Embed Size (px)
Citation preview

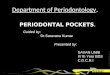
THE PERIODONTAL POCKET
Meenakshi KhasaMDS II yrDAV (C) Dental College, Yamunanagar

Contents Definition Classification Correlation of clinical features and histopathological
features Methods of location Pathogenesis Histopathology Microtopography of gingival wall Periodontal pocket as healing lesion Pocket contents Root surface wall Periodontal disease activity Site specificity Relationship between attachment loss and bone loss to
pocket depth Area between base of pocket and alveolar bone Relation of pocket to bone loss

Definition – Periodontal pocket
Shafer et al, 1983 – defined pocket as a pathologically altered gingival sulcus, lined to a variable extent with pocket epithelium and classified as either a gingival pocket or a periodontal pocket.
Goldman, 1949 – defined pocket as a space bordered on one side by the tooth and on the other by the crevicular epithelium, the base of the pocket being limited by the epithelial attachment.

Definition – Periodontal pocket
GPT, 2001 – A pathologic fissure between a tooth and the crevicular epithelium, and limited at its apex by the junctional epithelium. It is an abnormal apical extension of the gingival crevice caused by migration of the junctional epithelium along the root as the periodontal ligament is detached by a disease process.

Classification

Gingival pocket/Pseudo/ relative/false pocket
Intrabony/Infrabony/Subcrestal/Intralveolar pocket
Pockets
No destruction of supporting periodontal tissues
base of the pocket is coronal to the level of the underlying bone.
base of the pocket is apical to the level of the adjacent bone
Suprabony/Supracrestal/ Supraalveolar pocket
Periodontal pocket/absolute/true

According to involved tooth surfaces – Glickman & Smulow, 1974
Simple pocket Compound pocket Complex pocket

Correlation of Clinical and H/p Features of Periodontal Pocket
CLINICAL FEATURES HISTOPATHOLOGIC FEATURES
1. Gingival wall of pocket presents various degrees of
bluish red discoloration;
flaccidity;
a smooth, shiny surface; and
pitting on pressure.
1. By –
circulatory stagnation;
destruction of gingival fibers and surrounding tissues;
atrophy of epithelium and edema;
edema and degeneration.

Correlation of Clinical and H/p Features of Periodontal Pocket
CLINICAL FEATURES HISTOPATHOLOGIC FEATURES
2. pink and firm gingival wall - Less frequent
2. fibrotic changes predominate over exudation and degeneration, particularly in relation to outer surface of pocket wall.
However, inner wall of pocket presents degeneration and ulceration.

Figure- Periodontal pocket wall. The inner half is inflamed and ulcerated; the outer half is densely collagenous.

Correlation of Clinical and H/p Features of Periodontal Pocket
CLINICAL FEATURES HISTOPATHOLOGIC FEATURES
3. Bleeding on gently probing soft tissue wall of pocket.
3. It results from increased vascularity, thinning and
degeneration of epithelium, and
proximity of engorged vessels to inner surface.

Correlation of Clinical and H/p Features of Periodontal Pocket
CLINICAL FEATURES HISTOPATHOLOGIC FEATURES
4. When explored with a probe, inner aspect of pocket is painful.
5. pus expressed by applying digital pressure.
4. by ulceration of inner aspect of pocket wall.
5. occurs in pockets with suppurative inflammation of inner wall.

What is the method of location of a pocket?
method of locating periodontal pockets and determining their extent is probing of the gingival margin along each tooth surface.
Radiographically – by Gutta percha points. Hirschfeld points.

Probing depth(Listgarten, 1976)
Biologic/Histologic depth
• Distance between gingival margin and base of pocket (coronal end of junctional epithelium.
• Measured in histologic section.
Clinical/Probing depth
• Distance probe penetrates into pocket

Armitage et al, 1977 used beagle dogs to evaluate the penetration of probe using a standardized force of 25gms.
Healthy – probe
penetrated 2/3 of length.
Gingivitis – stopped
0.1mm short of apical end.
Periodontitis – tip went
past the most apical
cells JE.

Pathogenesis

Early concept of pathogenesis
Held that proliferation and apical migration of the cells of the epithelial attachment (junctional epithelium) with pocket formation are the initial and most significant pathologic changes associated with inflammatory gingival and periodontal disease.
Numerous hypothesis were devised to account for the proliferation and apical migration.

Gottlieb, 1921 considered alveolar atrophy and recession of the marginal bone to be a normal consequence of aging and continuous eruption of teeth.
He felt that pocket formation and “pyorrhea” were a consequence of irregularity or accentuation of this normal process.
This idea was strongly opposed by James and Counsell, 1927.
Gottlieb, 1921

Fish, 1935
Fish, 1935 questioned the importance of the epithelial proliferation and migration as the initial and cardinal event.
He maintained that long before this event occurred, an accumulation of inflammatory cells could be observed just deep to the junctional epithelium where proliferation subsequently occurs.

Fish and James and Counsell
Fish, 1935 and James and Counsell, 1927 referred this area as the primary zone of injury.
Their work diverted the attention from the proliferative phenomena and directed it toward the alterations within the underlying connective tissues.

Gottlieb, 1946
Gottlieb, 1946 presented his concept of “cementopathia”.
According to this hypothesis, interference with continuous cemental deposition results in a lack of attachment of the collagen fibers of the gingival and periodontal ligaments to the root surface and permits migration of the epithelial cells apically with pocket formation.

Aisenberg and Aisenberg, 1948
Aisenberg and Aisenberg, 1948 showed that tongues of epithelial cells migrate apically between normal connective tissue bundles, and
They proposed that the epithelial cells exert a lytic effect upon the underlying connective tissue.

Goldman, 1951
Goldman, 1951 noted that migration of the epithelial cells along the root surface could not occur as long as the dense connective tissue fibers underlying the attachment apparatus were intact, and
He postulated an initial degenerative change in these fibers followed by epithelial cell proliferation and migration.

Current thought
In spite of its conceptual limitations and a large body of evidence to the contrary, the idea that epithelial proliferation and apical migration with pocket formation are cardinal event in the pathogenesis of periodontal disease continues to pervade current thought.

Most accepted theory
The initial lesion in the development of periodontitis is the inflammation of the gingiva in response to a bacterial challenge.
Pocket formation starts as an inflammatory change in the connective tissue wall of the gingival sulcus.

Cellular and fluid inflammatory exudate
causes
degeneration of the surrounding connective tissue, including the gingival fibers.

Deporter & Brown, 1980; Schroeder HE, 1970 Just apical to the junctional epithelium
collagen fibers are destroyed and
area is occupied by inflammatory cells and edema (Fig.)
Figure - Note the densely inflamed connective tissue, and the proliferating and ulcerated pocket epithelium.

Early concepts assumed that after initial bacterial attack, periodontal tissue destruction is continued to be caused by bacteria.
However, recently, it was established that the host's immuno-inflammatory response to initial and persistent bacterial attack leads to collagen and bone destruction.

Mechanisms of collagen loss are
I. collagenases and other enzymes secreted by various cells in healthy and inflamed tissue, such as
Fibroblasts (Takada T, Donath, 1988) PMNs (Taichman, 1968) Macrophages (Page RC, Schroeder, 1977)
become extracellular and destroy collagen (these enzymes that degrade collagen and other matrix macromolecules into small peptides are called matrix metalloproteinases Ten Cate, 1994 )

Mechanisms of collagen loss are
II. fibroblasts phagocytize collagen fibers by extending cytoplasmic processes to the ligament-cementum interface and degrade the inserted collagen fibrils and the fibrils of the cementum matrix.
Deporter & Brown,1980;
Deporter & Tencate 1980

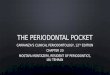
Figure - Low-power view of base of periodontal pocket and apical area. Note the dense inflammatory infiltrate on area of destroyed collagen fibers and the thin, fingerlike extension of epithelium covering the cementum denuded of fibers.
apical cells of the junctional epithelium proliferate along the root, extending fingerlike projections two
or three cells in thickness (fig.)
As a consequence of the loss of collagen,

Figure - View of the ulcerated lateral pocket wall of a periodontal pocket. Note the extension of epithelial cells and the dense accumulation of leukocytes within the epithelium and in the connective tissue.
PMNs invade the coronal end of the junctional epithelium in increasing numbers (Fig.)
As a result of inflammation,

When the relative volume of PMNs reaches approximately 60% or more of the junctional
epithelium,
the tissue loses cohesiveness and detaches from the tooth surface.
Thus the coronal portion of the junctional epithelium detaches from the root as the apical
portion migrates, resulting in its apical shift,
and the oral sulcular epithelium occupies an increasing portion of the sulcus (then a pocket)
lining. Schroeder & Attstrom, 1980

Extension of the junctional epithelium along the root requires the presence of healthy epithelial cells.
Marked degeneration or necrosis of the junctional epithelium impairs rather than accelerates pocket formation.

the gingiva increases in bulk and the crest of the gingival margin extends coronally
The apical cells of the junctional epithelium continue to migrate along the root and its coronal
cells continue to separate from it
With continued inflammation,

The epithelium of the lateral wall of the pocket
Leukocytes and edema from the inflamed connective tissue
proliferates to form
bulbous, cordlike extensions into the inflamed connective tissue
infiltrate the epithelium lining the pocket
resulting in
degeneration and necrosis

The transformation of a gingival sulcus into a periodontal pocket creates an area where plaque removal becomes impossible, and a feedback mechanism is established.
The rationale for pocket reduction is based on the need to eliminate areas of plaque accumulation.

Histopathology

Soft tissue wall
The connective tissue is edematous and densely infiltrated with
plasma cells (approx. 80%), lymphocytes, and a scattering of PMNs.
The blood vessels - increased in number, dilated, and engorged. Bonakdar et al, 1997
exhibits degeneration. Single or multiple necrotic foci are occasionally present. Orban & Ray, 1948
shows proliferation of the endothelial cells, with newly formed capillaries, fibroblasts, and collagen fibers.

Junctional epithelium
The junctional epithelium at the base of the pocket is usually much shorter than that of a normal sulcus.
Corono-apical length of the junctional epithelium is reduced to only 50 to 100 µm. Carranza , 1967
The cells may exhibit slight-to-marked degeneration.

Lateral wall of pocket
Exhibits the most severe degenerative changes.
Epithelial buds or interlacing cords of epithelial cells project from the lateral wall into the adjacent inflamed connective
tissue and may extend apical to the junctional epithelium.
These epithelial projections, and remainder of the lateral epithelium, are densely infiltrated by leukocytes and edema from the inflamed connective tissue.

Lateral wall of pocket
The cells undergo vacuolar degeneration and rupture to form vesicles.
Progressive degeneration and necrosis of the epithelium lead to ulceration of the lateral wall, exposure of the underlying inflamed
connective tissue, and suppuration.

Lateral wall of pocket
A comparative study of gingival changes in aggressive and chronic periodontitis revealed more pronounced degenerative changes in the
epithelium of aggressive cases with more open intercellular spaces, micro-clefts and necrotic areas. Hillmann et al, 1998
The severity of the degenerative changes is not necessarily related to pocket depth.

Lateral wall of pocket
The epithelium at the gingival crest of a periodontal pocket is generally intact and thickened, with prominent rete pegs.

Bacterial invasion – apical and lateral areas of pocket wall
In intercellular spaces of epithelium – Filaments, rods, and coccoid organisms with predominant gram-
negative cell walls Frank, 1980
P. gingivalis and P. intermedia found in the gingiva of aggressive periodontitis cases. Hillmann et al, 1998
Actinobacillus actinomycetemcomitans has also been found in the tissues. Christersson et al, 1987; Meyer et al, 1991; Saglie et al, 1998

Bacterial invasion – apical and lateral areas of pocket wall
Bacteria are also found between deeper epithelial cells and accumulating on the basement lamina.
Some bacteria traverse the basement lamina and invade the subepithelial connective tissue.
Saglie et al, 1982
The presence of bacteria in the gingival tissues has been interpreted as bacterial invasion or as “passive translocation” of plaque bacteria.
Listgarten, 1986

Microtopography of gingival wall
Using scanning electron microscopy, areas in the gingival wall of pocket have been described in which different types of activity take place.
Saglie et al, 1982
These areas are irregularly oval or elongated and adjacent to one another and measure about 50 to 200 µm.
These findings suggest that the pocket wall is constantly changing.
The following areas have been noted:

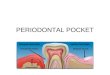
I. Areas of relative quiescence
shows a relatively flat surface with minor depressions and mounds and occasional shedding of cells.

Figure Scanning electron frontal micrograph of the periodontal pocket wall. Different areas can be seen in the pocket wall surface. A, Area of quiescence; B, bacterial accumulation; C, bacterial-leukocyte interaction; D, intense cellular desquamation. Arrows point to emerging leukocytes and holes left by leukocytes in the pocket wall.

II. Areas of bacterial accumulation
appear as depressions on the epithelial surface, with abundant debris and bacterial clumps penetrating into the enlarged intercellular
spaces.
These bacteria are mainly cocci, rods, and filaments, with a few spirochetes.

III. Areas of emergence of leukocytes
leukocytes appear in the pocket wall through holes located in the intercellular spaces.

IV. Areas of leukocyte-bacteria interaction
Numerous leukocytes are present and covered with bacteria in an apparent process of phagocytosis.
Bacterial plaque associated with the epithelium is seen either as an organized matrix covered by a fibrin-like
material in contact with the surface of cells or bacteria penetrating into the intercellular
spaces.

V. Areas of intense epithelial desquamation
consist of semi-attached and folded epithelial squames, sometimes partially covered with bacteria.

VI. Areas of ulceration
Areas of ulceration, with exposed connective tissue.

Figure - Left, Area of ulceration in the lateral wall of a deep periodontal pocket. A, Surface of pocket epithelium in a quiescent state; B, area of hemorrhage. Right, Magnification of the square on left. Connective tissue fibers and cells can be seen in the bottom of the ulcer.

VII. Areas of hemorrhage
Areas of hemorrhage, with numerous erythrocytes.

The transition from one area to another results from bacteria accumulating in previously quiescent
areas and triggering the emergence of leukocytes and the leukocyte-bacteria interaction.
This leads to intense epithelial desquamation and finally to ulceration and hemorrhage.

Periodontal pockets as healing lesions
Periodontal pockets are chronic inflammatory lesions and thus are constantly undergoing repair.
Complete healing does not occur because of the persistence of the bacterial attack, which continues to stimulate an inflammatory response, causing degeneration of the new tissue elements formed in the continuous effort at repair.

Pocket contents
debris consisting of microorganisms and their products (enzymes,
endotoxins, and other metabolic products), gingival fluid, food remnants, salivary mucin, desquamated epithelial cells, leukocytes. Plaque-covered calculus projecting from
tooth surface.

Pocket contents
Purulent exudate consists of living, degenerated, and necrotic leukocytes; living and dead bacteria; serum; and a scant amount of fibrin. McMillan et al,
1958
The contents of periodontal pockets filtered free of organisms and debris were found toxic when injected subcutaneously into animals. Graham, 1937

Significance of pus formation
Pus is a common feature of periodontal disease, but only a secondary sign.
It just reflects the nature of the inflammatory changes in the pocket wall.
It is not an indication of the depth of the pocket or the severity of the destruction of the supporting tissues.

Root surface wall of pocket
undergoes changes that perpetuate periodontal infection, cause pain, and complicate periodontal treatment.
Bosshardt and Selvig, 1997

I. Effect of gingival inflammation
1. Subsurface alterations Inflammation in connective tissue results in a –
Net loss of collagen Breakdown of dentogingival fibers
Loss of collagen cross-banding and dissolution of mineral crystals. Selvig, 1966 & 1968
Collagenous remnants of Sharpey's fibers undergo degeneration.

I. Effect of gingival inflammation
2. Cervical root resorption Inflammatory process in adjacent
connective tissue triggers root resorption defects in the cervical region.

II. Exposure to the oral environment
1. Bacterial contamination Cementum is porous and allows permeation of -
organic substances derived from saliva or bacterial plaque, Inorganic ions, Bacteria
Viable bacteria - found in roots of 87% of periodontally diseased non-carious teeth and suggested that cementum and dentin serve as reservoirs from which re-colonization of mechanically debrided root surfaces can occur, as well as infection of dental pulp. Adriaens et al, 1988

II. Exposure to the oral environment
1. Bacterial contamination Bacteria penetrate as deep as the
cemento-dentinal junction (Adriaens PA, DeBoever, 1986; Daly et al, 1982) and enter the dentinal tubules.
(Giuliana et al, 1997; Graham, 1937)
Bacterial lipo-polysacchanride detected in 40 – 70 µm deep surface layer of periodontally diseased roots. Lygre et al, 1992

II. Exposure to the oral environment
1. Bacterial contamination Bacterial penetration and growth leads to
fragmentation and breakdown of the cementum surface and
results in areas of necrotic cementum, separated from the tooth by masses of bacteria.
Pathologic granules represent areas of collagen degeneration or areas in which collagen fibrils are not fully mineralized initially. Bass, 1957; Armitage & Christie, 1973

II. Exposure to the oral environment
1. Bacterial contamination Endotoxins - detected in cementum wall
of pocket. Aleo & Vandersall, 1980; Aleo et al, 1974
Root fragments with periodontal disease if placed in tissue culture induce irreversible morphologic changes in cells of the culture. Hatfield & Baumhammers, 1971

Diseased root fragments prevent in vitro attachment of human gingival fibroblasts, whereas normal root surfaces allow the cells to attach freely. Aleo et al, 1975
Diseased root fragments placed in oral mucosa induce an inflammatory response even if they are autoclaved.
Lopez et al, 1980

These changes manifest as softening of the cementum surface, which is usually asymptomatic, but painful when a probe or explorer penetrates the area.
They constitute a reservoir for reinfection of the area after treatment. In the course of treatment, these necrotic areas are removed by root planing until a hard, smooth surface is reached.

II. Exposure to the oral environment
2. Decalcification & remineralization of cementum Areas of increased mineralization - result of an
exchange of minerals and organic components at the cementum-saliva interface. Selvig, 1969
mineral content of exposed cementum increases. Selvig, 1966
Minerals increased include calcium, Selvig & Zander, 1962 magnesium, Nakata, 1972; Selvig & Zander,
1962 phosphorus, Nakata, 1972 fluoride. Nakata, 1972

II. Exposure to the oral environment
2. Decalcification & remineralization of cementum
Micro-hardness remains unchanged. Rautiola & Craig, 1961; Warren et al,
1964
Hypermineralized superficial layer increases tooth resistance to decay. Aleo et al, 1975
Hypermineralized zones are associated with increased perfection of the crystal structure and organic changes suggestive of a subsurface cuticle.
Selvig, 1966 & 1969

II. Exposure to the oral environment
2. Decalcification & remineralization of cementum
These zones are 10 to 20 µm thick, with areas as thick as 50 µm. Selvig & Hals, 1977
No decrease in mineralization was found in deeper areas indicating that increased mineralization does not come from adjacent areas.
Subsurface condensation of organic material of exogenous origin. Selvig, 1966

II. Exposure to the oral environment
2. Decalcification & remineralization of cementum
Areas of demineralization are related to root caries.
As a results of proteolysis of embedded remnants of Sharpey's fibers; the cementum softens and undergoes fragmentation and cavitation.
Herting, 1967
Root surface caries progresses around rather than into the tooth. Mount, 1986

II. Exposure to the oral environment
2. Decalcification & remineralization of cementum
Active root caries lesions – well-defined yellowish or light-brown areas, frequently covered by plaque, softened or leathery consistency on probing.
Inactive lesions – well-defined darker lesions smooth surface harder consistency on probing. Fejerskov &
Nyvad, 1986

II. Exposure to the oral environment
2. Decalcification & remineralization of cementum
Active root caries lesions – well-defined yellowish or light-brown areas, frequently covered by plaque, softened or leathery consistency on probing.
Inactive lesions – well-defined darker lesions smooth surface harder consistency on probing. Fejerskov &
Nyvad, 1986

II. Exposure to the oral environment
2. Decalcification & remineralization of cementum
Predominant microorganism in root caries is Actinomyces viscosus Syed et al, 1975
Bacteria that produce root caries in animal models - Actinomyces naeslundii, Streptococcus mutans, Streptococcus salivarius, Streptococcus sanguis, Bacillus cereus

II. Exposure to the oral environment
2. Decalcification & remineralization of cementum
When plaque levels and pocket depths decrease after periodontal therapy, a shift in oral bacteria occurs, leading to reduction in periodontal pathogens and an increase in S. mutans and development of root
caries. Quirynen et al, 1999

II. Exposure to the oral environment
2. Decalcification & remineralization of cementum
Root caries – causes toothache in patients with periodontal disease and no evidence of coronal decay.
The necrotic cementum must be removed by scaling and root planing until firm tooth surface is reached, even if this entails extension into the dentin.

II. Exposure to the oral environment
2. Decalcification & remineralization of cementum Areas of cellular resorption of cementum and dentin
are common in roots unexposed by periodontal disease and they usually undergo repair. Sottosanti, 1977
If root is exposed by pocket before repair occurs, these areas appear as
isolated cavitations that penetrate into the dentin.
differentiated from root caries by their clear-cut outline and hard surface.
source of pain, requiring placement of a restoration.

Surface morphology of tooth wall
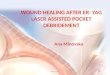
Figure Diagram of the area at the bottom of a pocket; c.t., connective tissue.

Zones at bottom of pocket1) Cementum covered by calculus
2) Attached plaque - covers calculus and extends apically from it to 100 to 500 µm.
3) Unattached plaque - surrounds attached plaque and extends apically to it.
4) Attachment of junctional epithelium to tooth – Extension in normal sulci is > 500 µm, Extension is reduced in periodontal pockets to <
100 µm.
5) Semidestroyed connective tissue fibers - apical to the junctional epitheliumSaglie et al, 1982

Plaque-free zone
Bass, 1946; Brady, 1973; Hoffman & Gold, 1971; Saglie et al, 1975; Waerhaug, 1952 “plaque-free zone” seen in extracted teeth - Unattached plaque Attachment of junctional epithelium to tooth Semidestroyed connective tissue fibers
Its total width varies according to- the type of tooth (wider in molars than in incisors) depth of the pocket (narrower in deeper pockets).
Saglie et al, 1975

Plaque-free zone
plaque-free zone refers only to attached plaque because unattached plaque contains gram-positive and gram-negative cocci, rods, filaments, fusiforms, and spirochetes.
The most apical zone contains predominantly gram-negative rods and cocci. Vrahopoulos et al, 1995

Periodontal disease activityFor many years the loss of attachment produced by periodontal disease was thought to be a slow but continuously progressive phenomenon. More recently, as a result of studies on the specificity of plaque bacteria, the concept of periodontal disease activity has evolved.

Periodontal disease activity
According to this concept, periodontal pockets go through periods of exacerbation and quiescence, resulting from episodic bursts of activity followed by periods of remission.
Periods of quiescence or inactivity - characterized by a reduced inflammatory response and little or no loss of bone and connective tissue
attachment.

Periodontal disease activity
A buildup of unattached plaque, with its gram-negative, motile, and anaerobic bacteria, starts a period of exacerbation or activity in which bone and connective tissue
attachment are lost and the pocket deepens.
This period lasts for days, weeks, or months and is followed by a period of remission or quiescence in which gram-positive bacteria proliferate and
a more stable condition is established.

Periodontal disease activity
Bone loss in untreated periodontal disease occurs in an episodic manner.
McHenry et al, 1981
Clinically, active periods show bleeding, gingival exudate.
Histologically, the pocket epithelium appears thin and ulcerated, an infiltrate composed predominantly of plasma cells,
(Davenport, 1982) PMNs, (Page & Schroeder, 1977) or both.

Periodontal disease activity
Bacterial samples from the pocket lumen show high proportions of motile organisms and spirochetes.
Listgarten & Hellden, 1978

Site specificity

Site specificity
Periodontal destruction does not occur in all parts of the mouth at the same time but rather on a few teeth at a time or even only some aspects of some teeth at any given time. This is referred to as the site specificity of periodontal disease.
Severity of periodontitis increases with the development of new disease sites and increased breakdown of existing sites.

Relationship of attachment loss and bone loss to pocket depth

Pocket depth or level of attachment?
POCKET DEPTH LEVEL OF ATTACHMENT
Distance between base of pocket and gingival margin.
not reliable indicators of extent of bone support because these measurements are made from the gingival margin.
The position of gingival margin changes with tissue swelling, overgrowth, and recession.
Distance between base of pocket and fixed point on crown (CEJ).
Better indicator of degree of periodontal destruction.

Pocket depth or level of attachment?
POCKET DEPTH LEVEL OF ATTACHMENT
calculated from measurements made from a fixed point that does not change.
Because bone level in health is approx. 2 mm apical to CEJ, clinical attachment levels provide a reliable indication of the extent of bone support.

Determining the loss of attachment

Pocket depth
When gingival margin apical to CEJ
distance between CEJ & GM
Level of attachment

Pocket depth
distance between CEJ & GM
Level of attachment
Pocket depth
When gingival margin coronal to CEJ

Pocket depth
Level of attachment
When gingival margin coincides CEJ

Area between base of pocket and alveolar bone

Area between base of pocket and alveolar bone
Distance between apical extent of calculus and alveolar crest in pocket
is constant having a mean length of 1.97 mm (±33.16%).
Stanley, 1955; Wade, 1960

Area between base of pocket and alveolar bone
Distance from attached plaque to bone is never less than 0.5 mm and never more than 2.7 mm. Waerhaug,
1952 & 1979
These findings suggest that the bone-resorbing activity induced by bacteria is exerted within these distances.

Relationship of pocket to bone

Distinguishing features
SUPRABONY POCKET INFRABONY POCKET
1. Base of pocket is coronal to level of alveolar bone.
2. Pattern of destruction of underlying bone is horizontal.
1. Base of pocket is apical to crest of alveolar bone so that bone is adjacent to soft tissue wall.
2. Pattern of bone destruction is vertical.

Distinguishing features
SUPRABONY POCKET INFRABONY POCKET
3. Interproximally, transseptal fibers that are restored during progressive periodontal disease are arranged horizontally in the space between base of pocket and alveolar bone.
3. Interproximally, transseptal fibers are oblique rather than horizontal. They extend from cementum beneath base of pocket along alveolar bone and over crest to cementum of adjacent tooth.

Distinguishing features
SUPRABONY POCKET INFRABONY POCKET
4. On facial and lingual surfaces, periodontal ligament fibers beneath pocket follow their normal horizontal-oblique course between the tooth and bone.
4. On facial and lingual surfaces, periodontal ligament fibers follow angular pattern of adjacent bone. They extend from cementum beneath base of pocket along alveolar bone and over crest to join with outer periosteum.
















![[PPT]PowerPoint Presentation · Web viewGingivectomy,Gingivoplasty Gingivectomy:Excision of soft tissue wall of periodontal pocket. Basic rational is pocket elimination to allow access](https://img.pdfslide.us/doc/110x75/5adb0e137f8b9a86378e2e11/pptpowerpoint-presentation-viewgingivectomygingivoplasty-gingivectomyexcision.jpg)