Embed Size (px)
DESCRIPTION
Citation preview


Pathophysiology of Respiratory Failure
Gamal Rabie Agmy ,MD ,FCCP Professor of Chest Diseases, Assiut University
ERS National Delegate of Egypt


Non Respiratory Functions
Biologically Active Molecules: *Vasoactive peptides
*Vasoactive amines
*Neuropeptides
*Hormones
*Lipoprotein complexes
*Eicosanoids

Non Respiratory Functions
Haemostatic Functions
Lung defense :
*Complement activation
*Leucocyte recruitment
*Cytokines and growth factors
Protection
Vocal communication
Blood volume/ pressure and pH regulation

Respiratory Functions
*Oxygenation
*CO2 Elimination


Definition
*Failure in one or both gas exchange functions:
oxygenation and carbon dioxide elimination
*In practice:
PaO2<60mmHg or PaCO2>50mmHg
*Derangements in ABGs and acid-base status

Definition
Respiratory failure is a syndrome of
inadequate gas exchange due to
dysfunction of one or more essential
components of the respiratory system

Types of Respiratory Failure
Type 1 (Hypoxemic ): * PO2 < 60 mmHg on room air.
Type 2 (Hypercapnic / Ventilatory): *PCO2 > 50
mmHg
Type 3 (Peri-operative): *This is generally a subset of
type 1 failure but is sometimes considered
separately because it is so common.
Type 4 (Shock): * secondary to cardiovascular
instability.

The respiratory System
Lungs Respiratory pump
Pulmonary Failure
• PaO2
• PaCO2 N/
Ventilatory Failure
• PaO2
• PaCO2
Hypoxic
Respiratory
Failure
Hypercapnic
Respiratory
Failure

Cardiogenic pulmonary edema
Pneumonia
pulmonary ARDS
extra pulmonary ARDS
Atelectasis
Post surgery changes
Aspiration
Trauma
Infiltrates in immunsuppression
Hypoxic
Respiratory
Failure Pulmonary fibrosis

Type 3 (Peri-operative)
Respiratory Failure
Residual anesthesia effects, post-
operative pain, and abnormal
abdominal mechanics contribute to
decreasing FRC and progressive
collapse of dependant lung units.

Type 3 (Peri-operative)
Respiratory Failure
Causes of post-operative atelectasis include;
*Decreased FRC
*Supine/ obese/ ascites
*Anesthesia
*Upper abdominal incision
*Airway secretions

Type 4 (Shock)
Type IV describes patients who are intubated and
ventilated in the process of resuscitation for
shock
• Goal of ventilation is to stabilize gas
exchange and to unload the respiratory
muscles, lowering their oxygen consumption
*cardiogenic
*hypovolemic
*septic

Hypoxemic Respiratory Failure (Type 1)
Causes of Hypoxemia
1. Low FiO2 (high altitude)
2. Hypoventilation
3. V/Q mismatch (low V/Q)
4. Shunt (Qs/Qt)
5. Diffusion abnormality
6. low mixed venous oxygen due to cardiac desaturation with one of above mentioned factors.

Physiologic Causes of Hypoxemia
Low FiO2 is the primary cause of ARF at high altitude and toxic gas inhalation
Hypoxemic Respiratory Failure (Type 1)

Physiologic Causes of Hypoxemia
However, the two most common causes of hypoxemic respiratory failure in the ICU are V/Q mismatch and shunt. These can be distinguished from each other by their response to oxygen. V/Q mismatch responds very readily to oxygen whereas
shunt is very oxygen insensitive.
Hypoxemic Respiratory Failure (Type 1)

V/Q: possibilities
0
1
∞
V/Q =1 is “normal” or “ideal”
V/Q =0 defines “shunt”
V/Q =∞ defines “dead space” or “wasted ventilation”

Hypoxemic Respiratory Failure (Type 1)
V/Q Mismatch
V/Q>1 V/Q<1
V/Q=o V/Q=∞

Why does “V/Q mismatch” cause
hypoxemia?
Low V/Q units contribute to
hypoxemia
High V/Q units cannot compensate
for the low V/Q units
Reason being the shape of the
oxygen dissociation curve which is
not linear

Hypoxic respiratory failure
Gas exchange failure
Respiratory drive responds
Increased drive to breathe
– Increased respiratory rate
– Altered Vd /Vt (increased dead space etc)
– Often stiff lungs (oedema, pneumonia etc)
Increased load on the respiratory pump which can push it into fatigue and precipitate secondary pump failure and hypercapnia

Hypoxemic Respiratory Failure (Type 1)
Types of Shunt
1. Anatomical shunt
2. Pulmonary vascular shunt
3. Pulmonary parenchymal shunt

Hypoxemic Respiratory Failure (Type 1)
Common Causes for Shunt
1. Cardiogenic pulmonary edema
2. Non-cardiogenic pulmonary edema (ARDS)
3. Pneumonia
4. Lung hemorrhage
5. Alveolar proteinosis
6. Alveolar cell carcinoma
7. Atelectasis

Causes of increased dead space ventilation
*Pulmonary embolism
*Hypovolemia
*Poor cardiac output, and
*Alveolar over distension.

Ventilatory Capacity versus Demand
Ventilatory capacity is the maximal
spontaneous ventilation that can be
maintained without development of
respiratory muscle fatigue.
Ventilatory demand is the spontaneous minute
ventilation that results in a stable PaCO2.
Normally, ventilatory capacity greatly
exceeds ventilatory demand.

Ventilatory Capacity versus Demand
Respiratory failure may result from either a reduction in ventilatory capacity or an increase in ventilatory demand (or both).
Ventilatory capacity can be decreased by a disease process involving any of the functional components of the respiratory system and its controller. Ventilatory demand is augmented by an increase in minute ventilation and/or an increase in the work of breathing.

Components of Respiratory System
*CNS or Brain Stem *Nerves
*Chest wall (including pleura, diaphragm)
* Airways * Alveolar–capillary units
*Pulmonary circulation

Type 2 ( Ventilatory /Hypercapnic
Respiratory Failure)
Causes of Hypercapnia
1. Increased CO2 production (fever, sepsis, burns, overfeeding)
2. Decreased alveolar ventilation
decreased RR
decreased tidal volume (Vt)
increased dead space (Vd)

Hypercapnic Respiratory Failure
Depressed drive: Drugs, Myxoedema,Brain stem lesions and sleep disordered breathing
Impaired neuromuscular transmision: phrenic nerve injury, cord lesions, neuromuscular blokers, aminoglycosides, Gallian Barre syndrome, myasthenia gravis, amyotrophic lateral sclerosis, botulism
Muscle weakness: fatigue, electrolyte Derangement ,malnutrition , hypoperfusion, myopathy, hypoxaemia
Resistive loads; bronchospasm, airway edema ,secretions scarring ,upper airway obstruction, obstructive sleep apnea
Lung elastic loads:PEEPi, alveolar edema, infection, atelectasis
Chest wall elastic loads:pleural effusion, pneumothorax, flail chest, obesity,ascites,abdominal distension

Why does “V/Q mismatch” cause
hypoxemia?
• Low V/Q units contribute to
hypoxemia
• High V/Q units cannot compensate
for the low V/Q units
• Reason being the shape of the
oxygen dissociation curve which is
not linear

Hypoxic respiratory failure
• Gas exchange failure
• Respiratory drive responds
• Increased drive to breathe
– Increased respiratory rate
– Altered Vd /Vt (increased dead space etc)
– Often stiff lungs (oedema, pneumonia etc)
Increased load on the respiratory pump which can push it into fatigue and precipitate secondary pump failure and hypercapnia

Hypoxemic Respiratory Failure (Type 1)
Types of Shunt
1. Anatomical shunt
2. Pulmonary vascular shunt
3. Pulmonary parenchymal shunt

Hypoxemic Respiratory Failure (Type 1)
Common Causes for Shunt
1. Cardiogenic pulmonary edema
2. Non-cardiogenic pulmonary edema (ARDS)
3. Pneumonia
4. Lung hemorrhage
5. Alveolar proteinosis
6. Alveolar cell carcinoma
7. Atelectasis

Causes of increased dead space
ventilation
*Pulmonary embolism
*Hypovolemia
*Poor cardiac output, and
*Alveolar over distension.

Ventilatory Capacity versus Demand
Ventilatory capacity is the maximal
spontaneous ventilation that can be
maintained without development of
respiratory muscle fatigue.
Ventilatory demand is the spontaneous minute
ventilation that results in a stable PaCO2.
Normally, ventilatory capacity greatly
exceeds ventilatory demand.

Ventilatory Capacity versus Demand
Respiratory failure may result from either a reduction in ventilatory capacity or an increase in ventilatory demand (or both).
Ventilatory capacity can be decreased by a disease process involving any of the functional components of the respiratory system and its controller. Ventilatory demand is augmented by an increase in minute ventilation and/or an increase in the work of breathing.

Components of Respiratory System
*CNS or Brain Stem *Nerves
*Chest wall (including pleura, diaphragm)
* Airways * Alveolar–capillary units
*Pulmonary circulation

Type 2 ( Ventilatory /Hypercapnic
Respiratory Failure)
Causes of Hypercapnia
1. Increased CO2 production (fever, sepsis, burns, overfeeding)
2. Decreased alveolar ventilation
• decreased RR
• decreased tidal volume (Vt)
• increased dead space (Vd)

Hypercapnic Respiratory
Failure
• Depressed drive: Drugs, Myxoedema,Brain stem lesions and sleep disordered breathing
• Impaired neuromuscular transmision: phrenic nerve injury, cord lesions, neuromuscular blokers, aminoglycosides, Gallian Barre syndrome, myasthenia gravis, amyotrophic lateral sclerosis, botulism
• Muscle weakness: fatigue, electrolyte Derangement ,malnutrition , hypoperfusion, myopathy, hypoxaemia
• Resistive loads; bronchospasm, airway edema ,secretions scarring ,upper airway obstruction, obstructive sleep apnea
• Lung elastic loads:PEEPi, alveolar edema, infection, atelectasis
• Chest wall elastic loads:pleural effusion, pneumothorax, flail chest, obesity,ascites,abdominal distension

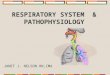
Hypercapnic Respiratory Failure
(PAO2 - PaO2)
Alveolar Hypoventilation
V/Q abnormality
NIF N P0.1
increased normal
N VCO2
PaCO2 >50 mmHg
Not compensation for metabolic alkalosis
Central
Hypoventilation
Neuromuscular
Problem
VCO2
V/Q
Abnormality
Hypermetabolism
Overfeeding
NNIF P0.1

Hypercapnic Respiratory Failure
Alveolar Hypoventilation
Brainstem respiratory depression
Drugs (opiates)
Obesity-hypoventilation syndrome
NIF
Central
Hypoventilation Neuromuscular
Disorder
N NIF
Critical illness polyneuropathy
Critical illness myopathy
Hypophosphatemia
Magnesium depletion
Myasthenia gravis
Guillain-Barre syndrome

NIF (negative inspiratory force). This is a measure
of the patient's respiratory system muscle
strength.
It is obtained by having the patient fully exhale.
Occluding the patient's airway or endotracheal
tube for 20 seconds, then measuring the maximal
pressure the patient can generate upon
inspiration.
NIF's less than -20 to -25 cm H2O suggest that the
patient does not have adequate respiratory muscle
strength to support ventilation on his own.
Evaluation of Hypercapnia

P0.1 max. is an estimate of the patient's respiratory drive.
This measurement of the degree of pressure drop during the first 100 milliseconds of a patient initiated breath. A low P0.1 max suggests that the patient has a low drive and a central hypoventilation syndrome.
Central hypoventilation vs. Neuro-muscular weakness
central = low P0.1 with normal NIF
Neuromuscular weakness = normal P0.1 with low NIF
Evaluation of Hypercapnia

n The P (A—a)O2 ranges from 10 mm Hg in young patients to approximately 25mm Hg in the elderly while breathing room air.
n P (A-a)O2 if greater than >300 on 100% = Shunt < 300 = V/Q mismatch
• RULE OF THUMB
The mean alveolar-to-arterial difference [P(A—a)o2] increases slightly with age and can be estimated ~ by the following equation:
Mean age-specific P(A—a)O2 age/4 + 4
A-a Gradient

Increased Work of Breathing
Work of breathing is due to physiological work and imposed work.
Physiological work involves overcoming the elastic forces during inspiration and overcoming the resistance of the airways and lung tissue
Imposed Work of Breathing In intubated patients, sources of imposed work of breathing include: n the endotracheal tube, n ventilator Circuit n auto-PEEP due to dynamic hyperinflation with airflow obstruction, as is
commonly seen in the patient with COPD. Increased Work of Breathing n Tachypnea is the cardinal sign of increased work of breathing n Overall workload is reflected in the minute volume needed to maintain
normocapnia.

Rationale for ventilatory assistance
Respiratory load
Respiratory muscles
capacity
Alveolar hypoventilation
PaO2 and PaCO2
Abnormal
ventilatory drive

Mechanical ventilation unloads the
respiratory muscles
Respiratory load Respiratory muscles
Mechanical
ventilation