Embed Size (px)
Citation preview


OUTLINE-Definition.
-Classification
-Clinical features & histopathology
-Pocket composition
-Pathogenesis
-Pocket as a healing lesion
-Periodontal pocket detection
-Management

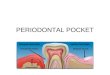
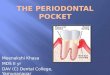
Definition
• Periodontal pocket is defined as pathologic deepening of the gingival sulcus

1)Gingival pocket2)Periodontal pocket
Classified according to :a) The relation to the crestal boneb) The number of surfaces involved

• Gingival pocket
(pseudo pocket): gingival enlargement without destruction of the underlying periodontal tissues
• Periodontal pocket:This type of pocket occurs with destruction of the supporting periodontal tissues

1. According to the relation to the crestal bone
Suprabonysupracrestal/supraalveolar
Intrabonysubcrestal/
intraalveolar

Suprabony pocket
1.Base of pocket is coronal to the level of alveolar bone.2.Horizontal pattern of bone destruction.3. pdl fibers beneath pocket follow their normalHorizontal- oblique course.4.Transeptal fibers are arranged horizontally.
Infrabony pocket
1.Base of pocket is apical to crest of alveolar bone , intrabony pockets most often occur interproximallybut may be located on the facial or the lingual tooth surfaces.
2.Vertical (angular) pattern of bone destruction.3.Pdl fibers follow angular pattern. 4. Transeptal fibers are arranged obliquely.

2. According to the number of surfaces involved
Simple: Pocket involving one tooth surface
Compound: Pockets involving more than one tooth surface
Complex: (spiral ) originating on one tooth surface and
twisting around the tooth to involve one or more additional surfacesThis type of pockets is most common in furcation areas


SymptomsLocalized Pain and sometimes radiating
deep into bone.
Sensitivity to hot and cold
Food impaction
Foul taste in localized areas

CLINICAL FEATURES
1.Various degrees of bluish red discoloration.-Flaccidity.-Smooth shiny surface.-Pitting on pressure.
2.Gingival wall may be pink and firm.3.Bleeding on probing.
4.On probing inner aspect of wall is generally painful.5.Pus may be expressed on applying digital pressure.
HISTOPATHOLOGIC FEATURES
1.Circulatory stagnation.-Destruction of gingival fibers.-Atrophy of epithelium.-Edema
2.Fibrotic changes .3.Increased vascularity, thinning and degeneration of epithelium.
4.Ulceration of inner aspect of pocket wall.5.Suppuratiove inflammation of inner wall.


1)Soft tissue wall 2)Hard tissue wall3) pocket content

First : pocket content1. Microorganisms and their products (enzymes, endotoxins,
and other metabolic products),
2. Gingival fluid
3. Food remnants
4. Salivary mucin
5. Desquamated epithelial cells, and leukocytes.
6. Plaque-covered calculus usually projects from the tooth surface
7. Purulent exudate

Significance of Pus formation
Pus is a common feature of periodontal disease, but it is only a SECONDARY
SIGN
It is NOT AN INDICATION OF THE DEPTH of the pocket or the severity of
the destruction of the supporting tissues

Second: soft tissue wallInflammatory changes in the connective tissue wall :
= Destruction of collagen fibers just apical to the junction epithelium , as this area becomes occupied by inflammatorycells and edema
=As a consequence of the loss of collagen, the apical cells of the junctional epithelium proliferate along the root, extending fingerlike projection two or three cells in thickness
= PMNLs invade the coronal end of the junctional epitheliumWhen the volume of PMNLs reach 60% of the junctionalepithelium, the tissues looses cohesiveness and detach from the tooth structure

Collagen loss is caused by 2 mecahnisms
PMNLs and macrophages secrete collagenase and other lysosymesextracelluaraly and destroy collagen fibers in gingival CT(matrix metalloproteinases)
Fibroblast phagocytize fibers by extending cytoplasmic process to the ligament cementum interface and degrade the collagen fibers in the cementummatrix

Collagen loss is followed by Degeneration of the junctional epithelium and
pocket formation
• The coronal portion of the junctional epithelium detaches from the root as the apical portions migrates
• The apical cellsof the junctional epithelium proliferate along the root extending fingerlike projections

Migration of the junctionalepithelium requires healthy, viable
cells
Therefore, marked degeneration or necrosis of the junctional
epithelium retards rather than
accelerates pocket formation

Third : Root surface wall• Collagen fibers embedded in the cementum
(Sharpey’s Fibers) are destroyed
• Cementum becomes exposed to the oral cavity
• Bacterial penetration in to cementum leads to breakdown of the cementum surface and necroticcementum results that will be separated from tooth by masses of bacteria.

• In the course of treatment, these necrotic areas are removed by root planinguntil a hard smooth surface is reached.
• Cementum is very thin in the cervical areas, and scaling and root planingoften removes it entirely, exposing the underlying dentin.
• Sensitivity to cold may result until secondary dentin is formed by the pulp tissue

Surface Morphology of Pocket WallsFive zones can be seen
the base of the pocket
1. Cementum covered by calculus.
2. Attached plaque
3. Zone of unattached plaque.
4. Zone where the junction epithelium is attached to the tooth.
5. The zone of semi destroyed C.T. fibers.
(3, 4, 5 called plaque free zone)


-The initial lesion in the development of periodontitis is the inflammation of the gingiva in response to a bacterialchallenge.
-Changes involved in the transition from the normal
gingival sulcus to the pathologic periodontal pocket
are associated with different proportions of bacterial cells
in dental plaque.
-Healthy gingiva is associated with few microorganisms, mostly coccoid cells and straight rods.
While Diseased gingiva is associated with increased numbers of spirochetes and motile rods

Early concepts :
assumed that after the initial bacterial attack, periodontal tissue destruction continued to be linked to bacterial action.
More recently:
it was established that the host’s immunoinflammatory response to the initial and persistent bacterial attack unleashes mechanisms that lead to collagen and bone destruction.

Genetics and Interventional studies implicating complement
C3 as a major target for the treatment of periodontitis
J Immunol. 2014 Jun 15;192(12):6020-7. doi: 10.4049/jimmunol.1400569. Epub 2014 May 7.

Chronic periodontitis leads to inflammatory destruction of tooth-supporting tissues
C3 complement is a point of convergence of complement activation mechanisms,
but its involvement in periodontitis was not previously addressed.

We investigated this question using two animal species models, namely, * C3-deficient or wild-type mice
with the local application of C3 complement
In mice, C3 was required for maximal periodontal inflammationand bone loss.
* nonhuman primates (NHPs)
locally treated with a potent C3 inhibitor.
local treatment of NHPs with C3 inhibitor inhibited ligature-induced periodontal inflammation and bone loss, together with lower gingival crevicular fluid levels of proinflammatorymediators (e.g., IL-17 and RANKL) as compared with control treatment.

ConclusionThis is the first time to prove that:
complement inhibition inhibit inflammatory processes that lead to bone loss.
These data strongly support the feasibility of
C3-targeted intervention for the treatment of human periodontitis.

Overexpression and Potential Regulatory Role of IL-17F in
Pathogenesis of Chronic Periodontitis.
Inflammation 2014 Nov 11. Epub 2014 Nov 11Zhenhua Luo, Hui Wang, Jiajun Chen, Jian Kang, Zheng Sun, Yafei
Wu

1) Periodontal local tissues were obtained from chronic periodontitis (CP) and healthy controls (HC) for real-time PCR (RT-PCR) detection with IL-17F and IL-17A messenger RNA (mRNA).
2) Primary human gingival fibroblasts (HGF) were derived from patients receiving crown-lengthening procedures.
Elevated levels of IL-17F and IL-17A mRNA in CP gingival tissues compared with HC group .
There is a correlation between IL-17F and IL-17A mRNA in CP group with the probing depth

3) IL-17F and IL-17A were used to stimulate the HGF cells.
4) Production of pro-inflammatory cytokines induced by IL-17F and IL-17A was detected by RT-PCR.
Both IL-17F and IL-17A could promote the inflammatory cytokines IL-6, CXCL8, and CCL20 production
This study indicates that IL-17F may be involved in pathogenesis of periodontitis like IL-17A.
The role of IL-17F in disease pathogenesis needs to be further investigated

PERIODONTALDISEASE ACTIVITY

Periodontal pockets go through periods of exacerbation and quiescence
Periods o f quiescence
• Reduced inflammatory response
• little or no loss of bone and connective tissue attachment
Period o f exacerbation
• Bone and connective tissue attachment are lost and the pocket deepens
• Bleeding, either spontaneously or with probing
• Greater amounts of gingival exudate


Periodontal pockets constantly undergoing repair.
Complete healing does not occur because of the persistence of the local irritants.

The condition of the soft tissue wall of the periodontal pocket result from the
destructive & constructive tissue changes.
The balance between the destructive & constructive changes determines the
clinical features ;(color ,consistency ,surface texture of the
pocket wall.)

Thus pocket wall can be eitherSoft & friable pocket wall
Fibrotic pocket wall


Probing depth: It ‘s the distance between the point of resistance under light pressure at the base of the pocket and the crest of the gingival margin
Attachment loss:It ‘s the distance between the point of resistance under light pressure at the base of the pocket and the cementoenamel junction

Severity of bone loss is generally, but not always, correlated with pocket depth
Extensive attachment loss & bone loss may be accompanied with shallow pockets in case of
gingival recession
And slight bone loss can occur with deep pockets

Pocket ProbingThe two different pocket depths
are:
Biologic or histologic depth
Clinical or probing depth

Biological Depth -Vs -Clinical Depth• The distance between the
gingival margin and the base of the pocket can be measured only in carefully prepared histologic
sections.
The distance to which the probe penetrates into the
pocket clinically
clinical depth
Histological depth


DETECTION OF POCKETS

The only accurate method of detecting and measuring periodontal pockets is careful exploration with a
periodontal probe

Limitations of radiograph• The periodontal pocket is a soft tissue change.
• Radiographs indicate areas of bone loss where pockets may be suspected
• They do not show pocket presence or depth, and consequently they show no difference before or after pocket elimination unless bone has been modified.

Gutta Percha points or
Calibrated Silver points can
be used with radiograph to
assist in determining the level
of attachment of periodontal
pocket.


Management of periodontal pockets include
I) Non surgical management ; Including:
a) phase I therapy
b) local drug delivery
c) systemic antimicrobials
II) Surgical management ; including :
a) resective surgeries
- gingival currettage
- gingivectomy
- flap operation
b) regenerative surgeries.

Randomized Controlled Trial AssessingEfficacy and Safety of Glycine Powder
Air Polishing in Moderate-to-DeepPeriodontal Pockets
This study assesses efficacy and safety of subgingivally applied glycine powder air polishing
(SubGPAP) in moderate-to-deep periodontal pockets
Thomas F. Flemmig,* Daniyel Arushanov,* Diane Daubert,* Marilynn Rothen,†
Gregory Mueller,†and Brian G. Leroux Submitted June 21, 2011.

Subgingival debridement was performed in deep periodontal pockets by SubGPAPusing a thin nozzle inserted into the periodontal pocket (A)
in shallow periodontal sites by SupraGPAP using a conventional hand piece aimed directly into the periodontal pocket (B).
Supragingival biofilm and stain were removed in all sites by SupraGPAP directed perpendicular to the tooth surface (C).

SubGPAP resulted in significantly lower total viable bacterial counts (as it is more efficacious in removing
subgingival biofilm) in moderate-to-deep pockets when compared to SRP .
full-mouth GPAP may result in a beneficial shift of the oral microbiota and appears to be well tolerated
There were no adverse events related to full-mouthGPAP.

Effect of tetracycline HCl in the treatment of chronic periodontitis - A clinical
study.
Sinha S1, Kumar S2, Dagli N3, Dagli RJ4.
J Int Soc Prev Community Dent. 2014 Sep;4(3)

This study was aimed to evaluate the efficacy of the adjunctive use of tetracycline fibers (Periodontal Plus AB(®)) as a local drug delivery with scaling and root planing,
as compared with the results of one episode of scaling and root planing for the treatment of chronic periodontitis.

RESULTS:
Significant improvement was found in all the variables, including reduction in p.d and gain in C.A.L, in both test and control groups in 3 months
But Mean reduction in P.D and gain in C.A.L were more in test than in control group.
CONCLUSION:
Tetracycline fiber therapy along with scaling and root planing improves the healing outcome, namely, reduction in pocket depth and gain in clinical attachment level, when compared to scaling and root planing alone.

In the treatment of periodontal infectionsThe local application of antibiotics in periodontal pockets
may be a promising approach to achieve sustained/controlled drug release, high antimicrobial
activity and low systemic side effects.
the effectiveness of conventional nonsurgical treatment is limited by lack of accessibility to bacteria in deeper periodontal pockets.
Development of local drug delivery systems provides an answer.

Novel local drug delivery agents used for the treatment of periodontal diseases are alendronate and simvastatin delivered as gels.
Alendronate is a novel bisphosphonate is a very potent inhibitor of bone resorption.
The net effect of alendronate on bone formation might be explained by its inhibition of osteoclasts, thus affecting bone maturation and remodeling.

Once taken up by bone, alendronate has a prolonged skeletal retention (half-life up to several years)
Alendronate gel has been found to increase bone formation on local delivery into the periodontal pocket.
In patients with type 2 diabetes mellitus and chronic periodontitis, local delivery of 1% alendronate gel into periodontal pockets resulted in:
a significant increase in the probing depth (p.d)reduction, clinical attachment level (A.L)gain, and improved bone fill compared to placebo gel as an adjunct to scaling and root planning
.Pradeep AR, Sharma A, Rao NS, BajajP, Naik SB, Kumari M. Local drug delivery of alendronate
gel for the treatment of patients with chronic periodontitis J Periodontol. 2012.

Simvastatin (SMV) is a specific competitive inhibitorof 3-hydroxy-2-methyl-glutaryl coenzyme-A reductase.
Pardeep et al [35] showed :
a greater decrease in gingival index and probing depth and a clinical attachment level gain at sites treated with scaling and root planing plus locally delivered SMV gel in patients with chronic periodontitis.
Pradeep AR, Thorat MS. Clinical effect of subgingivally delivered simvastatin in the treatment of patients with chronic periodontitis: a randomized clinical trial. JPeriodontol.
2010

Impact of Local and SystemicAlendronate on Simvastatin-Induced
New Bone Around Periodontal Defects
Amy C. Killeen,* Pota A. Rakes,* Marian J. Schmid,† Yijia Zhang,‡ Nagamani Narayana,†
David B. Marx,§ Jeffrey B. Payne,* Dong Wang,‡ and Richard A. Reinhardt*
December 2012

Simvastatin has been shown to stimulate new
bone growth on rat mandibles, but much of the bone is lost over time
The purpose of this study:
is to evaluate the impactof a systemically applied anti resorptive agent (alendronate) on simvastatin-induced bone formation
Conclusion: The use of a short course of systemic ALN during the healing period after bone anabolic SIM injections has the potential to enhance local bone augmentation.

Boric acid irrigation as an adjunct to mechanical periodontal therapy
in patients with chronic periodontitis: a randomized clinical
trial
Sağlam M1, Arslan U, Buket Bozkurt Ş, Hakki SSJ Periodontol. 2013 Sep;84(9):1297-308. doi:
10.1902/jop.2012.120467. Epub 2012 Nov 3.

The purpose of this clinical trial was to evaluate the effects of boric acid irrigation as an adjunct to SRP on clinical and microbiologic parameters and compare this method with chlorhexidine irrigation and SRP alone in patients with
chronic periodontitis (CP)
boric acid could be an alternative to chlorhexidine, and it might be more favorable because boric acid
was superior in whole-mouth BOP as well as PD and CAL reduction for moderate pockets.

Photo disinfection of Periodontal Pockets
Written by Véronique Benhamou, BSc, DDSMarch 2009

Photodisinfection of PeriodontalPockets
• Methylene blue dye is gently injected into the periodontal pocket
The dye binds to the Peptidoglycan layer on the cell walls of both gram-negative and gram-positive bacteria

Because of a difference in
thickness of the peptidoglycan layer in
their cell walls,GRAM-NEGATIVE
Bacteria take up the methylene blue stain
FASTER.

• Meanwhile, the Periowave nonthermal diode laserproduces photons whose frequency matches that of the molecule of the methylene blue dye.
• When the photons hit the dye molecules, they initiate the photodynamic chain of events.
• The oxygen molecules surrounding the dye are caused to lose an electron, and thus become free radicals.
• The free oxygen radicals are toxic to the bacterial cell walls and disrupt them, leading to the destruction of the bacteria.

Photodisinfection treatment is notmeant to replace traditional
mechanical SRP therapy but rather to complement it.
Photodisinfection may also be used during periodontal surgery to “disinfect” areas that
may be difficult to instrument (such as furcations), particularly prior to regenerative
procedures

Gingival Pocket (pseudopocket) Management
Treatment of pockets includes:
PHASE 1 THERAPY
then surgical removal of gingiva is done
(Gingivectomy)

Periodontal Pocket Management I)Suprabony Pocket
• Phase 1Therapy
• Maintenance
• Flap surgery

Flap Surgery

Infrabony Pocket

The use of a membrane: 1) maintaining space for clot stabilization.
2) Is for the prevention of epithelial migration along the cemental wall of the pocket thus temporarily separating them from the gingival epithelium and connective tissue
Excluding the epithelium and the gingival connective
tissue from the root surface during the postsurgical healing phase not only prevents epithelial migration into the wound but also favors repopulation of the area by cells from the periodontal ligament and the bone

Bone graft materials are evaluated based on their osteogenic,
osteoinductive, or osteoconductive potential.Osteogenesisrefers to the formation of new bone by cells contained in the graft.Osteoinductionis a chemical process by which molecules contained in the graft (e.g., bone morphogenetic proteins) convert the neighboring cells into osteoblasts, which in turnform bone. Osteoconductionis a physical effect by which the matrix of the graft forms a scaffold that favors outside cells to penetratethe graft and form new bone

Clinical Effectiveness of Diode Laser Therapy as an Adjunct to Non-Surgical Periodontal Treatment: A Randomized
Clinical Study -August 2013
The use of 980 nm diode laser in adjunct to scallingand root planning in comparison to scaling and root
planning only

Laser therapy showed improvement only in probing depth in moderate pockets ( 4-6 mm) while no difference
in Bleeding on probing nor Clinical attachment loss
For patients with aggressive periodontitis the adjunct use of diode laser with scaling and root planing ( SRP)
has shown superior effect over SRP alone

Morphological Alterations of Periodontal Pocket Epithelium
Following Nd:YAG Laser Irradiation
Ting Chun-Chan, Fukuda Mitsuo, Watanabe Tomohisa, Sanaoka Atsushi, Mitani Akio, and Noguchi Toshihide. Photomedicine and Laser Surgery.
November 13, 2014

Conclusion
The scanning electron microscopy and histologic
findings demonstrated the feasibility & effectivity of ablating pocket epithelium with an Nd:YAG laser
irradiation

Effects of citric acid and EDTA conditioning on exposed root dentin: An immunohistochemical analysis of
collagen and proteoglycans
Alessandra Ruggeri Jr.a, Carlo Pratib, Annalisa Mazzonia, Cesare Nuccib, Roberto Di Lenardac, Giovanni Mazzottia,
Lorenzo Breschic jan 2007

ConclusionsThis study supports the hypothesis that:
manual or ultrasonic instrumentation alone is notable to expose the sound dentin matrix,
whereas a subsequent acidic conditioning exposes collagen fibrils and associated proteoglycans.
The immunohistochemical technique revealed that despite their acidity, both citric acid and EDTA were able to preserve the structural and biochemical properties of the exposed dentin matrix

Results- Use of 10% citric acid revealed intense labeling “marking” for collagen fibrils and proteoglycans
- lower labeling was found after EDTA conditioning.
- unetched specimens showed residual smear layer on the dentin surface resulting in no evident surface labeling

Stem Cells for Periodontal Regeneration
Balkan J Med Genet. Jun 2013; 16(1): 7 – 12 Published online Oct 3, 2013. doi: 10.2478/bjmg-2013-0012
Periodontal regeneration of damaged tissue is the main goal of the periodontal treatment
This review provides an overview of adult human stem cells and their potential use in periodontal
regeneration

One approach to periodontal regeneration involves incorporation of progenitor cells in a periodontal
defect .
Autologous bone marrow, mesenchymal and adipose-derived stem cells do regenerate alveolar
bone and periodontal ligament-like structures after transplantation

An ideal source may be human adult dermal fibroblasts reprogrammed to pluripotency and to production of enough cells for regenerative
periodontal therapy
Enhanced stem cells techniques will be a way to achieve the desired periodontal
regeneration

THANK YOU



![[PPT]PowerPoint Presentation · Web viewGingivectomy,Gingivoplasty Gingivectomy:Excision of soft tissue wall of periodontal pocket. Basic rational is pocket elimination to allow access](https://img.pdfslide.us/doc/110x75/5adb0e137f8b9a86378e2e11/pptpowerpoint-presentation-viewgingivectomygingivoplasty-gingivectomyexcision.jpg)



![· Web viewEndodontic, Periodontal, Prosthodontic and Oral and Maxillofacial Surgical Services[20%] Orthodontic Treatment[50%]] Maximum Out of Pocket Maximum Out of Pocket means](https://img.pdfslide.us/doc/110x75/612f773f1ecc51586943768f/web-view-endodontic-periodontal-prosthodontic-and-oral-and-maxillofacial-surgical.jpg)