Embed Size (px)
Citation preview

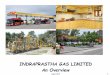
Patient with Ebola Hemorrhagic Fever, Bumba Zone, Equateur Province, DR Congo (Zaire), October 1976

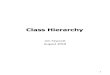
Active Surveillance for EHF Cases, Equateur Province, DR Congo (Zaire), November-December 1976

Investigations of EHF Cases in Villages, Equateur Province, DR Congo (Zaire), October-December 1976
Dr. M. Mbuyi & Nurse Sukato interviewing mourning family member

Ebola Hemorrhagic Fever in Democratic Republic of the Congo (Zaire), 1976-1977 Selected Events
Aug 26 First patient presents with fever in Yambuku, Equateur Province, receives chloroquine injection; fever resolves in 4 days
Sept 1 EHF begins in first patient
16 Local clinician reviews 17 patients; reports unknown disease to Kinshasa
23-25 First medical team visit from Kinshasa; typhoid feversuspected, vaccination; evacuation of Belgian nun to capital
30 Yambuku hospital closed, 11 of 17 staff members dead
Sept 30/Oct 20 Three nurses die in Kinshasa

Ebola Hemorrhagic Fever in Democratic Republic of the Congo (Zaire), 1976-1977 Selected Events
Oct 2-6 Second medical visit from Kinshasa; specimens
collected
3 Health zone quarantined by Minister
8-12 Transmission occurring in Kinshasa hospital
13-14 Filovirus seen on EM in Belgium, UK and USA
14 New virus (Ebola) identified at CDC
18 International Commission formed
19-27 Survey team to Yambuku; reports active cases
in 8 villages
30 Airlift of surveillance teams to NE DR Congo,
covers DRC-Sudan frontier

Nov 2 Plasmapheresis program begins with
convalescent patients
4 Widespread surveillance in epidemic zone
5 Last case dies
16 Surveillance, research and clinical care
support arrives in Yambuku
Dec 16 Emergency officially over
Jan 28 Plasmapheresis program ends
Selected Events (cont’d)
EHF in DR Congo (Zaire), 1976-1977

Ebola Hemorrhagic Fever in Democratic Republic of the Congo (Zaire), 1976-1977
International Commission Discoveries
Virology
• Isolation and characterization of Ebola virus
• Differentiation from Marburg virus
• Immunology

Ebola Hemorrhagic Fever in Democratic Republic of the Congo (Zaire), 1976-1977
Clinical
• Described symptoms and signs including
– Hemorrhagic manifestations
– Pancreatitis
• Incubation period
International Commission Discoveries

Patient Management and Control
Ebola Hemorrhagic Fever in Democratic Republic of the Congo (Zaire), 1976-1977
• Isolation of patients effective
• Surveillance of households, villages
• Plasmapheresis of convalescents
International Commission Discoveries

Ebola Hemorrhagic Fever in Democratic Republic of the Congo (Zaire), 1976-1977
Epidemiology
• Mode of transmission
• Risk groups
• Attack rates; individuals, families, villages
• Geographic distribution and spread
International Commission Discoveries

Ebola Hemorrhagic Fever in Democratic Republic of the Congo (Zaire), 1976-1977
Immunology
• Developed IFA test for Ebola
• Found evidence of previous infection
International Commission Discoveries

Ebola Hemorrhagic Fever in Democratic Republic of the Congo (Zaire), 1976-1977
Epidemic in northern DR Congo (Zaire)
• 100% of villages affected
• 100% of persons in villages affected
• 100% of affected persons in villages dead
Initial Information

Ebola Hemorrhagic Fever in Democratic Republic of the Congo (Zaire), 1976-1977
• Cause?– Typhoid– Lassa fever– Yellow fever
Initial Information
• Sources of Information– International plantation manager (confidential)– World Health Organization (limited)– US Embassy (limited)
– Scientists in Belgium and France

Ebola Hemorrhagic Fever in DR Congo (Zaire), 1976
Risk Factors Associated with Person to Person Spread
Person to Person Family Contacts
(non-infected)
Risk Factor Cases % Yes Cases % Yes P
Touched cases
Attended burial
Cared for case
Slept in same room
Prepared cadaver
Aided in delivery ofchild from sick patient
126
126
119
116
116
104
86
86
71
69
59
18
91
98
84
86
58
74
84
86
71
68
58
9
ns
ns
ns
ns
ns
p<0.001

Ebola Hemorrhagic Fever in DR Congo (Zaire), 1976
Distribution of Cases in Villages Cases Number of Villages % of Villages Cumulative %
1
2-5
6-9
10-14
15-19
20-29
30
17
18
12
4
1
1
2
55
31
33
22
7
2
2
4
31
64
86
93
95
97
101

Family Contact Attack Rate by Generation of Illness
Generation
1*
2
3
4
Total
No. of Families of Cases
61
62
18
5
146
No. of Family Exposures
496
459
117
29
1103
No. of Subsequent
Cases
38
20
3
1
62
Attack Rate (%)
7.5
4.4
2.6
3.4
5.6
* persons acquiring disease by injection
Ebola Hemorrhagic Fever in DR Congo (Zaire), 1976

Distribution of Ebola Hemorrhagic Fever Cases by Transmission Type, Yambuku, DR Congo (Zaire), 1976
Injection
Person-to-person
Both possible
Unknown
Neonatal
CasesNo.
85
149
43
30
11
318
%
27
47
14
9
3
100
SurvivorsNo.
0
30
4
4
0
38
%
0
79
11
11
0
101
Transmission History
Ebola Hemorrhagic Fever in DR Congo (Zaire), 1976

Ebola Hemorrhagic Fever, DR Congo (Zaire), 1977
Case Definitions
Probable:
• Living in epidemic area
• Died after 1 days with 2 of the following:
– headache, fever, abdominal pain, nausea/vomiting,
bleeding
• With 3 preceding weeks received an injection or had
contact with a probable or proven case
• No other diagnosis

Ebola Hemorrhagic Fever, DR Congo (Zaire), 1977
Case Definitions
Proven:
• Ebola virus isolated or shown by EM
• Or IFA titer of 1:64 after 3 weeks of symptom onset

Ebola Hemorrhagic Fever, DR Congo (Zaire), 1977
Case DefinitionsInfection:
• IFA titer 1:64 with no symptoms/signs August 15-
November 19, 1976
Possible:
• Headache and/or fever for 24 hours with or without other signs/symptoms
• Contact with a probable or proven case, within 3 weeks
• Treated with antimalarials, antibiotics, antipyretics
• Bled and checked for antibodies
• Any case of fever and bleeding anywhere in DR Congo
Neonatal:
• Newborns of probable cases if died within 28 days

Ebola Hemorrhagic Fever, DR Congo (Zaire), 1977
Case Definitions
Primary Contact:
• Face to face contact with a probable or proven case
• Between 2 days before symptom onset and death or recovery
• Surveillance 21 days from last contact
Secondary Contact:
• Face to face contact with primary contact

Ebola Hemorrhagic Fever, DR Congo (Zaire), 1976-77
Major Gaps and Challenges
• Natural history undefined
• Surveillance and response weak
• No specific treatment or precaution
• Limited application of modern technologies
• Few laboratories involved
• Filovirus and other “orphan” diseases receive
low priority