Embed Size (px)
DESCRIPTION
Pathology lecture for medical students. Pathologenesis of COPD,
Citation preview

“Within the mind are all the resources required for successful living. Ideas are present in the consciousness, which when released and given scope to grow and take shape, lead to successful events” - Wings of Fire: An Autobiography of Dr. APJ Abdul Kalam.

“ Whether you think you can or you can't, you are right…!”
– Henry Ford

CPC14: Mrs. PT. 64y Fem. SOB
Mrs. P.T. 64 y female, to ED at TTH. Worsening SOB, years, worst today - At rest• Previously SOB after exertion- COPD. • Gradually worsening over the years, now O2 at night.• Sputum chronic clear white, but light brown today. • Cough - on and off for years, No wheeze, no hemoptysis, • Chest pain worse with breathing today, fever, sweaty.• Smoked 3 packs/day for 35 years; quit 7y ago. Foreign travel: Norfolk Island 3wks. No health problem. RX: Pneumonia, COPD, Emphysema, CCF

CPC: 2011 – 58M Chronic cough. Trevor is 58 year old Caucasian man,
years of coughing. pneumonia 3 years ago; bronchitis several times a year, Dyspnoea, Hoover’s & Campbell sign positive, leans forward for breathing.heavy smoker (30+/day); quit 3 years ago.
• Previous PFT: FEV1 = 1.3 FVC = 2.6 FEV1/FVC = 50%. (too sick to perform PFT today.)
What is the significance of…
1. Leaning forward – “arms on knees”
2. Intercostal in-drawing
3. Hoover's sign ? Tracheal tug ?
4. Campbell's sign ?
1. Pathogenesis of symptoms ?
2. Further questions ?
3. Differential diagnosis ?
4. Learning issues? PFT

Clinical Feature - ? Pathogenesis SOB, Dyspnoea Cough Wheezing, Stridor. Rhonchi, Crackles/ Rales. Dullness Hyper-resonance Hyperventilation Tachypnoea Pleural rub Pleurisy (pleuritis) Sleep apnoea
central/obstructive.
• White sputum (frothy)• Rusty, Yellow, green sputum• Haemoptysis• Night sweats• Sleep apnoea• Kussmaul’s breathing.• Ataxic breathing• Apneustic breathing. • Cheyne-Stokes breathing.• Paradoxical breathing• Resp acidosis / alkalosis.

COPD: Questions What is Chronic Bronchitis & Emphysema ? Pathogenesis of COPD/CB/Emphysema ? Smoking – Disease, Pathogenesis ? Difference.. Obstructive / Restrictive disease ? What findings on PFT expected ? How is he maintaining normal pO2 & pCo2 ? why is he pink & puffing ? What Gross & Microscopic features in his lung ? What complications are expected ? Pneumoconiosis, TB, DPF,

COPD: Questions Bronchiectasis ? Atelectasis ? Lung abscess ? Honeycomb lung ? Pneumothorax ? Tension pneumothorax? Pleural effusion Emphysema types.
• Panacinar - α1AT def.• Paraseptal• Irregular• Bullous• compensatory Text Book:
Robbins Basic Pathology, 8th or 9th edition
• Tuberculosis• Primary, secondary, anergic,
milliary, • caseous, fibrocaseous, fibrosing.• Asthma – types.• Atopic, non-atopic, drugs,
occupational etc.• Pathogenesis, gross, micro• Curschmann spirals, Charcot-
Leyden crystals.• Pneumoconioses• Silicosis, Anthracosis, Asbestosis• IPF – Ideopathic pulm. fibrosis.

Core Learning Issues: Major:
• COPD Pathology – Restrictive / Obstructive.• Emphysema & Bronchitis – types, pathology & clinical.• Pathology of Tobacco related disorders.• PFT - FEV1/FVC & its use and interpretation.• Pneumonia – types & Pathology (Lobar, Broncho & Int.)• Allergic bronchitis, Asthma, Tuberculosis * self study.
Minor:• Pneumoconiosis – Asbestosis, silicosis etc.• Cor pulmonale, Pulmonary hypertension.• Diffuse Pulmonary Fibrosis & honeycomb lung.• Acute lung injury - ARDS, DAD, HMD of infants.• Sarcoidosis ?

The cigarette does the smoking,..!

Normal Lung
Dia
ph
r.
CP a
ngle
Tr.Air Sh
Br. Mar.
CP angle
Gastr
ic a
ir
Colon air


Normal Lung Tissue

LungHistology
Type 1-Pneumocyte
Type 2 Alv. Macro.
RBC-Cap
Type 2
Bronchiole
Alveoli

There is only one secret to staying young, being happy, and
achieving success - You've got to
“enjoy what you do”…!
Including studying pathology…..

Pathology of
COPD, Chronic lung diseases & Pneumonia*
Dr. Shashidhar Venkatesh Murthy.A/Prof. & Head of Pathology

00
0.50.5
1.01.0
1.51.5
2.02.0
2.52.5
3.03.0
Proportion of 1965 Rate Proportion of 1965 Rate
0.0
0.5
1.0
1.5
2.0
2.5
3.0
1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998
–59%–59% –64%–64% –35%–35% +163%+163% –7%–7%
CoronaryHeart
Disease
CoronaryHeart
Disease
StrokeStroke Other CVDOther CVD COPDCOPD All OtherCauses
All OtherCauses
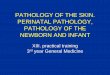
Percent Change in Age-Adjusted Death Rates, U.S., 1965-1998
4th leading cause of death, women more, smoking >80%

Pathology of Smoking Research evidence: smoking disease >4000 chemicals, 43 carcinogens. >90% of COPD is due to smoking. 15% of smokers develop COPD. Injury & inflammation central to damage. Smoking a single cigarette results in an acute
increase in neutrophils at 1 hour. Increased neutrophils in smokers, which
decrease following reduction/quitting. Patients with COPD have sputum neutrophilia
that persists even after cessation of smoking.

Smoking effects: FEV 1 & Age

Smoking related diseases:
Non-neoplastic: • Bronchitis, pneumonia, bronchiectasis.• Chronic bronchitis, emphysema (COPD)• Atherosclerosis IHD, Stroke, MI. • Gastritis, Peptic Ulcer, Oesophagitis.• Arteriosclerosis – Berger’s disease.
Neoplastic:• Lung Cancer (many types)• Oral, laryngeal & oesophageal cancer.• Carcinoma of bladder, Pancreas, cervix, larynx.

Ask, Aspire, Achieve..! …..Ask questions
J. Robin Warren Australian 2005 Nobel price in Medicine - at RCPA conference 2006 Sydney.

Pathogenesis of
COPD
Dr. Shashidhar Venkatesh Murthy.A/Prof. & Head of Pathology

Pathogenesis of COPD
1. Smoke, irritants, carcinogens.
2. Tissue irritation & destruction
3. Inflam Mucous production.
4. Airway damage Narrowing.
5. Alveolar damage widening. Increase in
• Alveolar marcrophages• CD8 Lymphocytes• Neutrophils• Proteases.
Airway inflam Bronchitis Alveoli damage Emphysema. Both COPD.
α1AT def.. Emphysema
Bronchitis Emphysema

The mind is everything. What you think you become! -- Buddha

Pathogenesis – Chronic Bronchitis
3pK-RasC-myc
p53
Irritation COPD Initiation Promotion Ca.
Pathogenesis:1. Smoking – carcinogens2. 3p – tumor suppressor gene loss3. Mutations (p53, KRAS, EGFR..)4. Dysplasia5. Infiltration6. Spread7. Metastases.
Chronic Bronchitis

COPD Pathogenesis: Emphysema

COPD: Overlap of Clinical syndromes
COPD

Both affected COPD (common)

Chronic Bronchitis - Emphysema:
Predominant Bronchitis
Predominant Emphysema
Age (yr) 40-45 50-75Dyspnea Mild; late Severe; earlyCough Early; copious sputum Late; scanty sputumInfections Common OccasionalRespiratory insufficiency
Repeated Terminal
Cor pulmonale Common Rare; terminalAirway resistance
Increased Normal or slightly increased
Elastic recoil Normal LowChest radiograph
Prominent vessels; large heart
Hyperinflation; small heart
Appearance Blue bloater Pink puffer
Both affected COPD (common)

“Know more today about the world than yesterday and lessen the suffering of others. You'd be surprised how far that gets you.”
― Neil deGrasse Tyson

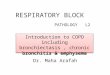
Lung Normal & in Smokers:

Smokers Lung: COPD - Emphysema
Upper lobe – black spots of anthracotic (Co2) pigmentation (centre of each lobule).
Centrilobular alveolar destruction with carbon pigmentation.
Other types: *• Panacinar• Paraseptal• Bullous• Interstitial• Irregular.
C

Normal - Emphysema

Normal Emphysema

Normal - COPD
CB
Emphysema

Centrilobular Emphysema:
Pink Puffer:Lean/weight lossNo cyanosisForward stoopingBarrel chestFlat diaphragmHyperlucent Lung

Whether you think that you can or that you can't,
you are right…!
– Henry Ford

Chronic Bronchitis:
• Squamous Metaplasia.
• mucous gland. Hyperplasia
Normal Chronic Bronchitis

Emphysema: Other types Panacinar
• Congenital, α1AT def. Paraseptal, Bullous
• Old scar. Irregular
• Past diffuse scaring.

Complications of COPD:
1. Pneumothorax, Infections, Bronchectasis.
2. Polycythemia – hypoxia.
3. End-stage lung disease.
4. Acute Exacerbations.
5. Cor Pulmonale – Right heart failure.• syncope, hypoxia, pedal edema, passive
hepatic congestion and death. Lung Cancer
RV LV

Bronchiectasis: Permanent dilatation & Infection of
bronchi. Cough, copious purulent sputum, mixed
infections. Lower lobes common Secondary to COPD, Pneumonia or
localised obstructions. Complications:
• Pneumonia, empyema, septicemia, meningitis.
Types:• Cylindrical, Saccular, Fusiform (no
significance)

Bronchiectasis:
• Permanent dilatation with secondary infection• Pus* filled, *visible bronchi till *periphery.• Abundant, greenish, sputum, mix culture +ve.

COPD Summary: Definition: Progressive Irreversible Chronic airflow
limitation due to inflammatory response to noxious substances. Progressive decrease in PF.
Diagnosis: FEV1<80%, FEV1/FVC <70%
Etiology • >90% smoking (15% of smokers COPD)• Pollution, 1AT def. , genetic susceptibility, Asthma,
idiopathic.
Clinical Syndromes: CB, Emphysema, COPD, Asthma, & Bronchiectasis.
Complications: Pulmonary failure, RS Cardiac failure, Endstage disease, Cancer.

Self Study
- Restrictive Lung Disorders.- IPF, Diffuse fibrosis, - Honeycomb lung.- Pneumoconiosis - Silicosis, Asbestosis, Coal.
- Tuberculosis.- Asthma- Good pasteur’s syndrome.- DAD: ARDS/HMD

Pneumonia: Clinical vignette 50y man, alcoholic, high fever, cough, copious foul
smelling brown sputum, pleuritic rt sided chest pain. HPC: wife reports that he was brought home in a semi-
conscious state a few days ago – drunk. Thin, distressed, pursed lip breathing, using accessory
muscles of respiration, cannot speak in full sentences, leaning forwards…*
39°C, RR-22/min, peripheral cyanosis. Chest-rib in-drawing, diminished air entry, soft expiratory
wheezes, bronchial breathing L lower post chest. PE: fever, consolidation right middle and lower lobes. sputum microscopy - abundant PMN and mixed oral
flora.
Pathogenesis, Differential diagnosis…..?

Pneumonia: Questions What is pneumonia? Types? pathogenesis? Lobar, Broncho & Interstial pneumonia? Community acquired / Nosocomial / hospital acquired
pneumonia ? What is the difference ? Acute, Chronic & recurrent pneumonia? Typical, Atypical pneumonia? Common organisms causing pneumonia? Microbiology – lab diagnosis, culture, tests. Gross and microscopy of pneumonia. Phases of pneumonia – Congestion, Red hepatization, Grey
hepatization, Resolution? Complications of pneumonia? Lipoid pneumonia, Carcinomatous & Aspiration pneumonia ?

Goodpasture Synrome:? Etiology? Clinical? Pathogenesi
s? Diagnosis.

Diffuse Alveolar Damage (DAD):? Etiology? Clinical? Pathogenesis? Diagnosis.
Diffuse bilateral consolidation with honeycombing in both lower lobes, focal in upper lobes.Microscopy: Hyaline membrane in ARDS.

Saddle Thomboemobulus:? Etiology? Clinical? Pathogenesi
s? Diagnosis.

The cigarette does the smoking,..!

Clinical Problem Solving - Course
Free online course from UCSFhttps://class.coursera.org/clinprobsolv-001/class/index
Future of Education…?

Restrictive lung disorders:Definition: Reduced expansion of lung.A. Intrinsic Lung Disorders:
• Sarcoidosis, diffuse fibrosis, pneumoconiosis.• Tuberculosis, Interstitial Pneumonia
B. Extrinsic Disorders (chest wall):• Scoliosis, Kyphosis, Gross Obesity,• Pleurisy, rib fracture etc.
C. Neuromuscular Disorders:• Paralysis of the diaphragm, Myasthenia Gravis,
Poliomyelitis, • Generalized Weakness – malnutrition.

Restrictive Disorders: Pathogenesis Interstitial inflammation
& fibrosis. Lymph+Macrophages.

Idio. Pulm. Fibr.(IPF)>50y, ?viral, ?Imm ?Env "dry Velcro like inspiratory
crackles.UIP (usual Int. Pneum) /
Cryptogenic fibrosing alveolitis.Bilateral, lower and peripheral
coarse reticulonodular shadowing and small lungs.
CT – Peripheral honeycomb & scarring.
Poor prognosis. (~3years)

Idiopathic Pulmonary Fibrosis: UIP/IFA
Type 2 Pneum

Pneumoconioses: Disease due to inhaled dusts inorganic (mineral) or organic Reaction may be inert, fibrous,
allergic or neoplastic. Morphologic Types: Inert - coal-worker's pneum. Fibrous - asbestosis, silicosis Allergic - extrinsic allergic
alveolitis (Bird Neoplastic - mesothelioma, lung
carcinoma.

Silicosis: Inorganic – sand &
stone dust. Toxic to macrophages –
destruction fibrosis. Scattered multiple
small,fibrotic Nodules Surrounding Irregular
emphysema. Restrictive pattern of
PFT.

Asbestosis: Asbestos bodies in sputum.
• (Protein & Hemosiderin)
“Inconsumable”, Beaded 5-100mm x 0.25mm.
Within alveoli at lung bases. Dyspnoea, dry cough Clubbing is common. Diffuse fibrosis: Honey comb
lung: Massive fibrosis: Coal-miners.

Coal Miner’s Lung: Athraco-Silicosis: Dense cardon
pigmentation – Anthracosis and nodules of silicosis.
Commonly seen in coal miners.

Sarcoidosis: Granulomatous, immune,
multisystem, ??? Etiology. Multiple fine nodules. Like TB (no caseation). Smokers – Uncommon SOB, Erythema nodosum,
lymphadenopathy, hypercalcemia, nephrocalcinosis, occular, skin & nerve damage.. Etc.
Stage I asymptomatic to Stage IV – Pulm fibrosis.

Tuberculosis: Mycobacterium tuberculosis (typical) Atypical mycobacteria – HIV Primary & Secondary, Pulm/non-pulm Chronic, Hypersensitivity, debilitating,
weight loss. Upperlobe, nodular/cavity/fibrosing. Pleural effusion Caseating Granuloma
• lymph, marcrophages fibrosis Macrophages - LH giant cells.
Systemic spread, miliary spread. Tuberculin Test – hypersensitivity.

Restrictive vs Obstructive
Interstitial - (stiff lung)Increased tissue Relatively normal FEV1:FVC ratio
Normal PEFR. Types:Acute – ARDS,Viral.Chronic - pneumoconioses & sarcoidosis, Int. fibrosis.
Obstructive (soft lung)Destruction of tissue.Low FEV1:VC ratio
Low PEFR.Types:
•Localised & Diffuse•Reversible & progressive.•COPD •Asthma•Bronchiectasis,

Pulmonary Function Testing: FVC - Forced Vital Capacity – Liters - diagnosis of obstructive and
restrictive diseases. FEV1 - Forced Expiratory Volume in One Second –
obstructive/restrictive diseases. FEV1/FVC - FEV1 Percent (FEV1%) - it indicates what percentage
of the total FVC was expelled from the lungs during the first second of forced exhalation. critically important in differentiating obstructive from restrictive diseases.
FEV3 - Forced Expiratory Volume in Three Seconds – equal to FVC in normal.
FEV3/FVC - FEV3% - normal is 1 or 100% PEFR - Peak Expiratory Flow Rate - this is maximum flow rate
achieved by the patient. For monitoring response to treatment. FEF - Forced Expiratory Flow - is a measure of how much air can
be expired from the lungs (liters/second or liters/minute). The FVC expiratory curve is divided into quartiles and therefore there is a FEF that exists for each quartile. The quartiles are expressed as FEF25%, FEF50%, and FEF75% of FVC.

PFT: interpretation: Check FVC & FEV1 – normal normal PFT If FVC and/or FEV1 are low - Pathology. Check FEV1/FVC ratio: FEV1/FVC% (<70%) - Obstructive. FEV1 /FEVC% (>80%)- Restrictive. An improvement in FEV1 of 200ml or more after
bronchodilator suggests versibility Asthma.

“A person with belief never grovels before anyone, whining and whimpering that it’s all too much, that he lacks support, that he is being treated unfairly. Instead, such a person tackles problems head on and then affirms, I am greater than anything that can happen to me.”
- Wings of Fire: An Autobiography of Dr. APJ Abdul Kalam.

Asthma: Reversible & intermittent COPD
Increased irritability of bronchi causes bronchospasm
Paroxysmal attacks Hyper inflated lungs Mucus plugs in bronchi Enlarged bronchial mucous glands

Asthma Types: Atopic – Immune, hypersensitivity, IgE. Non-atopic – Non immune - infections Aspirin-induced – Genetic, excess cyclo-
oxygenase inhibition. Occupational – Immune, hypersensitivity. Allergic bronchopulmonary aspergillosis:
Hypersensitivity to inhalation of spores.

Asthma Pathogenetic Types:
Extrinsic (Immune)• Atopic - IgE• Occupational - IgG• A. Bronchopulomonary Aspergillosis - IgE
Intrinsic (Non immune)• Aspirin induced• Infections induced• Excercise

Asthma: Reversible & intermittent obstruction
Hyperresponsive airways• Increased irritability of bronchi causes
bronchospasm Episodic attacks Inflammation Excessive and thick mucus plugs Hyperplasia of mucous glands and smooth
muscle, minimal fibrosis

Asthma Types: Atopic – Immune, hypersensitivity. Non-atopic – Non immune - infections Aspirin-induced – Genetic hypersensitivity. Exercise induced Occupational – Immune, hypersensitivity. Allergic bronchopulmonary aspergillosis:
Hypersensitivity to inhaled aspergillus Ag

Asthma Pathogenetic Types:
Extrinsic (Immune)• Atopic - IgE• Occupational - IgG• A. Bronchopulomonary Aspergillosis - IgE
Intrinsic (Non immune)• Aspirin induced• Infections induced• Excercise

INFLAMMATIONAirflow Limitation
SYMPTOMSCough Wheeze
Dyspnoea
TRIGGERS Allergens, Exercise,
Cold Air, SO2 Particulates
Asthma Pathogenesis:
AirwayHyper-responsiveness
Genetic*
INDUCERSAllergens,Chemical sensitisers,Air pollutants, Virus infections
Hygiene hypothesis?

Asthma : Pathogenesis
Early phase (immediate) and late phase reactions

Asthma Pathology:
Barnes PJ
Allergen
MucushypersecretionHyperplasia
VasodilatationNew vessels
Plasma leak Oedema
BronchoconstrictionHypertrophy/hyperplasia
Cholinergic reflex
Subepithelialfibrosis
Sensory nerve activation
Eosinophil
Mast cell
Th2 cell Neutrophil
Macrophage/dendritic cell
Mucus plugEpithelial shedding
Nerve activation
LeukotrienesC4, D4 & E4
LeukotrienesAchHistamineProstaglandin DPlatelet activating factorInterleukins

Asthma Morphology: Bronchial obstruction with overinflation
• Small areas of atelectasis (collapse) may be seen
Inflammation & thickening of mucosa. Bronchial wall smooth muscle hypertrophy Thickening of bronchial basement membrane. Mucus plugging of bronchi Curschmann spirals: whorls of shed epithelium
within mucus plugs Charcot-Leyden crystals: Within aggregates of
eosinophils – crystalloids of galectin-10

Asthma Morphology:
Asthma Microscopy1.Mucous Plugs +eosinophils2.Goblet cell hyperplasia3.Inflammation + Eosinophils4.Smooth muscle hyperplasia5.Mucous gl. Hyperplasia.

Asthma – Lung Gross features: Inflamed thick bronchi obstructed by mucous plugs.

Asthma : Microscopy
Inflammed bronchi
Obstruction by mucous plug
Alveoli (normal)

Asthma : Microscopy
Dilated BV Inflammatory cellsCartilageMucous plug over
the surface.

Asthma : Microscopy

Hyperinflation Status Asthmaticus:

Status Asthmaticus : Mucous plug

Status Asthmaticus : Mucous plug

Curschmann spirals:

Charcot-Leyden Crystals:

“ Whether you think you can or you can't, you are right…!”
– Henry Ford

Lung volumes

Total Lung Capacity (TLC) - the total volume of the lung, the volume of air contained in the lung at the end of maximal inspiration
Inspiratory Reserve Volume (IRV) - volume, which can be inspired beyond a restful inspiration
Tidal Volume (TV) – volume of a single breath, usually at rest Functional Residual Capacity (FRC) - The amount of air left in the lungs
after a tidal breath out, the amount of air that stays in the lungs during normal breathing
Vital Capacity (VC) – maximum volume which can be ventilated in a single breath
Inspiratory Capacity (IC) - the maximal volume that can be inspired following a normal expiration
Expiratory Reserve Volume (ERV) – volume, which can be expired beyond a restful expiration
Residual Volume (RV) – volume remaining in the lungs after a maximum expiration

Volumes
Forced Vital Capacity (FVC) - the volume of air that can forcibly be blown out after full inspiration, measured in litres
Forced Expiratory Volume in 1 Second (FEV1) - the maximum volume of air that can forcibly blow out in the first second during the FVC manoeuvre, measured in liters
FEV1/FVC (FEV1%) - in healthy adults this should be approximately 75–80%.
• Obstructive diseases (asthma, COPD) FEV1 is ↓ & FVC n/↑ so FEV1/FVC is decreased (<80%, often ~45%).
• In restrictive diseases (Lung fibrosis/silicosis) FEV1 and FVC are both reduced proportionally and the FEV1/FVC value may be normal or even increased as a result of decreased lung compliance

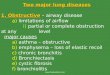
Obstructive lung diseases airway obstruction restricted expiration FEV1, FEV1/FVC compliance, elasticity
Chronic bronchitis• Bronchiolitis
Asthma Emphysema Bronchiectasia Cystic fibrosis
Normal
Asthma
COPD

Flow volume curves

Condition Major changes Causes Symptoms
Chronic Hyperplasia Tobacco smoking Productivebronchitis and hypersecretion and air pollutants cough of mucus glands
Bronchiectasis Dilation and scarring Persistent severe Cough, purulent of airways infections
sputum and fever
Asthma Smooth muscle Immunologic Episodic wheezing
hyperplasia or idiopathic cough and dyspnea
Excessive mucusInflammation
Emphysema Airspace enlargement Tobacco smoking Dyspnea Genetic and wall
destruction

Bronchogenic Carcinoma:

Asthma pathogenesis:

Pathophysiology of Cor-Pulmonale:

2013 feedback Did not go well - reorganize talk. No Asthma, restrictive disorders &
pneumonia – next week. Check quiz – remove unwanted. Next year combine pneumonia + COPD.