Embed Size (px)
Citation preview

1
Optimizing Early Therapy:
Future Options and Considerations
Gavin Giovannoni
Bernd Kieseier

Disclosures
▪ Professor Giovannoni has provided consultation to
Bayer-Schering Healthcare, Biogen-Idec, Genzyme,
GlaxoSmithKline, Merck-Serono, Novartis, Protein
Discovery Laboratories, Teva-Aventis, UCB Pharma.
Ironwood, Eisai, Vertex, Roche, Synthon, Canbex. He
has received grant support from Bayer-Schering
Healthcare, Biogen-Idec, Merck-Serono, Merz, Novartis,
Teva-Aventis, GW Pharma
▪ Professor Kieseier has provided consultation to Bayer
Schering, Biogen Idec, Medac, Merck Serono, Novartis,
Sanofi-Aventis, Talecris, Teva. He has received grant
support from Bayer Schering, Biogen Idec, Biotest,
Merck Serono, Teva
2

C-1900
Phase 2
6-months MRI
257 patients
Phase 1 Healthy Volunteer Studies
• C-1903 Food Effect
• 109HV101 Cardiac QTc
• 109HV102 Absorption, Metabolism,
Excretion
• 109HV103 Drug-Drug Interaction
with Avonex
• 109HV104 Drug-Drug Interaction
with Glatiramer Acetate (GA)
• 109HV105 Relative Bioavailability
• 109HV106 PK, Safety, Tolerability
• 109HV107 PK Bioequivalence
• 109HV321 Tolerability study
Study 303 (109MS303)
Dose-blind, open-label
extension study
1738 patients
Study 201 (109MS201)
Phase 2 IFN/GA
6-months add-on
Safety/MRI
108 patients Completed Studies
Ongoing Studies
Study 301 (109MS301)
Phase 3, 2-year
monotherapy
1237 patients
109MS101
Phase 1
PK
48 patients
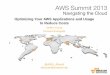
By the filing date, 2560 MS patients had received dimethyl fumarate;
approximately 3600 person-years of exposure
• 109HV108 PK in Asia Pacific
MS Clinical Development Plan
Study 302 (109MS302)
Phase 3, 2-year monotherapy
GA comparator group
1430 patients
3 PK=pharmacokinetics; MRI=magnetic resonance imaging; IFN=interferon.

CHMP Opinion: Dimethyl Fumarate
Category Opinion
Indication Treatment of adult patients with relapsing remitting multiple sclerosis
Active
substance
Dimethyl fumarate, a nervous system drug (N07XX09), that primarily
acts by triggering the activation of the nuclear factor (erythroid-derived
2)-like 2 (Nrf2) transcriptional pathway.
Benefits Ability to reduce the number of relapses in patients with relapsing-
remitting multiple sclerosis
Most common
side effects
Flushing and gastrointestinal events (eg, diarrhea, nausea, and
abdominal pain)
4
Detailed recommendations for the use of this product will be described in the summary of product characteristics (SmPC), which will be
published in the European public assessment report (EPAR) and made available in all official European Union (EU) languages after the
marketing authorization has been granted by the European Commission (EC).
CHMP=Committee on Human Medicinal Products.
▪ A pharmacovigilance plan will be implemented
▪ Treatment should be initiated under the supervision of a physician experienced in the
treatment of the disease

Dimethyl Fumarate: Research into Mechanism of
Action Concurrent with Clinical Development
5
Inflammation,
tissue damage
Nrf2
Cell tissue and
cytoprotection
Protective
response against
neurotoxic insult
Dimethyl Fumarate
Anti-inflammatory
response
Scannevin RH et al. J Pharmacol Exp Ther. 2012;341:274-284; Kappos L et al. Lancet. 2008;372:1463−1472;
Gold R et al. N Engl J Med. 2012;367:1098−1107; Fox RJ et al. N Engl J Med 2012;367:1087−1097.
Transcriptional profiling suggests
dimethyl fumarate activates the
Nrf2 Oxidative Stress Response
Pathway
WT Nrf2 Knockout0
200
400
600
800
7
Gen
es In
du
ced
by D
MF
4 h
r T
reatm
en
t (p
< 1
0-5
)
Confirmation in Nrf2 Knockout Mice

C-1900
Phase 2
6-months MRI
257 patients
Phase 1 Healthy Volunteer Studies
• C-1903 Food Effect
• 109HV101 Cardiac QTc
• 109HV102 Absorption, Metabolism,
Excretion
• 109HV103 Drug-Drug Interaction
with Avonex
• 109HV104 Drug-Drug Interaction
with Glatiramer Acetate (GA)
• 109HV105 Relative Bioavailability
• 109HV106 PK, Safety, Tolerability
• 109HV107 PK Bioequivalence
• 109HV321 Tolerability study
Study 303 (109MS303)
Dose-blind, open-label
extension study
1738 patients
Study 201 (109MS201)
Phase 2 IFN/GA
6-months add-on
Safety/MRI
108 patients Completed Studies
Ongoing Studies
Study 301 (109MS301)
Phase 3, 2-year
monotherapy
1237 patients
109MS101
Phase 1
PK
48 patients
By the filing date, 2560 MS patients had received dimethyl fumarate;
approximately 3600 person-years of exposure
• 109HV108 PK in Asia Pacific
MS Clinical Development Plan
Study 302 (109MS302)
Phase 3, 2-year monotherapy
GA comparator group
1430 patients
6 PK=pharmacokinetics; MRI=magnetic resonance imaging; IFN=interferon.

*Any patient with significant protocol-defined disability progression may switch to open-label MS treatment at any time; CONFIRM: any patient with 2
INEC-confirmed relapses at any time may switch to open-label MS treatment after 48 weeks on study; †double-blind only for dimethyl fumarate and
placebo; rater-blinded for all arms; INEC fully blinded to all arms.
DEFINE=Determination of the Efficacy and Safety of Oral Fumarate in Relapsing-Remitting MS; CONFIRM=Comparator and an Oral Fumarate in
Relapsing-Remitting MS; PO=by mouth; TID=3 times daily; BID=twice daily; GA=glatiramer acetate; SC=subcutaneous; INEC=independent neurology
evaluation committee.
Gold R et al. N Engl J Med. 2012;367:1098-1107; Fox R et al. N Engl J Med. 2012;367:1087-1197.
*Any patient with significant protocol-defined disability progression may switch to open-label MS treatment at any time; DEFINE: any patient with 1 INEC-
confirmed relapse on or after week 24 may switch to open-label MS treatment after 48 weeks on study; †double-blind only for dimethyl fumarate and
placebo; rater-blinded for all arms; INEC fully blinded to all arms.
Dimethyl Fumarate Phase 3 Study Schematic:
DEFINE and CONFIRM
7
Screening
240 mg PO BID (480 mg/day)
240 mg PO TID (720 mg/day)
Optional open-label MS treatment*
Placebo Randomization
1:1:1
Year 1 Year 2
GA SC (20 mg/day)
Multicenter, double-blind, dose-comparison study
(N=1237; MRI N=540)
Multicenter, double-blind, reference comparator,
dose-comparison study (N=1430; MRI N=681)†
Randomization
1:1:1:1

0.40
0.220.20
0.29
0
0.1
0.2
0.3
0.4
0.5
0.6
Placebo
(n=363)
240 mg BID
(n=359)
240 mg TID
(n=345)
GA
(n=350)
0.36
0.170.19
0
0.1
0.2
0.3
0.4
0.5
0.6
Placebo(n=408)
240 mg BID(n=410)
240 mg TID(n=416)
44%
reduction
vs placebo
P<0.001
51%
reduction
vs placebo
P<0.001
*Annualized relapse rate calculated with negative binomial regression, with prespecified adjustment for baseline EDSS score (≤2.0 vs >2.0),
baseline age (<40 vs ≥40 years), region, and number of relapses in the 1 year prior to study entry; data after switch to alternative MS therapy
were excluded; Gold R et al. N Engl J Med. 2012;367:1098-1107; Fox R et al. N Engl J Med. 2012;367:1087-1197.
29%
reduction
vs placebo
P<0.05
Annualized Relapse Rate at 2 Years
8
53%
reduction
vs placebo
P<0.001
48%
reduction
vs placebo
P<0.001
An
nu
ali
ze
d R
ela
ps
e R
ate
* (9
5%
CI)
An
nu
ali
ze
d R
ela
pse
Rate
* (9
5%
CI)
CONFIRM DEFINE

New or Newly Enlarging
T2-Hyperintense Lesions at 2 Years*
9
*Negative binomial regression analysis, adjusted for region and baseline T2 lesion volume.
Gold R et al. N Engl J Med. 2012;367:1098-1107; Fox R et al. N Engl J Med. 2012;367:1087-1197.
Ne
w o
r N
ew
ly E
nla
rgin
g T
2 L
es
ion
s*
(me
an
)
17.0
2.6
4.4
0
5
10
15
20
25
Placebo(n=165)
240 mg BID (n=152)
240 mg TID(n=152)
Ne
w o
r N
ew
ly E
nla
rgin
g T
2 L
es
ion
s*
(me
an
)
74%
reduction
vs placebo
P<0.001
85%
reduction
vs placebo
P<0.001
17.4
5.1 4.7
8.0
0
5
10
15
20
25
Placebo(n=139)
240 mg BID(n=140)
240 mg TID(n=140)
GA(n=153)
71%
reduction
vs placebo
P<0.001
73%
reduction
vs placebo
P<0.001
54%
reduction
vs placebo
P<0.001
CONFIRM DEFINE

Gd+ Lesions at 2 Years*
10
*Ordinal logistic regression analysis, adjusted for region and baseline number of Gd+ lesions.
Gd+=gadolinium-enhancing.
Gold R et al. N Engl J Med. 2012;367:1098-1107; Fox R et al. N Engl J Med. 2012;367:1087-1197.
Gd
+ L
es
ion
s (
me
an
)
1.8
0.1
0.5
0.0
0.5
1.0
1.5
2.0
2.5
Placebo (n=165) 240 mg BID (n=152)
240 mg TID(n=152)
Gd
+ L
es
ion
s (
me
an
)
2.0
0.5 0.4
0.7
0.0
0.5
1.0
1.5
2.0
2.5
Placebo(n=144)
240 mg BID(n=147)
240 mg TID(n=144)
GA(n=161)
73%
reduction
vs placebo
P=0.001
90%
reduction
vs placebo
P<0.001
74%
reduction
vs placebo
P<0.001
65%
reduction
vs placebo
P=0.001
61%
reduction
vs placebo
P=0.001
CONFIRM DEFINE

New T1-Hypointense Lesions at 2 Years*
11
Ne
w T
1-H
yp
oin
ten
se
Le
sio
ns
* (m
ea
n)
5.6
1.5
2.1
0
5
10
Placebo (n=165) 240 mg BID(n=152)
240 mg TID(n=152)
New
T1-H
yp
oin
ten
se L
esio
ns*
(mean
)
7.0
3.0
2.4
4.1
0
5
10
Placebo(n=139)
240 mg BID(n=140)
240 mg TID(n=140)
GA(n=154)
*Negative binomial regression analysis, adjusted for region and baseline T1 lesion volume.
Arnold DL et al. Presented at ECTRIMS, October 19–22, 2011. Amsterdam, The Netherlands. P831; Fox R et al.
N Engl J Med. 2012;367:1087-1197.
63%
reduction
vs placebo
P<0.001
72%
reduction
vs placebo
P<0.001
57%
reduction
vs placebo
P<0.001
65%
reduction
vs placebo
P<0.001
41%
reduction
vs placebo
P<0.001
CONFIRM DEFINE

12-Week Confirmed Disability Progression
12
*Estimated proportion of patients with progression and time to progression up to 96 weeks based on the Kaplan-Meier product limit method; †based on Cox proportion hazards model, adjusted for baseline EDSS score (≤2.0 vs >2.0), region, and baseline age (<40 vs ≥40 years).
Gold R et al. N Engl J Med. 2012;367:1098-1107; Fox R et al. N Engl J Med. 2012;367:1087-1197.
Pa
tie
nts
wit
h D
isa
bil
ity P
rog
res
sio
n*
(%)
12 24 36 48 60 72 84 96
Time on Study (weeks)
0
10
20
30 240 mg BID=38% risk reduction, P=0.005†
240 mg TID=34% risk reduction, P=0.013†
18
16
27
BL
Placebo
240 mg BID
240 mg TID
12 24 36 48 60 72 84 96
Time on Study (weeks)
0
240 mg BID=21% risk reduction, P=0.25†
240 mg TID=24% risk reduction, P=0.20†
GA=7% risk reduction, P=0.70†
16
17
BL
Placebo
240 mg BID
240 mg TID
13
GA
10
20
30
Pati
en
ts w
ith
Dis
ab
ilit
y P
rog
ressio
n*
(%)
13
CONFIRM DEFINE

Dimethyl Fumarate Activation of the Nrf2
Pathway in MS Patients
13
Changes of Blood NQO1 Over Time
in DEFINE Phase 3 Trial
0 10 20 30 40 50-5%
0%
5%
10%
15%
20%
25%
30%
35%Placebo
BID
TID
Week
No
rmalized
%C
han
ge N
QO
1
*
*
* *
*P<0.05 compared with placebo.
NQO1=NADPH (nicotinamide adenine dinucleotide phosphate) quinone oxidoreductase; BID=twice daily; TID=3 times daily.
Biogen Idec, data on file.

Integrated Analysis: Overview of Safety*
14
Event, % Patients
Placebo
(n=836)
240 mg BID
(n=769)
240 mg TID
(n=823)
Any adverse event 92 95 93
Serious adverse event† 21 18 15
Discontinuation due to adverse event 11 14 14
Study withdrawal due to adverse event 4 8 8
Infection 56 60 60
Serious infection 1.4 2.2 1.8
Malignancy <1 <1 <1
Death <1‡ <1§ <1¶
*The safety population for the integrated analysis includes patients treated with placebo or dimethyl fumarate 240 mg TID from the phase 2 dose-
ranging study, as well as all patients from the phase 3 studies, DEFINE and CONFIRM; †includes MS relapses fitting the classification of a serious
adverse event; ‡due to ischemic stroke after switch to alternative MS medication; §due to road traffic accident/traumatic brain injury after study
withdrawal; ¶due to road traffic accident and MS relapse complicated by intraventricular hemorrhage after last dose (within 30 days of study
withdrawal).
Selmaj K et al. Presented at ECTRIMS; October 10–13, 2012; Lyon, France. P484.

Integrated Analysis: Common Adverse Events
(≥10% in Any Group)
15
Event, % Patients
Placebo
(n=836)
240 mg BID
(n=769)
240 mg TID
(n=823)
Flushing 5 34 29
MS relapse 43 29 26
Nasopharyngitis 20 22 22
Headache 16 17 17
Diarrhea 10 14 17
Urinary tract infection 11 14 12
Upper respiratory tract infection 11 13 12
Nausea 9 12 14
Fatigue 11 12 13
Back pain 11 12 10
Abdominal pain upper 6 10 11
Proteinuria* 7 9 10
The overall incidence of any GI event was 31%, 40%, and 43% in the placebo, 240 mg BID, and 240 mg TID groups, respectively; *no notable differences
in levels of BUN and creatinine, urine β2-microglobulin, and urine microalbumin were observed across treatment groups with monitoring every 4 weeks.
GI=gastrointestinal; BUN=blood urea nitrogen.
Selmaj K et al. Presented at ECTRIMS; October 10–13, 2012; Lyon, France. P484.
Indicates ≥3% higher incidence in either dimethyl fumarate group vs placebo.

Integrated Analysis: Events Leading to Study
Drug Discontinuation (≥1% in Any Group)
16
Event, % Patients
Placebo
(n=836)
BG-12
240 mg BID
(n=769)
BG-12
240 mg TID
(n=823)
Discontinued study drug 11 14 14
MS relapse 6 1 2
Flushing <1 3 2
GI event
Diarrhea
Nausea
Vomiting
Abdominal pain, upper
Abdominal pain
<1
<1
0
0
<1
0
4
<1
<1
1
<1
<1
6
2
2
1
1
1
Selmaj K et al. Presented at ECTRIMS; October 10–13, 2012; Lyon, France. P484.

Integrated Analysis: Incidence of Flushing Events*
and Gastrointestinal Events† by Study Month
17
*Flushing events included the preferred terms “flushing,” “hot flush,” “erythema,” “generalized erythema,” “burning sensation,” “skin burning
sensation,” “feeling hot,” and “hyperemia”; †gastrointestinal events included the preferred terms in the level 2 subordinate standardized
MedDRA queries “gastrointestinal nonspecific inflammations” or “gastrointestinal nonspecific symptoms and therapeutic procedures.”
Selmaj K et al. Presented at ECTRIMS; October 10–13, 2012; Lyon, France. P484.
Placebo (n=408)
240 mg BID (n=410)
240 mg TID (n=416)
10
5
25
30
35
20
15
0 1 2 3 4 5 6 7 8 9 10 11 12 24
Month
Pa
tie
nts
(%
)
30
25
20
15
10
5
0 1 2 3 4 5 6 7 8 9 10 11 12 24
Month
Pa
tie
nts
(%
)
35
Flushing Events
Gastrointestinal Events

GI Events in First 3 Months of Treatment
for BID Dose (n=769)
Events, n (%)
Abdominal Pain
Adverse Events
Nausea/
Vomiting
Adverse Events
Diarrhea
Adverse Events
Any type of this event 121a 120a 78a
Severity
Mild
Moderate
Severe
68 (56)
42 (35)
11 (9)
65 (54)
49 (41)
6 (5)
49 (63)
26 (33)
3 (4)
Symptomatic Therapy 46 (38) 39 (33) 20 (26)
Resolvedb 113 (93) 114 (95) 75 (96)
18
aUsed as the denominator for percentages.; patients may have experienced more than one event. bEvents may have resolved at any time during the
study. GI events=preferred terms in the level 2 subordinate standardized MedDRA queries: “Gastrointestinal nonspecific inflammations” or
“gastrointestinal nonspecific symptoms and therapeutic procedures.”
Bar-Or A et al. Presented at LACTRIMS. November 28-30, 2012; Rio de Janeiro, Brazil.

Dimethyl Fumarate Efficacy and Safety:
Conclusions
▪ Compared with placebo, dimethyl fumarate significantly reduced
- Annualized relapse rate and MRI activity
- 12-week confirmed disability progression (DEFINE only)
- No serious safety signals in ~3600 patient-years exposure
▪ Most common adverse events were flushing and GI events
- Majority were mild to moderate
- Few discontinued treatment (3% due to flushing and 4% due to
GI intolerability)
- Strategies for management are under further investigation (aspirin,
administration with food, dose reduction, symptomatic treatment)
19

CHMP Opinion: Teriflunomide
Category Opinion
Indication Treatment of adult patients with relapsing-remitting multiple sclerosis
Active
substance
Teriflunomide, a selective immunosuppressant (L04AA31) with anti-
inflammatory properties. The exact mechanism by which teriflunomide
exerts its therapeutic effect in MS is not fully understood, but it is
known to reduce the proliferation of lymphocytes by blocking the
mitochondrial enzyme dihydroorotate dehydrogenase (DHO-DH).
Benefits Ability to reduce the relapse rate in patients with relapsing-remitting
multiple sclerosis
Most common
side effects
Upper respiratory tract infections, urinary tract infections, diarrhea,
nausea, paraesthesia (pins and needles), alopecia (loss of hair) and
increase in the liver enzyme alanine aminotransferase
20
Detailed recommendations for the use of this product will be described in the summary of product characteristics (SmPC),
which will be published in the European public assessment report (EPAR) and made available in all official European Union
(EU) languages after the marketing authorization has been granted by the European Commission (EC).
▪ A pharmacovigilance plan will be implemented
▪ Treatment should be initiated under the supervision of a physician experienced in the
treatment of the disease

Extension
Extension
Extension
Extension
Teriflunomide Clinical Development Program
Monotherapy
21
Extension
TERACLES: Phase
3 adjunctive therapy
program
TEMSO RMS/placebo
TOWER: RMS/placebo
TENERE: RMS/IFNβ
TOPIC: CIS/placebo
Phase 2 IFN*
Phase 2 GA
Extension
June 2012
TERIKIDS:
pediatric study
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Adjunctive therapy
*Phase 2 study with IFN add-on included any currently available IFNs.
Accelerated elimination of teriflunomide by cholestyramine was utilized in all studies, as required.
RMS=relapsing multiple sclerosis; IFNβ=interferon beta; CIS=clinically isolated syndrome; GA=glatiramer
acetate. Data available at http://clinicaltrials.gov. Accessed June 15, 2012.
Phase 2 RMS/placebo

TEMSO and TOWER Study Design
22
Randomization
N=1088
Reallocation of
placebo group
O’Connor PW et al. N Engl J Med. 2011;365:1293-1303; O’Connor PW et al. Presented at: ECTRIMS; October 19–22, 2011; Amsterdam, The Netherlands. P924;
Kappos L et al. MS Presented at ECTRIMS. October 10-13, 2012; Lyon, France. P153.
14 mg/day
14 mg/day
Placebo (n=363) 7 mg/day
Teriflunomide 7 mg/day (n=365)
Teriflunomide 14 mg/day (n=358)
Screening
Week –4 0 12 24 36 48 60 72 84 96 108
7 mg/day
RMS patients
screened
N=1388
Entry into extension* or
post-study washout
Randomization
N=1169 Placebo (n=388)
Teriflunomide
Teriflunomide
Screening
Week –4 0 12 24 36 48 60 72 84 96 108 120 132 144 152
14 mg/day
14 mg/day
Extension
Study ended when last patient randomized completed 48 weeks of treatment
Variable study treatment duration of 48–152 weeks
Minimum treatment time
TEMSO
TOWER
7 mg/day (n=407)
14 mg/day (n=370)

0.54
0.37 0.37
0
0.1
0.2
0.3
0.4
0.5
0.6
Teriflunomide: Annualized Relapse Rate
23
Placebo Teriflunomide
7 mg
Teriflunomide
14 mg
Ad
juste
d*
An
nu
ali
ze
d R
ela
pse
Rate
n=363 n=365 n=358
31.2% P<0.001
31.5% P<0.001
0.50
0.39
0.33
0
0.1
0.2
0.3
0.4
0.5
0.6
Placebo Teriflunomide
7 mg
Teriflunomide
14 mg
Ad
juste
d*
An
nu
ali
ze
d R
ela
pse
Rate
n=388 n=407 n=370
22.3% P<0.02
36.3% P<0.001
*Adjusted for EDSS score strata at baseline and takes into account duration of treatment. 1O’Connor PW et al. N Engl J Med. 2011;365:1293-1303; 2Kappos L et al. Presented at ECTRIMS; October 10–13, 2012; Lyon, France. P153.
TOWER2 TEMSO1

Teriflunomide: 12-week Sustained
Disability Progression
24
HRR=hazard ratio reduction 1O’Connor PW et al. N Engl J Med. 2011;365:1293-1303; 2Kappos L et al. MS Presented at ECTRIMS; October 10–13, 2012; Lyon, France. P153.
0
10
20
30
40
12
-week S
usta
ine
d D
isa
bilit
y P
rog
res
sio
n (
%)
0 12 24 36 48 60 72 84 96 108
Weeks
27.3
21.7 20.2
Placebo
Teriflunomide 7 mg
Teriflunomide 14 mg
Placebo
Teri 7 mg
Terif14 mg
363
365
358
336
343
329
306
309
302
279
290
285
258
266
262
242
252
251
224
238
234
211
234
227
200
224
217
160
178
175
Number of Patients at Risk
HRR=23.7%; P=0.08
HRR=29.8%; P=0.03
TOWER2 TEMSO1
12-W
ee
k C
on
firm
ed
Dis
ab
ilit
y P
rog
ress
ion
(%
)
0 12 24 36 48 60 72 84 96 108 120 132
0
10
20
30
40
Weeks
21.0 22.2
15.8
HRR=4.5%; P=0.76
HRR=31.5%; P=0.04
Placebo
Teriflunomide 7 mg
Teriflunomide 14 mg
Placebo
Teri 7 mg
Terif14 mg
388
406
370
354
375
340
325
337
310
295
314
286
271
286
267
241
248
245
195
202
211
156
163
162
128
114
124
83
77
87
Number of Patients at Risk 57
61
63
33
38
40

42.3
48.6
37.8
0
10
20
30
40
50
60
TENERE Outcomes
25
Annualized Relapse Rate Treatment Failure
SC IFNβ-1a Teriflunomide
7 mg
Teriflunomide
14 mg
Pa
tie
nts
(%
)
n=104 n=109 n=111
0.22
0.41
0.26
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0.45
SC IFNβ-1a Teriflunomide
7 mg
Teriflunomide
14 mg
Ad
juste
d*
An
nu
ali
ze
d R
ela
pse
Rate
n=104 n=109 n=111
*Adjusted annualized relapse rate, confirmed relapse.
TENERE=Teriflunomide and Rebif® in Patients with RMS; SC=subcutaneous; IFNβ=interferon beta.
Vermersch P et al. Presented at ENS; June 9–12, 2012; Prague, Czech Republic.
P=0.03

1.67
0.81
0.39
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
Placebo(n=363)
Teriflunomide7 mg (n=365)
Teriflunomide14 mg (n=358)
TEMSO: MRI Outcomes
TEMSO=Teriflunomide Multiple Sclerosis Oral trial.
O’Connor PW et al. N Engl J Med. 2011;365:1293-1303.
1.33
0.57
0.26
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
Placebo(n=363)
Teriflunomide7 mg (n=365)
Teriflunomide14 mg (n=358)
Gd
+ L
esio
ns p
er
T1
-Weig
hte
d S
can
57%
reduction
P<0.001 80%
reduction
P<0.001
Gd+ Lesions
T1-Hypointense
Lesions T2 Lesions
Vo
lum
e C
han
ge (
mL
)
44.0%
reduction
P=0.04 76.7%
reduction
P<0.001
Vo
lum
e C
han
ge (
mL
)
16.7%
reduction
P=0.19 31.3%
reduction
P=0.02
0.53 0.5
0.33
0
0.1
0.2
0.3
0.4
0.5
0.6
Placebo(n=363)
Teriflunomide7 mg (n=365)
Teriflunomide14 mg (n=358)
26

Teriflunomide: Overview of Adverse Events and
Serious Adverse Events
27
Proportion
of Patients (%)
TEMSO TOWER
Placebo
(n=363)
Teri
7 mg
(n=368)
Teri
14 mg
(n=358)
Placebo
(n=385)
Teri
7 mg
(n=409)
Teri
14 mg
(n=371)
Any adverse event 87.5 89.1 90.8 83.1 84.1 86.3
Serious adverse events 12.8 14.1 15.9 12.2 12.7 11.9
Deaths 0 0 0 0.3 0.2 0.5
Adverse events leading to
treatment discontinuation 8.1 9.8 10.9 6.2 13.0 15.6
O’Connor PW et al. N Engl J Med. 2011;365:1293-1303;
Kappos L et al. MS Presented at ECTRIMS; October 10−13, 2012; Lyon, France. P153.

TEMSO: Safety and Tolerability*
(Adverse Events with Incidence ≥10% in Any Group)
Adverse Events, %
Placebo
(n=360)
Teriflunomide 7 mg
(n=368)
Teriflunomide 14 mg
(n=358)
Any class 87.5 89.1 90.8
Nasopharyngitis 27.2 25.5 26.0
Headache† 17.8 22.0 18.7
Diarrhea† 8.9 14.7 17.9
Fatigue 14.2 12.8 14.5
Elevated ALT† 6.7 12.0 14.2
Nausea† 7.2 9.0 13.7
Hair thinning, decreased
hair density†
3.3 10.3 13.1
Influenza 10.0 9.2 12.0
Back pain 13.1 10.6 11.5
Urinary tract infection 9.7 7.3 10.3
Pain in arms or legs‡ 13.1 7.1 9.2
28
*Events are displayed in order of decreasing incidence in the teriflunomide 14 mg group; †adverse events occurring at a higher rate in the
teriflunomide group; ‡adverse events occurring at a higher rate in the placebo group.
ALT=alanine aminotransferase.
O’Connor PW et al. N Engl J Med. 2011;365:1293-1303.
Difference in incidence of ≥3% between teriflunomide and placebo.

Teriflunomide: Common Adverse Events
29
Adverse Event, %
TEMSO TOWER
Placebo
(n=360)
Teri
7 mg
(n=368)
Teri
14 mg
(n=358)
Placebo
(n=385)
Teri
7 mg
(n=409)
Teri
14 mg
(n=371)
Diarrhea 8.9 14.7 17.9 7.3 12.0 11.1
Nausea 7.2 9.0 13.7 8.8 8.3 10.2
Elevated ALT 6.7 12.0 14.2 8.3 11.2 14.0
Hair thinning/
decreased hair density 3.3 10.3 13.1 4.4 10.3 13.5
Hypersensitivity or skin
disorders 7.2 10.3 11.2 Not Reported
O’Connor PW et al. N Engl J Med. 2011;365:1293-1303;
Kappos L et al. MS Presented at ECTRIMS; October 10−13, 2012; Lyon, France. P153.

TEMSO: Pregnancy Concerns
▪ Pregnancy was reported as an adverse event, and 11 pregnancies occurred
during the study1
- 4 spontaneous abortions (1 in placebo and 3 in teriflunomide 14 mg group)
- 6 induced abortions (5 in teriflunomide 7 mg and 1 in teriflunomide 14 mg)
- 1 patient in the teriflunomide 14 mg group delivered a healthy baby1
▪ Patients who withdrew from the study for any reason or who did not
participate in the extension study underwent an 11-day elimination period,
during which they received cholestyramine or activated charcoal1
▪ If a pregnancy is planned, plasma levels of teriflunomide have to be <0.02
mg/L in 2 separate tests 14 days apart2
▪ Without cholestyramine, half-lives (t½) of up to 96 days have been found
(population kinetics analysis). For full safety in the worst case scenario, an
estimated 11×t½, or approximately 2 years, would be needed to reach a
plasma level of <0.02 mg/L3
30
1. O’Connor MD et al. N Engl J Med. 2011;365:1293-1303; 2. Claussen MC et al. Clin Immunol. 2012;142:49-56;
3. Aubagio (teriflunomide) [prescribing information]. Cambridge, MA: Genzyme Corporation; 2012.

Key Takeaways
▪ Two new oral therapies are coming soon
▪ Indicated for treatment of adults with RRMS
▪ The CHMP considers there to be a favourable benefit-risk balance for both
therapies on the basis of the data submitted:
- Quality
- Safety
- Efficacy
▪ Recommendations for approval were published on March 21, 2013
31
EMA/167896/2013 and EMA/167897/2013. Committee for Medicinal Products for Human Use. © European Medicines Agency, 2013.