Embed Size (px)
Citation preview
|
Peeking behind the test – insights and innovations
Medical Council of Canada
Dr. Ian Bowmer, Dr. André De Champlain,
Stephen Abraham, Jessica Hertzog-Grenier
|
Overview
Introduction
› Assessment Review Task Force (IAN)
› Blueprint Project (ANDRE)
› Flexible exam delivery (ANDRE)
Innovations
› Automated Item Generation (Andre)
› Automated Marking (Stephen)
› New item bank (MOC5) (Stephen)
Other developments
› Orientation
› Preparatory materials
Q&A
2 Insights and innovations from the Medical Council of Canada
|
Introduction –
Recalibrating for the 21st Century:
Report of the Assessment Review Task
Force of the Medical Council of Canada (October, 2011)
• Outlined 6 recommendations to focus
on in the MCC’s reassessment &
realignment of exams
3
Assessment Review Task Force
|
Introduction –
6 ARTF RECOMMENDATIONS
Recommendation 1
• LMCC becomes ultimate credential (legislation issue)
Recommendation 2
• Validate & update blueprint for MCC examinations
Recommendation 3
• More frequent scheduling of the exams and associated automation
Recommendation 4
• IMG assessment enhancement and national standardization
(NAC & Practice Ready Assessment)
Recommendation 5
• Physician performance enhancement assessments
Recommendation 6
• Implementation oversight, Committee priorities and budgets4
Assessment Review Task Force
|
Introduction –
Recommendation #2
That the content of MCC examinations be expanded by:
• Defining the knowledge and behaviours in all the CanMEDS roles that
demonstrate competency of the physician about to enter independent practice
• Reviewing the adequacy of content and skill coverage on the blueprints for all
MCC examinations
• Revising the examination blueprints and reporting systems with the aim of
demonstrating that the appropriate assessment of all core competencies is
covered and fulfills the purpose of each examination
• Determining whether any general core competencies considered
essential cannot be tested employing the current MCC examinations, and
exploring the development of new tools to assess these specific
competencies when current examinations cannot5
Blueprint Project
|
Introduction –
6
Blueprint Project
Assessment of innovative item types to better target blueprint
gaps (audio/video, technology-based, etc.)
• Can MCC exams “evolve” towards meeting blueprint domains
more fully with the addition of innovative item types?
• Impacts both the MCCQE Parts I and II
• Advisory group meeting (March, 2015)
• Overview of technology-based items (“hot spots”, “drag & drop”),
higher-order cognitive skills (“pharma ads”, “abstract searches”)
• SJT-type vignettes might prove most useful to pursue to
assess aspects of Professionalism & Communication
|
Introduction –
Piloting of new OSCE stations to better assess non-cognitive
skills (CM, PF) and complex patient presentations (multiple
morbidities)
• Piloted 4 new OSCE stations in Fall, 2014 exam
• Stations discriminated well and were generally more difficult
than traditional counterparts
• Provides some preliminary evidence to support the evolving
nature of the MCCQE Part II exam
7
Blueprint Project
|
Introduction –
Recommendation #3
The timing for taking the MCCQE Part I and II, and the frequency
with which they are offered, be revisited by exploring:
• Options allowing more flexibility in scheduling all of the MCC
examinations
• Options permitting the components of the MCCQE Part I (knowledge
and clinical decision-making) to be offered at the appropriate times in
the learning/assessment continuum
• The development of an integrated national assessment strategy for
physicians in training in collaboration with the CFPC and RCPS
8
Flexible exam delivery
|
Introduction –
How can we offer our exam more frequently and with
a greater degree of flexibility?
• By adopting evidence-based simplified scoring
◦ CEC (December, 2012) endorsed R&D recommendation to
drop checklist/component weighting for MCCQE Part 2
starting with spring 2013 MCCQE Part II exam
◦ Rasch IRT scoring model applied to MCCQE Part I exam as of
spring, 2015
◦ Version 1.0 of Automated Scoring System for MCC exams
9
Flexible exam delivery
|
Introduction –
How can we offer our exam more frequently and with a
greater degree of flexibility?
• By automating manual processes
◦ Automated marking of CDM questions using natural language
processing (NLP)
› Preliminary findings are very encouraging
› NLP marking of CDM questions in concordance with human
markings over 96% of the time, on average
› Would allow the automation of what is currently a very
laborious process
10
Flexible exam delivery
|
Introduction –
How can we offer our exam more frequently and with a
greater degree of flexibility?
• By increasing item pool size using AIG
◦ Supplementing/re-envisioning current MCC TD processes
to create large pools of items in targeted areas
◦ AIG might not only allow us to better meet ARTF #3 but
also enable us to address other needs (self-assessments,
progress tests, etc.)
11
Flexible exam delivery
|
Innovations –
What is AIG?
• Automated item generation (AIG) is the process of using
item models to generate test items with the aid of
computer technology
• AIG uses a 3-stage process for generating items where
the cognitive mechanism required to solve the items is
identified and manipulated to create new items (“cognitive
map”)
12
Automated item generation
|
Innovations –
13
Automated item generation
The model includes three key outcomes:
1. Identification of THE PROBLEM
(i.e., Post-Operative Fever)
2. Specification of SOURCES of information required to
diagnose the problem (i.e., Type of Surgery, Physical
Examination, etc.)
3. Description of Elements within each information source
(e.g., Guarding and Rebound, Fever, Calf Tenderness, etc.)
needed to create different instances of the problem
|
Innovations –
14
Automated item generation
Item Model• Item models are created using the cognitive model content, where an item
model is like a template, a rendering, or a mold of the assessment task (i.e., it’s
a target where we want to place the content for the item)
• A 54-year-old woman has a <Type of Surgery>. On post- operative day
<Timing of Fever>. The patient has a temperature of 38.5c. Physical
examination reveal <Physical Examination>. Which one of the following is
the best next step?
• Type of Surgery: Gastrectomy, Right Hemicolectomy, Left Hemicolectomy,
Appendectomy, Laparoscopic Cholecystectomy
• Timing of Fever: 1 to 6 days
• Physical Examination: Red and Tender Wound, Guarding and Rebound,
Abdominal Tenderness, Calf Tenderness
|
Innovations –
Lessons Learned
• The MCC has been working on AIG with the U of A researchers for
the past 5+ years
• Thousands of items have been generated across 50+ cognitive maps
• Predictive identification accuracy ranged from 32% to 52% across 4
experts, with an average accuracy rate of 42%
• Experts cannot systematically differentiate AIG from traditional items
• Piloted AIG items cover shallow areas of our pool very well
◦ On average, AIG items are more difficult and discriminating (based
on classical and IRT statistics)
◦ Directly attributable to the AIG process15
Automated item generation
|
Innovations –
Next Steps
• Undertake 2 additional AIG content development workshops in May
and September, 2015
◦ ~ 20 new cognitive maps
• Pretest ~70 AIG items in the spring, 2015 MCCQE Part I exam cycle
◦ Selected from 2014 cognitive maps and generated items
• Create several apps that will further automate the AIG process and
allow us to fully transition AIG to the MCC
• Finalize a cost-benefit analysis of AIG vs. traditionally written items
16
Automated item generation
|
Innovations –
The Challenge• MCC QE1 has Clinical Decision Making (CDM) component which
includes Write-in answers marked by Physician markers
• Spring Administration - 4,200 candidates answer 86 (scored) questions each
• There are 4,200 X 86 = 361,200 distinct answers to score
• And… 2 rounds to ensure quality
• Over 700,000 answers marked!
• 50 physicians are required to mark
• Difficult to sustain more frequent and flexible test administrations
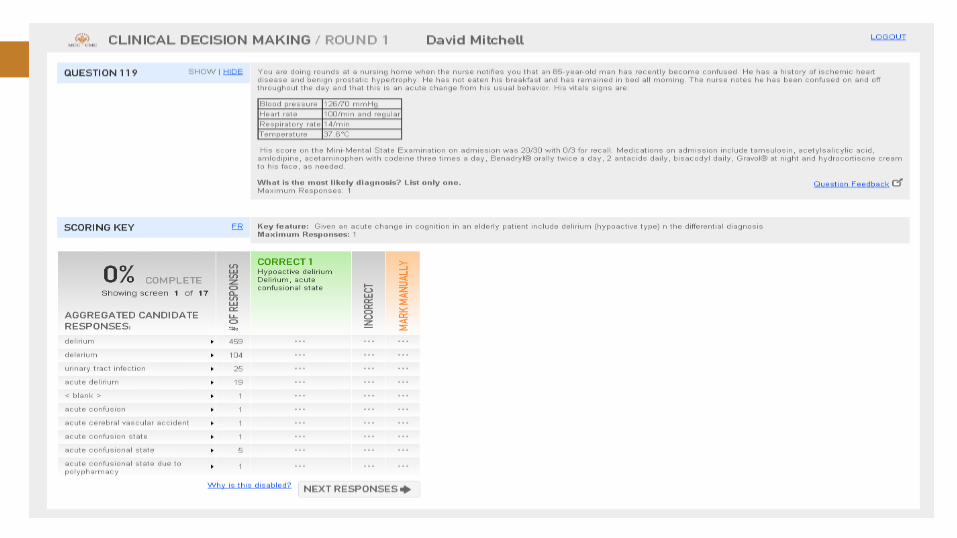
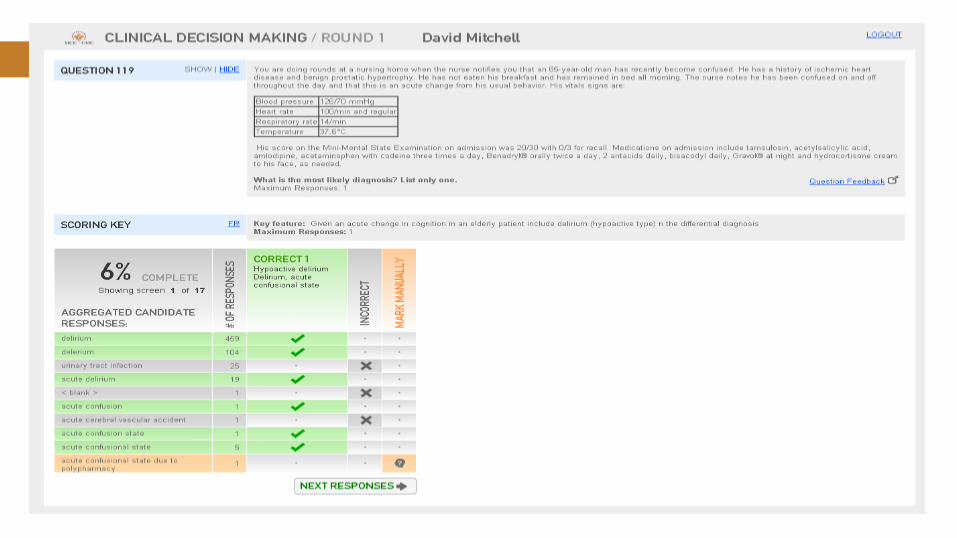
Streamlining CDM marking
|
Innovations –
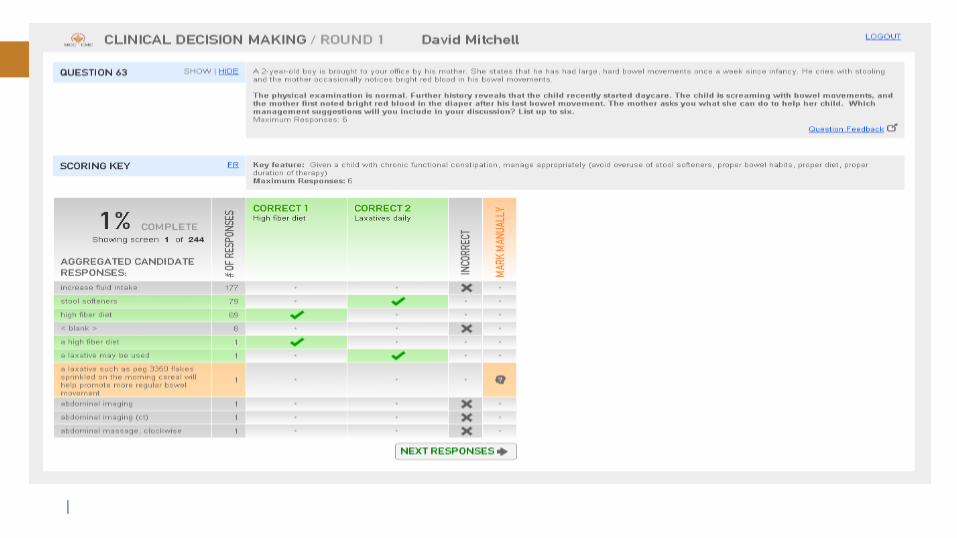
Our solution
• Re-think our approach
• Combine all identical answers
• Display aggregated answers along with number of
occurrences
• Allow for one-click bulk marking
Streamlining CDM marking
|
Innovations –
|
Innovations –
|
Innovations –
|
Innovations –
|
Innovations –
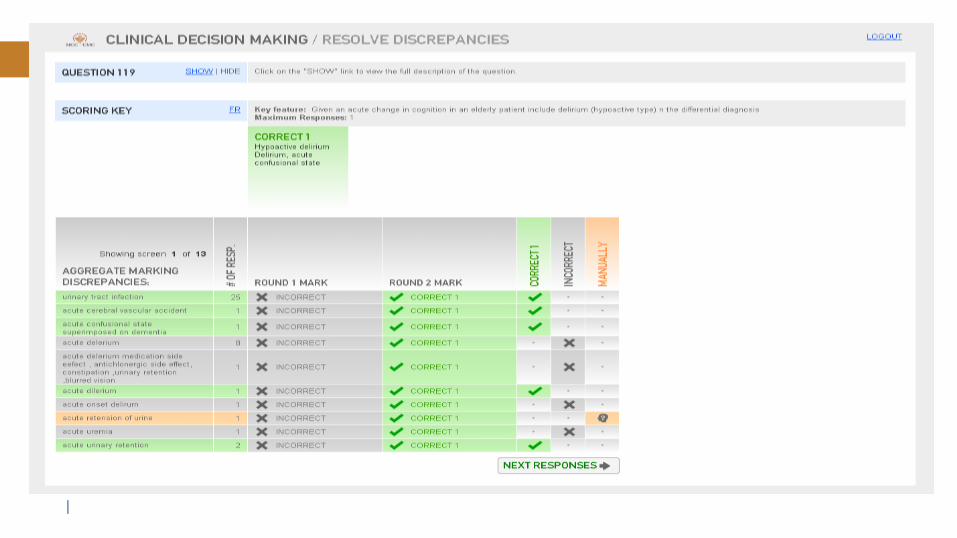
• Marked examination in ~half the time
• Improved quality
• Provides insight into question development (well-formed
questions prompt fewer distinct responses)
• Happier, less fatigued markers
• Reduced marking costs
CDM Marking Results
|
Innovations –
The Challenge
• Items from MCC’s 5 exams managed in 5 systems
• Varied Item types; MCQ, CDM, OSCE
• Varied business processes for item development and
managed – constrained by systems
• Wanted a single consistent system and processes
• No product exists on market (bilingual, committee driven
item development)
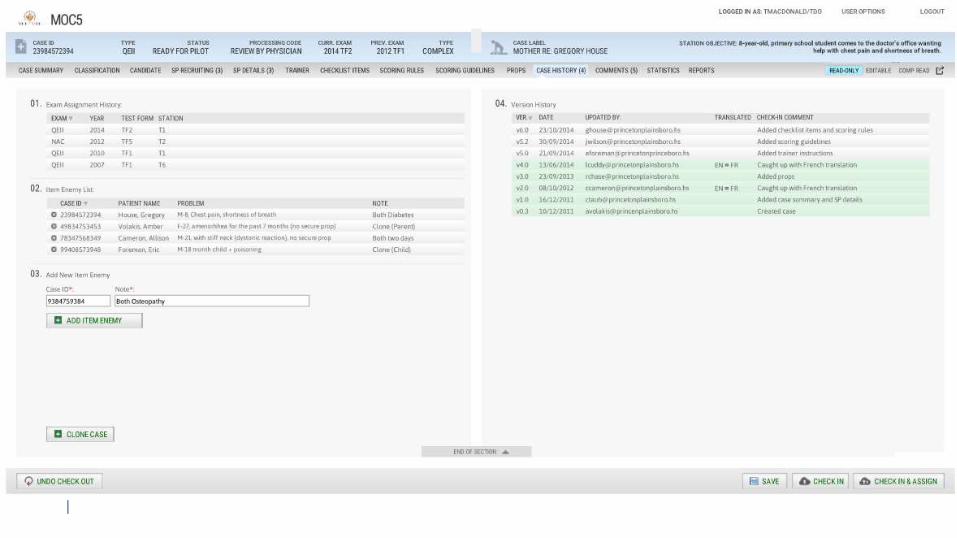
Integrated Item Bank
|
Innovations –
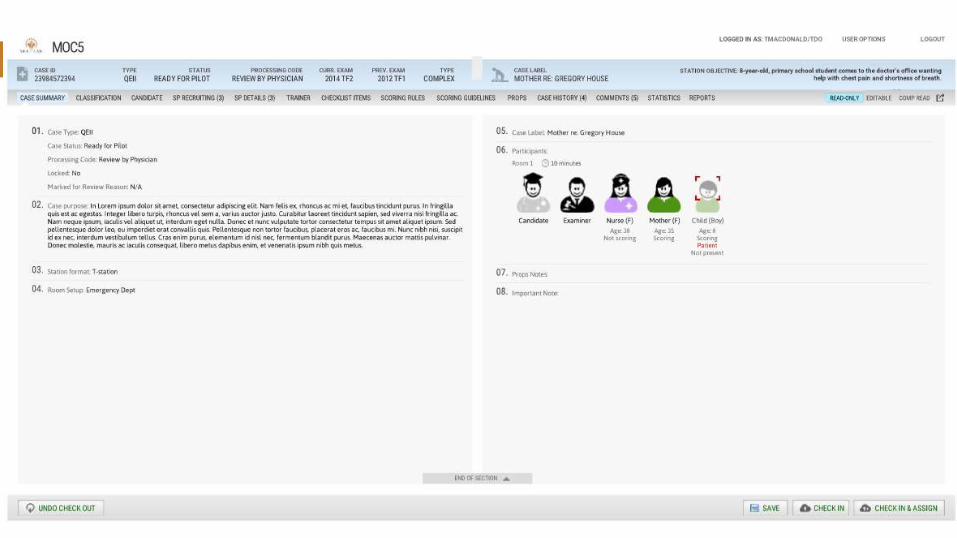
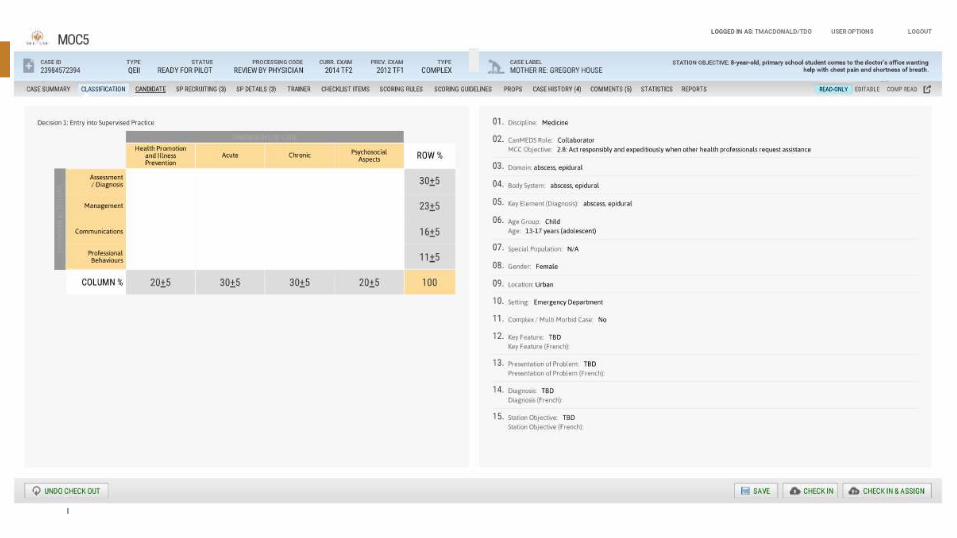
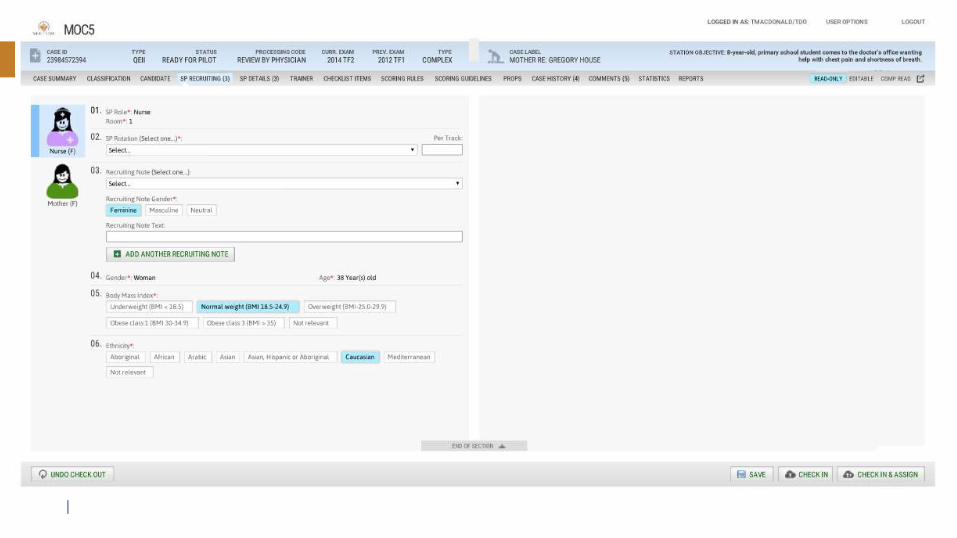
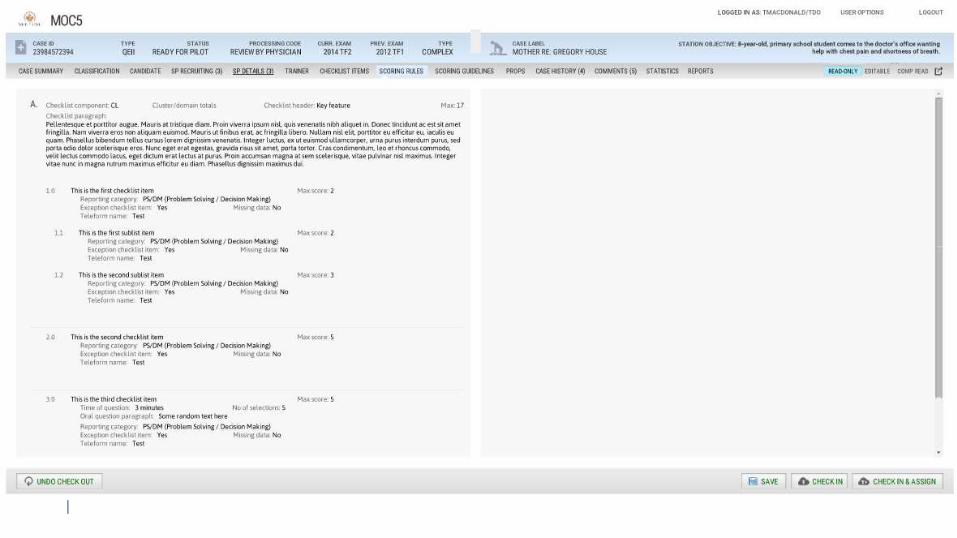
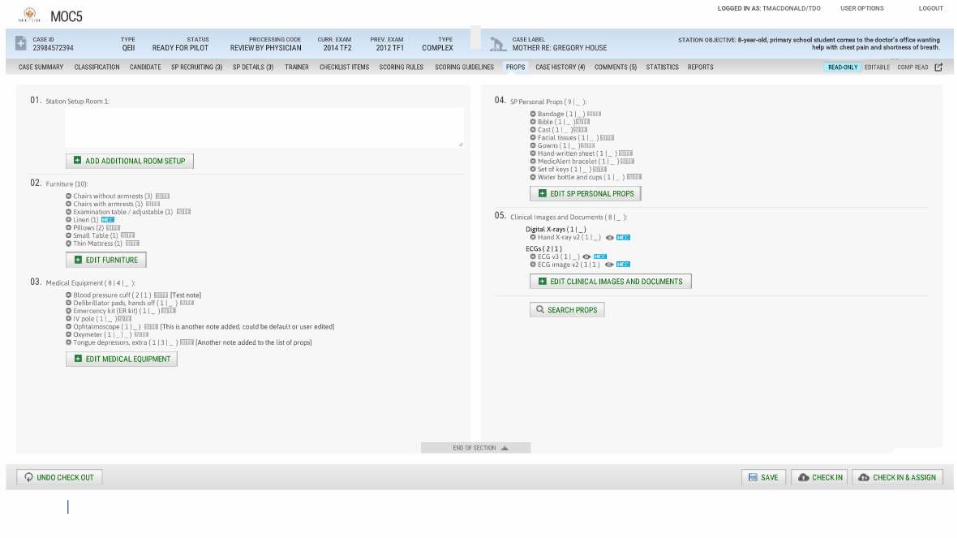
Our Solution
• Writing our own – “MOC5”
• Development began late last year
• OSCE IB to be ready for Fall
• MCQ’s and CDM’s to follow
Integrated Item Bank
|
Innovations –
|
Innovations –
|
Innovations –
|
Innovations –
|
Innovations –
|
Innovations –
|
Innovations –
• Development well underway
• 3 Phases:
• Fall 2015 – OSCE Items
• Spring 2016 – MCQ Items
• Fall 2016 – CDM Items
Integrated Item Bank
|
Other developments –
• Practice ready assessment – online orientation
• Two themes: culture & communication
• Tool repurposing
• Working group review
• Re-filming, translation and launch of web platform
33
Orientation

|
Other developments –
34
Orientation case topics
|
Other developments –
• Coming to a website near you! – Sept. 2015
• Pilots with PRA programs
• Integration with programs’ current orientation activities
• Broader adoption and use
35
Orientation
|
Other developments –
• In support of the international delivery of the MCCQE
Part I:
• Enhanced self-assessments
• Prep guide
• Orientation modules
• Expected launch – 2018-2019
36
Preparatory materials

|
Q & A
37

|
THANK YOU!
*8
*8
*8
*8
Dr. Ian Bowmer [email protected]
Dr. André De Champlain
Stephen Abraham
Jessica Hertzog-Grenier