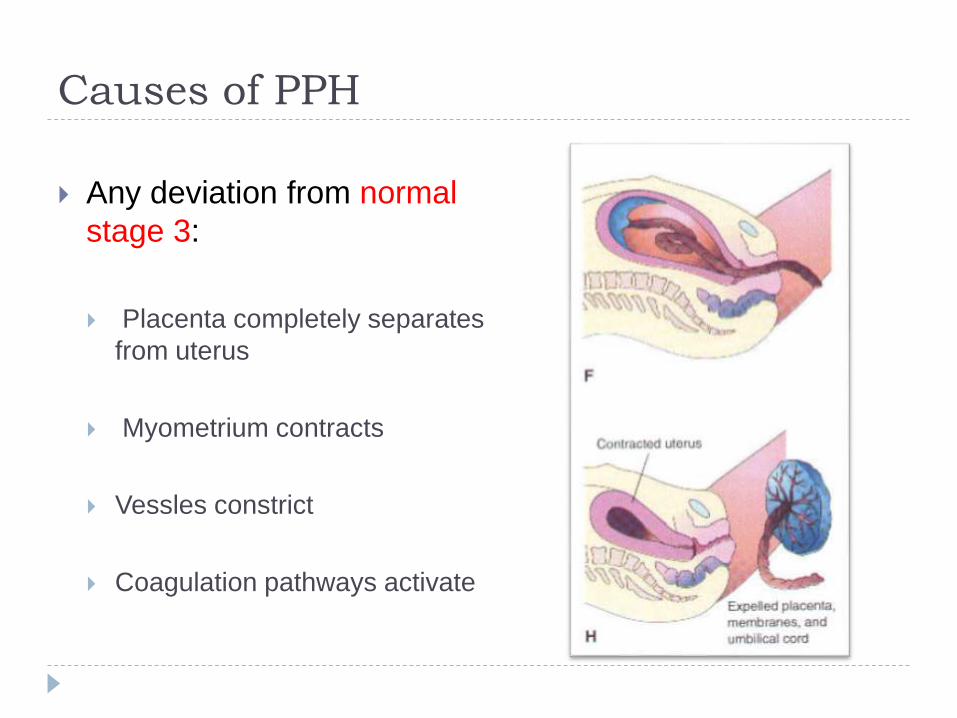
Causes of PPH
Any deviation from normal
stage 3:
Placenta completely separates
from uterus
Myometrium contracts
Vessles constrict
Coagulation pathways activate
4 T’s of PPH
Tone: Failure of uterus to contract
Tissue: Retained products in uterus
Trauma: Vaginal, perineal, uterine
Thrombin: Coagulation abnormalities
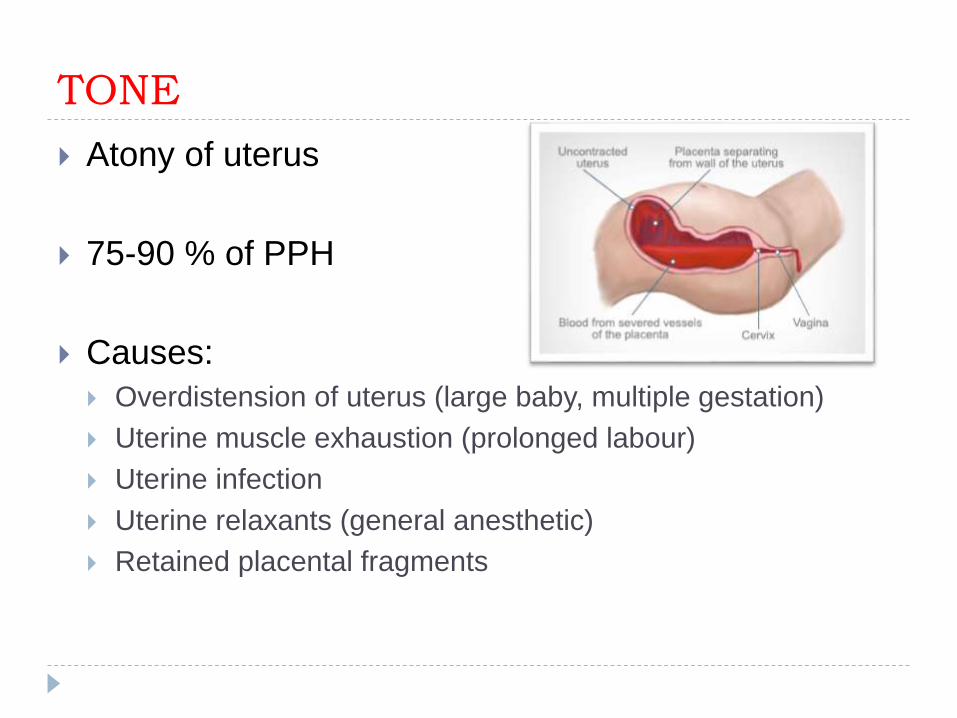
TONE
Atony of uterus
75-90 % of PPH
Causes:
Overdistension of uterus (large baby, multiple gestation)
Uterine muscle exhaustion (prolonged labour)
Uterine infection
Uterine relaxants (general anesthetic)
Retained placental fragments
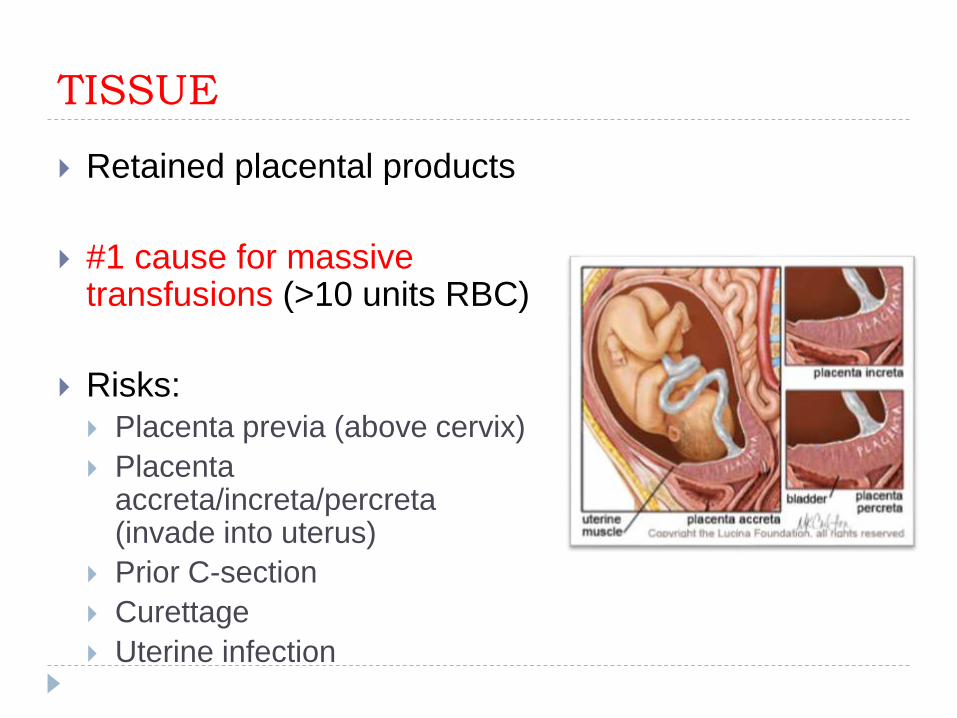
TISSUE
Retained placental products
#1 cause for massive transfusions (>10 units RBC)
Risks: Placenta previa (above cervix)
Placenta accreta/increta/percreta(invade into uterus)
Prior C-section
Curettage
Uterine infection
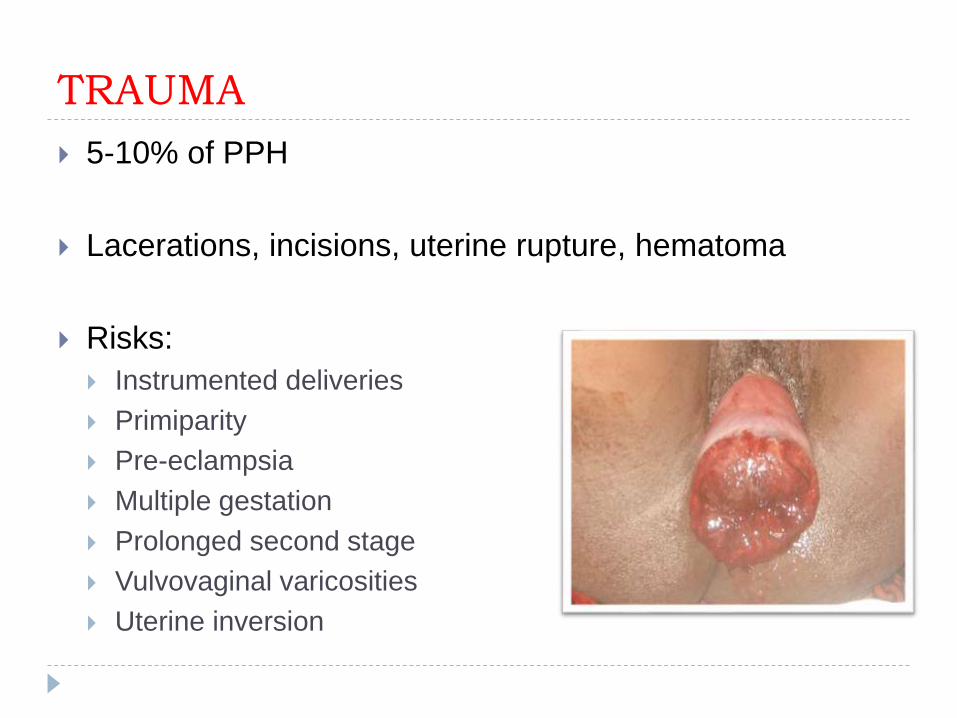
TRAUMA
5-10% of PPH
Lacerations, incisions, uterine rupture, hematoma
Risks:
Instrumented deliveries
Primiparity
Pre-eclampsia
Multiple gestation
Prolonged second stage
Vulvovaginal varicosities
Uterine inversion
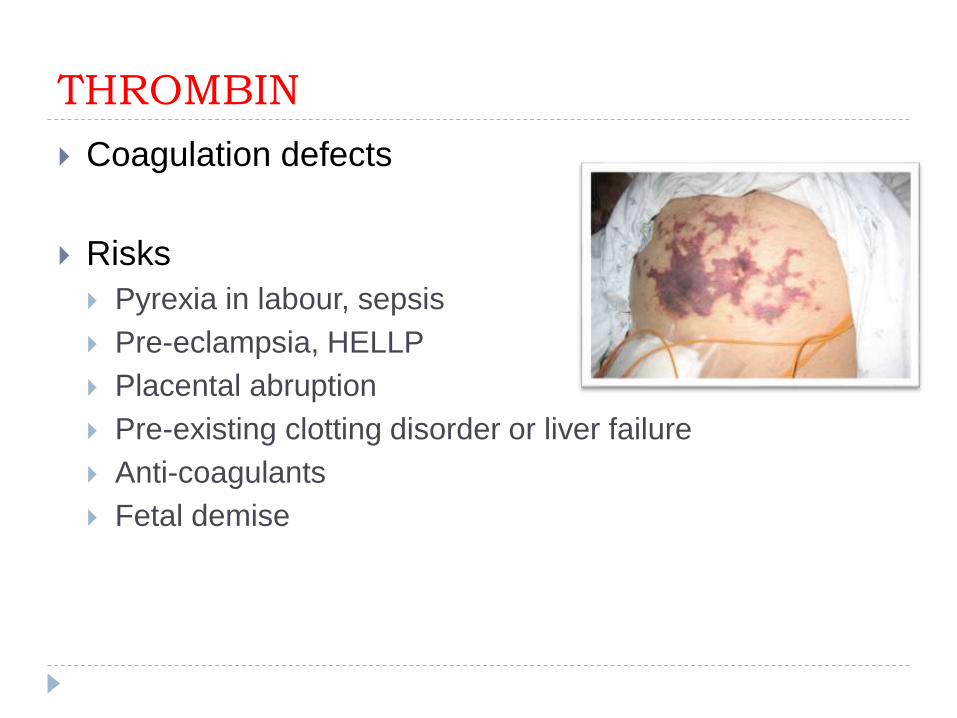
THROMBIN
Coagulation defects
Risks
Pyrexia in labour, sepsis
Pre-eclampsia, HELLP
Placental abruption
Pre-existing clotting disorder or liver failure
Anti-coagulants
Fetal demise
Review of some risks
Abnormal or retained placenta
Prolonged or precipitous labour
Lacerations or use of instruments
Distended uterus
Hypertensive disorders (Pre-eclampsia)
Induction of labour or oxytocin use
Previous PPH
Fetal demise
Coagulation disorders
….
Case - Mary
25 year old G1P0
Pregnancy complicated by pre-eclampsia
Labour has been prolonged (stage 1/2: >25 hours)
Serial blood work stable: Hb 120, normal CBC and lytes
Vitals stable, but blood pressure has been ~160/90
A Case - Mary
Resistant to assisted delivery, but eventually agrees to use of foreceps
Baby is delivered soon after with 2rd degree tear
Placenta delivered: appears intact with no missing or extra lobes
Bleeding estimated at 400 mL, with a slow trickle from tear
During suturing of her tear you note vitals deteriorating to HR 120, BP 90/60, pallor, feels dizzy
Management
Bedside evaluation, frequent vitals, ABCs
CBC, extended lytes, PT/PTT, screen and x-match
*Hb and Hct may not reflect acute changes
Reverse coagulopathies or electrolyte abnormalities
Active management of 3rd stage
Cord traction, uterine massage, remove retained products
Uterotonics: Oxytocin, carboprost, misoprostol
IV access & fluids, urine output, transfusion as needed
Blood products
Blood should be drawn q30-60 min to guide replacement (CBC, lytes, ionized calcium, PTT/INR)
No hard/fast rules: 2 units pRBC if hemodynamics do not improve after 2-3 liters of NS, EBL > 1500 mLs and continued bleeding expected
Typically FPP:pRBC = 1:2-3 (to stop dilutional coagulapathy)
Goals: HB >75
Platelets > 50 000
PTT and INR > 1.5 control
Fibrinogen > 200 mg/dL
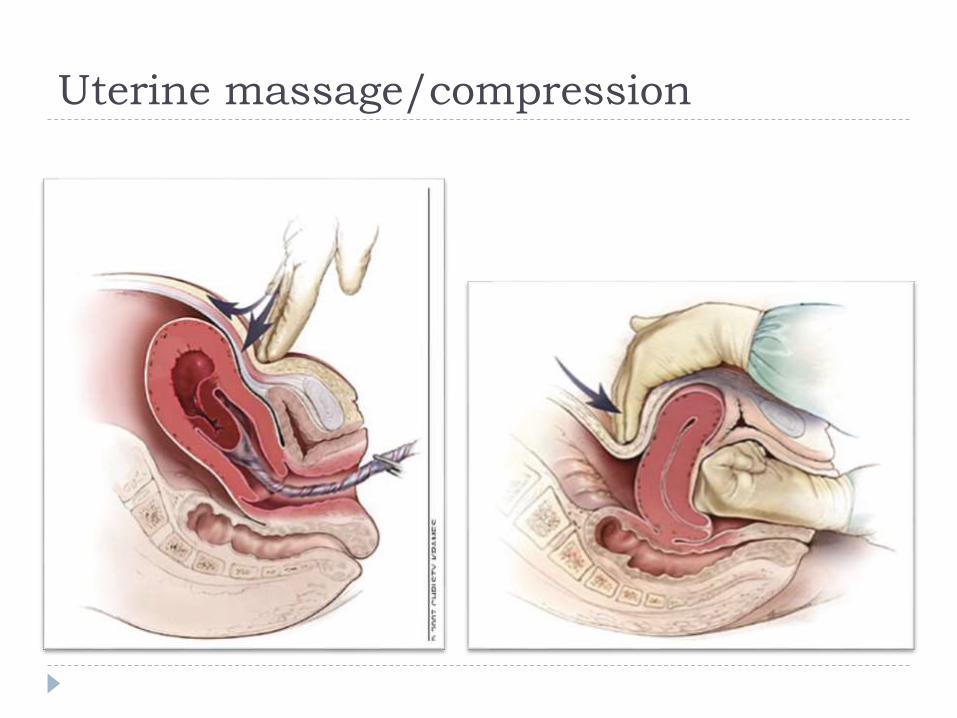
Uterine massage/compression
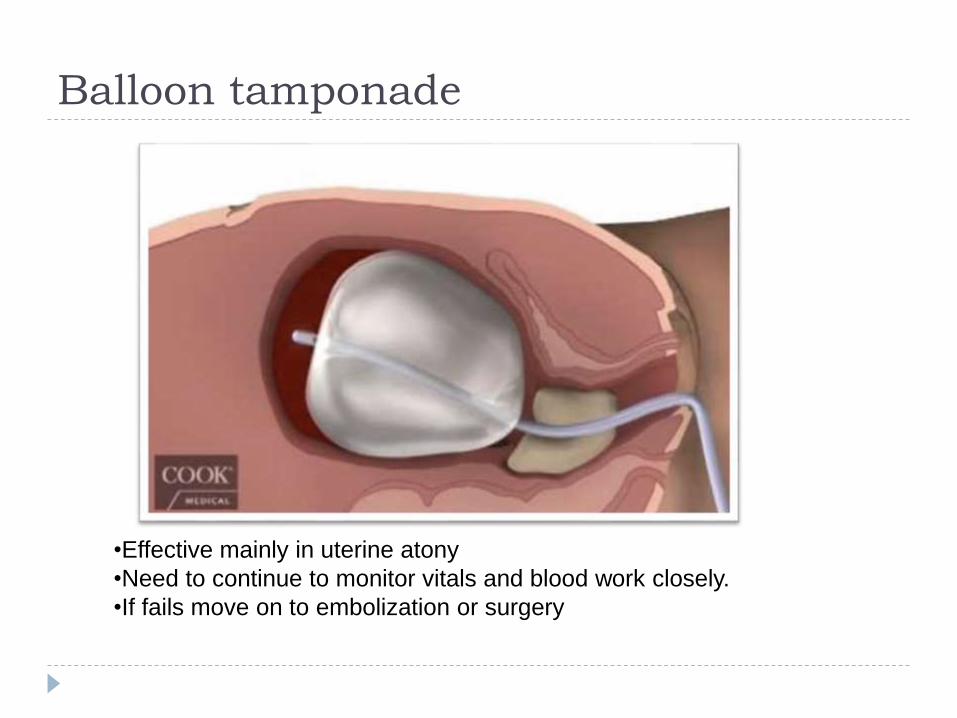
Balloon tamponade
•Effective mainly in uterine atony
•Need to continue to monitor vitals and blood work closely.
•If fails move on to embolization or surgery
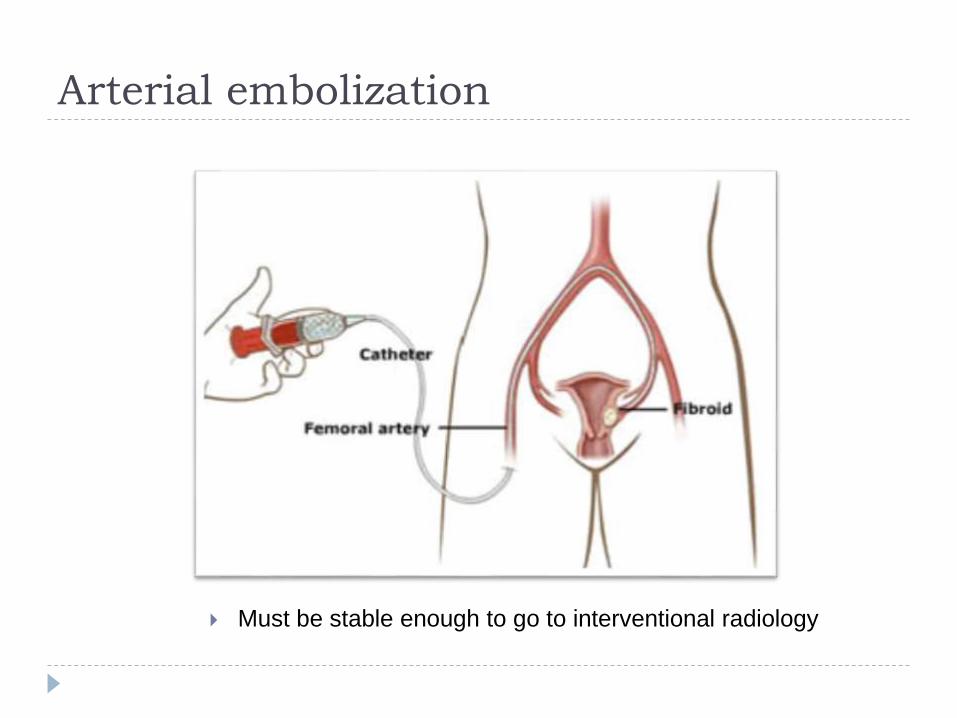
Arterial embolization
Must be stable enough to go to interventional radiology
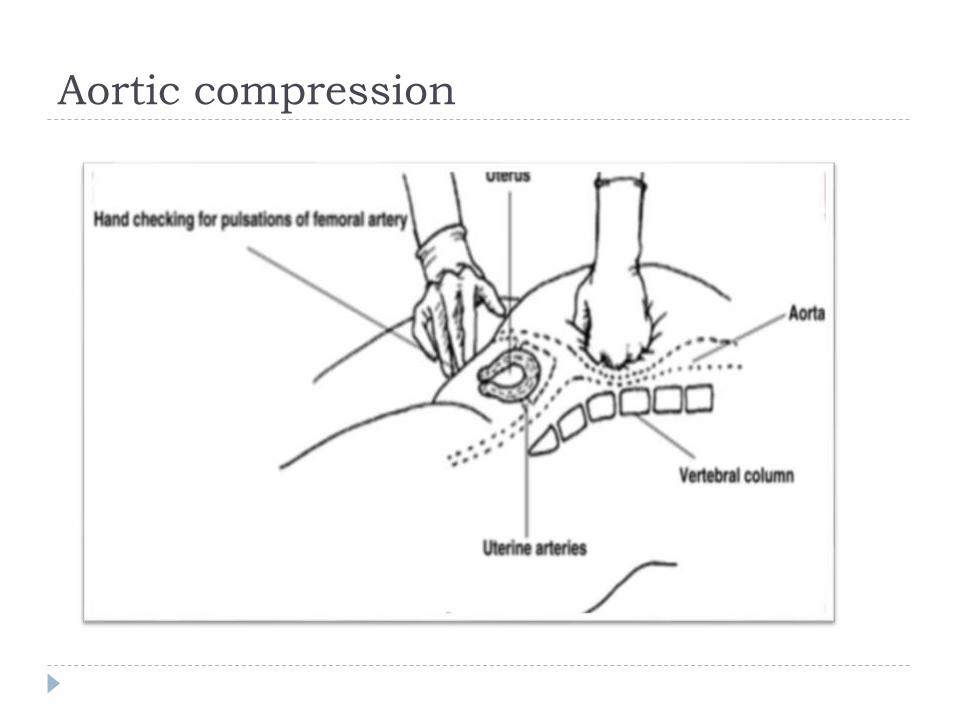
Aortic compression
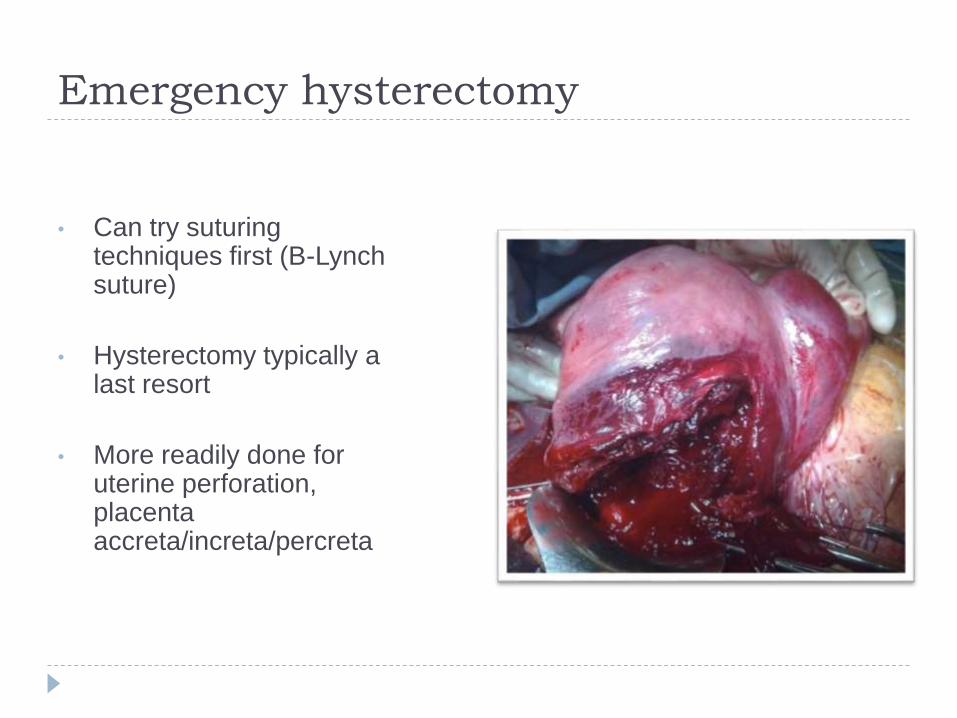
Emergency hysterectomy
• Can try suturing techniques first (B-Lynch suture)
• Hysterectomy typically a last resort
• More readily done for uterine perforation, placenta accreta/increta/percreta
Case - Mary
You suspect uterine atony so you give oxytocin (10
units IM) and call the team
Ask nurses to start 2 large bore IVs and fluids, blood
work, foley catheter, give oxygen
Uterine massage followed by compression
Uterus initially feels boggy but after ~1 minute
contracts causing a large gush of pooled blood to
exit the vagina (~800 mL)
Case - Mary
Vitals stabilize after 3 liters of NS and she is weaned off
O2
Vaginal tear repaired
Hb remains stable ~95-100, remaining bloodwork normal
Urine output stays above 40 ml/hr
Mary is closely monitored and recovers well over next
couple of days (her baby is healthy too!)





























