Embed Size (px)
Citation preview

PARANEOPLASTIC
SYNDROMES
Dr. ABHILASH GAVARRAJU
JR-II

Introduction Group of clinical disorders associated with
malignant diseases that are not directly related to the physical effects of the primary or metastatic tumor.
The syndromes may be due to
- Tumor production of substances causing distant symptoms
- Depletion of normal substances
- Host response to the tumor
Successful treatment leads to disappearance of syndrome but many do not predictably resolve with treatment
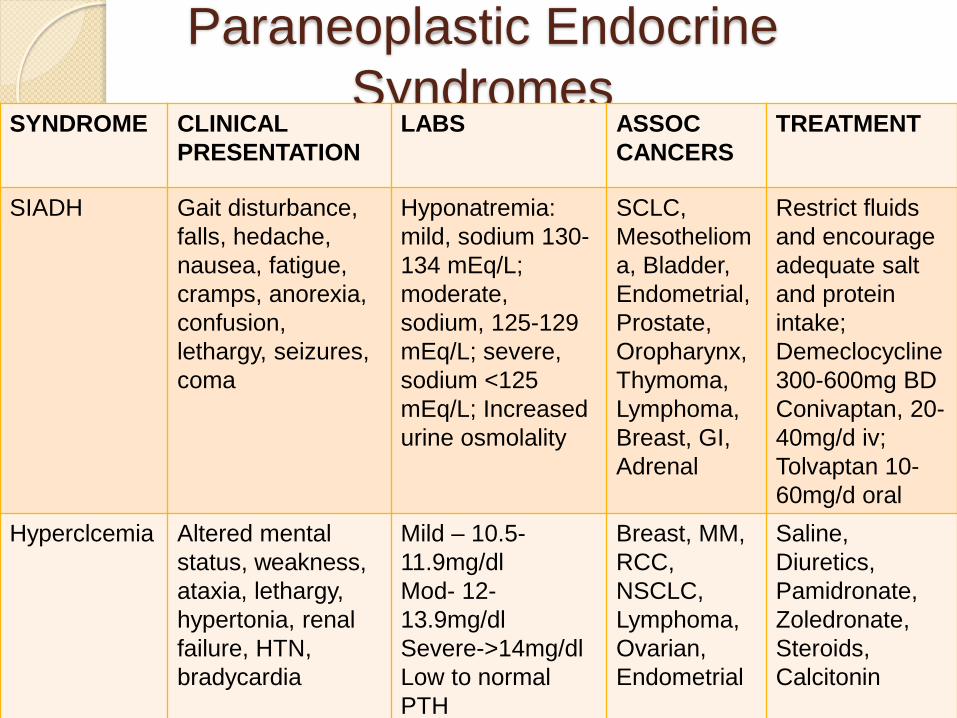
Paraneoplastic Endocrine
SyndromesSYNDROME CLINICAL
PRESENTATION
LABS ASSOC
CANCERS
TREATMENT
SIADH Gait disturbance,
falls, hedache,
nausea, fatigue,
cramps, anorexia,
confusion,
lethargy, seizures,
coma
Hyponatremia:
mild, sodium 130-
134 mEq/L;
moderate,
sodium, 125-129
mEq/L; severe,
sodium <125
mEq/L; Increased
urine osmolality
SCLC,
Mesotheliom
a, Bladder,
Endometrial,
Prostate,
Oropharynx,
Thymoma,
Lymphoma,
Breast, GI,
Adrenal
Restrict fluids
and encourage
adequate salt
and protein
intake;
Demeclocycline
300-600mg BD
Conivaptan, 20-
40mg/d iv;
Tolvaptan 10-
60mg/d oral
Hyperclcemia Altered mental
status, weakness,
ataxia, lethargy,
hypertonia, renal
failure, HTN,
bradycardia
Mild – 10.5-
11.9mg/dl
Mod- 12-
13.9mg/dl
Severe->14mg/dl
Low to normal
PTH
Breast, MM,
RCC,
NSCLC,
Lymphoma,
Ovarian,
Endometrial
Saline,
Diuretics,
Pamidronate,
Zoledronate,
Steroids,
Calcitonin
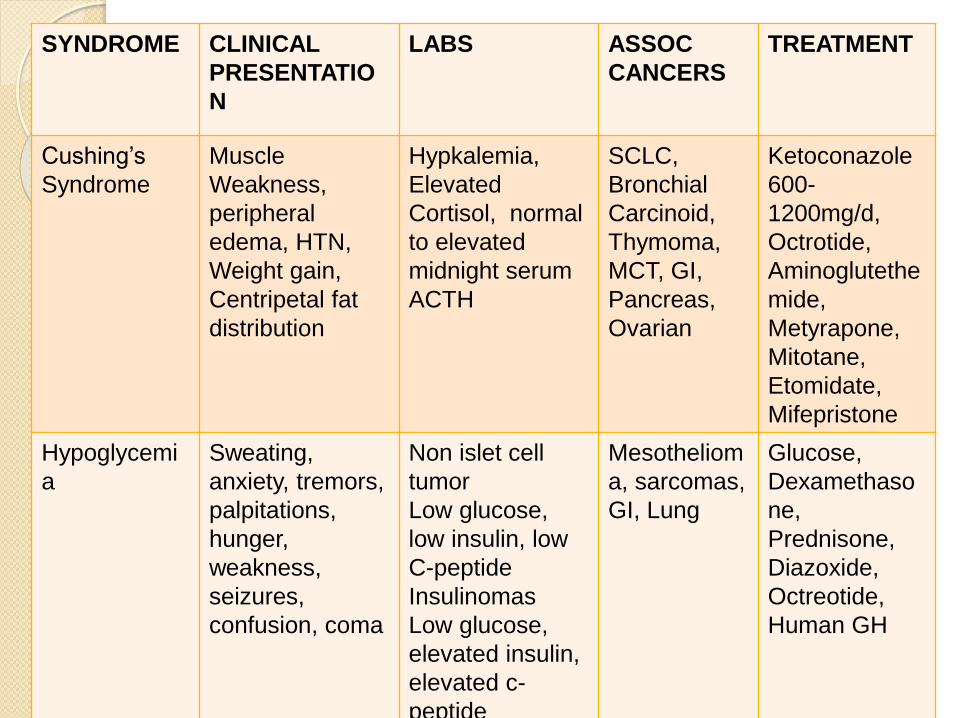
SYNDROME CLINICAL
PRESENTATIO
N
LABS ASSOC
CANCERS
TREATMENT
Cushing’s
Syndrome
Muscle
Weakness,
peripheral
edema, HTN,
Weight gain,
Centripetal fat
distribution
Hypkalemia,
Elevated
Cortisol, normal
to elevated
midnight serum
ACTH
SCLC,
Bronchial
Carcinoid,
Thymoma,
MCT, GI,
Pancreas,
Ovarian
Ketoconazole
600-
1200mg/d,
Octrotide,
Aminoglutethe
mide,
Metyrapone,
Mitotane,
Etomidate,
Mifepristone
Hypoglycemi
a
Sweating,
anxiety, tremors,
palpitations,
hunger,
weakness,
seizures,
confusion, coma
Non islet cell
tumor
Low glucose,
low insulin, low
C-peptide
Insulinomas
Low glucose,
elevated insulin,
elevated c-
peptide
Mesotheliom
a, sarcomas,
GI, Lung
Glucose,
Dexamethaso
ne,
Prednisone,
Diazoxide,
Octreotide,
Human GH
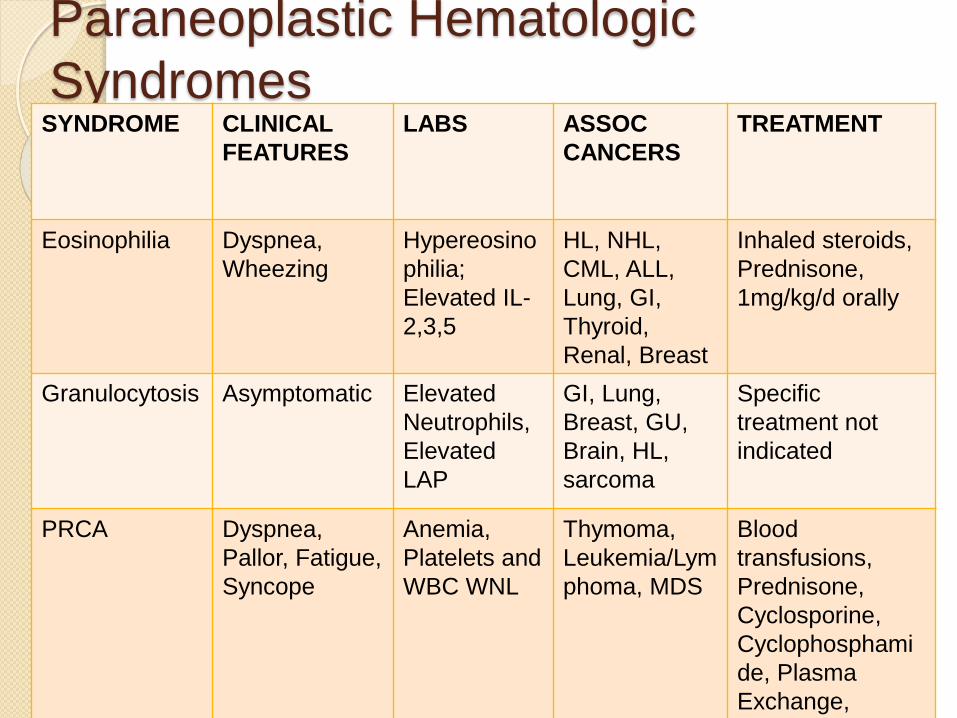
Paraneoplastic Hematologic
SyndromesSYNDROME CLINICAL
FEATURES
LABS ASSOC
CANCERS
TREATMENT
Eosinophilia Dyspnea,
Wheezing
Hypereosino
philia;
Elevated IL-
2,3,5
HL, NHL,
CML, ALL,
Lung, GI,
Thyroid,
Renal, Breast
Inhaled steroids,
Prednisone,
1mg/kg/d orally
Granulocytosis Asymptomatic Elevated
Neutrophils,
Elevated
LAP
GI, Lung,
Breast, GU,
Brain, HL,
sarcoma
Specific
treatment not
indicated
PRCA Dyspnea,
Pallor, Fatigue,
Syncope
Anemia,
Platelets and
WBC WNL
Thymoma,
Leukemia/Lym
phoma, MDS
Blood
transfusions,
Prednisone,
Cyclosporine,
Cyclophosphami
de, Plasma
Exchange,
Splenectomy
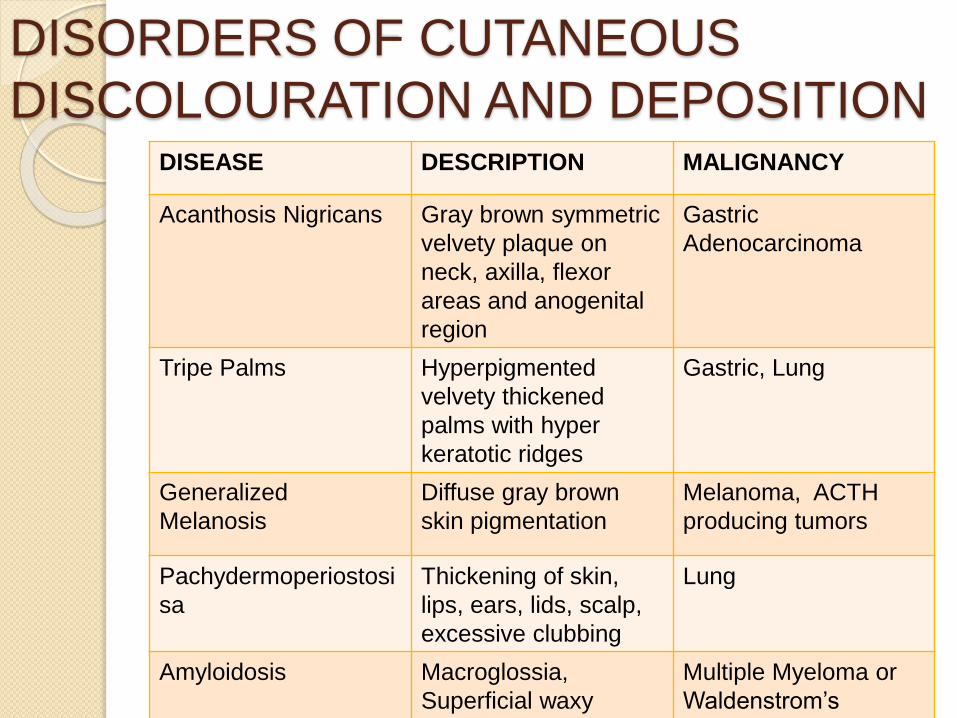
DISORDERS OF CUTANEOUS
DISCOLOURATION AND DEPOSITIONDISEASE DESCRIPTION MALIGNANCY
Acanthosis Nigricans Gray brown symmetric
velvety plaque on
neck, axilla, flexor
areas and anogenital
region
Gastric
Adenocarcinoma
Tripe Palms Hyperpigmented
velvety thickened
palms with hyper
keratotic ridges
Gastric, Lung
Generalized
Melanosis
Diffuse gray brown
skin pigmentation
Melanoma, ACTH
producing tumors
Pachydermoperiostosi
sa
Thickening of skin,
lips, ears, lids, scalp,
excessive clubbing
Lung
Amyloidosis Macroglossia,
Superficial waxy
yellow and pink
Multiple Myeloma or
Waldenstrom’s
Macroglobulinemia

Cutaneous Manifestations of
Cancer They may precede, be concurrent
with, or follow the discovery of the
underlying malignancy.
Appropriate Systematic Evaluation
A TRUE paraneoplastic process
satisfies two criteria : Strong
association of dermatoses with
malignancy and its parallel course
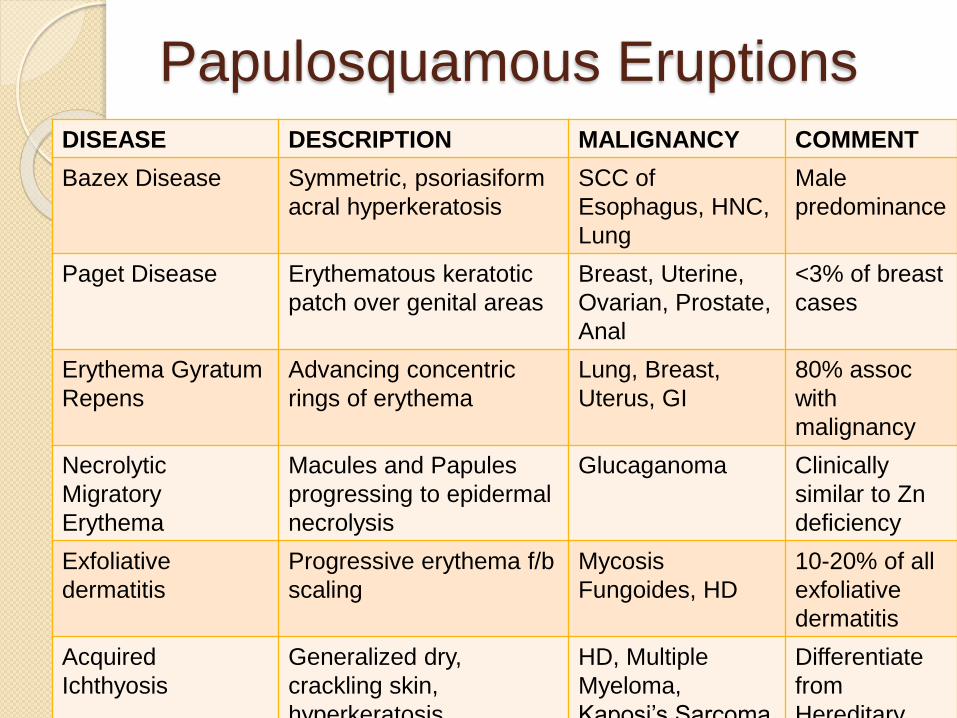
Papulosquamous EruptionsDISEASE DESCRIPTION MALIGNANCY COMMENT
Bazex Disease Symmetric, psoriasiform
acral hyperkeratosis
SCC of
Esophagus, HNC,
Lung
Male
predominance
Paget Disease Erythematous keratotic
patch over genital areas
Breast, Uterine,
Ovarian, Prostate,
Anal
<3% of breast
cases
Erythema Gyratum
Repens
Advancing concentric
rings of erythema
Lung, Breast,
Uterus, GI
80% assoc
with
malignancy
Necrolytic
Migratory
Erythema
Macules and Papules
progressing to epidermal
necrolysis
Glucaganoma Clinically
similar to Zn
deficiency
Exfoliative
dermatitis
Progressive erythema f/b
scaling
Mycosis
Fungoides, HD
10-20% of all
exfoliative
dermatitis
Acquired
Ichthyosis
Generalized dry,
crackling skin,
hyperkeratosis
HD, Multiple
Myeloma,
Kaposi’s Sarcoma
Differentiate
from
Hereditary

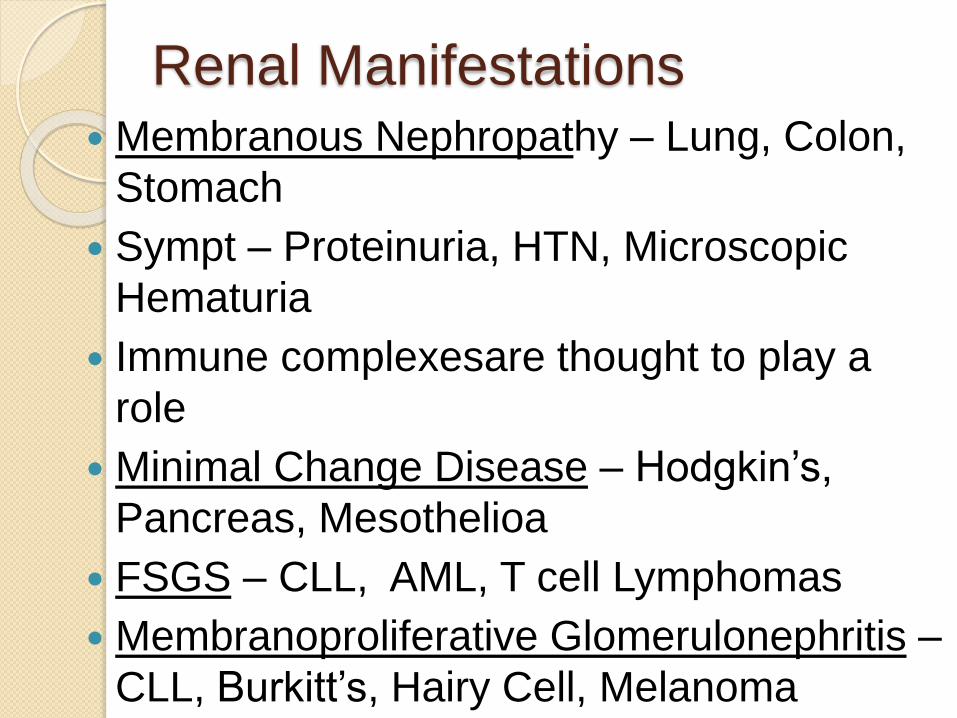
Renal Manifestations Membranous Nephropathy – Lung, Colon,
Stomach
Sympt – Proteinuria, HTN, Microscopic
Hematuria
Immune complexesare thought to play a
role
Minimal Change Disease – Hodgkin’s,
Pancreas, Mesothelioa
FSGS – CLL, AML, T cell Lymphomas
Membranoproliferative Glomerulonephritis –
CLL, Burkitt’s, Hairy Cell, Melanoma
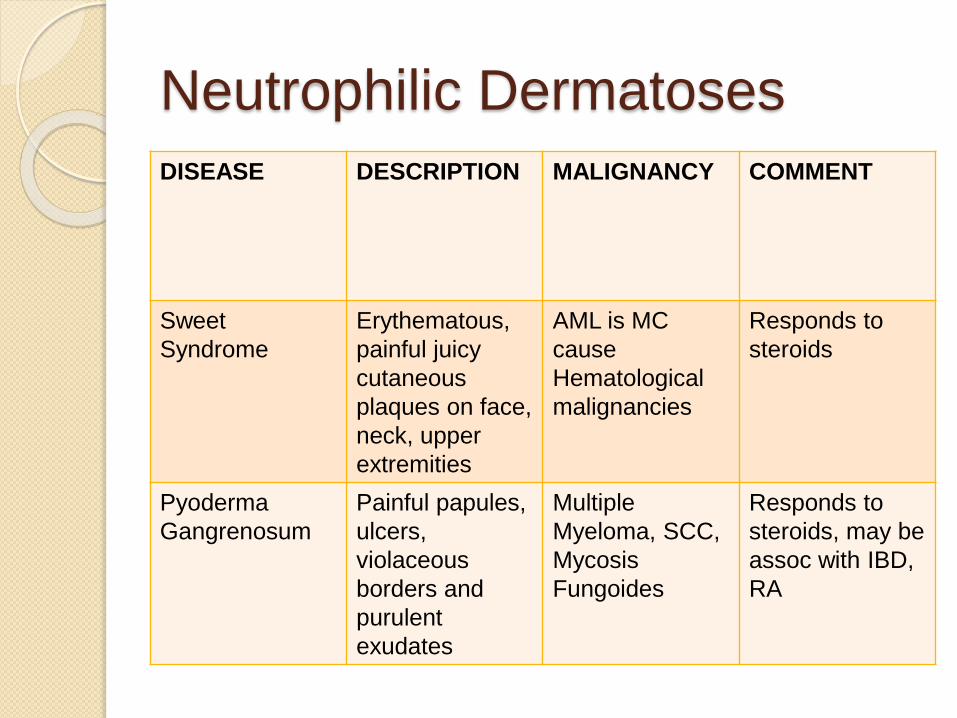
Neutrophilic Dermatoses
DISEASE DESCRIPTION MALIGNANCY COMMENT
Sweet
Syndrome
Erythematous,
painful juicy
cutaneous
plaques on face,
neck, upper
extremities
AML is MC
cause
Hematological
malignancies
Responds to
steroids
Pyoderma
Gangrenosum
Painful papules,
ulcers,
violaceous
borders and
purulent
exudates
Multiple
Myeloma, SCC,
Mycosis
Fungoides
Responds to
steroids, may be
assoc with IBD,
RA

Vascular Abnormalities
Vasculitis observed in 4.5 – 8%
malignancies.
NSCLC, SCC of esophagus, Prostate,
Hematological malignancies
Purpura – Thrombocytopenia, DIC,
vascular injury, vasculitis
Multifocal migratory thrombophlebitis -
<50 yrs, GI, lung, prostate, ovarian
cancer
Mondor disease – Cordlike
thrombophlebitis of anterior chest seen
in Breast Cancer.
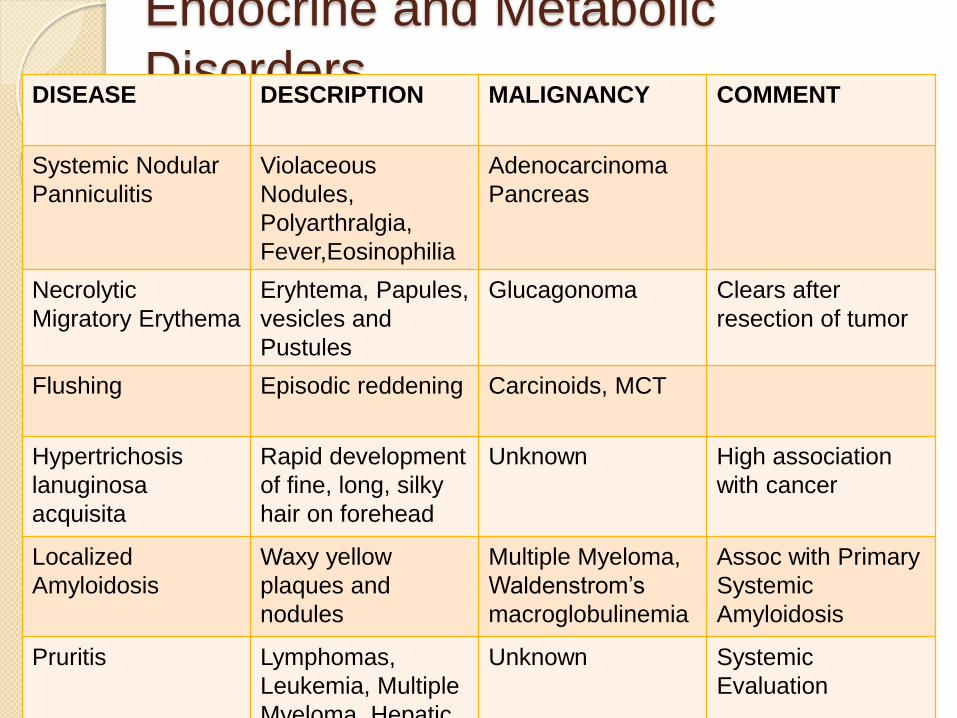
Endocrine and Metabolic
DisordersDISEASE DESCRIPTION MALIGNANCY COMMENT
Systemic Nodular
Panniculitis
Violaceous
Nodules,
Polyarthralgia,
Fever,Eosinophilia
Adenocarcinoma
Pancreas
Necrolytic
Migratory Erythema
Eryhtema, Papules,
vesicles and
Pustules
Glucagonoma Clears after
resection of tumor
Flushing Episodic reddening Carcinoids, MCT
Hypertrichosis
lanuginosa
acquisita
Rapid development
of fine, long, silky
hair on forehead
Unknown High association
with cancer
Localized
Amyloidosis
Waxy yellow
plaques and
nodules
Multiple Myeloma,
Waldenstrom’s
macroglobulinemia
Assoc with Primary
Systemic
Amyloidosis
Pruritis Lymphomas,
Leukemia, Multiple
Myeloma, Hepatic
Unknown Systemic
Evaluation

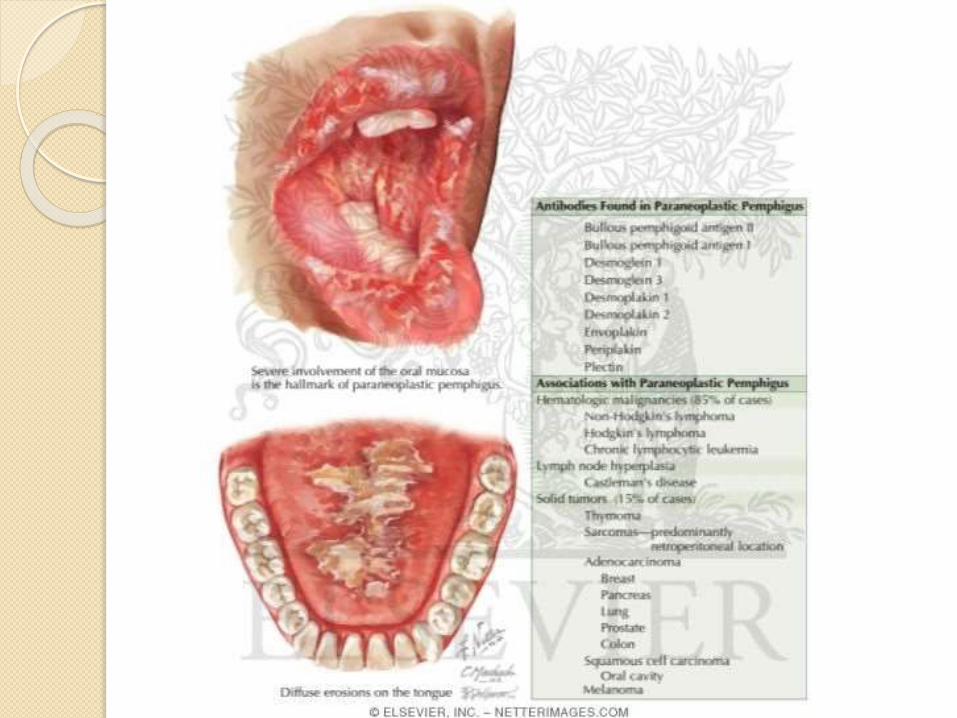
Bullous disorders Paraneoplastic Pemphigus is most frequently
seen in B-cell lymphopriferative disorders in cluding lymphomas, CLL, Castleman disease, thymoma, Waldenstrom’s macroglobulinemia and Spindle cell neoplasms.
Painful oral stomatitis, conjunctival ulcers and erosive skin lesions.
Internal organ involvement is common with 30% patients having respiratory failure.
Severe mucosal involvement and pathology reminiscent of erythema multiforme –HALLMARK OF PARANEOPLASTIC PEMPHIGUS
Rx – Steroids, Cyclosporine, Mycophenolatemofetil

Collagen Vascular Diseases
Dermatomyositis (DM) linked to malignancy in 25% cases.
Heliotrope rash of periorbital skin, Shawl Sign, V neck erythema and Gottron Sign, proximal muscle weakness.
MC associated with cancers of reproductive organs in women (MC Breast) and Lung, respiratory tract in both genders.
Most frequent pattern is onset of cancer within 1 year of diagnosis of DM.

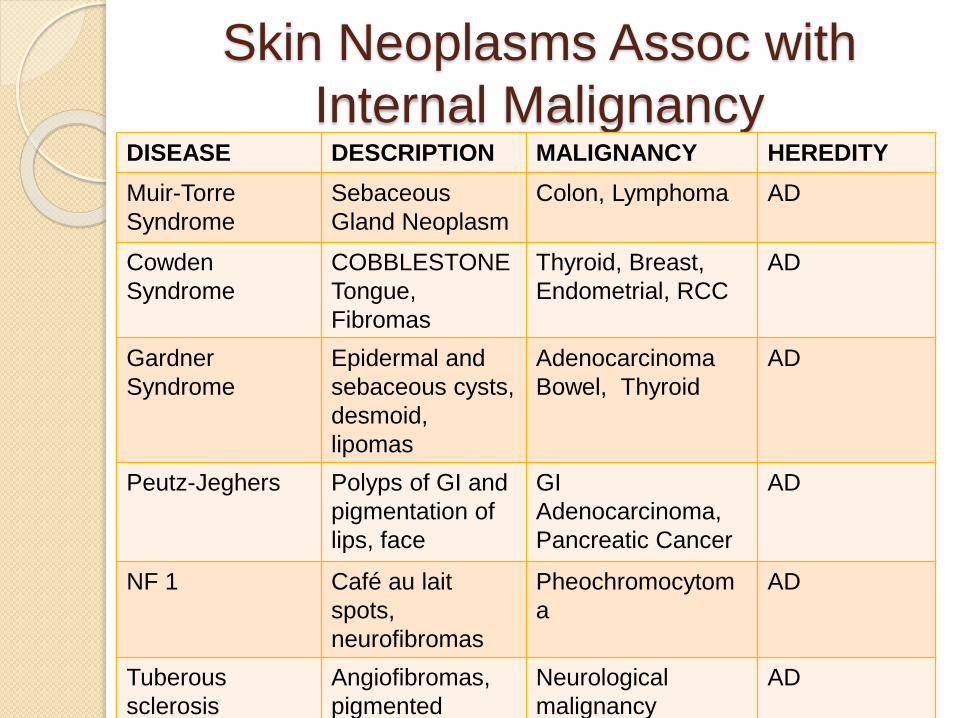
Skin Neoplasms Assoc with
Internal MalignancyDISEASE DESCRIPTION MALIGNANCY HEREDITY
Muir-Torre
Syndrome
Sebaceous
Gland Neoplasm
Colon, Lymphoma AD
Cowden
Syndrome
COBBLESTONE
Tongue,
Fibromas
Thyroid, Breast,
Endometrial, RCC
AD
Gardner
Syndrome
Epidermal and
sebaceous cysts,
desmoid,
lipomas
Adenocarcinoma
Bowel, Thyroid
AD
Peutz-Jeghers Polyps of GI and
pigmentation of
lips, face
GI
Adenocarcinoma,
Pancreatic Cancer
AD
NF 1 Café au lait
spots,
neurofibromas
Pheochromocytom
a
AD
Tuberous
sclerosis
Angiofibromas,
pigmented
macules,
Neurological
malignancy
AD

DISEASE DESCRIPTION MALIGNANCY HEREDITY
VHL Syndrome Skin
ecchymoses,
retinal
malformation,
papilloedema
RCC,
Pheochromocytom
a
AD
Sturge Weber
Syndrome
Port wine stains
in C.N V
distribution
Rare neurological
malignancy
Somatic
mutation in
fibronectin
gene
AT Telangiectasis Lymphomas,
Leukemias
AR
Bloom
Syndrome
Photosensitivity,
telangiectasis,
butterfly
erythema of
face
Leukemias,
Lymphomas
AR
Chediak Higashi
Syndrome
Recurrent
pyoderma,
partial albinism
Lymphomas AR
Werner
Syndrome
Scleroderma
like, premature
aging, leg
Sarcomas,
Meningiomas
AR
Miscellaneous Lesions
Multicentric Reticulohistocytosis
- Violaceous papules over joints with
arthritis mutilans in 50% patients.
- Ca. Pancreas, SCC Lung, Melanoma
- Due to destructive effects of
proteinases.
Pruritis
- HD, Polycythemia vera, Mycosis
Fungoides

Neurological Manifestations of
CancerSYNDROME % PARANEOPLASTIC
Lambert-Eaton myasthenic
syndrome
60
Subacute Cerebellar Degeneration 50
Subacute Sensory Neuronopathy 20
Opsoclonus-myoclonus (children) 50
Opsoclonus-myoclonus (adults) 20
Sensory motor peripheral
neuropathy
10
Encephalomyelitis 10
Dermatomyositis 10
Approach to a patient with
Paraneoplastic Neurological
Disease Complete history and Neurological examination
MRI with and without contrast
MRI and FDG-PET – Monitor response to therapy
PET-CT – Most sensitive to identify occult tumors
CSF Examination
Effective tumor ablation either with surgery or systemic therapies is more effective then immunosuppression.
Immunosuppression with steroids, plasma exchange, IvIg (frequent choice), immunoasorption is variably effective.
Limbic Encephalitis Clinical symptoms range from rapid onset
psychotic symptoms to status epilepticus May be mistaken for Herpes Simplex
Encephalitis. MRI – Mesial temporal contrast
enhancement or T2 signal hyper intensities. CSF – Elevated protein, lymphocytic
pleocytosis. SCLC, Testicular Cancer, Breast Cancer,
HL, NHL. Treatable forms of CNS Paraneoplasms Rx – Treatment of Primary +
Immunosuppression

Autonomic Neuropathy
25% patients with anti-Hu syndrome and SSN-EMN have autonomic dysfunstion
Usually associated with SCLC
Autonomic dysfuction may occur in patients with Myasthenia Gravis
GI dysmotility is usually a core complaint with orthostatic hypotension, hypoventilation, sleep apnea and cardiac dysrhythmias.
Treatment may stabilize disease but usually unable to reverse
Progressive Cerebellar
Degenaration (PCD)
Difficulty with walking, diplopia,
vertigo, loss of dexterity, dysarthria,
oscillopsia
CSF – lymphocytic pleocytosis, mild
elevated protein, oligoclonal bands
Breast Cancer, Ovarian Cancer,
Hodgkin’s Disease
Antibody negative PCD may occur in
conjunction with Lambert-Eaton
syndrome. MC associated tumor is
SCLC
Paraneoplastic Visual Loss
Photoreceptor degeneration causes night blindness, photopsias, and blurred vision. Colour perception loss if cones are involved. ERG is abnormal.
MC antibody – anti carcinoma associated retinal antigen antibody; target antigen is recoverin.
SCLC, NSCLC, Breast Cancer
Progressive vision loss with retinal pigment changes – Melanoma or Adenocarcinoma of gut
Melanoma associated retinopathy

Opsoclonus-Myoclonus
Disorder of ocular motility and
multifocal myoclonus.
Described in children with
Neuroblastoma
No one antigen seems to be common
Anti-Ri Breast or Gynecological
Cancer
Paraneoplastic OM without Ri
antibodies assoc with Hodgkin’s
Lymphoma
Paraneoplastic MND
Separated into three groups in a
series by MSKCC
1. Anti-Hu antibodies
2. Assoc with Breast cancer
3. Assoc with underlying solid tumors
Patients with HL and NHL also
reported
Patients present with multifocal motor
weakness

Paraneoplastic Peripheral
Neuropathies Subacute sensorimotor neuropathy usually
presents with progressive distal, symmetric sensory loss and weakness in legs. Lung Cancer is MC associated
Nerve Biopsy – Axonal injury and demyelination
Can also occur in women with breast cancer.
Demyelinating neuropathies may respond to therapy but axonal neuropathies respond poorly to immunosuppresion
Acute polyradiculoneuropathy (APN) increased frequency with Hodgkin’s lymphoma which responds to plasmapharesis and IvIg.
Contd..
Secondary amyloidosis may also
cause painful sensorimotor
neuropathy in patients
Waldenstrom’s – Rx is Fludarabine,
Rituximab, Stem Cell Transplant
Myeloma – POEMS Syndrome
Painful mononeuritis multiplex –
SCLC, Prostate, Endometrial,
Lymphoma, RCC
Inflammatory Brachial Neuritis - HL
Neuromuscular Junction
Disorders Typical myasthenia assoc with
Thymoma in 15% cases. All patients to undergo CT chest to rule out thymoma.
Lambert Eaton syndrome assoc with SCLC – Proximal weakness, paresthesias, erectile dysfunction; Most patients benefit from plasmapharesis and immunosuppressants
Augmentation of compound motor action potential with repetitive stimulation
Paraneoplastic Syndrome with
Muscle Rigidity
Stiff-person syndrome- stiffness and rigidity in paraspinal and
abdominal muscles- Breast, HL, Colon- Antibodies against amphiphysin or glutamic
acid decarboxylase Neuromyotonia- spontaneous and continuous muscle fiber
activity of peripheral origin- Myasthenia in thymoma, HL, Plasma cell
dyscrasia, SCLC Peripheral nerve hyper excitability
disorders
Movement Disorders
Hyperkinetic syndromes predominate
Chorea – SCLC, ALL, RCC, HL
Parkinson’s – extremely rare; reported
in a man with multiple myeloma;
mechanism unclear.
Hypokinetic parkinsonism like features
reported in testicular seminoma
Movement disorders also reported in a
patient of B-cell lymphoma.