-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
1/18
2003 European Society of Veterinary Dermatology 279
Veterinary Dermatology2003, 14, 279 296
BlackwellPublishingLtd.
Invited Review
Cutaneous paraneoplastic syndromes in dogs and cats: a review
ofthe literature
MICHELLE M. TUREK
School of Veterinary Medicine, Department of Surgical Sciences,
University of Wisconsin-Madison, 2015Linden Drive Madison, WI
53706, USA
(Received24 January2003; accepted15 May2003)
Abstract Cutaneous paraneoplastic syndromes are a group of
noncancerous dermatoses associated with internalmalignancy. Their
recognition can facilitate detection and timely treatment of
underlying cancer. More than 30such disorders have been identified
in the human scientific literature, whereas only a few are
described in veterinarymedicine. This may reflect a lower incidence
in animals than in people or may be the result of failure to
recognizean association between certain skin lesions and neoplasia.
Establishing a relationship between a cutaneous dis-order and
neoplasia can be difficult unless the skin lesions are rare and
almost always associated with a particulartumour type, as is the
case for most recognized veterinary paraneoplastic dermatoses.
Among these are felineparaneoplastic alopecia, feline
thymoma-associated exfoliative dermatitis, nodular dermatofibrosis,
feminizationsyndrome associated with testicular tumours,
superficial necrolytic dermatitis and paraneoplastic pemphigus.The
aetiology of most cutaneous paraneoplastic syndromes has remained
elusive in both people and animals.
Keywords:alopecia, cat, dog, exfoliative dermatitis,
feminization, nodular dermatofibrosis, paraneoplastic,pemphigus,
skin, superficial necrolytic dermatitis
Paraneoplastic syndromes (PNSs) are
noncancerous,neoplasm-related disorders that occur at a site
distinctfrom the primary tumour or its metastases. They pro-duce
signs that reflect the remote effects of cancer ratherthan the
direct effects caused by tumour growth or inva-sion. Presenting as
endocrine, haematological, gastroin-testinal, neurological, renal
or cutaneous aberrations,PNSs may be the first sign of an
underlying malignancyand may herald a certain tumour type. Their
recognition,therefore, can be important to facilitate early
diagnosisand treatment of the neoplasm, and to identify
tumourrecurrence following therapy. Additional clinical sig-
nificance of PNSs lies in their morbidity, which, in manycases,
can cause greater compromise of quality of lifethan the tumour
itself.
The frequency of PNSs in veterinary medicine isundetermined. In
people, estimates suggest that as manyas 50% of patients will
experience a PNS at some pointin the course of their
malignancy.1PNSs most com-monly involve the endocrine and
haematological sys-tems in both people and animals. One of the
bestcharacterized PNSs in veterinary medicine results
inpolyuria/polydipsia, polyphagia, bilateral symmetricalopecia,
hyperpigmentation, muscle atrophy and
pot-belly appearance, the distant effects of excessivecortisol
production by an adrenal gland adenoma inhyperadrenocortism.2,3
Cutaneous paraneoplastic syndromes are externalclues to internal
malignancy. More than 30 such disor-ders have been documented in
the human scientific lit-erature (Table 1),4although the incidence
of underlyingmalignancy varies greatly among them.5 In
contrast,only a few cutaneous PNSs have been reported in
vet-erinary medicine (Table 2). This may reflect a lower inci-dence
in animals than in people or may be the result offailure to
recognize an association between certain skin
lesions and neoplasia. The classification of a syndromeas
paraneoplastic is fairly straightforward in the case ofa rare
dermatosis, whose rarity and frequent occurrencewith neoplasia make
the association apparent,6 as isthe case for most recognized
veterinary paraneoplasticdermatoses. More common skin
manifestations can bedifficult to classify because many of them
frequentlyappear without any underlying cancer.6 It has
beenproposed that in order to classify a disorder as a cuta-neous
PNS, the onset or recognition of a malignancyand the skin condition
should occur at the same timeand should follow a parallel
course.4However, becauseoccult cancers can go undetected for many
years, it can
be difficult to prove that the two conditions
developedconcomitantly. Therefore, clinically, the appearance
ofparaneoplastic signs may precede, follow or coincide withthe
detection of the related neoplasm.4,79In addition,
Correspondence: M. M. Turek, School of Veterinary
Medicine,Department of Surgical Sciences, University of
Wisconsin-Madison,2015 Linden Drive Madison, WI 53706, USA. E-mail:
[email protected]
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
2/18
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
3/18
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
4/18
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
5/18
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
6/18
284 M. M. Turek
2003 European Society of Veterinary Dermatology, Veterinary
Dermatology, 14, 279296
because of the presence of clinically undetectable,microscopic
tumour cells that may remain after an app-arently complete clinical
remission, the course of thetwo conditions may appear to
diverge.8,9
The pathophysiological mechanism(s) by which neo-plasia causes
development of distant, noncontiguous
dermatoses in people (Table 1) and in animals has notbeen well
established in most cases. A variety of aetiol-ogies has been
postulated, including tumour-inducedantigenantibody interactions
and abnormal or abnor-mally excessive production of biologically
active hor-mones, growth factors or cytokines by tumour cells orby
accessory cells in response to the tumour.6
Because many cutaneous PNSs in people, includingthe
papulosquamous disorders listed in Table 1, areproliferative in
nature, growth factors (GFs) have beensuggested in several human
case reports to have a pos-sible aetiological role.1014Normal
keratinocyte func-tion is regulated by various GFs, and among the
mostimportant for proliferation is transforming growth fac-tor
alpha (TGF-), a member of the epidermal growthfactor (EGF) family.
TGF-acts through the epider-mal growth factor receptor (EGFR or
ErbB1), whoserole in normal keratinocyte function as well as in
car-cinogenesis, particularly as pertains to epithelial neo-plasia,
a common inducer of papulosquamous PNSdisorders, has been
extensively studied.1517TGF-isthe most commonly implicated GF in
the pathogenesisof papulosquamous cutaneous PNSs in people,
althoughdefinitive evidence of an aetiologic connection is
lacking.Individual human case reports associate paraneoplas-
tic types of acanthosis nigricans,1012 sign of Leser-Trlat10and
tripe palms13with abnormally elevatedserum,12,13urine,10
tumour11,12 and/or cell messengerRNA13levels of TGF-. In all
reported cases, effectivetreatment of the underlying neoplasia,
including gastriccarcinoma,11,12melanoma10and
mastocytosis,13resultedin simultaneous decrease of TGF-levels and
clinicalimprovement of the dermatosis. However, in partbecause TGF-
has not been demonstrated in thecutaneous lesions of these
dermatoses, it is not possi-ble to attribute a direct causal role
to this GF. Interest-ingly, TGF-overexpression in three of these
cases was
associated with concurrent overexpression of EGFR intumour
tissue11,12and/or lesional skin10,12as shown
byimmunohistochemical10,12or Southern blot11analysis.
In addition, hyperinsulinism and insulin resistancemediated by
tumour-induced anti-insulin receptor anti-bodies may be linked to
the pathogenesis of paraneo-plastic acanthosis nigricans in people
(Table 1), as isthe case in the endocrinopathy-related form of the
der-matosis.8,18According to the hypothesis, the
epidermalproliferation that is characteristic of the dermatosismay
be stimulated by the high levels of insulin that isstructurally
similar to insulin-like growth factor (ILGF)and that cross-binds to
the ILGF receptor, whose acti-
vation, like that of EGFR, stimulates proliferation ofnormal
keratinocytes.8,18
Other mechanisms of pathogenesis that have beenconsidered in
both human and veterinary literature
include antigenantibody interactions mediated bycross-reactivity
between tumour antigens and antigensin the normal skin, as well as
tumour-induced deple-tion of certain physiological
substances.6These are dis-cussed in detail later in relation to the
autoimmunedisorder, paraneoplastic pemphigus, and to
superficial
necrolytic dermatitis, respectively.
FELINE PARANEOPLASTIC ALOPECIA
Feline paraneoplastic alopecia (FPA) manifests as anonpruritic,
progressive, symmetrical alopecia. This clin-ically and
histologically characteristic dermatosis hasbeen reported in
association with pancreatic carcinomain 12 cats,1923and biliary
carcinoma in two cats.20,24
Affected animals range in age from 7 to 16 years (median13
years). There appears to be no breed predilection.
The chief presenting complaint in all reports is
acute,progressive alopecia of 2 weeks to 10 months duration(median
4 weeks). Cats have concurrent signs of systemicillness including
weight loss in all animals and variabledegrees of inappetance,
vomiting, diarrhoea and leth-argy in some. Hair loss is symmetrical
and progressesfrom the ventrum to the head and to primarily
themedial aspect of the extremities. Hair is easily epilatedand
alopecic skin is shiny, inelastic and thin, but notfragile. Some
affected cats are reported to groom exces-sively,20,24 and it has
been postulated that the shinyappearance of the skin arises from
exfoliation of thestratum corneum as a result of excessive
grooming.20,22
In addition, foot pad involvement is common. Affectedpads are
painful and appear either dry, crusted and fis-sured, or
erythematous and moist. Although FPA is anonpruritic disorder,
pruritus has been reported withsecondary Malasseziaspp. infections
and flea infesta-tions.21,23,24 In a recent report of feline skin
biopsiescomplicated by the presence of Malassezia spp.,
his-topathology from 7 of 15 cases was consistent with FPA.23
Although pancreatic carcinoma was confirmed in onlyfour of these
cats, it was suggested that the presence ofyeast organisms in
histopathological specimens from catswith generalized skin disease
could serve as a harbinger
of internal malignancy.
23
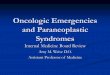
Histopathological evaluation of alopecic skin revealsa
nonscarring alopecia with characteristic marked fol-licular
telogenization, miniaturization and atrophy(Fig. 1). Less specific
findings include mild epidermalacanthosis and hyperplasia with
thinning or absence ofthe stratum corneum and patchy parakeratosis
with amild, predominantly mononuclear, perivascular inflam-matory
infiltrate of the dermis.19,20,22,24
Clinical differential diagnoses include feline endo-crinopathies
such as hyperadrenocorticism and hyper-thyroidism, dermatophytosis,
demodicosis, self-inducedalopecia, telogen defluxion, feline
symmetrical alo-
pecia and alopecia areata.19,22Specific features of theclinical
presentation as well as diagnostic tests includ-ing
adrenocorticotropic hormone (ACTH) stimulationand dexamethasone
suppression tests, thyroid hormone
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
7/18
2003 European Society of Veterinary Dermatology, Veterinary
Dermatology, 14, 279296
Cutaneous paraneoplastic syndromes 285
measurement, Woods lamp examination, fungal culture,skin
scraping, KOH preparation, faecal examination,trichograms and skin
biopsy are important to ruleout these possibilities. Abdominal
radiography and/orultrasonography, as well as thoracic radiographs
toevaluate for pulmonary metastasis, are important if FPAis
suspected. Exploratory laparotomy with tissue biopsymay be
necessary to confirm the diagnosis of neoplasia.
Neoplastic diseases of the exocrine pancreas and bili-ary tree
are rare in the cat. In the vast majority of cases,
the disease has metastasized to distant sites includingliver,
lymph nodes, other intraperitoneal structures andlungs at the time
of diagnosis, and the prognosis is there-fore grave.25,26Twelve of
the fourteen cats reported inthe literature died or were euthanized
within 8 weeks ofonset of clinical signs.19,20,23,24
Skin lesions did not improve in any cat treated
withcorticosteroids. Little else can be concluded about
themanagement of FPA, as most cats were euthanizedprior to
diagnosis or at the time of diagnosis owing toadvanced stage of
disease. However, resolution of FPAwas documented after surgical
resection in a single case
of solitary pancreatic tumour.
22
Recrudescence of cutan-eous lesions at the time of metastasis 18
weeks later inthis case provides further evidence for the
classificationof FPA as a PNS.
FELINE THYMOMA-ASSOCIATED
EXFOLIATIVE DERMATITIS
Paraneoplastic exfoliative dermatitis has been reportedin cats
in association with thymoma. Six cases have beendescribed,2730five
of which were characterized clini-cally and
histopathologically.27,28,30The disorder presents
as diffuse erythema of the skin accompanied by exfolia-tion or
scaling. Lymphomas and leukaemias are the mostcommon cancers
associated with this PNS in people(Table 1).31Interestingly,
exfoliative dermatitis has not
been reported in association with thymoma in people.In addition
to malignancy, other causes of exfoliative
dermatitis include drug eruption, pre-existing derma-toses such
as contact dermatitis, pemphigus foliaceus,systemic lupus
erythematosus and cutaneous bacterial,fungal, parasitic or yeast
infections, as well as hyper-
adrenocortism.3
The reaction can also be idiopathic, asis the case in up to 50%
of human patients.31In the docu-mented veterinary cases of
paraneoplastic exfoliativedermatitis, all affected cats were
concurrently diagnosedwith thymoma. However, the association
between thy-moma and the skin lesions may be controversial in
onecase in which antibiotic therapy was used within onemonth of the
development of skin lesions,27and in ano-ther in which fungal
culture was positive for Microsporumcanisat the onset of cutaneous
signs five months priorto diagnosis of thymoma.27Notably, the
dermatitis inthe latter case progressed despite treatment with
grise-ofulvin.27Furthermore, and in addition to the six
catsreviewed herein, another report describes a case of pos-sible
paraneoplastic exfoliative dermatitis in combina-tion with erythema
multiforme in a cat recently treatedwith an imidacloprid
preparation. Although a drugeruption was initially strongly
suspected in this casebased on histopathological findings
consistent witherythema multiforme, as well as the temporal
associa-tion between drug application and the onset of
dermatosis,the cat was diagnosed with a previously
unobservedthymoma four months after the onset of the
dermatosis.32
Feline thymoma-associated exfoliative dermatitisbegins as
nonpruritic scaling and mild erythema on the
head and pinnae in an apparently otherwise healthycat.27
Progressively, lesions become generally distrib-uted, and, as the
scaling intensifies, alopecia develops(Fig. 2).27Brown, waxy,
keratosebaceous debris accu-mulates between the digits, in the nail
beds, and in theear canals.27Crusts and ulcers may
develop.27Althoughnot a common feature of this condition, pruritus
wasreported in conjunction with secondary overgrowth ofMalassezia
spp. in one case of thymoma-associated
Figure 1. Feline paraneoplastic alopecia. Severe follicular
atrophywith epidermal hyperplasia and orthokeratotic
hyperkeratosis.Haematoxylin & eosin (H&E), original
magnification 12.5. (Photo-micrograph courtesy of Dr Elizabeth
Mauldin; previously publishedin Veterinary Dermatology, Vol.
13.)
Figure 2. Feline thymoma-associated exfoliative dermatitis.
Alopeciaassociated with severe scaling and mild erythema of the
head, neckand pectoral regions. (Photograph courtesy of Dr
Elizabeth Mauldin.)
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
8/18
286 M. M. Turek
2003 European Society of Veterinary Dermatology, Veterinary
Dermatology, 14, 279296
exfoliative dermatitis,30as well as in three cats with
his-topathological changes characteristic of
paraneoplasticexfoliative dermatitis where the possibility of
under-lying malignancy was not fully investigated.23 Skinlesions
were refractory to corticosteroid therapy in onecase so
treated.27
Histopathologically, skin lesions are characterized bya
cell-poor hydropic interface dermatitis wherein mul-tifocal areas
of hydropic degeneration of basal cells andapoptotic keratinocytes
are found in the epidermis and
infundibular region of the hair follicle.27The epidermisis
mildly to moderately hyperplastic and there is mildto marked
orthokeratotic hyperkeratosis and focal par-akeratotic
hyperkeratosis (Fig. 3). Erosions may develop.An inflammatory
infiltrate, primarily lymphoid, maybe present perivascularly in the
dermis and within theepidermis. These histological changes along
with a rel-evant history, physical findings and negative
routinediagnostic tests including skin scrapings, trichographyand
cytology should alert the clinician to the possibil-ity of a
paraneoplastic dermatosis and evaluation ofthe cranial mediastinum
should be pursued. If a diag-
nosis of thymoma-associated exfoliative dermatitis issuspected,
thoracic radiographs should be performed.Radiographically, the
presence of a variably sized massin the cranial mediastinum,
occasionally accompaniedby pleural effusion, is suggestive of the
diagnosis.33Forconfirmation, transthoracic fine-needle aspirates
andneedle core biopsies of the mass can be safely performedwith
ultrasound guidance.33
Five of the six published cases of feline thymoma-associated
exfoliative dermatitis resulted in euthanasiawithin 45 months of
the onset of clinical signs due torefractory and progressive skin
disease, suggesting apoor prognosis.2729However, in three of these
cases no
attempt was made to treat the underlying malignancy,as the
diagnosis was made only at necropsy. Importantly,one report
describes complete resolution of Malassezia-complicated exfoliative
dermatitis six months after
surgical resection of the tumour.30Fourteen months aftersurgery,
the cat had neither recurrence of the thymomanor the skin lesions.
These reports underscore theimportance of recognizing exfoliative
dermatitis as apossible marker of neoplasia in the cat, allowing
forearlier detection and prompt treatment that might sig-
nificantly affect survival.The mechanism of thymoma-associated
exfoliativedermatitis is unknown, as is true for
paraneoplasticexfoliative dermatitis in people. The interface
dermatitisand lymphoid cellular infiltrate described in cats
suggestthat a tumour-induced immune-mediated process may
beinvolved.27This idea is supported, at least in theory, bythe fact
that the normal thymus is an important com-ponent of the immune
system and that aberrant immu-nological responses induced by a
diseased gland arebelieved to be related to other immunologically
basedconditions such as myositis and myasthenia gravis.30
Thymoma is uncommon in the cat. Surgical resectionis the
treatment of choice. Tumours that are noninvasiveand easily
excisable carry a good prognosis with mediansurvival of almost two
years.33In contrast, cats withinvasive tumours often do not survive
the perioperativeperiod, representing15% of cases.33Unfortunately,
evenwith sophisticated imaging modalities such as
computedtomography, tumour resectability is in many casesimpossible
to predict preoperatively. Metastasis is rare.
NODULAR DERMATOFIBROSIS
Nodular dermatofibrosis (ND) is a well-documentedPNS
characterized by the development of multiple,cutaneous nodules of
collagenous origin in associationwith renal cystadenocarcinoma or
cystadenoma. Thesyndrome was initially reported in Alsatians in
1983.34
Thereafter, all additional cases, except two, have beendescribed
in German Shepherd dogs.3539 Pedigreeanalysis of affected German
Shepherd dogs stronglyindicates that the disease is inherited in an
autosomaldominant pattern.35In addition, recent genetic evalu-ation
of a canine colony that was bred for developmentof this syndrome
localized the condition to a region on
canine chromosome 5 and suggested a possible causalrole for a
previously unidentified tumour suppressorgene.40The syndrome has
been also described in oneGolden Retriever and one German Shepherd
Cross.36,41
Skin lesions consist of multiple, firm,
well-circumscribednodules, ranging in diameter from 2 mm to 5 cm,
andrepresent the most common presenting complaint ofthis
syndrome.3439,41Nodules are nonpruritic, locatedin the dermis or
subcutis, and are freely moveable.39
Most are covered by an intact epidermis, although somelesions
become ulcerated and secondarily inflamed.34,35,39
Lesions are localized primarily to the extremities (Fig.
4),although distribution can be diffuse.3439,41 Histologi-
cally, nodules consist of irregular bundles of dense,
well-differentiated collagen fibres in the dermis or subcutiswith
no sharp demarcation from surrounding connec-tive
tissue.3438,41
Figure 3. Feline thymoma-associated exfoliative dermatitis.
Severehyperkeratosis with multifocal keratinocyte necrosis; mild
pleocellularinfiltrate in dermis which focally obscures
dermoepidermal junction.H&E, original magnification 62.5.
(Photomicrograph courtesy ofDr Elizabeth Mauldin.)
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
9/18
2003 European Society of Veterinary Dermatology, Veterinary
Dermatology, 14, 279296
Cutaneous paraneoplastic syndromes 287
Most affected dogs present with the primary com-plaint of
nonpainful cutaneous nodules.39The meanage at onset of skin
changes, based on a report of 51 dogs,is 6 years.39 However,
clinical signs can vary greatlydepending upon stage of renal
pathology at the time of
presentation and may include haematuria, abdominaldistension and
pain secondary to renal cyst rupture,depression, fever and loss of
appetite. Importantly, NDalmost always antecedes systemic signs of
illness relatedto tumour-induced renal failure or metastasis by
monthsto years.39In contrast to the mean age at onset of
skinlesions, the mean age of diagnosis of renal changes is8
years.39This highlights the importance of recogniz-ing ND as a
marker of renal neoplasia, allowing for earlydetection of the
syndrome.
Renal changes are slowly progressive and almostalways
bilateral.35,36,38,39,41 Histopathology reveals
cystadenocarcinomas or, less commonly,
cystadeno-mas.3539,41Grossly, kidneys appear enlarged and
irre-gular with multiple solid or cystic tumours.3539,41
Microscopic examination shows epithelial changes rang-ing from
multifocal hyperplasia to highly malignantepithelial
proliferation.35,38,39,41It has been speculated thatproliferation
of the epithelium represents a preneoplas-tic change that develops
progressively from hyperplasiato adenoma to carcinoma over many
months to years.35
A recent study showed the presence of microscopic renalcystic
lesions lined by hyperplastic renal tubular epi-thelium in two,
clinically healthy, 1-year-old progeny ofa dog diagnosed with renal
cystadenocarcinoma and ND,
suggesting that microscopically detectable renal changesoccur in
carriers of the disease at a young age.42Inter-estingly, affected
bitches almost always have concurrentuterine leiomyomas that carry
little clinical significance.35,39
In addition, there are some reports of incidental hyper-plastic
polyps and hypertrophy of collagen in the smallintestine,
suggesting multiple organ involvement.36,39
Upon presentation of an adult dog, especially of theGerman
Shepherd breed, with nonpainful, firm cuta-neous nodules involving
primarily the extremities, a
diagnosis of ND should be considered. Skin biopsy shouldbe
performed as one of the first diagnostic tests if NDis suspected.
To investigate the possibility of underly-ing neoplasia, the
kidneys should be evaluated withradiography, ultrasonography,
computed tomographyor contrast nephrography. Enlarged and
abnormallyshaped kidneys can be palpated in 60% of
cases.39Serumbiochemistry analysis may reveal renal insufficiency
orfailure, and scintigraphy can be performed to evaluatethe
relative glomerular filtration rate of each kidney.Renal biopsy is
necessary for confirmation, however,concurrent characteristic skin
lesions and morphologicrenal changes in a German Shepherd is
stronglysuggestive of the diagnosis.
Unfortunately, no effective treatment has been foundfor this
syndrome, including glucocorticoid therapy.39
Given the bilateral nature of the renal neoplasia, uni-lateral
nephrectomy is seldom curative and, thus,lifespan does not seem to
be affected by early diagno-sis.39Chemotherapy trials have not been
reported. Inan attempt to avoid complications such as rupture
ofrenal cysts, unilateral nephrectomy of large, nonfunc-tioning
kidneys may be performed. In addition, skinnodules that are
ulcerated or that interfere with loco-motion can be removed
palliatively with surgery or cry-
otherapy. In light of the lack of effective treatment forthe
underlying cancer, prognosis for long-term survivalis poor. It is
important, however, to recognize ND as aslowly progressive disease
with a protracted clinicalcourse if renal disease is in the early
stages. The meantime from first observation of ND to death is
about2.5 years.39Dog owners should be well educated in thisregard
to avoid premature euthanasia that could resultfrom the knowledge
that the underlying cause of theskin lesions is an untreatable
cancer. Ultimately, thecause of death or euthanasia in the majority
of cases isattributable to progressive neoplasia and renal
disease.39
Less commonly, the decision to euthanize is related
toprogressive or complicated ND.39Metastasis from renaltumours is
found at necropsy in approximately half ofaffected dogs and occurs
in lymph nodes, lungs, liver,pleura and peritoneum.39Given the
probable hereditarybasis of this disease, affected dogs should not
be bred.
The mechanism of association between the develop-ment of ND and
renal cystic changes is unclear. It hasbeen postulated that renal
tumours may secrete collagen-stimulating growth factors or
cytokines that acceleratecollagen accumulation.3638,41However, no
such factorhas been isolated. TGF-has been theoretically
impli-cated by some authors3741in light of the possible asso-
ciation of this growth factor with various
proliferativecutaneous paraneoplastic syndromes in people.1013
Alternatively, cutaneous and renal lesions may arise
inde-pendently from a common inherited genetic defect.36,40
Figure 4. Nodular dermatofibrosis in a German Shepherd dog
withmultiple dermal and subcutaneous nodules on an
extremity.(Photograph courtesy of Professor Dr Frode Lingaas.)
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
10/18
288 M. M. Turek
2003 European Society of Veterinary Dermatology, Veterinary
Dermatology, 14, 279296
FEMINIZATION SYNDROME ASSOCIATED
WITH TESTICULAR NEOPLASIA
Sertoli cell tumours, seminomas and interstitial celltumours
represent the three most common histologicaltypes of testicular
neoplasms in the dog,43and arise from
the oestrogen-secreting sustentacular cells of semini-ferous
tubules, the germinal epithelium and the Leydigcells, respectively.
Occurring in approximately equalfrequencies,43they represent a
common type of neopla-sia in the intact dog.43The vast majority of
testiculartumours have a low metastatic potential and
thereforecarry an excellent prognosis. A strong associationbetween
increased risk for development of neoplasia,particularly of Sertoli
cell tumours and seminomas,and cryptorchidism has been well
established.43,44
In general, most dogs with testicular tumours areasymptomatic,
or they present with only local swellingand/or testicular atrophy
of the contralateral, non-neoplastic testicle.45The feminization
syndrome is re-ported to occur in 2457% of dogs bearing Sertoli
celltumours,44,46,47and results from hormonal imbalancesecondary to
a functional tumour. Occasional reportshave described the syndrome
in association with inter-stitial cell tumour or
seminoma.46,4850However, becauseof their relative rarity, the
histological classification ofthe tumours in some of these reports
may be questioned;a recent study examining the
immunohistochemicalcharacteristics of testicular neoplasia revealed
that adiagnosis based on histology alone was insufficient in20% of
cases.51
The feminization syndrome is characterized by vari-ous
combinations of gynecomastia, attraction of othermale dogs,
pendulous prepuce, penile atrophy, pros-tatic squamous metaplasia
and myelosuppression inaddition to skin changes.3,45,46The major
dermatologi-cal feature is slowly progressive, bilateral,
symmetricalalopecia that typically originates on the neck,
lumbarregion, perineum and genital area.3Occasionally, thereis
thinning of the epidermis.3Histological changes
includeorthokeratotic hyperkeratosis, follicular dilatation
andatrophy, follicular keratosis, telogenization of hair fol-licles
and sebaceous gland atrophy.3Other clinical find-
ings include, coat colour change, macular melanosisaround the
inguinal, perineal and genital areas, as wellas linear preputial
dermatosis.3This latter term des-cribes a linear narrow pigmentary
change that extendsfrom the preputial orifice to the scrotum and is
consid-ered specific for testicular neoplasia.3 Histologically,this
lesion is characterized only by some mild vasculardilatation and
congestion.3
Dogs with testicular neoplasia can have skin
changes,feminization or both. When skin changes appear alone,the
differential diagnoses include hypogonadism, adrenalsex hormone
imbalance and, less likely, hypothyroidismand
hyperadrenocorticism.3 Unless accompanied by
obvious testicular enlargement, the diagnosis of para-neoplastic
feminization syndrome may not be straightfor-ward. Histopathology
of affected skin is nonspecific.Testicular ultrasound may be
helpful in identifying a
nonpalpable tumour and in association with a fine nee-dle
aspirate can be diagnostic for testicular neoplasia.Because the
incidence of feminization syndrome ishighest in association with
cryptorchid neoplastic tes-tes,44,4649,5256ultrasound evaluation of
the inguinalregion and abdominal cavity for retained testicles
is
indicated. In addition, complete haematological evalu-ation
should be performed in all dogs with suspectedtesticular tumours,
particularly in those with feminiza-tion, to evaluate for
hormonally induced myelosup-pression characterized by pancytopenia.
In dogs withblood dyscrasias, the prognosis for survival is
generallypoor even with treatment,48,49,52,54,56although
somereports of recovery exist.48,56Death in these cases isrelated
to severe aplastic anaemia, septicaemia and/or
thromboembolism.48,49,52,54,56 Ultimately, the dia-gnosis of
feminization syndrome is based on clinicalfindings, histological
evaluation of neoplastic testiclesand response to therapy after
bilateral orchiectomy.In cases uncomplicated by myelosuppression or
metas-tasis, resolution of clinical signs usually occurs
withinmonths.3,47,53 Although the metastatic potential oftesticular
neoplasia is low, occurring in fewer than 10%of dogs,45 complete
clinical staging is warranted inall cases and should include
abdominal ultrasoundand thoracic radiographs for evaluation of
possibleabdominal lymph node and pulmonary
metastasis,respectively.
Hyperestrogenism has been implicated in the patho-genesis of
feminization because of the high incidence ofthe syndrome in
association with Sertoli cell tumour,
whose nontransformed cellular counterpart is
oestrogen-secreting. However, direct evidence of this hypothesishas
been lacking, due to a lack of quantitative hormo-nal analyses in
many reported cases and due to con-flicting results among those
studies in which oestrogenlevels were measured. Increased blood
oestrogen levelswere detected in some cases,48,49,52,57,58whereas
normaloestrogen levels were described in
others.48,59,60Untilrecently, these reported hormonal analyses have
beenbased on single case reports or on very small case
series,making it impossible to draw statistically based
conclu-sions. In contrast, two recent comparative
publications50,61
have reported significantly increased concentrationsof
oestradiol-17in peripheral venous50,61and testicularvenous50blood
of dogs with Sertoli cell tumours com-pared to normal dogs. Dogs
with Sertoli cell tumoursand feminization syndrome had greater
increasedoestradiol-17 concentrations in peripheral venousand
testicular venous blood than did dogs with Sertolicell tumours
without feminization.50In both reports,testosterone concentrations
were reduced in dogs withSertoli cell tumours compared with normal
dogs.50,61
The calculation of the testosterone/oestradiol ratio
wassuggested to be a more reliable diagnostic tool thanthe
individual hormone values, as it was better cor-
related to clinical signs of feminization.61Interestingly,dogs
with interstitial cell tumours also had greaterconcentrations of
oestradiol-17in peripheral venousand testicular venous blood than
did normal dogs.50
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
11/18
2003 European Society of Veterinary Dermatology, Veterinary
Dermatology, 14, 279296
Cutaneous paraneoplastic syndromes 289
In contrast, oestradiol-17 concentrations in dogs withseminoma
were not different50or were decreased61com-pared with normal dogs,
suggesting that seminomas arenot endocrinologically active.
Although these data indicate a direct association bet-ween
hyperestrogenism and feminization syndrome,
not all feminized dogs in these series had elevated levelsof
oestradiol-17.61It has been suggested, therefore,that the shift of
balance between testosterone andoestradiol may be more important
than the absoluteoestradiol level.61Alternatively, disparate
results maybe explained by the fluctuation of hormonal
concen-trations such that laboratory measurement may provideonly a
snap shot view of the hormonal state.61Lastly,the occurrence of
feminization in the face of normaloestradiol-17concentration may
reflect the produc-tion of other physiological forms of oestrogen,
such asoestrone or oestriol, that are not detected by
standardradioimmunoassays, or the production of
unknownoestrogen-like substances.48,61Interestingly, symmetri-cal
endocrine alopecia has also been described in asso-ciation with
hyperprogesteronaemia in a dog withSertoli cell tumour.53
SUPERFICIAL NECROLYTIC
DERMATITIS
Superficial necrolytic dermatitis (SND) is a well-described,
necrotizing skin condition of dogs thatoccurs in association with
internal disease. The human
counterpart, necrolytic migratory erythema (NME) isa distinctive
cutaneous eruption that accompanies aglucagon-secreting alpha cell
tumour of the pancreas(Table 1). Human patients develop
erythematous macu-lae and papules that progress to erosions
secondary toepidermal necrosis. The pattern of distribution of
skinlesions in people is distinctive, involving the face, abdo-men,
perineum, groin, thighs, as well as sites of fric-tion.31The
intensity of the dermatosis typically waxesand wanes.62Accompanied
by elevated serum gluca-gon concentrations, glucose intolerance or
mild diabe-tes mellitus, hypoaminoacidaemia, stomatitis,
diarrhoea
and weight loss, NME is a common feature of the con-stellation
of symptoms known asglucagonoma syndromein people.4,31,62Notably,
the dermatosis also occurs ina small proportion of people without
pancreatictumours who suffer from benign or malignant liver
dis-ease, enteropathy or chronic pancreatitis.6366However,by far
the majority of NME cases are associated withthe glucagonoma
syndrome.63
Superficial necrolytic dermatitis in dogs shares manyfeatures
with NME.67However, in contrast to people,SND in dogs appears to
occur far more commonly inassociation with hepatopathy than with
glucagon-secreting neoplasia,67giving rise to the familiar name
of hepatocutaneous syndrome. There are seven reportedcases of
paraneoplastic SND associated with glucagon-secreting tumours in
dogs6873and one case of pancre-atic carcinoma in a cat.74In two of
the reported dogs,
glucagonoma occurred in the liver without a histologi-cally
detectable pancreatic tumour.69,73
The main presenting complaints of glucagonoma-associated SND are
progressive skin lesions of 3 weeksto many months,6873with
concurrent lethargy and inap-petance in some dogs.69,70,73 Major
dermatologicalfindings include erosions and ulcerations, with
alopecia,exudation and adherent crusts on the feet, pressurepoints
such as the elbows and hocks, flank, perinealarea, muzzle, facial
mucocutaneous junctions and/ororal cavity.6871,73Hyperkeratosis and
fissuring of footpads occur in all animals (Fig. 5).6871,73Lesions
maybe painful and pruritic.70,71All five dogs in whom mea-
surement was performed had hyperglucagonaemia6973and all but
one71 were hyperglycemic.6870,72,73Theselaboratory abnormalities
are not, however, specific forglucagon-secreting tumours, as
similar changes arefound in dogs with SND-related
hepatopathy.75Plasmaamino acid levels were measured in three of
thereported dogs and all had marked hypoaminoacidae-mia involving
various amino acids.70,71,73,75Hypoami-noacidaemia may therefore
represent a commonfeature of paraneoplastic SND in dogs, although
italso is nonspecific. Interestingly, a recent report evalu-ated
plasma amino acid concentrations in dogs with
nonglucagonoma-associated SND.
76
When comparedwith normal dogs and dogs with acute or chronic
hepa-titis whose circulating amino acid levels are increasedowing
to decreased hepatic metabolism, the plasmaamino acid
concentrations of dogs with SND weresignificantly lower.76These
disparities suggest that thepathogenesis of SND is likely not
related to compro-mised hepatic function as postulated
previously.76In thatreport, the mean values of all amino acids,
with theexception of glutamic acid, phenylalanine, tryptophanand
ornithine, were 60% or less in dogs with SND thanin normal dogs,
and the total amino acid concentrationwas 30% that of normal
dogs.76
Similar to NME in people, the histopathologicalfindings of SND
are distinctive and can be stronglysuggestive of the diagnosis. The
epidermis has ared, white and blue appearance when stained with
Figure 5. Superficial necrolytic dermatitis in a dog. The foot
padsare proliferative, crusted and fissured. (Photograph courtesy
of DrLynette Phillips.)
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
12/18
290 M. M. Turek
2003 European Society of Veterinary Dermatology, Veterinary
Dermatology, 14, 279296
haematoxylin and eosin (Fig. 6). Parakeratotic hyper-keratosis
and crusting create the upper eosinophilic layer.Oedema and
necrosis of keratinocytes in the stratumspinosum make up the pale
middle layer. Hyperplasticbasal cells give rise to the deep
basophilic layer.67,77Inaddition, secondary clefting can occur at
the level ofthe devitalized middle layer, which may lead to
ulcera-tion.6772,74,75,77A mixed, inflammatory infiltrate mayoccupy
the dermis.
Skin biopsy of intact, crusted lesions is the key todiagnosis of
SND and can help differentiate other pos-
sible differential diagnoses such as erythema multi-forme, drug
eruption, pemphigus foliaceus, systemiclupus erythematosus,
contact-irritant dermatitis, and,although less likely in the
presence of foot pad involve-ment, demodicosis, dermatophytosis and
bacterial fol-liculitis.6772,74,75,77Furthermore, SND can, in
certaincases, histopathologically resemble other disorders
inclu-ding zinc-responsive dermatosis, generic dog food der-matosis
and mucocutaneous candidiasis.77The presenceof internal metabolic
disease is the principal differentiatingfeature in these cases.
Useful diagnostic tests, in addition to skin biopsy,
include a serum biochemistry panel, serum bile acidevaluation
and abdominal ultrasonography. If liverdisease, the more common
SND-associated internaldisorder, is not supported by these tests,
investigationshould be directed toward glucagonoma.
Hypoami-noacidaemia and hyperglycaemia may be helpful butare
nonspecific for the diagnosis, as mentioned above.77
An elevated serum glucagon concentration can be use-ful but is
also non-specific.77Moreover, the accuracy ofthe human glucagon
assay in measuring glucagon con-centrations in dogs has been
questioned because of itslimited use in veterinary
medicine.67,78Abdominal ultra-sonography is an important diagnostic
tool, although
false-negative examinations can occur given the inher-ent
difficulty of imaging the pancreas.79In light of thepancreas small
size, similar echogenicity to surround-ing structures and close
proximity to gas-containing
gastrointestinal organs, visualization of the pancreasmay be
incomplete.80Therefore, the lack of abnormal-ities on an ultrasound
examination does not excludepancreatic disease.79,80To this effect,
four of the five dogsreported herein with confirmed pancreatic
glucagonomahad false-negative ultrasound examinations.68,7072
However, the use of more sophisticated ultrasoundequipment by
experienced ultrasonographers mayimprove the accuracy of pancreatic
assessment.79 Inhuman medicine, computed tomography and
magneticresonance imaging are commonly used to evaluate
thepancreas.79To date, these modalities are not in stand-ard use
for abdominal imaging of veterinary patients.79
Therefore, exploratory laparotomy may be indicated incases when
SND is suspected based on clinical and his-topathological findings
of skin lesions and where thereis no evidence of hepatopathy or
pancreatic neoplasiaafter routine diagnostic testing. Because
glucagon isproduced by alpha cells in the pancreas, stomach
andduodenum, all of these organs should be
thoroughlyevaluated.75Glucagon immunoreactivity on
immuno-histochemical staining of tumour cells was present inall
seven reported canine cases,6872and therefore appearsto be highly
supportive of a diagnosis of glucagonomain dogs, as it is in
people.62In people, staining intensitydoes not relate to the
severity of hormonal symptoms.62
Tumour tissue can also be variably immunoreactive forother
pancreas-derived hormones including insulin,islet amyloid
polypeptide, pancreatic polypeptide andsomatostatin.68,71,72
The pathogenesis of SND in dogs and NME in peo-
ple is unknown. It has been suggested that because glu-cagon
results in sustained gluconeogenesis and is involvedin the
catabolism of amino acids, chronic elevation ofthe hormone, as seen
in association with glucagono-mas, may be the direct cause of
hypoaminoacidaemia,which may lead to epidermal protein depletion
andsubsequent keratinocyte necrolysis.65,67,68,70,71 Thishypothesis
is supported by the rapid dermatologicalimprovement that is seen in
people (and one dog)71
after surgical resection of the tumour62,63or with
glucagon-inhibiting somatostatin analogue treatment,62,63 aswell as
by the temporary resolution of skin lesions in
people after intravenous infusion of amino acids.
81,82
However, and not in accordance with this hypothesis,the
dermatosis also occurs in individuals, both humanand canine, with
glucagon concentrations within thenormal range.66,70,71,78In an
effort to explain this, ithas been proposed that because glucagon
exists innumerous immunoreactive fractions,65,67,75 the assayused
to measure concentrations of the hormone maybe insensitive to some
glucagon species.67,78In people,pancreatic glucagon consists of at
least four fractions,each of a different molecular mass.65,67,75The
biologi-cally active species has a molecular mass of 3500 Daand is
accurately measured by human bioassays.65,75
Other fractions include the 90 000 Da big glucagon,the 9000 Da
proglucagon, and the low molecularmass glucagon of 3000
Da.65,67,75Gut-derived gluca-gon exists in two fractions (3500 and
7000 Da) and is
Figure 6. Superficial necrolytic dermatitis in a dog. The
epidermishas a layered, red, white and blue appearance: diffuse
parakeratosis(thick arrow), intracellular oedema in the spinous
layer (thin arrow),and basal cell hyperplasia (arrowhead). H&E,
original magnification31.2. (Photomicrograph courtesy of Dr Michael
Goldschmidt.)
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
13/18
2003 European Society of Veterinary Dermatology, Veterinary
Dermatology, 14, 279296
Cutaneous paraneoplastic syndromes 291
indistinguishable from pancreatic glucagon.65,67 Glu-cagon
metabolism is handled by the kidney and liver,the latter
responsible primarily for extraction andmetabolism of the 3500 Da
fraction.75It appears thatthe fractional breakdown of glucagon in
the dog is sim-ilar to that described in people.65,75However, it
remains
to be established whether NME or SND are related tosome unusual
combination of different glucagon frac-tions that could explain the
lack of correlation betweenhormone levels and clinical
signs.65,67The existence ofan uncharacterized glucagon-like peptide
has also beenhypothesized.67
Alternatively, it has also been proposed that gluca-gon may not
be directly related to the development ofskin lesions. Because many
human patients with gluca-gonoma syndrome experience diarrhoea and
malab-sorption and occasionally have concurrent deficienciesof
serum zinc and/or fatty acid levels, and given thesimilarity of the
corresponding cutaneous lesions withNME, deficiencies in zinc and/
or fatty acids have beenhypothesized to have an aetiologic role in
the dermati-tis.63However, this theory has since fallen out of
favourdue to a lack of clinical response associated with
sup-plementation of zinc and/or fatty acids in people.63
Similarly, SND was refractory to zinc supplements inthree dogs
with glucagonoma,69,71,83 although sometemporary improvement is
reported in association withhepatopathy-related SND.67,75Fatty acid
supplemen-tation, reported in one dog, did not result in a
clinicalresponse.70
Finally, hepatic impairment has also been implicated
as a possible mechanism.63,75 Intuitively, this seems
areasonable theory in light of the more frequent associ-ation of
SND with hepatopathy than pancreaticneoplasia in the dog.
Interestingly, many although notall canine and human patients with
hepatopathy-related SND/ NME also have elevated serum
glucagonlevels.66,70,75,78This may further support the implica-tion
of liver impairment in the pathogenesis of the con-dition, perhaps
by way of decreased metabolism ofglucagon.66,67,75
There is no currently known effective therapy forparaneoplastic
SND in dogs. Surgical resection of the
malignancy is the therapy of choice. Although excisionof
localized glucagonoma usually results in rapid anddurable
resolution of skin lesions in people, the major-ity of human
patients present with metastasis at the timeof diagnosis.62Even in
these cases, a debulking proce-dure is often recommended, as
reduction in tumourburden will lead to significant palliation of
symptomsin 75% of patients.62 Several reports in dogs havedescribed
temporary clinical improvement of cutane-ous lesions with
glucocorticosteroid therapy.68,69,75,83
However, the state of glucose intolerance of many dogswith SND
and the risk of inducing diabetes mellituspreclude their
use.67,75In people, glucagon-inhibiting
somatostatin and the long-acting somatostatin
analogue,octreotide, are associated with significant improve-ment
of NME.62,84Interestingly, serum glucagon levelsand tumour size are
often not influenced by this treat-
ment.62The use of somatostatin has not been evaluatedin canine
patients, although its efficacy has been des-cribed anecdotally in
one dog with metastatic gluca-gonoma that experienced
dermatological improvementwithin 14 days.3 Improvement is also seen
in somehumans treated with amino acid infusions.62To this
effect,
amelioration of skin lesions has been described in dogswith
hepatopathy-related SND after dietary supple-mentation with egg
yolk, resulting in concurrent impro-vement of decreased serum amino
acid levels.78Fromthis, feeding of a high-quality protein diet has
been rec-ommended.67Anecdotal reports of amino acid infu-sion in
dogs with SND suggest remarkable alleviationof cutaneous signs with
this therapy.67Finally, chemo-therapeutic agents appear to have
little antitumour acti-vity against human glucagonoma.62However,
durabletumour regression has occasionally been observed inpeople
using various drug combinations of streptozotocin,5-fluorouracil
and dacarbazine.62
There exists little information regarding the out-come of dogs
with SND and glucagonoma. One reportdocuments complete resolution
of SND, as well as nor-malization of hyperglucagonaemia and
hypoaminoaci-daemia, following excision of the tumour and its
nodalmetastasis.71This supports the classification of somecases of
SND as a PNS. Among the remaining casesreported, three dogs were
diagnosed with pancreaticneoplasia only at necropsy69,70,72and, in
two otherdogs, postsurgical pancreatitis resulted in death
afterexcision of solitary neoplastic tissue.68 Metastasis,involving
the liver and /or lymph nodes, was reported in
the three dogs in which a diagnosis was not establisheduntil the
time of necropsy. This further underscores theimportance of
recognizing SND as a possible markerof neoplasia in the dog,
allowing perhaps for earlierdiagnosis and prompt treatment of a
cancer that mightotherwise go undetected until late in the course
of disease.
PARANEOPLASTIC PEMPHIGUS
In people, paraneoplastic pemphigus (PNP) is an un-common, but
well-characterized, immune-mediated
blistering disorder associated with both benign andmalignant
lymphoproliferative processes (Table 1). Asthe name implies, it
shares some similarities with clas-sic pemphigus, notably pemphigus
vulgaris (PV), buthas recently emerged as a distinct PNS of
autoimmunepathogenesis. It differs from PV in its clinical
features,histological characteristics, immunofluorescent
patterns,systemic involvement, association with neoplasia,
res-ponsiveness to therapy, prognosis and pathophysiol-ogy.85In
veterinary medicine, one case of canine PNP,confirmed by molecular
immunological techniques,has been reported.86Further investigation
of immu-nopathological features has demonstrated a similar
target antigen profile to the human counterpart.87The cutaneous
lesions of PNP in people are charac-
terized by vesicobullous changes, reminiscent of pem-phigus
vulgaris or erythema multiforme, affecting the
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
14/18
292 M. M. Turek
2003 European Society of Veterinary Dermatology, Veterinary
Dermatology, 14, 279296
head, trunk and extremities.85,88Intractable stomatitisis a
consistent feature in people and is usually the firstsign of
disease. Oral erosive lesions are more severethan in PV and extend
from the mouth to the uppergastrointestinal and respiratory tracts.
Unlike in classicpemphigus, in which lesions arise from otherwise
normal
appearing skin, erythema and inflammation is alwaysassociated
with the maculae, papules and plaques inPNP, resembling the
appearance of erythema multi-forme.85 Conjunctival involvement
occurs in mosthuman patients.88In addition, and distinct from
classicpemphigus, many people with PNP develop fatal respi-ratory
involvement wherein aspiration of sloughed,immune-targeted
bronchial epithelial cells results inocclusion of smaller airways
and alveoli.85
Histopathological findings of mucocutaneous lesions,including
suprabasal cleft-forming acantholysis withan attached rim of basal
keratinocytes (tombstoneappearance), resemble those of PV. Unique
to PNP,however, is the presence of dyskeratotic or
necrotickeratinocytes located at all levels of the epidermis,basal
vacuolization and intense epidermal exocytosisof cytotoxic
lymphocytes, natural killer cells and mac-rophages.85,88,89In
addition, the degree of acantholysisis less prominent compared to
PV.88
In human PNP, direct immunofluorescence allowsidentification of
deposition of immunoglobulin G andcomplement in epidermal
intercellular spaces as well asalong the basement membrane of
affected tissues. Con-trarily, in PV immunoreactants are found only
in theintercellular spaces in both people and dogs.85,90With
indirect immunofluorescence of human cases usingpatient serum,
patient antibodies stain various normalepithelial tissue
substrates, including human or rodentskin, oesophagus, bladder and
airways.85Immunopre-cipitation and immunoblotting techniques allow
forthe isolation and detection of the autoantibodies inhuman
patient serum that bind the cellular adhesionproteins specifically
targeted in PNP, and are the mostdefinitive tests for diagnosis of
the disorder.85,88,89,91
Specifically, these targets are proteins of 250, 230, 210,190
and 170 kDa that have been identified as membersof the plakin
family, constituent proteins of desmo-
somes and hemidesmosomes: desmoplakin I (250 kDa),bullous
pemphigoid antigen 1 (230 kDa), envoplakinand desmoplakin II (both
210 kDa) and periplakin(190 kDa). The 170 kDa protein is as yet
unidenti-fied.85,88,92In contrast, the major pemphigus
vulgarisantigen is a 130-kDa protein, desmoglein 3.3,89
In people, PNP is most commonly associated withthymoma and
lymphoproliferative malignancies, par-ticularly non-Hodgkins
lymphoma and chronic lym-phocytic leukaemia.88Isolated human cases
have alsobeen reported with acute myelogenous leukaemia, pul-monary
squamous cell carcinoma, sarcoma, Walden-stroms macroglobulinaemia
and Castlemans disease,
a nonmalignant lymphoproliferative disorder.7 Neo-plasia almost
always develops prior to mucocutaneouslesions.85PNP is reported to
be potentially triggered byradiotherapy.93,94With the exception of
cases of thy-
moma, in which excision typically results in resolutionof PNP,
prognosis related to skin lesions is poor evenin the face of
successful treatment of the underlyingneoplasia.88The mortality
rate in people is 90% withpatients generally succumbing to sepsis,
multiorganfailure or respiratory failure.88Unlike classic
pemphigus,
treatment with glucocorticoids or immunosuppressivedrugs almost
never results in improvement of lesions.85,88
In summary, human PNP is defined by the followingcriteria:
1 Mucocutaneous eruption with blisters and/orerosions.
2 Histological features including epidermal acantho-lysis,
keratinocyte necrosis, and vacuolar interfacedermatitis.
3 Epidermal and basement membrane-zone deposi-tion of
immunoglobulin G and complement (viadirect immunofluorescence).
4 Detection of serum autoantibodies reactive to nor-mal
epithelia (via indirect immunofluorescence).
5 Immunoprecipitation with serum antibodies ofthe above
characteristic complex of proteins.88,89
In the only reported veterinary case of PNP, a 7-yearold Bouvier
dog presented with anorexia and severeerosive and ulcerative oral
lesions.86Cutaneous vesi-cobullous lesions developed on the head
and progressedto the extremities and trunk. Mediastinal lymphomawas
diagnosed at necropsy. Fulfilling four of the fivecriteria
described above, a diagnosis of PNP was made
based on histology of skin biopsies, indirect
immun-ofluorescence using normal canine lip as well as
bovinebladder epithelium as substrate, and Western blot anal-ysis
using extracts of canine lip epithelium. Blot analysisrevealed the
presence of autoantibodies against two proteinsof 210 and 190 kDa,
confirming PNP. Direct immunoflu-orescence was not performed due to
lack of preservedtissue. Further immunopathological investigation
con-firmed target antigen proteins of 210, 190 and 170 kDain canine
PNP and identified the first two as envo-plakin and periplakin,
respectively.87The authors con-cluded that PNP exists in the dog
and resembles the
human disease, making it an excellent comparativemodel.87 In
addition, a published report of a horsediagnosed with bullous
stomatitis in association withhaemangiosarcoma describes
histopathological features,indirect immunofluorescence reactivity
and immuno-precipitation characteristics of human PNP.95
This article describes cutaneous PNSs recognized inveterinary
medicine. These syndromes are reported rela-tively rarely compared
with human medicine, whichmay indicate true rarity of occurrence in
animals or alack of recognition by clinicians. This latter
possibilityis supported by the multiple individual case reports
ofuncharacterized skin lesions that occur in association
with neoplasia.9699 Recognition of these and otherskin lesions
as possible indicators of cancer may allowfor earlier diagnosis of
malignancy which may result inimproved survival. Based on the
literature, the presence
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
15/18
2003 European Society of Veterinary Dermatology, Veterinary
Dermatology, 14, 279296
Cutaneous paraneoplastic syndromes 293
of most cutaneous PNSs would seem to indicate a poorprognosis.
However, given the overall paucity of reportsof attempted therapy
for the underlying neoplasm, andthe possibility of successful
treatment as reported in afew cases, accurate assessment of
prognosis is not possi-ble in most cases at this time.
ACKNOWLEDGEMENTS
Photos courtesy of Dr Elizabeth Mauldin (Fig. 1,
felineparaneoplastic alopecia; Figs 2 and 3, feline
thymoma-associated exfoliative dermatitis), Prof Dr FrodeLingaas
(Fig. 4, nodular dermatofibrosis), Dr LynettePhillips (Fig. 5,
superficial necrolytic dermatitis, gross)and Dr Michael Goldschmidt
(Fig. 6, superficial necro-lytic dermatitis, photomicrograph). The
author is gratefulto Dr Elizabeth Mauldin for editorial assistance
withphotomicrograph figure legends.
REFERENCES
1. Nathanson, L., Hall, T.C. Introduction:
paraneoplasticsyndromes. Seminars in Oncology1997; 24: 2658.
2. Fox, L.E. The paraneoplastic disorders. In: Bonagura,
J.D.,Kirk, R.W., eds. Kirks Current Veterinary Therapy XII:Small
Animal Practice. W.B. Saunders, Philadelphia,1995: 53042.
3. Scott, D.W., Miller, W.H., Griffin, C.E.Muller and KirksSmall
Animal Dermatology, 6th edn. W.B. Saunders,Philadelphia, 2001.
4. Weiss, P., ORourke, M.E. Cutaneous paraneoplastic
syndromes. Clinical Journal of Oncology Nursing2000;4: 257
62.
5. Sabir, S., James, W.D., Schuchter, L.M.
Cutaneousmanifestations of cancer. Current Opinion in Oncology1999;
11: 139 44.
6. Politi, Y., Ophir, J., Brenner, S. Cutaneous
paraneoplasticsyndromes. Acta Dermato-Venereologica1993; 73:
16170.
7. Cohen, P.R., Kurzrock, R. Mucocutaneous paraneo-plastic
syndromes. Seminars in Oncology 1997; 24 (3):33459.
8. Kurzrock, R., Cohen, P.R. Cutaneous paraneoplasticsyndromes
in solid tumors. American Journal of Medi-cine1995; 99: 662 71.
9. Kurzrock, R., Cohen, P.R. Mucocutaneous paraneo-plastic
manifestations of hematologic malignancies.American Journal of
Medicine1995; 99: 207 16.
10. Ellis, D.L., Kafka, S.P., Chow, J.C. et al.Melanoma,growth
factors, acanthosis nigricans, the sign of Leser-Trlat, and
multiple acrochordons: a possible role foralpha-transforming growth
factor in cutaneous parane-oplastic syndromes. New England Journal
of Medicine1987; 317(25): 15827.
11. Wilgenbus, K., Lentner, A., Kuckelkorn, R. et
al.Furtherevidence that acanthosis nigricans maligna is linked
toenhanced secretion by the tumour of transforminggrowth factor
alpha. Archives of Dermatological Re-search1992; 284(25):
26670.
12. Koyama, S., Kazuho, I., Sato, M. et al. Transforminggrowth
factor-alpha (TGF)-producing gastric carci-noma with acanthosis
nigricans: an endocrine effect ofTGFin the pathogenesis of
cutaneous paraneoplastic
syndrome and epithelial hyperplasia of the esophagus.Journal of
Gastroenterology1997; 32: 717.
13. Chosidow, O., Bcherel, P.-A., Piette, P.-C. et al.Tripepalms
associated with systemic mastocytosis: the role oftransforming
growth factor-and efficacy of interferon-alfa. British Journal of
Dermatology 1998; 138: 698703.
14. Bolognia, J.L., Brewer, Y.P., Cooper, D.L. Bazex
syndrome(acrokeratosis paraneoplastica): an analytic review.
Medi-cine1991; 70(4): 26980.
14a.Braverman, I.M. Skin manifestations of internal malig-nancy.
Clinics in Geriatric Medicine2002; 18(1): 1 19.
15. Hashimoto, K. Regulation of keratinocyte function bygrowth
factors. Journal of Dermatological Science2000;24(Suppl. 1): S46
S50.
16. Mendelsohn, J. The epidermal growth factor receptor asa
target for cancer therapy. Endocrine-Related Cancer2001; 8: 39.
17. Normanno, N., Bianco, C., De Luca, A. et al.The role
ofEGF-related peptides in tumor growth. Frontiers in Bio-
science2001; 6: D685707.17a.Agarwala, S.S. Paraneoplastic
syndromes. Medical Clinicsof North America1996; 80(1): 17384.
18. Matsuoka, L.Y., Goldman, J.G., Wortsman, J. et al.Antibodies
against the insulin receptor in paraneoplasticacanthosis nigricans.
American Journal of Medicine1987; 82: 1253 6.
19. Brooks, D.G., Campbell, K.L., Dennis, J.S.et al.Pancre-atic
paraneoplastic alopecia in three cats. Journal of theAmerican
Animal Hospital Association1994; 30: 55763.
20. Pascal-Tenorio, A., Olivry, T., Gross, T.L. et
al.Paraneo-plastic alopecia associated with internal malignancies
inthe cat. Veterinary Dermatology1997; 8: 4752.
21. Godfrey, D.R. A case of feline paraneoplastic alopecia
with secondary Malassezia-associated dermatitis. Journalof Small
Animal Practice1998; 39: 3946.
22. Tasker, S., Griffon, D.J., Nuttall, T.J. et al.Resolution
ofparaneoplastic alopecia following surgical removal of apancreatic
carcinoma in a cat. Journal of Small AnimalPractice1999; 40:
1619.
23. Mauldin, E.A., Morris, D.O., Goldschmidt, M.H.
Ret-rospective study. The presence of Malassezia in felineskin
biopsies. A clinicopathological study. VeterinaryDermatology2002;
13: 713.
24. Barrs, V.R., Martin, P., France, M. et al.What is
yourdiagnosis? Journal of Small Animal Practice 1999; 40:5946.
25. Withrow, S.J. Exocrine cancer of the pancreas. In:Withrow,
S.J., MacEwen, E.G., eds. Small Animal ClinicalOncology, 3rd edn.
W.B. Saunders, Philadelphia, 2001,3213.
26. Thamm, D.H. Hepatobiliary tumors. In: Withrow, S.J.,MacEwen,
E.G., eds. Small Animal Clinical Oncology,3rd edn. W.B. Saunders,
Philadelphia, 2001, 327 34.
27. Scott, D.W., Yager, J.A., Johnston, K.M. Exfoliative
der-matitis in association with thymoma in three cats.
FelinePractice1995; 23: 813.
28. Carpenter, J.L., Holzworth, J. Thymoma in 11 cats.Jour-nal
of American Veterinary Medical Association 1982;181: 248 51.
29. Loveday, R.K. Thymoma in a Siamese cat.Journal of the
South African Veterinary Medical Association1959; 30:334.
30. Forster-Van Hijfte, M.A., Curtis, C.F., White,
R.N.Resolution of exfoliative dermatitis and Malassezia
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
16/18
294 M. M. Turek
2003 European Society of Veterinary Dermatology, Veterinary
Dermatology, 14, 279296
pachydermatisovergrowth in a cat after surgical
thymomaresection. Journal of Small Animal Practice 1997;
38:4514.
31. Boyce, S., Harper, J. Paraneoplastic dermatoses.Derma-tology
Clinics2002; 20: 523 32.
32. Godfrey, D.R. Dermatosis and associated systemic signsin a
cat with thymoma and recently treated with an imi-
dacloprid preparation.Journal of Small Animal Practice1999; 40:
3337.
33. Withrow, S.J. Thymoma. In: Withrow, S.J., MacEwen, E.G.,eds.
Small Animal Clinical Oncology, 3rd edn. W.B.
Saunders,Philadelphia, 2001: 64651.
34. Suter, M., Lott-Stolz, G., Wild, P. Generalized
nodulardermatofibrosis in six Alsatians. Veterinary Pathology1983;
20: 6324.
35. Lium, B., Moe, L. Hereditary multifocal renal
cystaden-ocarcinomas and nodular dermatofibrosis in the
Germanshepherd dog: macroscopic and histologic changes.Veterinary
Pathology1985; 22: 447 55.
36. Cosenza, S.F., Seely, J.C. Generalized nodular der-
matofibrosis and renal cystadenocarcinomas in aGerman shepherd
dog. Journal of American MedicalAssociation1986; 189: 1587 90.
37. Gilbert, P.A., Griffin, C.E., Walder, E.J. Nodular
der-matofibrosis and renal cystadenoma in a Germanshepherd dog.
Journal of American Animal HospitalAssociation1990; 26: 2536.
38. Atlee, B.A., DeBoer, D.J., Ihrke, P.J. et al.Nodular
der-matofibrosis in German shepherd dogs as a marker forrenal
cystadenocarcinoma. Journal of American AnimalHospital
Association1991; 27: 4817.
39. Moe, L., Lium, B. Hereditary multifocal renal
cystaden-ocarcinomas and nodular dermatofibrosis in 51 Ger-man
shepherd dogs. Journal of Small Animal Practice
1997; 38: 498505.40. Jnasdttir, T.J., Mellersh, C.S., Moe, L. et
al.
Genetic mapping of a naturally occurring hereditaryrenal cancer
syndrome in dogs. Proceeding of theNational Academy of Science of
the USA2000; 97(8):41327.
41. Marks, S.L., Farman, C.A., Peaston, A. Nodular
der-matofibrosis and renal cystadenomas in a goldenretriever.
Veterinary Dermatology1994; 4: 1337.
42. Moe, L., Gamlem, H., Jnasdttir, T.J. et al. Renalmicroscopic
tubular lesions in two 1-year-old dogs anearly sign of hereditary
renal cystadenocarcinoma?Journal of Comparative Pathology2000; 123:
218 21.
43. Hayes, H.M. Jr., Pendergrass, T.W. Canine testiculartumors:
epidemiologic features of 410 dogs. Interna-tional Journal of
Cancer1976; 18: 4827.
44. Reif, J.S., Brodey, R.S. The relationship between
cryp-torchidism and canine testicular neoplasia. Journal ofthe
American Veterinary Medical Association1969; 155(12): 200510.
45. Cooley, D.M., Waters, D.J. Tumors of the male repro-ductive
system. In: Withrow, S.J., MacEwen, E.G., eds.Small Animal Clinical
Oncology, 3rd edn. W.B. Saunders,Philadelphia, 2001, 47889.
46. Lipowitz, A.J., Schwartz, A., Wilson, G.P. et al.Testicu-lar
neoplasms and concomitant clinical changes in thedog. Journal of
the American Veterinary Medical Asso-
ciation1973; 163(12): 13648.47. Weaver, A.D. Survey with
follow-up of 67 dogs with
testicular Sertoli cell tumours. Veterinary Record 1983;113:
1057.
48. Morgan, R.V. Blood dyscrasias associated with testicu-lar
tumors in the dog. Journal of the American AnimalHospital
Association1982; 18: 9705.
49. Suess, R.P. Jr., Barr, S.C., Sacre, B.J.et al.Bone
marrowhypoplasia in a feminized dog with an interstitial celltumor.
Journal of the American Animal Hospital Asso-ciation1992; 200(9):
13468.
50. Peters, M.A.J., de Jong, F.H., Teerds, K.J. et
al.Ageing,testicular tumours and the pituitarytestis axis in
dogs.Journal of Endocrinology2000; 166: 153 61.
51. Peters, M.A.J., Teerds, K.J., van der Gaag, I. et al.Useof
antibodies against LH receptor, 3-hydroxysteroiddehydrogenase and
vimentin to characterize differenttypes of testicular tumour in
dogs. Reproduction 2001;121: 287 96.
52. Sanpera, N., Masot, N., Janer, M. et al. Oestrogen-induced
bone marrow aplasia in a dog with a Sertolicell tumour. Journal of
Small Animal Practice2002; 43:3659.
53. Fadok, V.A., Lothrop, C.D. Jr., Coulson, P. Hyperpro-
gesteronemia associated with Sertoli cell tumor andalopecia in a
dog. Journal of the American VeterinaryMedical Association1986;
188(9): 10589.
54. Edwards, D.F. Bone marrow hypoplasia in a feminizeddog with
a Sertoli cell tumor. Journal of the AmericanVeterinary Medical
Association1981; 178(5): 494 6.
55. Lindberg, R., Jonsson, O.-J., Kasstrm, H. Sertoli
celltumours associated with feminization, prostatitis andsquamous
metaplasia of the renal tubular epithelium ina dog. Journal of
Small Animal Practice1976; 17: 4518.
56. Sherding, R.G., Wilson, G.P., Kociba, G.J. Bone
marrowhypoplasia in eight dogs with Sertoli cell tumor. Journalof
the American Veterinary Medical Association 1981;178(5):
497501.
57. Kawakami, E., Hori, T., Tsutsui, T. Relationship bet-ween
testicular transferrin and plasma estradiol-17concentrations of
dogs with azoospermia and dogs withSertoli cell tumors. Journal of
Veterinary Medical Sci-ence2001; 63(5): 57981.
58. Comhaire, F., Mattheeuws, D., Vermeulen, A. Testoster-one
and oestradiol in dogs with testicular tumours.
ActaEndocrinologica1974; 77: 408 16.
59. Siegel, E.T., Forchielli, E., Dorfman, R.I. et al.An
estro-gen study in the feminized dog with testicular
neoplasia.Endocrinology1967; 80: 2727.
60. Pierrepoint, C.G. The metabolismin vitroof
dehydroepi-androsterone and dehydroepiandrosterone sulfate by
Sertoli cell tumors of the testis of two dogs with clinicalsigns
of hyperestrogenism. Journal of Endocrinology1968; 42: 99107.
61. Mischke, R., Meurer, D., Hoppen, H.-O. et al.Bloodplasma
concentrations of oestradiol-17, testosteroneand
testosterone/oestradiol ratio in dogs with neoplas-tic and
degenerative testicular diseases. Research inVeterinary
Science2002; 73: 26772 .
62. Wermers, R.A., Fatourechi, V., Wynne, A.G. et
al.Theglucagonoma syndrome: clinical and pathologic fea-tures in 21
patients. Medicine1996; 75(2): 5363.
63. Kasper, C.S. Necrolytic migratory erythema. Unre-solved
problems in diagnosis and pathogenesis. A casereport and literature
review.Cutis1992; 49: 1208.
64. Doyle, J.A., Schroeter, A.L., Rogers, R.S. III.
Hyperglu-cagonaemia and necrolytic migratory erythema incirrhosis
possible pseudoglucagonoma syndrome. BritishJournal of
Dermatology1979; 100: 5817.
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
17/18
2003 European Society of Veterinary Dermatology, Veterinary
Dermatology, 14, 279296
Cutaneous paraneoplastic syndromes 295
65. Kasper, C.S., McMurry, K. Necrolytic migratory ery-thema
without glucagonoma versus canine superficialnecrolytic dermatitis:
is hepatic impairment a clue topathogenesis? Journal of the
American Academy of Der-matology1991; 25: 534 41.
66. Marinkovich, M.P., Botella, R., Datloff, J. et
al.Necro-lytic migratory erythema without glucagonoma in
patients with liver disease. Journal of the American Acad-emy of
Dermatology1995; 32: 6049.
67. Byrne, K.P. Metabolic epidermal
necrosishepatocutaneoussyndrome. Veterinary Clinics of North
America: SmallAnimal Practice1999; 29(6): 133755.
68. Gross, T.L., OBrien, T.D., Davies, A.P. et
al.Glucagon-producing pancreatic endocrine tumors in two dogswith
superficial necrolytic dermatitis. Journal of Amer-ican Veterinary
Medical Association1990; 197: 161922.
69. Miller, W.H. Jr., Anderson, W.I., McCann, J.P.
Necrolyticmigratory erythema in a dog with a
glucagon-secretingendocrine tumor. Veterinary Dermatology1991; 2:
179 82.
70. Bond, R., McNeil, P.E., Evans, H. et al.Metabolic epi-
dermal necrosis in two dogs with different underlyingdiseases.
Veterinary Record1995; 136: 466 71.71. Torres, S.M.F., Caywood,
D.D., OBrien, T.D.et al.Reso-
lution of superficial necrolytic dermatitis followingexcision of
a glucagon-secreting pancreatic neoplasmin a dog. Journal of
American Animal Hospital Associ-ation1997; 33: 313 19.
72. Torres, S., Johnson, K., McKeever, P. et
al.Superficialnecrolytic dermatitis and a pancreatic endocrine
tumorin a dog. Journal of Small Animal Practice 1997; 38:24650.
73. Allenspach, K., Arnold, P., Glaus, T. et
al.Glucagon-producing neuroendocrine tumour associated
withhypoaminoacidaemia and skin lesions. Journal of
Small Animal Practice2000; 41: 4026.74. Patel, A., Whitbread,
T.J., McNeil, P.E. A case of meta-
bolic epidermal necrosis in a cat. Veterinary Dermatology1996;
7: 2216.
75. Miller, W.H., Scott, D.W., Buerger, R.G.et
al.Necrolyticmigratory erythema in dogs: a hepatocutaneous
syn-drome. Journal of American Animal Hospital Associa-tion1990;
26: 573 81.
76. Outerbridge, C.A., Marks, S.L., Rogers, Q.R. Plasmaamino
acid concentrations in 36 dogs with histologicallyconfirmed
superficial necrolytic dermatitis. VeterinaryDermatology2002; 13:
177 86.
77. Gross, T.L., Ihrke, P.J. Necrotizing diseases of the
epi-
dermis (superficial necrolytic dermatitis). In: Gross,
T.L.,Ihrke, P.J., Walder, E.J., eds. Veterinary Dermatopa-thology:
A Macroscopic and Microscopic Evaluation of
Canine and Feline Skin Disease. Mosby Year Book, St.Louis, MO,
1992, 468.
78. Gross, T.L., Song, M.D., Havel, P.J. et al.
Superficialnecrolytic dermatitis (necrolytic migratory erythema)in
dogs. Veterinary Pathology1993; 30: 7581.
79. Nyland, T.G., Mattoon, J.S., Herrgesell, E.J. et
al.Pancreas. In: Nyland, T.G., Mattoon, J.S., eds. SmallAnimal
Diagnostic Ultrasound, 2nd edn. W.B. Saunders,Philadelphia, 2002:
14457.
80. Cartee, R.E., Selcer, B.A., Hudson, J.A. et
al.PracticalVeterinary Ultrasound. Williams & Wilkins,
Philadel-
phia, 1995, 529.81. Norton, J.A., Kahn, C.R., Schiebinger, R. et
al.Amino
acid deficiency and the skin rash associated with gluca-gonoma.
Annals of Internal Medicine1979; 91: 213 15.
82. Shepherd, M.E., Raimer, S.S., Tyring, S.K. et al.Treat-ment
of necrolytic migratory erythema in glucagonomasyndrome.Journal of
the American Academy of Dermatology1991; 25: 92528.
83. Walton, D.K., Center, S.A., Scott, D.W. et
al.Ulcerativedermatitis associated with diabetes mellitus in the
dog: areport of four cases. Journal of American Animal Hospi-
tal Association1986; 22: 7988.84. Rosenbaum, A., Flourie, B.,
Chagnon, S. et al.Octre-
otide (SMS 201-995) in the treatment of metastaticglucagonoma:
report of one case and review of the liter-ature. Digestion1989;
42: 116 20.
85. Nguyen, V.T., Ndoye, A., Bassler, D.D. et
al.Classifica-tion, clinical manifestations, and
immunopathologicalmechanisms of the epithelial variant of
paraneoplasticautoimmune multiorgan syndrome. Archives of
Derma-tologica2001; 137: 193206.
86. Lemmens, P., de Bruin, A., de Meulemeester, J. et
al.Paraneoplastic pemphigus in a dog. Veterinary Derma-tology1998;
9: 127 34.
87. de Bruin, A., Muller, E., Wyder, M. et al.Periplakin
andenvoplakin are target antigens in canine and humanparaneoplastic
pemphigus. Journal of the AmericanAcademy of Dermatology1999; 40:
6825.
88. Allen, C.M., Camisa, C. Paraneoplastic pemphigus: areview of
the literature. Oral Diseases2000; 6: 208 14.
89. Horn, T.D., Anhalt, G.J. Histologic features of
paraneoplasticpemphigus. Archives of Dermatology1992; 128: 1091
5.
90. Gross, T.L., Ihrke, P.J. Bullous and vesicular diseases
ofthe epidermis and dermal-epidermal junction (pemphi-gus
vulgaris). In: Gross, T.L., Ihrke, P.J., Walder, E.J.,eds.
Veterinary Dermatopathology: A Macroscopic andMicroscopic
Evaluation of Canine and Feline Skin Dis-
ease. Mosby Year Book, St. Louis, 1992: 314.
91. Hashimoto, T., Amagai, M., Watanabe, K. et
al.Char-acterization of paraneoplastic pemphigus autoantigensby
immunoblot analysis. Journal of Investigative Derma-tology1995;
104: 829 34.
92. Kiyodawa, C. Envoplakin and periplakin are the
parane-oplastic pemphigus antigens. Kurume Medical Journal1999; 46:
718.
93. Lee, M., Kossard, S., Ho, K.K.L. et
al.Paraneoplasticpemphigus triggered by radiotherapy. Australian
Journalof Dermatology1995; 36: 206 10.
94. Fried, R., Lynfield, Y., Vitale, P. et
al.Paraneoplasticpemphigus appearing as bullous pemphigoid-like
erup-tion after palliative radiation therapy. Journal of the
American Academy of Dermatology1995; 29: 81517.95. Williams,
M.A., Dowling, P.M., Angarano, D.W. et al.Paraneoplastic bullous
stomatitis in a horse.Journal of theAmerican Veterinary Medical
Association1995; 207: 3314.
96. Finley, M.R., Rebhun, W.C., Dee, A. et al.Paraneoplas-tic
pruritus and alopecia in a horse with diffuse lym-phoma. Journal of
the American Veterinary MedicalAssociation1998; 213: 102 4.
97. Schwartzman, R.M. Cutaneous amyloidosis associatedwith a
monoclonal gammopathy in a dog. Journal of theAmerican Veterinary
Medical Association1984; 185: 1024.
98. Ashley, P.F., Bowman, L.A. Symmetric cutaneous necro-sis of
the hind feet and multicentric follicular lymphomain a cat. Journal
of the American Veterinary Medical
Association1999; 214: 211 14.99. Miller, W.H. Cutaneous flushing
associated with
intrathoracic neoplasia in a dog. Journal of the AmericanAnimal
Hospital Association1992; 28: 217 19.
-
8/10/2019 Cutaneous Paraneoplastic Syndromes in Dogs and Cats- A
Review of the Literature (Pages 279296)
18/18
296 M. M. Turek
Rsum Les syndromes cutans paranoplasiques reprsentent un
ensemble de dermatoses non cancreuses,associes la prsence d'une
tumeur interne. Le'ur diagnostic peut faciliter la dtection et le
traitement d'un cancersous-jacent. Plus de trente syndromes
diffrents ont t identifis chez l'homme, et seul un petit nombre
chez l'ani-mal. Ceci peut tre li une incidence plus faible chez
l'animal, ou un sous-diagnostic de telles lsions cutanes.La mise en
vidence d'une relation entre des lsions cutanes et la prsence d'une
noplasie peut tre difficile, moins que les lsions cutanes ne soient
rares et toujours associes un type particulier de tumeur, comme
c'estle cas pour la plupart des syndromes paranoplasiques dcrits en
mdecine vtrinaire. Parmi ces maladies, sont
dcrites l'alopcie paranoplasique fline, la dermatose exfoliative
associe un thymome, la deramtofibrosenodulaire, le syndrome de
fminisation associ une tumeur testiculaire, la dermatite
superficielle ncrolytiqueet le pemphigus paranoplasique. L'tiologie
de la plupart des syndromes paranoplasiques cutans est encorepeu
claire, la fois chez l'homme et chez l'animal.
Resumen Los sndromes paraneoplsicos cutneos son un grupo de
dermatosis no-cancerosas asociadas aenfermedades malignas internas.
Su reconocimiento puede facilitar la deteccin y el tratamiento
oportuno delcncer subyacente. Ms de treinta alteraciones de este
tipo se han identificado en la literatura cientfica humana,mientras
que solamente algunas se describen en veterinaria. Esto puede
reflejar una incidencia ms baja en losanimales comparada con la
presente en las personas o puede ser el resultado de la falta de
reconocimiento deuna asociacin entre ciertas lesiones de piel y una
neoplasia. Establecer una relacin entre una lesin cutnea yuna
neoplasia puede ser difcil a menos que las lesiones de piel sean
raras y casi siempre asociadas con un tipoparticular de tumor, como
es el caso de las dermatosis paraneoplsicas veterinarias
reconocidas. Entre stas estn
la alopecia paraneoplsica felina, la dermatitis exfoliativa
felina asociada a timomas, la dermatofibrosis nodular,el sndrome
del feminizacin asociado a tumores testiculares, la dermatitis
necroltica superficial y el penfigoparaneoplsico. La etiologa de la
mayora de los sndromes paraneoplsicos cutneos sigue siendo evasiva
tantoen humana como en animales.
Zusammenfassung Kutane paraneoplastische Syndrome sind eine
Gruppe nichtkanzerogener Dermatosen, diein Verbindung mit Tumoren
an inneren Organen auftretend. Ihre Diagnose kann den Nachweis und
die rech-tzeitige Behandlung der primren Krebserkrankung
erleichtern. Whrend in der humanmedizinischen Fachlit-eratur mehr
als dreissig solcher Erkrankungen dargestellt wurden, sind in der
veterinrmedizinischen Literaturnur wenige beschrieben. Dies mag auf
einer im Vergleich zum Menschen geringeren Hufigkeit beim
Tierberuhen, oder daran liegen, dass der Zusammenhang zwischen
bestimmten Hautlsionen und Neoplasien nichterkannt wird. Es kann
schwierig sein, eine Verbindung zwischen einer Hauterkrankung und
einer Neoplasie her-zustellen, es sei denn, es handelt sich um
Hautlsionen, die selten auftreten und fast immer mit einem
bestimmten
Tumortyp assoziiert sind, wie dies bei den meisten der in der
Veterinrmedizin bekannten paraneoplastischenDermatosen der Fall
ist. Hierunter fallen die feline paraneoplastische Alopezie, feline
Thymom-assoziierte exfo-liative Dermatitis, nodulre Dermatofibrose,
das mit testikulren Tumoren verbundene Feminisierungssyndrom,die
superfizielle nekrolytische Dermatitis und der paraneoplastischer
Pemphigus. ber die tiologie der meistenparaneoplastischen Syndrome
bei Mensch und Tier ist bisher wenig bekannt.



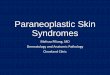








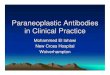


![Paraneoplastic Syndromes Associated with Laryngeal CancerLaryngeal cancers, regardless of histology, have rarely been associated with paraneoplastic syndromes [1, 2, 11–13]. In this](https://img.pdfslide.us/doc/110x75/5f0c10597e708231d43390f8/paraneoplastic-syndromes-associated-with-laryngeal-cancer-laryngeal-cancers-regardless.jpg)