Embed Size (px)
Citation preview

Prapti Patel
Resident Lecture Series
2.4.15
PLATELET DISORDERS: ITP, TTP, HIT

IMMUNE THROMBOCYTOPENIC PURPURA

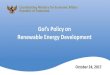
• Barnes-Jewish Hospital, 1950:
postulated that patients with ITP had a
“blood factor” that caused destruction
of platelets
• To test this hypothesis, Harrington
received a transfusion of 500 ml of
blood from a patient with ITP.[
• Within three hours, his platelets
dropped to dangerously low levels
• platelet count remained extremely
low for four days, finally returning
to normal levels by the fifth day
PATHOPHYSIOLOGY OF ITP: HARRINGTON-
HOLLINGSWORTH EXPERIMENT

PATHOPHYSIOLOGY OF ITP
• Platelets phagocytized Membrane GPIIb/IIIa or GPIb/IX digested into a peptide and
presented to macrophages CD4+ T cell is activated T cell secretes IL-6 activate
antibody producing B cells autoantibodies bind to platelets platelets are phagocytized
by splenic macrophages
• Antibodies can bind to megakaryocytes, thus decreasing overall platelet production

PATHOPHYSIOLOGY OF ITP: WHAT CAUSES IGG
PRODUCTION?
• Infections: anti-viral antibodies cross react with platelet glycoproteins
• CMV, EBV
• HIV: molecular mimicry of HIV proteins and GPIIb/IIIa
• Hep C: molecular mimicry between HCV core envelope protein 1 and GP IIb/IIIa
• Bacterial products (LPS) attach to platelet surface and increase phagocytosis
• Autoimmune disorders
• SLE, antiphospolipid syndrome, post-HSCT thrombocytopenia, sarcoidosis
• Lymphoproliferative disorders
• CLL
• Drug associated ITP
• Fludarabine

• Purpura
• NOT palpable and asymptomatic
• Mucosal bleeding
• Blood blisters
• Asymptomatic
ITP: A VARIABLE CLINICAL PRESENTATION

EPIDEMIOLOGY
• Observational study in Denmark from 1973 to 1995 and UK from 1990 to 2005
• Incidence 22-44 per million per year
• 70% are Women
• 70% are under age 40
• Typically chronic disease and asymptomatic, lasting for years
• Acute and symptomatic in children
• Death from bleeding is rare
• Death more likely related to immunosuppression

• Evaluate for systemic disease
• Coagulation studies
• DIC, TTP
• MAHA: heart valves
• Splenomegaly
• Splenic sequestration
• hematologic malignancy
• Other cytopenias
• Marrow failure: MDS
• Lypmhoproliferative or myeloproliferative disorders
• EDTA dependent platelet agglutination
• Pregnancy
• Drugs
• Heparin, quinine, sulfas,
antibiotics
• Viral infections
• HIV, EBV, rubella, CMV
• Autoimmune disorders
• SLE
• Congenital platelet disorder
DIAGNOSIS OF EXCLUSION
Must have isolated thrombocytopenia and no other signs of systemic disease

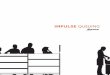
DIAGNOSIS BY PERIPHERAL BLOOD SMEAR

DIAGNOSIS BY PERIPHERAL BLOOD SMEAR
Schistocytes: TTP, DIC, HUS Clumping: EDTA

INDICATIONS TO TREAT
• Major bleeding is rare in ITP
• Mostly occurs at <10,000
• Goal of treatment:
• Reach a platelet count that will prevent bleeding
• Prevent toxicity of treatment itself
• When to treat
• Asymptomatic with moderate thrombocytopenia does not require treatment
• General cutoff: 30,000/µL
• Watch for worsening thrombocytopenia or new onset of symptoms

FIRST LINE TREATMENT: STEROIDS
• Prednisone 1 mg/kg/day
• 40-60% response rate with a response by 2 weeks
• Taper after initial response occurs, with most flares occurring during taper
• Goal oft therapy
• Keep plt’s at 50,000 or greater
• Minimize steroid induced side effects
• Give calcium and vitamin D
• Check DEXA scan

INTRAVENOUS IMMUNOGLOBULIN
• Quick, but temporary response
• Can be used in life threatening bleeding or preparing for splenectomy/surgery
• Helps to prevent platelet destruction after transfusion
• 2 forms
• IVIg: 1 g/kg for 1-2 days
• Anti-Rh(D) in Rh+ patients: 50-75 mcg/kg/day

• Mechansm is unknown
• Inhibit the autoantibody and cause steric hinderance so antibody can’t bind to platelets
• Inhibit the Fc receptor of the macrophages, decreaseinguptake of antibody coated platelets
• Clinical Data (Br J Haematol. 1999;107(4):716.)
• 1g/kg dose resulted in platelet count >80,000 in 28% of patients by day 2 and 67% by day 4 (N=35)
IVIG

FAILURE OF TREATMENT
• Failure to respond to high dose gluccocorticoids
• No response after 2 weeks of therapy
• Continued symptomtatic thrombocytopenia
• Failure to maintain response
• Case sereies of 208 patients with ITP:
• 39% complete response rate with prednisone
• Only 18% sustained complere response at 6 months
• Am J Med. 1995;98(5):436.

• Mechanism of action:
• Spleen is major site of platelet destruction
• Spleen is 25% of total lymphoid mass, which produced autoantibodies
• Response rates
• Usually occurs within 2 weeks of surgery
• Complete remission rate of 60-70%
• Durable remissions
• Partial remission rate of 15-20%
SPLENECTOMY FOR REFRACTORY ITP

• Prospective controlled phase II trial
(Blood. 2008;112(4):999.)
• 60 patients with ITP >6 months
and platelet count of <30,000
• Given rituximab 375 mg/m2 Q
week x 4
• 40% able to maintain a plt count of
>50,000 at one year
• 33% at two years
• No trial comparing rituximab to
splenectomy
RITUXIMAB FOR REFRACTORY ITP

THROMBOPOIETIN RECEPTOR AGONISTS FOR
REFRACTORY ITP

• 118 patients with plt<50,000 and failed
one prior therapy randomized to oral
eltrombopag vs placebo
• End point: plt count >50K by day 43
• Eltrombopag 75 mg: 81%, mean
platelet count 183,000
• Placebo: 11%, mean platelet counts
16,000
• Patients with ITP randomized (2:1) to romiplostim vs placebo
• ½ had a splenectomy
• Given SQ weekly therapy for 24 wks to maintain plt count b/w 50-200K
• Assessed durable plt response: Goal platelet count maintained for >6 weeks
• Splenectomized:38% vs 0% (p<0.0013)
• Nonsplenectomized: 56% vs 0% (p<0.0001)
THROMBOPOIETIN RECEPTOR AGONISTS VS
PLACEBO
Romiplostim: Lancet. 2008;371(9610):395. Eltrombopag: N EJM. 2007;357(22):2237.

THROMBOPOIETIN STIMULATING AGENTS
• FDA approved for ITP in adults with insufficient response to steroids, IVIG, or
splenectomy
• ASH 2011 guidelines: use in patients at risk for bleeding who have a contraindication to
splenectomy and have failed at least one other therapy other than steroids
• EMA: approved these agents for "splenectomized adults who are refractory to other
treatments."
• Expensive: one year of Romiplostim is >$55,000
• Long term effects not known
• Increase risk of clotting/bleeding?
• Increase bone marrow fibrosis?

EMERGENT TREATMENT OF ITP
• Platelet transfusion
• IVIG: 1g/kg for 1-2 days
• High dose IV steroids
• Methylprednisolone 1 gram or 30 mg/kg/day for 2-3 days

THROMBOTIC THROMBOCYTOPENIC
PURPURA

HISTORICAL PERSPECTIVE
• First described in 1924 by Eli Moshcowitz
• 16 year old girl that presented with fever, anemia leukocytosis, petechiae, hemiparesis
• Urine had albumin and granular casts
• Died 2 weeks later
• Autopsy showed hyaline thrombi in terminal arterioles, especially heart and kidney
• 1966: First clinical review
• 272 patients with TTP
• Classic pentad of: thrombocytopenia, hemolytic anemia, neurological symptoms, fever,
renal damage
• Mortality 90%
• No one was treated with plasma

HISTORICAL PERSPECTIVE OF TREATMENT
• Transfusion therapy not looked at until 1976
• 14 patients had whole blood transfusions
• 8/14 had clinical response
• Plasmapheresis
• Response if replacement fluid was plasma
• No response if replacement fluid was albumin
• Conclusion: There’s something in the plasma that can ameliorate TTP

PATHOGENESIS
• Link between TTP and vWF made in 1982
• Based on study of 4 patients
• Had much larger vWF multimers
• Proposed a defect in depolymerase activity that would normally cleave vWF
• Plasma exchange provides this missing depolymerase activity
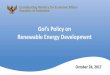
• 1996: metalloprotease in plasma shown to cleave vWF multimers
• Children with congenital TTP had a deficiency in this metalloprotease and adults with
acquired TTP had an antibody to it
• Metalloprotease was purified, cloned, and named ADAMTS13

STRUCTURE OF VWF



IDIOPATHIC TTP
• Polyclonal IgG autoantibody to ADAMTS13
• Associated with 30% relapse after initial remission
• Incidence 3.8 million a year in the US
• Peak incidence of idiopathic TTP is ages 30-50
• African ancestry
• Obesity
• Genetic predisposition

CLINICAL PRESENTATION-THE PENTAD
• Must haves:
• Hemolytic anemia
• Thrombocytopenia
• Purpura or petechiae
• Rarely bleeding
• Maybes: present in 50%
• Fever
• Renal failure
• Neurologic findings
• Headache
• Visual disturbances
• Vertigo
• Personality changes
• Confusion/lethargyComa
• Siezures
• Focal sensory or motor deficits/aphasia
• PRES

• Thrombocytopenia
-50% of patients have platelets <20,000
• Evidence of hemolysis
• 33% of patients have Hgb <6
• Schistocytes : >5 per high powered field
• Elevated retic count
• Evidence of tissue ischemia
• Elevated LDH: median LDH is 1200
• Ruled out AIHA, DIC
LABORATORY PRESENTATION
ADAMTS13 activity level is NOT a criteria

ADAMTS13 TESTING AS A DIAGNOSTIC TOOL
• ADAMTS13 activity correlates with clinical presentation, but not clinical course
• Study of 48 patients with clinical diagnosis TTP-HUS
• 16 had severe ADAMTS 13 deficiency
• Clinical course was variable and no different than other 32 patients
• Assay techniques are not standardized
• Levels vary with pregnancy, age, cirrhosis, CKD, postoperative course, acute
inflammatory states, sepsis, acute hepatitis, VOD after HSCT
• Activity level <5% is consistent with TTP
• Only 5% needed to maintain homeostasis

SECONDARY THROMBOTIC
MICROANGIOPATHY (TMA)
• Infection and DIC
• Malignancy
• Postop
• Malignant Hypertension
• Bone Marrow Transplant Patients
• Allografts
• Total body irradiation
• GVHD
• Autoimmune disorders
• Lupus vasculitis (TMA)
• Antiphospholipid Sx (TMA)
• Evans Sx
• Pregnancy
• HELLP (TMA)
• Eclampsia (TMA)
Not associated with ADAMTS13
deficiency
Can be associated with ADAMTS13
deficiency

DRUGS AS A CAUSE OF TMA
• Quinine
• Chemotherapy
• Mitomycin C
• Bleomycin
• Gencitabine
• Cisplatin
• Immunosuppression
• Cyclosporine
• Tacrolimus
• Ticlopidine
• Clopidogrel
• Treat like TTP with plasma exchange
• No relapse reported after stopping drug
Associated without ADAMTS13 antibody Associated with ADAMTS13 antibody

TREATMENT
• Plasma infusion (FFP): giving back
ADAMTS13
• More effective in congenital TTP
• Temporizing measure in acquired
TTP
• Plasma exchange: giving ADAMTS13 and
removing antibody and large vWF
multimers
• Exchange of single plasma volume
• Larger volume exchanges may have
benefit

TREATMENT: CRYO-POOR PLASMA
• Results from removal of cryoprecipitate from plasma
• Depleted in factor VIII, vWF, factor XIII, fibrinogen
• Can be used in patients with volume issues
• Still has ADAMTS13
• RCT of 27 patients comparing CPP and FFP demonstrated equivalence
• Time to response: 5.5 vs 6.0 days
• Survival: 79% vs 77%

TREATMENT: PLASMA EXCHANGE
• Continue daily until following is met for 3 days:
• Platelet count >150K
• LDH normal
• Resolution of neurologic symptoms
• Resolution of renal disease may be slow and incomplete
• Then taper to QOD to twice a week
• Average time on daily exchange: 7-16 days
• Time on exchange (including taper) is variable
• 3 to 145 exchanges

TREATMENT: STEROIDS
• Rationale: need to eliminate antibody production
• Benefit not clearly demonstrated
• Common practice: 1 to 2 mg/kg/day during plasma exchange then taper
• Alternative: methylprednisolone 1 gram IV daily for 3 days or 125 mg IV BID for 4 days
• Or can be started if plasma exchange cannot be tapered

RESISTANT OR RELAPSING DISEASE
• 10-20% of patients will have transient, incomplete, or no response to exchange
• Can increase the frequency of exchange or:
• Steroids
• Rituximab
• Cyclosporine
• Cyclophosphamide

PLATELET TRANSFUSION IN TTP
• Can correlate with acute decompensation and worsening thrombosis
• Retrospective study: 89 pts received platelet transfusions in setting of TTP
• 8% had new neurological event or death
• Study from TTP registry in Oklahoma reviewed course of 54 patients
• No difference in neurological events or death
• Party line on platelet transfusions:
• Do not need to transfuse platelets for procedures
• Can transfuse platelets prior to emergency surgery after plasma exchange

HEPARIN INDUCED THROMBOCYTOPENIA
(HIT)

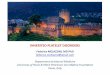
COAGULATION CASCADE AND MECHANISM OF
ACTION OF HEPARIN

PATHOPHYSIOLOGY OF HIT
• Heparin causes thrombocytopenia: results in HIT
• Type I: non-immune mediated
• Platelet count falls 2 days after starting heparin and resumes to normal despite
continued heparin use
• Due to increased platelet activation
• Type II: immune mediated
• Due to formation of antibodies against heparin-platelet factor 4 complex

TYPE I VS TYPE II
Type I Type II
Frequency 10-20% 1-3%
Timing of onset after starting
heparin
1-4 days 5-10 days
Nadir platelet count >100,000 >20,000
Antibody mediated No Yes
Thromboembolic sequelae None 30-80%
Hemorrhagic sequelae None Rare
Management observe Stop heparin and start non-
heparin anticoagulant to
prevent arterial thromboses
Brieger, DB, Mak, KH, Kohke-Marchant, K, et al. J Am
Coll Cardiol 1998; 31:1449.

• Heparin and platelet factor 4 forms a
highly immunogenic complex
• PF4 is a heparin neutralizing
protein contained in alpha
granules of platelets
• Heparin induces a conformational
change in PF4, inducing a new
epitope
• Induces an antibody reaction
• IgG, IgM, IgA is formed
TYPE II IMMUNE MEDIATED HIT

• Once PF4-heparing complex forms, it binds to platelet surface
• HIT ab (usually IgG) binds to the surface/complex
• Fc portion of the antibody activates adjacent platelets, leading
• 1. platelet activation and release of additional PF4 and procoagulantmicroparticles
• 2. aggregated platelets, leading to increased removal by RES
TYPE II IMMUNE MEDIATED HIT

EPIDEMIOLOGY AND RISK FACTORS
• Seen in ~5% of patients treated with heparin
• Risk factors for developing HIT (Blood. 2006;108(9):2937.)
• Unfractionated heparin vs LMWH (RR 5.3; 95% CI 2.8-9.9)
• Surgical patients vs medical patients (RR 3.2; 95% CI 2.0-5.4)
• Female patients (RR 2.4; 95% CI 1.4-4.1)
• Female surgical patients receiving UFH (RR 17; 95% CI 4.2-72)

• Platelets decreased 30-50% from baseline during first 72 hours of bypass surgery
• due in part to prolonged contact of platelets with the artificial surface of the extracorporeal circuit
• usually receive large amounts of unfractionated heparin
• incidence of HIT antibodies is as high as 25 to 70 percent by immunoassay and 4 to 20 percent by platelet activation assay.
• several other potential causes of thrombocytopenia are often present
CARDIAC SURGERY

CLINICAL PRESENTATION
• Fall in platelet count >50% of baseline within 5-10 days of initiating heparin
• It takes 5-10 days to produce IgG
• Earlier onset can be seen be seen in prior exposure (due to preformed antibodies)
• No other cause of thrombocytopenia
• Platelet counts usually <20,000, median platelet count 60,000
• Bleeding is unusual
• Venous and Arterial Thrombosis (platelet rich)
• Due to activated platelets
• Most common: PE, limb gangrene, cerebral sinus thrombosis, DVT
• Less common: MI, CVA, organ infarction
• Skin necrosis
• Adrenal hemorrhage

• 0-3: low probablity of HIT (0.9%)
• 4-5: intermediate probability (11.4%)
• 6-8: high probability (34%)
CLINICAL DIAGNOSIS: 4T SCORE
2 points 1 point 0 point
Thrombocytopenia >50% fall and nadir ≥20k
30-50% fall, or nadir 10-19k;
or >50% fall directly resulting
from surgery
<30% fall,
or nadir <10k
Timingb of Platelet Count Fall
Clear onset between days 5-
14;
or ≤1 day (prior heparin
exposure within 30 days)
Consistent with day 5-14 fall, but
not clear (e.g. missing plt
counts);
or onset after day 14;
or ≤1 day (prior heparin
exposure 30-100 days ago)
Platelet count fall ≤4 days
without recent exposure
Thrombosis or other sequelae
New thrombosis (confirmed);
skin necrosis; acute systemic
reaction after iv UFH bolus
Progressive or recurrent
thrombosis; non-necrotizing
(erythematous) skin lesions;
suspected thrombosis (not
proven)
None
Other causes of
thrombocytopeniaNone apparent Possible Definite

• Heparin-PF4 complexes are coated on plate
• Patient serum is added
• If heparin IgG antibody is present, will bind to complex
• Alkaline phosphatase-labeled anti-human globulin added to detect the
IgG causing agglutination
• The optical density (OD) is reported: OD values >0.40 are considered
positive and indicate the presence of heparin-induced antibodies.
• OD: measure of penetrance of light
• Sensitivity: 91-97%, negative test rules out HIT
• Specificity: 74-86%, (hemodialysis patients, cross reactivity of other
antibodies or non-IgG HIT Ab)
LABORATORY DIAGNOSIS: ELIZA TEST

LABORATORY DIAGNOSIS: SEROTONIN RELEASE
ASSAY
• Gold standard for HIT diagnosis
• Platelets from normal donor are radiolabeled with 14C serotonin
• Patient serum added with heparin
• If HIT ab is present bind to heparinactivate plateletsgranules are emptied
• Positive test: 14C serotonin is released
• Sensitivity: >95%
• Specificity: 97%
• Not available in all centers

TREATMENT
• First step: stop heparin and LMWH
• Start anticoagulation with direct thrombin inhibitors to treat existing thromboses and
prevent new ones
• Lepirudin/Bivalirudin: renally cleared
• Argatroban: hepatically cleared

• 2 mg/kg/hr CIVI
• 3 trials let to FDA approval
• Arch Intern Med. 2003;163(15):
1849
• Circulation. 2001;103(14):1838.
• Chest. 2006;129(6):1407.
• Reduction in thrombotic events
• 0.1 to 0.15 mg/kg/hour CIVI
• Prospective series of 82 patients: 89%
of patients has increase in platelet
counts (Circulation. 1999;99(1):73.)
• Retrospective series of 205 patinets:
less death, amputation, new
thromboses than historical control,
25% vs 52% (J Thromb Haemost.
2005;3(11):2428.)
TREATMENT
Lepirudin Argatroban

LONG TERM THERAPY
• Transition to long term therapy once platelets return to normal (>150,000) with direct
thrombin inhibitors
• Warfarin
• Both DTI and warfarin increase INR
• Goal INR is 2-3
• 5 days of overlapping therapy with warfarin and DTI before DTI is discontinued
• Avoid induction of hypercoagulable state by lowering of protein C levels
• No firm data on length of therapy
• 3 months if no thrombosis
• 6 months if thrombosis was present

THE END