Embed Size (px)
Citation preview
MEETING THE PRIMARY HEALTH CARE NEEDS OF
RURAL ASSAM THROUGH INTRODUCTION OF MID
LEVEL HEALTH CARE WORKERS- LESSONS FROM INDIA’S
EXPERIENCE WITH RURAL HEALTH PRACTITIONERS
DR. SUCHITRA LISAM, MBBS , MPH, PDCE
INTERNATIONAL CONFERENCE ON GLOBAL PUBLIC HEALTH 2014; 3th-4th
JULY, 2014, NEGOMBO, SRILANKA
BACKGROUND
• Lack of health workers is one of the main constraints in achieving population health goals in many countries including India
• India has 1 skilled service providers (doctors, nurses and midwives) per 1,000 population as against the international norm of 2.3 per 1,000 population to achieve 80 percent coverage of the population with skilled attendants at birth
• Majorities (70%) of health workers employed in private sector and 60% of these health workers reside in urban areas which skews the distribution of health workers
• Density of allopathic physicians in urban and rural areas was 11.3 and 1.9 respectively, reflecting the higher proportion of physicians reporting insufficient qualifications in rural areas.
INTERVENTIONS FOR ATTRACTION AND RETENTION OF HEALTH
WORKERS IN REMOTE & RURAL AREAS
Ref: WHO Global Policy Recommendations, 2010
A. Education
A1 Students from rural backgrounds
A2 Health professional schools outside of major cities
A3 Clinical rotations in rural areas during studies
A4 Curricula that reflect rural health issues
A5 Continuous professional development for rural health workers
B. Regulatory
B1 Enhanced scope of practice
B2 Different types of health workers
B3 Compulsory service
B4 Subsidized education for return of service
C. Financial incentives C1 Appropriate financial incentives
D. Professional and personal support
D1 Better living conditions
D2 Safe and supportive working environment
D3 Outreach support
D4 Career development programmes
D5 Professional networks
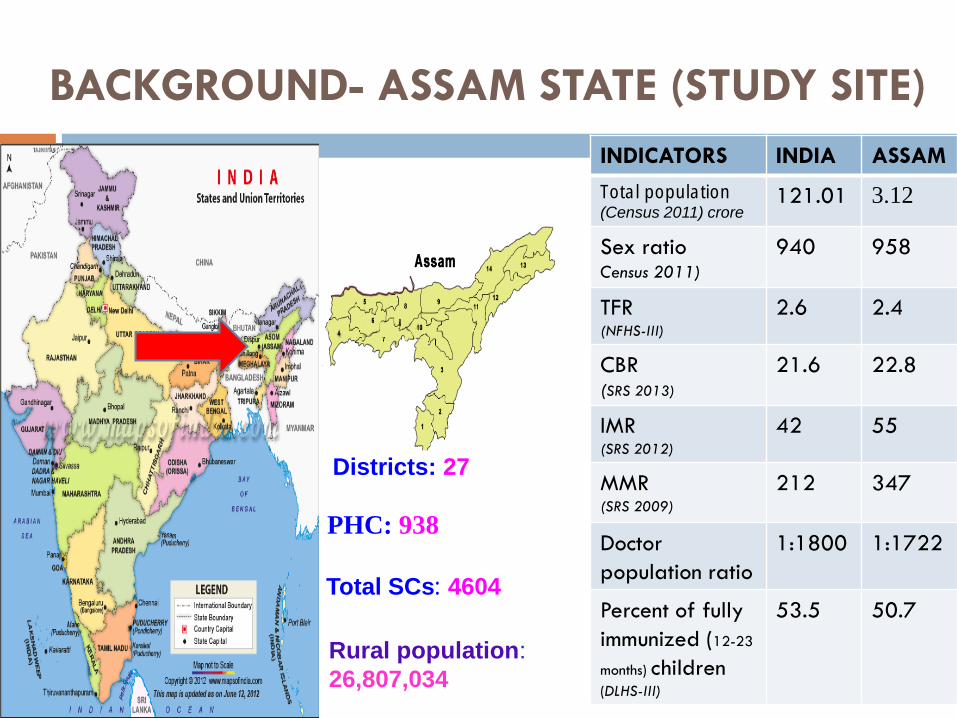
BACKGROUND- ASSAM STATE (STUDY SITE)
PHC: 938
Districts: 27
Total SCs: 4604
INDICATORS INDIA ASSAM
Total population(Census 2011) crore
121.01 3.12
Sex ratioCensus 2011)
940 958
TFR(NFHS-III)
2.6 2.4
CBR(SRS 2013)
21.6 22.8
IMR(SRS 2012)
42 55
MMR(SRS 2009)
212 347
Doctor
population ratio
1:1800 1:1722
Percent of fully
immunized (12-23
months) children (DLHS-III)
53.5 50.7
Rural population:
26,807,034
BACKGROUND
Assam passed the “Assam Rural Health Regulatory Act in
Sep’2004 for creation of mid-level health professionals to serve
the rural population
Vide the Act, Assam Rural Health Regulatory Authority was
formed to regulate and develop the 3 yrs curriculum of Diploma
in Medicine and Rural Health Care (DMRHC) course
Under the Act, Jorhat Rural Medical Institute was established
for starting the DMRHC course in Sep’2005
Act defined the diploma holders in DMRHC as “Rural Health
Practitioners” who are eligible to practice medicine /rural
health carein rural areas, perform notified procedures, treat
notified common ailments/ diseases, use common notified drugs
and are not permitted to use “Doctor” or “Dr” before and after
his name
STUDY OBJECTIVES
To examine the trend in ranges , types and uptake of health care
services before and after deployment of RHPs at SCs
To assess & compare performance of SCs with RHPs to those SCs
without RHPs in studied districts
To understand the perspectives of beneficiaries, community, officials
and ANMs about the ranges, types and quality of health care services
provided before and after deployment of RHPs
To understand the perspective of RHPs about DMRHC, their
role, work experiences, challenges faced etc
To provide suggestions for improvement of RHP model
STUDY DESIGN
Mixed Research method – primarily qualitative complemented by
quantitative technique
Triangulation method for consolidation/validation of data
obtained from varied sources-
o Review of secondary data on RCH indicators for SCs/districts;
o Review of government documents
o In-depth interviews /FGDs using semi-structured questionnaire
Purposive random sampling method used for selection of 8 high
focus districts (HFDs) out of 14 HFDs on the basis of criteria like:
o Average performing district (RCH indicators)
o Availability of RHPs in SCs in district in 1 year prior to study
o Feasibility to conduct field visits (study period: Apri-Sep’13)
CRITERIA FOR AVERAGE PERFORMING
DISTRICT
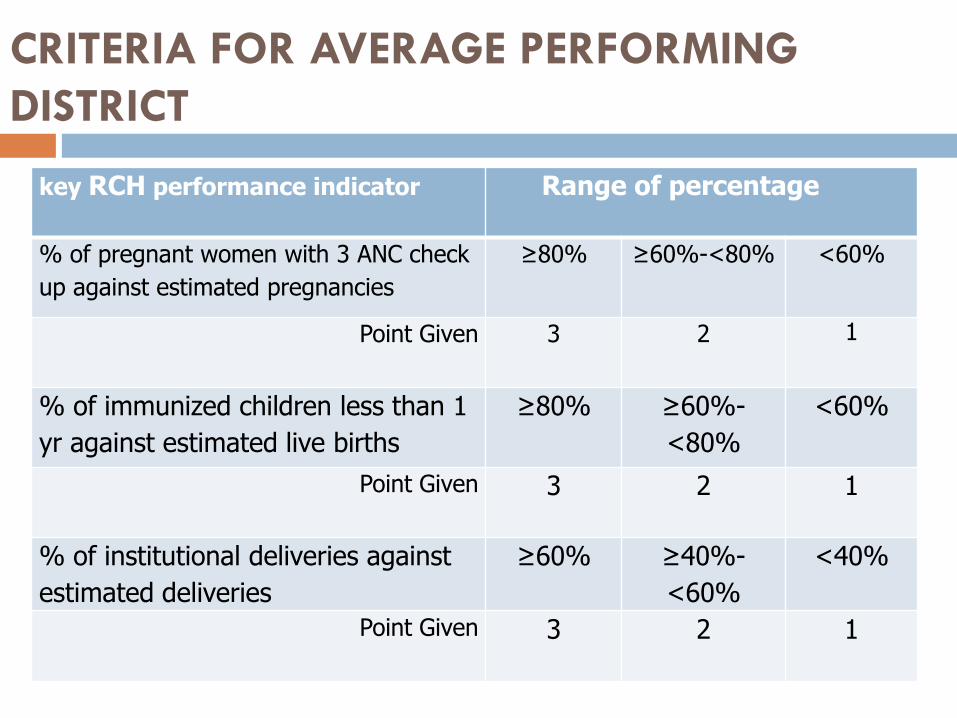
key RCH performance indicator Range of percentage
% of pregnant women with 3 ANC check
up against estimated pregnancies
≥80% ≥60%-<80% <60%
Point Given 3 2 1
% of immunized children less than 1
yr against estimated live births
≥80% ≥60%-
<80%
<60%
Point Given 3 2 1
% of institutional deliveries against
estimated deliveries
≥60% ≥40%-
<60%
<40%
Point Given 3 2 1
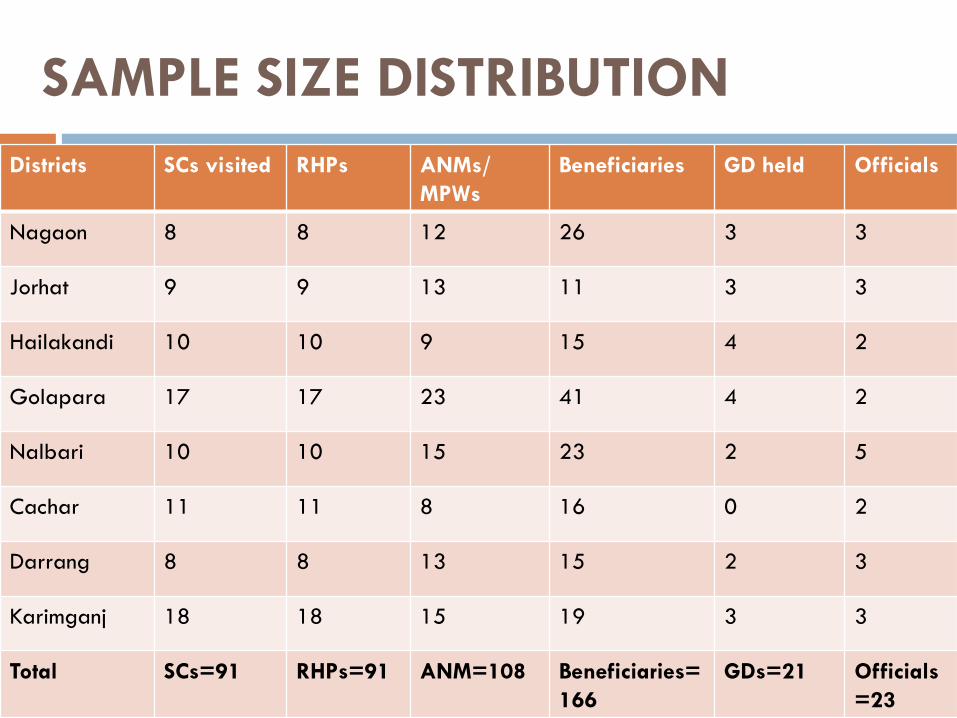
SAMPLE SIZE DISTRIBUTION
Districts SCs visited RHPs ANMs/
MPWs
Beneficiaries GD held Officials
Nagaon 8 8 12 26 3 3
Jorhat 9 9 13 11 3 3
Hailakandi 10 10 9 15 4 2
Golapara 17 17 23 41 4 2
Nalbari 10 10 15 23 2 5
Cachar 11 11 8 16 0 2
Darrang 8 8 13 15 2 3
Karimganj 18 18 15 19 3 3
Total SCs=91 RHPs=91 ANM=108 Beneficiaries=
166
GDs=21 Officials
=23
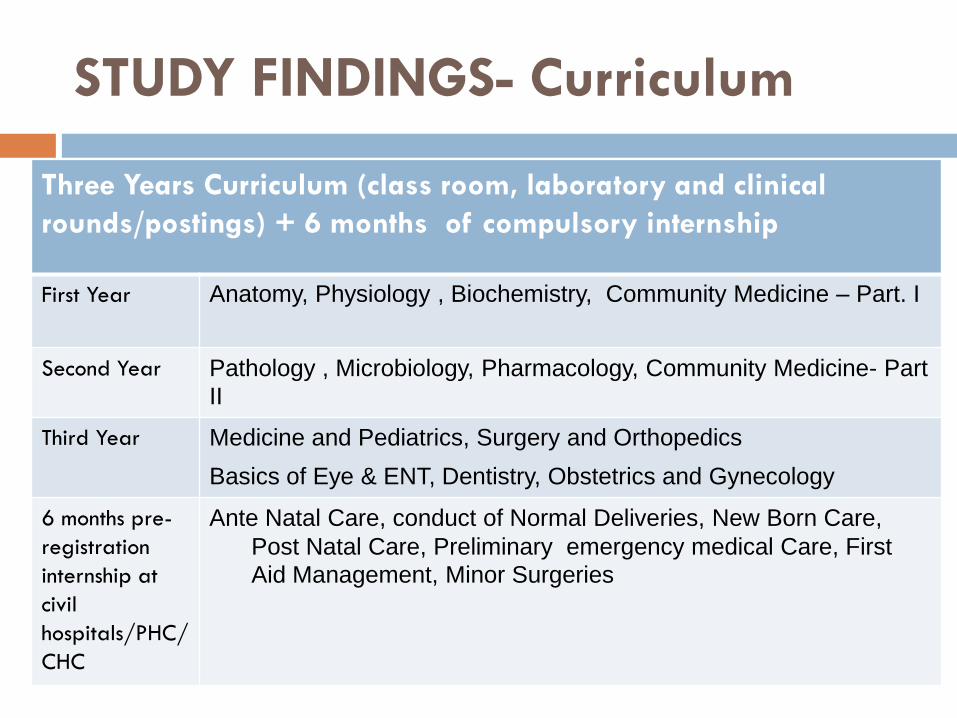
STUDY FINDINGS- Curriculum
Three Years Curriculum (class room, laboratory and clinical
rounds/postings) + 6 months of compulsory internship
First Year Anatomy, Physiology , Biochemistry, Community Medicine – Part. I
Second Year Pathology , Microbiology, Pharmacology, Community Medicine- Part
II
Third Year Medicine and Pediatrics, Surgery and Orthopedics
Basics of Eye & ENT, Dentistry, Obstetrics and Gynecology
6 months pre-
registration
internship at
civil
hospitals/PHC/
CHC
Ante Natal Care, conduct of Normal Deliveries, New Born Care,
Post Natal Care, Preliminary emergency medical Care, First
Aid Management, Minor Surgeries
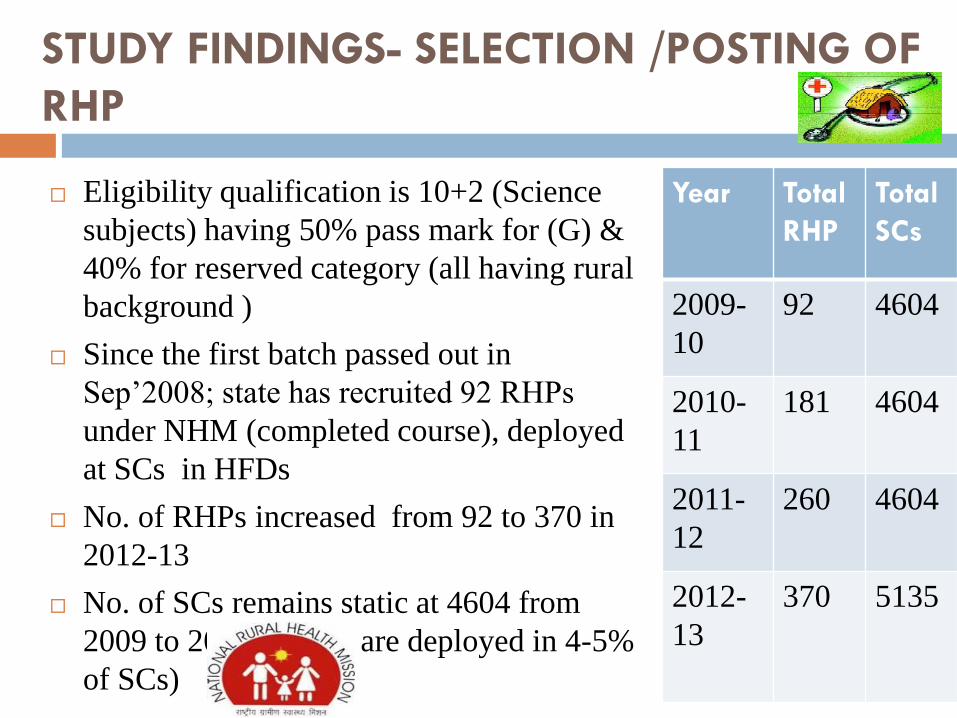
STUDY FINDINGS- SELECTION /POSTING OF
RHP
Eligibility qualification is 10+2 (Science
subjects) having 50% pass mark for (G) &
40% for reserved category (all having rural
background )
Since the first batch passed out in
Sep’2008; state has recruited 92 RHPs
under NHM (completed course), deployed
at SCs in HFDs
No. of RHPs increased from 92 to 370 in
2012-13
No. of SCs remains static at 4604 from
2009 to 2012 ( RHPs are deployed in 4-5%
of SCs)
Year Total
RHP
Total
SCs
2009-
10
92 4604
2010-
11
181 4604
2011-
12
260 4604
2012-
13
370 5135
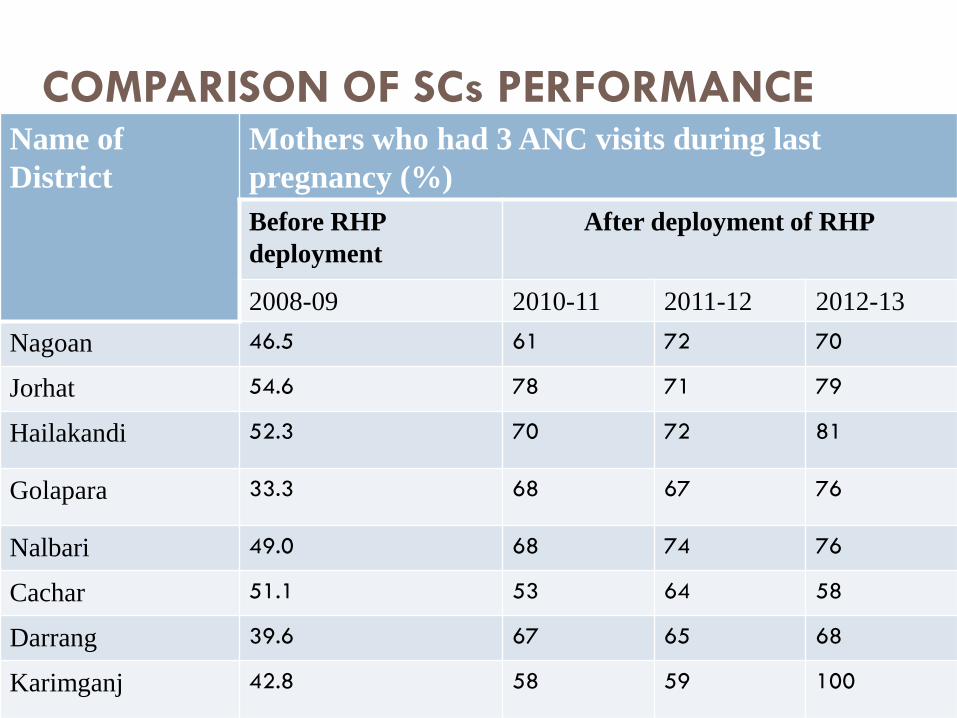
COMPARISON OF SCs PERFORMANCE Name of
District
Mothers who had 3 ANC visits during last
pregnancy (%)
Before RHP
deployment
After deployment of RHP
2008-09 2010-11 2011-12 2012-13
Nagoan 46.5 61 72 70
Jorhat 54.6 78 71 79
Hailakandi 52.3 70 72 81
Golapara 33.3 68 67 76
Nalbari 49.0 68 74 76
Cachar 51.1 53 64 58
Darrang 39.6 67 65 68
Karimganj 42.8 58 59 100
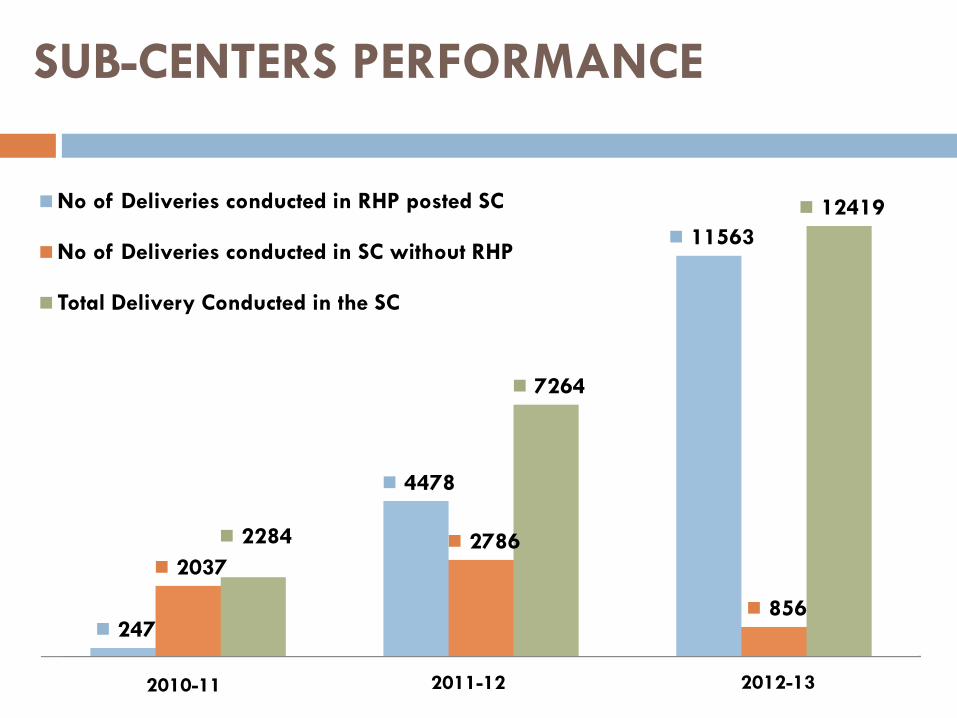
SUB-CENTERS PERFORMANCE
247
4478
11563
20372786
856
2284
7264
12419No of Deliveries conducted in RHP posted SC
No of Deliveries conducted in SC without RHP
Total Delivery Conducted in the SC
2010-11 2011-12 2012-13
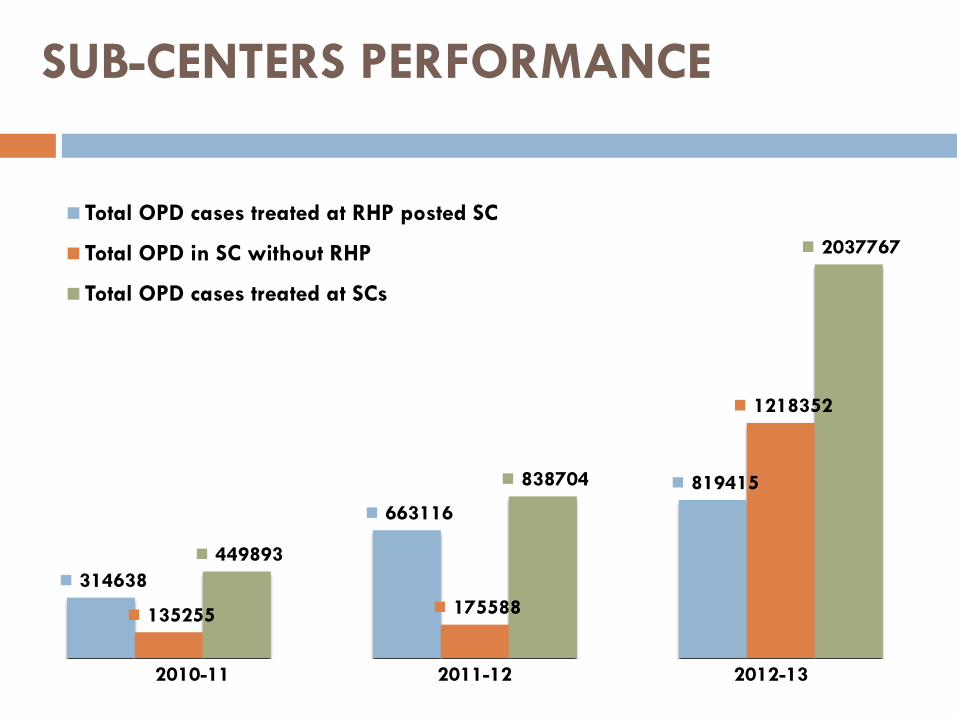
SUB-CENTERS PERFORMANCE
314638
663116
819415
135255 175588
1218352
449893
838704
2037767
Total OPD cases treated at RHP posted SC
Total OPD in SC without RHP
Total OPD cases treated at SCs
2010-11 2011-12 2012-13
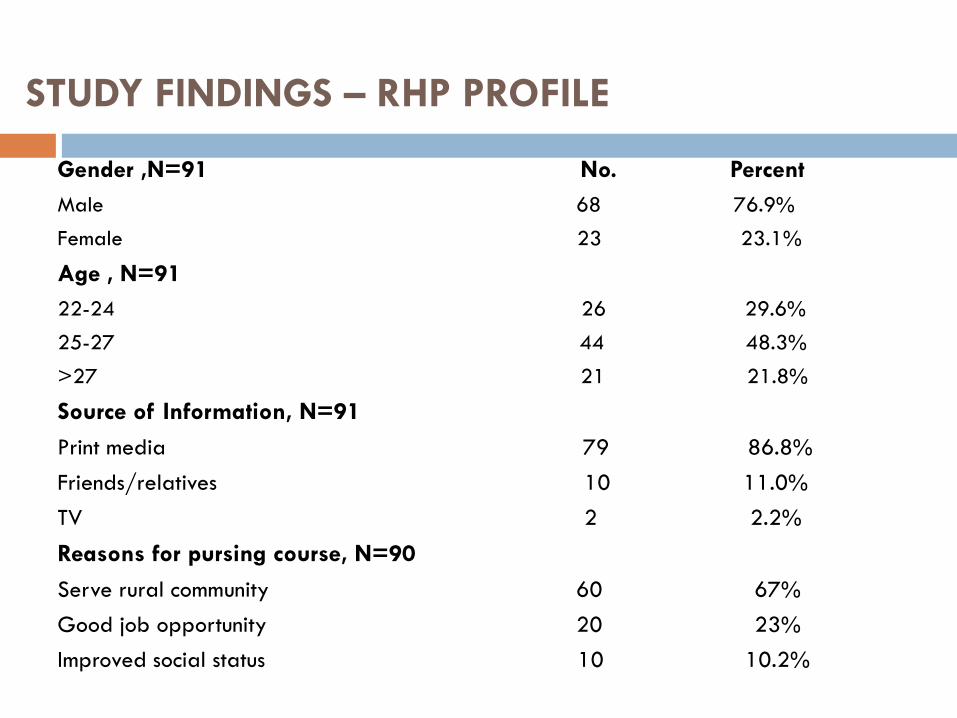
STUDY FINDINGS – RHP PROFILE
Gender ,N=91 No. Percent
Male 68 76.9%
Female 23 23.1%
Age , N=91
22-24 26 29.6%
25-27 44 48.3%
>27 21 21.8%
Source of Information, N=91
Print media 79 86.8%
Friends/relatives 10 11.0%
TV 2 2.2%
Reasons for pursing course, N=90
Serve rural community 60 67%
Good job opportunity 20 23%
Improved social status 10 10.2%
RHP’S PERSPECTIVE
Print media was the major source of information about the course.
Interest for serving community and good job perspectives remained the main reason for pursing the course among RHPs.
DMRHC was similar to MBBS course in terms of subjects and contents taught; notable differences was the lack of Forensic Medicine, Major Surgery, Dermatology & Psychiatry and relatively shorter duration of course. Few wanted extension of course duration and internship period.
Majority of respondents considered that course was suitable for serving in rural health settings and felt that internship program was very helpful in delivering their routine duties.
Current posting was located outside their home-district and State Government has not provided any residential facility/quarter.
Main treatment provided was symptomatic management of minor ailments (common cold, fever, diarrhea etc.), NCD (diabetes, hypertension etc.),communicable diseases, initiation of deliveries
Challenges faced by RHPs were location of SC, lack of accommodation and referral transport facilities
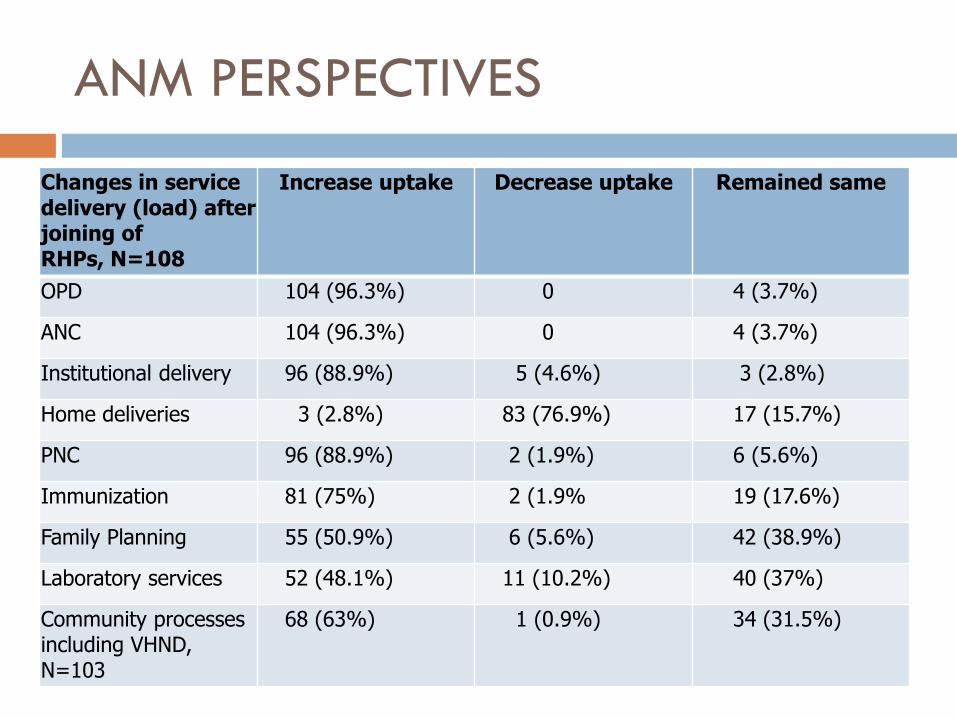
ANM PERSPECTIVES
Changes in service delivery (load) after joining of RHPs, N=108
Increase uptake Decrease uptake Remained same
OPD 104 (96.3%) 0 4 (3.7%)
ANC 104 (96.3%) 0 4 (3.7%)
Institutional delivery 96 (88.9%) 5 (4.6%) 3 (2.8%)
Home deliveries 3 (2.8%) 83 (76.9%) 17 (15.7%)
PNC 96 (88.9%) 2 (1.9%) 6 (5.6%)
Immunization 81 (75%) 2 (1.9% 19 (17.6%)
Family Planning 55 (50.9%) 6 (5.6%) 42 (38.9%)
Laboratory services 52 (48.1%) 11 (10.2%) 40 (37%)
Community processes including VHND, N=103
68 (63%) 1 (0.9%) 34 (31.5%)
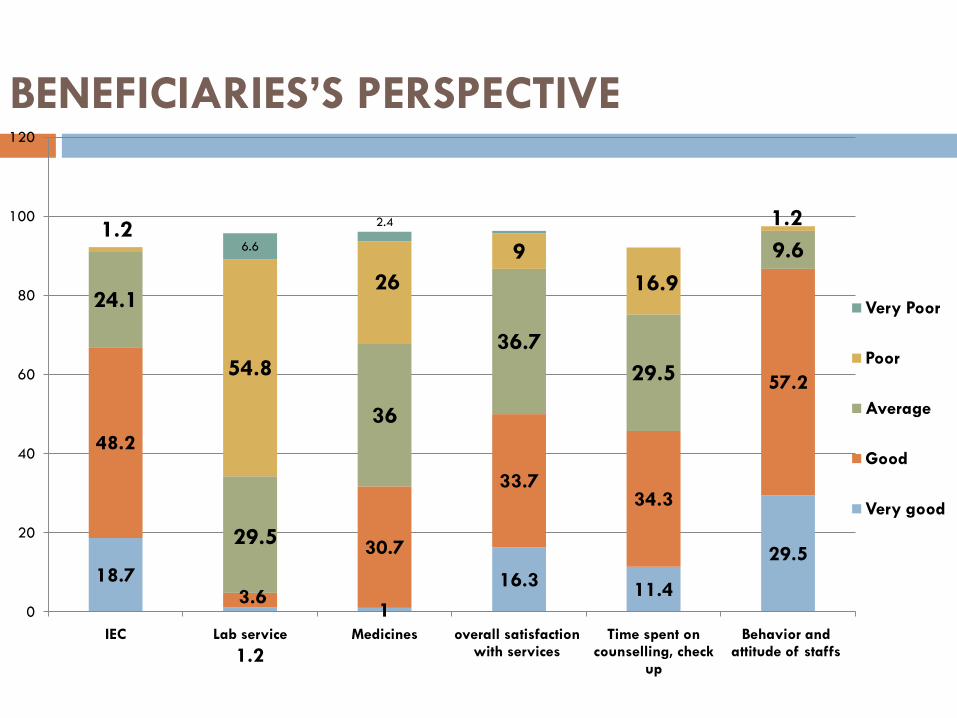
BENEFICIARIES’S PERSPECTIVE
18.7
1.2
1
16.311.4
29.5
48.2
3.6
30.7
33.734.3
57.2
24.1
29.5
36
36.7
29.5
9.61.2
54.8
26
9
16.9
1.26.6
2.4
0
20
40
60
80
100
120
IEC Lab service Medicines overall satisfaction with services
Time spent on counselling, check
up
Behavior and attitude of staffs
Very Poor
Poor
Average
Good
Very good
COMMUNITY’S PERSPECTIVE
Provision of ANC/PNC services have become more
systematic and available daily
SCs have started conducting institutional
deliveries, manage common ailments, manage accidental
& emergency cases like burns etc
Availability of medicines has improved
Decreased case of Infant and Maternal related illnesses
and deaths due to timely referral
People are increasingly availing Family Planning and
Immunization services.
Effective screening of patients before making referrals
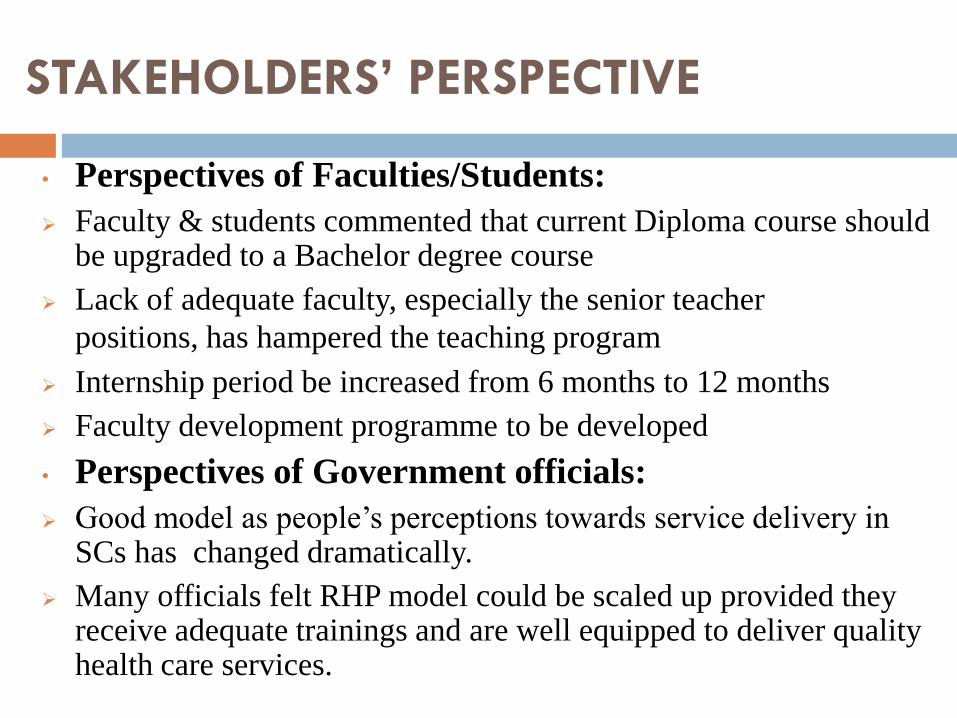
STAKEHOLDERS’ PERSPECTIVE
• Perspectives of Faculties/Students:
Faculty & students commented that current Diploma course should be upgraded to a Bachelor degree course
Lack of adequate faculty, especially the senior teacher
positions, has hampered the teaching program
Internship period be increased from 6 months to 12 months
Faculty development programme to be developed
• Perspectives of Government officials:
Good model as people’s perceptions towards service delivery in SCs has changed dramatically.
Many officials felt RHP model could be scaled up provided they receive adequate trainings and are well equipped to deliver quality health care services.
DISCUSSION
Deficiencies in DMRHC
Improve Access & service utilization
Infrastructure gaps/ other support system
Potential for scaling up of RHPs
Weak capacity building /support
system
CONCLUSIONS
Education
• Up-gradation of DMRHC to Bachelor course
• Review of internship period
• Preferential selection of candidates from minority/difficult areas
HR Managerial
• Revision of current Roles/Responsibilities of RHPs
• Creation of career pathways
Training & Supervision
• Development of Integrated Training program
• Establishment of a support supervisory system
Enabling work environment
Provision of residential quarter & rental arrangement
Regular supply of water & electricity , infrastructure up-gradation
The importance of recruiting and admitting future physicians who have grown up in rural and remote settings now seems clearly established... However... only a fraction of what could be done in this area is currently being done.
By Barer Stoddart, 1999




![SLFRS for SMEs - Kandy 09 05 2012 [Read-Only] - CA Sri Lanka · 2012-08-27 · • Sri Lanka: 50,000+ but only 311+ listed A Presentation to practitioners and prep arers of financial](https://img.pdfslide.us/doc/110x75/5f0bb8717e708231d431e2fd/slfrs-for-smes-kandy-09-05-2012-read-only-ca-sri-lanka-2012-08-27-a-sri.jpg)
























