Embed Size (px)
Citation preview

by
Scott Cerreta, BS, RRT
Director of Education
www.copdfoundation.org
COPD Pathology with3D Interactive
COPD: Change in Definition
• COPD used to include 5 disease processes1
1 Chronic Bronchitis
2 Emphysema
3 Asthma
4 Bronchiectasis
5 Cystic fibrosis & fibrosis from Tb
• Differential diagnosis separates 3 to 5
COPD: Definitions of 21st Century1
• Preventable and treatable
• Airflow limitation that is not fully reversible
• Progressive disease
• Abnormal inflammatory response of the lungs
• Subsets of patients
Chronic bronchitis Emphysema
Asthma
COPDCOPDDC
COPD Includes Chronic Bronchitis2
• Productive cough for 3 months in 2 consecutive years with intermittent wheezing and variable degrees of recurring dyspnea on exertion
• Inflammation of cells that line the bronchus resulting in excess sputum
• Mucous glands enlarge and bronchial walls thicken, resulting in a deformed and narrow airway lumen

COPD Includes Emphysema2
• Abnormal permanent enlargement of the airspaces distal to the terminal bronchioles, accompanied by destruction of their walls and without obvious fibrosis.
• Destruction occurs in the alveoli and the orderly appearance of the acinus is disturbed.
• Normal elasticity is lost, air becomes trapped in over-inflated lungs.
COPD: Airway Effects7
Normal Emphysema
Structural changes of Emphysema10 Pathology, Pathogenesis, & Pathophysiology
• Pathology– Characteristics and effects of COPD
• Pathogenesis– Origin and cause of COPD
• Pathophysiology– Biologic and physical manifestations of COPD
• Processes within the body that result in signs and symptoms

COPD: Anatomy Review
Divisions of lower respiratory tract1. Trachea – cartilage; conducting airway
2. Mainstem bronchi – ß2 smooth muscle; conducting airway
3. Secondary bronchi – ß2 smooth muscle; conducting airway
4. Tertiary bronchi – ß2 smooth muscle; conducting airway
5. Bronchioles – ß2 smooth muscle; conducting airway
6. Terminal bronchioles – ß2 smooth muscle; conducting airway
7. Respiratory bronchioles – gas exchange starts here
8. Alveoli – gas exchange; septa are alveolar walls
COPD: Pathology
COPD Compromises Four Compartments of the Lung
1. Central airways – cartilaginous >2mm diameter
• Bronchial glands hypertrophy – increased sputum production
• Airway epithelium metaplasia changes – loss of cilia and cilliary
dysfunction, increased smooth muscle and connective tissue
• Inflammatory cells predominate – lymphocytes (CD8+),
neutrophils, and macrophages
COPD: Pathology
COPD Compromises Four Compartments of the Lung
2. Peripheral airways – non-cartilaginous < 2mm diameter
• Bronchiolitis present in early stages of COPD
• Increased number of goblet cells and epethilial metaplasia
• Inflammatory cells predominate – lymphocytes (CD8+),
neutrophils, and macrophages
• Advanced disease reveals fibrosis and more collagen in walls
Cigarette smoke
(and other irritants)
PROTEASES Neutrophil elastaseCathepsinsMMPs
Alveolar wall destructionveolar wall destruct(Emphysema)
Mucus hypersecretion
CD8+
lymphocyte
Alveolar macrophageEpithelialcells
Fibrosis
(Obstructivebronchiolitis)
Fibroblast
MonocyteNeutrophil
Chemotactic factors
Source: Peter J. Barnes, MD
Inflammatory Cells Involved in COPD10

COPD: Pathology1
COPD Compromises Four Compartments of the Lung
3. Lung parenchyma – respiratory bronchioles, alveoli, and
capillaries
• Emphysema – enlargement of air spaces distal to terminal
bronchioles, Two types
1. Centrolobular – dilation and destruction of respiratory bronchioles
2. Panlobular – destruction of entire acinus, Alpha1-antitrypisin
• Loss of alveolar attachments – airway collapse
• Inflammation similar to previous
• Development of bullae
Alveolar wall destruction
Loss of elasticity
Destruction of pulmonary
capillary bed
↑ Inflammatory cells
macrophages, CD8+ lymphocytes
Source: Peter J. Barnes, MD
Changes in the Lung Parenchyma in COPD Patients10
COPD: Pathology1
COPD Compromises Four Compartments of the Lung
4. Pulmonary vasculature
• Begins early in disease
• Vessel wall thickening and endothelial dysfunction
• Increased vascular smooth muscle tone
• Infiltration of vessel wall with CD8+ and T lymphocytes
• Advanced stages – develop collagen deposition and capillary
bed destruction leading to pulmonary hypertension and cor-
pulmonale
Endothelial dysfunction
Intimal hyperplasia
Smooth muscle hyperplasia
↑ Inflammatory cells
(macrophages, CD8+ lymphocytes)
Source: Peter J. Barnes, MD
Changes in Pulmonary Arteries in COPD Patients10

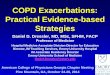
COPD: Key Concept
Not everyone that smokes gets
COPD
Age (years)25 35 45 55 65
4
3
2
1
0
Disability
Death
Nonsmoker
Average
smoker
“Susceptible”
smoker
FE
V1 (
lite
rs)
70 75
Susceptible Smokers & COPD14
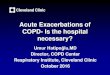
10-15ml/yr
15-25ml/yr
40-80ml/yr
0 1 2 3 4 5 6 7 8 10 119
2.8
2.6
2.4
2.2
2.0
FE
V1, lit
ers
3 4 5 6 7 8
Years of followup
Sustained quitters
Continuous smokers
Anthonisen et al, AJRCCM, 2002
COPD: Benefits of Smoking Cessation Lung Health Study
Age (years)25 35 45 55 65
4
3
2
1
0
Disability
Death
Nonsmoker
Average
smoker
“Susceptible”
smoker
FE
V1 (
lite
rs)
70 75
Susceptible Smokers & COPD14

COPD: Pathogenesis1
• Tobacco smoking is the main risk factor for COPD
• Some smokers display an exaggerated protected inflammatory response, which causes tissue destruction, impairs defense and repair mechanisms, thus leading to characteristics of COPD
COPD: Pathogenesis1
Three processes important to Pathogenesis
1. Inflammation cascade
• Differs from bronchial asthma cascade
2. Proteinase and antiprotease imbalance
• Released by inflammatory cells
3. Oxidative Stress
• Oxidizing biological molecules leads to cell
dysfunction and/or death
LUNG INFLAMMATION
COPD PATHOLOGY
Oxidative
stressProteinases
Repair
mechanisms
Anti-proteinasesAnti-oxidants
Host factors
Amplifying mechanisms
Cigarette smokeBiomass particles
Particulates
Source: Peter J. Barnes, MD
COPD: Pathogenesis10
COPD
Macrophages
PMNs
CD8 T cells
proteases
LTB4
IL-8, TNF-a
Asthma
Eosinophils
Mast cells
CD4 T cells
mediators
LTD4
IL-4, IL-5, Il-13
Inflammation in Asthma & COPD1

COPD: Pathophysiology1
Pathogenic mechanisms produce pathological changes, giving rise to four physiological abnormalities in COPD
1. Mucous hypersecretion and ciliary dysfunction
• First physiologic abnormality developed in COPD
• Enlarged mucous glands and epithelial cell metaplasia
Mucus gland hyperplasia
Goblet cell
hyperplasia
Mucus hypersecretion Neutrophils in sputum
Squamous metaplasia of epithelium
↑ Macrophages
No basement membrane thickening
Little increase in
airway smooth muscle
↑ CD8+ lymphocytes
Source: Peter J. Barnes, MD
Changes in Large Airways of COPD Patients10
COPD: Pathophysiology1
2. Airflow limitation and hyperinflation
• Expiratory (largely irreversible) airflow limitation
– Physiologic hallmark of COPD
• Major site is smaller conducting airways <2mm
• Loss of elastic recoil due to alveolar wall destruction
• Destruction of alveolar attachments
• Accumulation of inflammatory cells, mucous and plasma exudate in the bronchi
• Smooth muscle contraction (tense vagal tone) and dynamic hyperinflation during exercise
– Major factor affecting exercise limitation in patients
COPD: Pathophysiology1
3. Gas exchange abnormalities
• Occurs in advanced COPD characterized by hypoxemia with or without hypercapnia
• Abnormal gas exchange as a result of anatomical alterations as described previously
4. Pulmonary hypertension
• Occurs after severe gas exchange abnormalities
• Results from hypoxic vasoconstriction, endothelial dysfunction, remodeling of pulmonary arteries and destruction of capillary bed
• Leads to right sided heart failure – cor pulmonale

Chronic hypoxia
Pulmonary vasoconstriction
Muscularization
Intimal hyperplasia
Fibrosis
Obliteration
Pulmonary hypertension
Cor pulmonale
Death
Edema
Source: Peter J. Barnes, MD
Chronic hypoxia
Pulmonary Hypertension in COPD10 Only Two Things Clinically Proven to Prolong Life for COPD Patients
1. Quitting Tobacco
2. LTOT only for those who qualify
Pro-Active vs. Passive Referral
1-800
• Fax Referral System
• 50% enrollment rate
• 35-45% abstinence at 6mos
• 25-35% abstinence at 1 year
• Results = 20 @ 6mos / 15@yr
• Leaving it up to the individual
to call when ready
• According to research
conducted at San Diego State
University only 3% of clients
receiving literature containing
quit line information made a
call to the quit line
• Results = 1.2 @ 6mos / 1@yr
Pro-Active vs. Passive Referral

QuitFax Referral Form – Quick and Easy!
ASHLine 1-800-55-66-222
www.ashline.org
National Quit Line
1-800-Quit Now
COPD: Treatment & Management10
Four Components of Care
1. Assess and monitor disease• Spirometry is the tool
2. Reduce risk factors
3. Manage stable COPD• Pharmacologic and non-pharmacologic
4. Manage acute exacerbations• Steroids, antibiotics, ventilation support
FEV1 / FVC < 70%
I: MildFEV1>80% pred
II:ModerateFEV1 50-80% pred
III: SevereFEV1 30-50% pred
IV: Very SevereFEV1 < 30% pred
Avoidance of risk factor(s); influenza vaccination
Add short-acting bronchodilator when needed: ß2 agonists
Add regular treatment with one or more long-acting bronchodilators: ß2 agonists and anticholinergics
Add rehabilitation
Add ICS for repeated exacerbations
Add LTOT
Surgical interventions
GOLD Standards COPD Pharmacotherapy9 Manage Exacerbations: Introduction1
• An exacerbation of COPD is an event in the natural course of the disease characterized by a sudden change in the patients baseline symptoms: dyspnea, cough, and/or sputum that is beyond normal day-to-day variations
• May warrant a change in regular medication usage

COPD Exacerbations: Epidemiology
• Exacerbations play a role in decline of FEV1
– Decline in FEV1 of 46.1 ml/yr with frequent (>1.5) exacerbations per year
– Decline in FEV1 of 25.3 ml/yr with infrequent (<1.5) exacerbations per year
– Greater lung function decline value observed in COPD exacerbations amongst current smokers
Donaldson et al, Thorax 2002;57;847-52)
COPD Exacerbations: Epidemiology1
• Seasonality
– 50% more likely in the winter
• Recurrent Exacerbations
– 30% of those hospitalized have another
exacerbation within 8 weeks
COPD Exacerbations: Epidemiology8
• The most common causes are:– Infection of the tracheobronchial tree
– Air pollution
• Cause of 1/3 of severe exacerbations unknown
• Conditions that mimic exacerbations: pneumonia, CHF, PE, pneumothorax, pleural effusions, arrhythmia– Important to Differential Diagnosis
WORLD COPD DAYNovember 16, 2011
Raising COPD Awareness Worldwide

Interactive COPD Education System
Click to Launch the
COPD Active Learning Module
This interactive module is provided by Syandus, Inc.
References
1. American Thoracic Society – European Respiratory Society: Standards for the Diagnosis and Management of Patients with COPD, 2004. download manual:
http://www.thoracic.org/sections/copd
2. Arizona Department of Health Services: Arizona Comprehensive Lung Disease Control Plan, download manual: http://www.azdhs.gov/phs/tepp/pdf/lungdiseaseplan.pdf
3. National Heart Lung and Blood Institute, COPD Learn More Breathe Better: COPD: It has a Name, 2007. download provider edition:
http://www.nhlbi.nih.gov/health/public/lung/copd/campaign-materials/index.htm
4. National Heart Lung and Blood Institute, COPD Learn More Breathe Better: COPD: It has a Name, 2007. download consumer edition:
http://www.nhlbi.nih.gov/health/public/lung/copd/campaign-materials/index.htm
5. National Heart Lung and Blood Institute, COPD Learn More Breathe Better: COPD: Are You at Risk, 2007. download handout:
http://www.nhlbi.nih.gov/health/public/lung/copd/campaign-materials/index.htm
6. National Heart Lung and Blood Institute, COPD Learn More Breathe Better: Breathing Better with a COPD Diagnosis, 2007. download handout:
http://www.nhlbi.nih.gov/health/public/lung/copd/campaign-materials/index.htm
References
7. National Lung Health Education Program: Prevent COPD Now! Information for Patients Who May Be Developing COPD, 2007. download Save Your Breath, America!:
http://www.nlhep.org/pdfs/saveyourbreath.pdf
8. Global Initiative for Chronic Lung Disease, Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: Executive Summary, 2006. download manual: http://www.goldcopd.com/Guidelineitem.asp?l1=2&l2=1&intId=996
9. Global Initiative for Chronic Lung Disease, Pocket Guide to COPD Diagnosis, Management, and Prevention: A Guide for Health Care Professionals, 2006. download manual:
http://www.goldcopd.org/Guidelineitem.asp?l1=2&l2=1&intId=1116
10. Global Initiative for Chronic Lung Disease, Power Point Presentation with NHLBI diagrams by: Peter J. Barnes, M.D., 2006. download manual:
http://www.goldcopd.com/OtherResourcesItem.asp?l1=2&l2=2&intId=969
11. National Lung Health Education Program and AlphaMedia, Inc., Simple Office Spirometry, Thomas L. Petty, M.D., and Paul L. Enright, M.D., download manual:
http://www.ndd.ch/Downloads/Docs/Petty-Enright-SimpleOfficeSpirometryForPrimaryCarePractitioners.pdf
12. American Thoracic Society – European Respiratory Society: Standards for the Diagnosis and Management of Individuals with Alpha-1 Antitrypsin Deficiency, 2006. download manual:
http://www.thoracic.org/sections/publications/statements/pages/respiratory-disease-adults/alpha1.html
References
13. Rau JL: Respiratory Care Pharmacology, Mosby, 2002.
14. American Lung Association of Minnesota, COPD Educator Course, 2006. Cheryl Sasse; Jeff Rubins, MD; Kathy Schultz, RRT; Charles McArthur, RRT, RPFT; Janet Malkiewicz, RN, PHN; Lynn Sieben, RRT; Dick Stenholz LSW; Bob McVoy, RRT, FAARC; Charlene McEvoy, MD
15. Arizona Department of Health Services, Tobacco Education & Prevention Program, University of Arizona HealthCare Partnership, Basic Tobacco Intervention Skills Certification Guidebook, 2006.
Medical Reviewer: Dr. David R. Sanderson, M.D., Professor of Medicine: Emeritus Mayo Clinic College of Medicine