Embed Size (px)
Citation preview


Malignant Arrhythmias in Critically Ill
V. arrhythmias� Ischemic HD
� Cardiomyopathy
� Heart Failure

Malignant Arrhythmias in Critically Ill
� The long QT Syndrome,
� RV Dysplasia,
� Brugada Syndrome.
Ventricular Arrhythmias in:

Malignant Arrhythmias in Critically Ill
� Preexcited A. Fibrillation
� A. Flutter with 1:1 conduction
� Incessant forms of SVT Automatic AT
Uncommon type of AVNRT

Malignant Arrhythmias in Critically Ill
Adverse Effects of Dysrhythmias are
related to:
� Underlying Heart Disease.
� Potential for Progression (Degeneration).
� Refractoriness to Therapy.

Malignant Arrhythmias in Critically Ill
Electrolyte & Acid Base derangements
� Hypokalemia, Hypomagnesemia,
� Alkalosis
� Hypoxia “Resp. failure, Pulm-Embolism”
� Sympathodrenal activation “endogenously secreted
or exogenously administered”

Malignant Arrhythmias in Critically Ill
� Empiric Pharmcologic Therapy.
� DC External Cardioversion & Defibrillation
� Surgical Resection
Classic Approach:

Malignant Arrhythmias in Critically Ill
� EP Guided Pharmocologic Therapy,
� DC Internal Cardioversion,
� Anti Tachycardia Pacing.
Modified Approach:

Malignant Arrhythmias in Critically Ill
� Radiofrequency Catheter Ablation,
� Implantable Cardioverter Defibrillators,
� Cardiac Transplantation and
� Hopefully Gene Therapy
Modern Approach:

Malignant Arrhythmias in Critically Ill
� ECG Monitoring: Diagnostic limitations
� HRV and QT Dispersion: Risk stratification
� Signal Averaged ECG: High negative and
Low positive predictive valve

� Torsade de points: Starts with long short
coupling intervals,
� Polymorphic VT: R an T ventricular ectopics.
� Supraventricular tachycardia: Abrupt onset &
abrupt termination.
Routine monitoring:
Record the initiation & termination of arrhythmias:
Arrhythmias in Critically Ill

� Lewis Lead
� Intra atrial lead
� Esophageal ECG
Special techniques:
Arrhythmias in Critically Ill

� May not detect the full PR, QRS, or QT interval,
� The waveforms generated may be so small that they
do not consistently trigger the detection device.
� Artifacts may lead to over counting of electrical
events generated by the heart.
Arrhythmias in Critically Ill

� Positional changes may lead to severe axis
shifts, which may be misleading if only one lead
is being monitored.
� Loose electrodes may create artifacts resembling
ventricular fibrillation or asystole
� Other mechanical activity such as gastric
suction, teeth brushing, may be responsible for
creation of artifacts.
Arrhythmias in Critically Ill

Malignant Arrhythmias in Critically Ill
Programmed Electric Stimulation
� Inducibility
� Optimal drug selection
� Candidates for ICD implantation.

Malignant Arrhythmias in Critically Ill
� Arrhythmogenic Substrate,
� Autonomic Modulation, and
� Triggering Arrhythmias.
Targetted Against:

Malignant Arrhythmias in Critically Ill
Improving Myocardial Ischemia
Correcting Hypoxia, Alkalosis, Hypokalemia
Reducing Mechanical Overload
Arrhythmogenic Substrate:
NitratesPTCACABG
ACEIAng II Blockersβ-Blockers

Malignant Arrhythmias in Critically Ill
Adrenergically mediated: B-Blockers, Alpha, Beta
Blockers
Vagally-mediated:
� Vagolytic drugs,
� Pacing,
� Potassium-Channel- Blockers “Amiodarone”.
Autonomic Modulation:
α

� Xylocaine.
� Amiodarone.
� Procainamide Hcl
Pharmacologic Therapy:
Triggering Arrhythmias:
Arrhythmias in Critically Ill

� Identify & correct abnormal homeostesis,
� Suppress Triggering Arrhythmias,
� Correct Overactive Autonomic System,
� Terminate arrhythmia.
Treatment Algorithm:
Arrhythmias in Critically Ill

Emergency Termination (ADENOSINE)
� A short-acting drug (seconds) that is effective in
terminating AV nodal reentry tachyarrhythmias.
� Also used for diagnostic purposes.
� Causes transient complete AV block.
� Administered rapidly to maximize its negative
dromotropic effect.
Arrhythmias in Critically Ill

Aminophylline is a competitive antagonist and
prevents the action of adenosine.
If an initial bolus of adenosine does not cause AV
block, the dose should be doubled until block
occurs.
Emergency Termination (ADENOSINE)
Arrhythmias in Critically Ill

Ventricular Tachycardia
Supraventricular Tachycardia with:
� Aberrant conduction,
� Preexisting BBB,
� Antidromic conduction over an A-V bypass tract.
Arrhythmias in Critically Ill

ECG Differentiation:
Fusion beats
Capture beats
V. ectopics having the same tachycardia
configuration recorded before the episode.
Definite markers{
Arrhythmias in Critically Ill

� Left axis deviation � wide CRS > 14 sec� Monophasic QS in V1-V6
Suggestive markers
� A-V dissociation with V. faster than A.
Mainly EPS characterization
ECG Differentiation:
Arrhythmias in Critically Ill

Atrial flutter-fibrillation with frequent multrifocal VPCs and ventricular group beats (indicated by arrows)

Sinus rhythm with frequent VPCs and ventricular group beats (2 in a row)

A and B were obtained from the same patient with acute diaphragmatic MI. A. The rhythm is sinus with first degree AV block, APCs (X), and frequent VPCs (V) with
group beats and a short run of VT. Leads II-a, II-b, II-c, and II-d are continuous. B. Soon after the tracing A was taken, the patient developed VT as a result of frequent
VPCs with the R-on-T phenomenon. Leads II-a, II-b, and II-c are continuous

Sinus rhythm with intermittent nonparoxysmal VT (rate: 96 beats/min). None ventricular fusion beats
(FB). Leads II-a and II-b are continuous

Malignant Arrhythmias in Critically Ill
1. Antiarrhythmic drugs
Quinidine, procainamide, disopyramide, ajmaline,
amiodarone, and lidocaine
2. Other drugs
Prenylamine, phenothiazines, tricyclic antidepressant
drugs
A. Drug induced

Sinus rhythm with first degree AV block and frequent VPCs (V) with R-on-T phenomenon leading to multiform VT (torsade de pointes) and VF. The ECG abnormalities are fundamentally
caused by quinidine-induced prolonged Q-T interval with broad T wave. Leads II-a, Leads II-a, II-b, II-c, and II-e are continuous.

Malignant Arrhythmias in Critically Ill
1. Congenital Q-T prolongation syndrome
a. Jervell-Lange-Nielson syndrome
b. Romano-Ward syndrome
2. Electrolyte disturbances
a. Hypokalemia b. Hypomagnesemia
B. Nondrug induced

Malignant Arrhythmias in Critically Ill
3. Intrinsic cardiac diseasesa. Myocardial ischemia and infarction b. Myocarditis
c. Bradyarrhythmias
1) Marked sinus bradycardia (e.g., sick sinus syndrome)
2) Advanced or complete AV block
d. Mitral valve prolapse syndrome (MVPS)
4. Liquid protein diets
5. Central nervous system disorders (e.g., subarachnoid
hemorrhage)
6. Hypothermia

Ventricular flutter with a rate of 214 beats/min

Atrial fibrillation with anomalous AV conduction because of WPW syndrome, Ventricular tachycardia is closely simulated

In (C) a 12-lead ECG is depicted during sinus rhythm and orthodromiccircus movement tachycrdia in a right free-wall and (D)
anteroseptally located AP. ECG indicates electrocardiogram; and AP, accessory pathway.

In the left panel, AV conduction of 2:1 is present, changing into 1:1 AV conduction. The origin of the arrhythmia is low in the intra-atrial septum. AT indicates atrial tachycardial; and AV, atrioventricular

Shown here is AF in a patient with the WPW syndrome (A). Note AV conduction over the AP on the left and right side of the panel, with AV conduction over the AV node in the middle. As shown, the ventricular rate can become very high
during AV conduction over the AP. In (B), a posteroseptal location of the AP is shown during sinus rhythm. AAAF indicates atrial fibrillation; WPW, Wolff-
Parkinson-White; AV, atrioventricualr; and AP, accessory pathway

Shown here is VT with a relatively slow rate,
allowing the occurrence of capture and fusion
beats. The tracing was recorded in a patient with recent anterior wall MI. Note the QR pattern is
several leads during VT, VT indicates ventricular
tachycardia; and MI, myocardial infarction.

Here, a VT shows a negative concordant pattern in the precordial leads. This is diagnostic of VT. The QRS following termination of
VT shows an old antero-apical MI. VT indicates ventricular tachycardia; and MI, myocardial infarction.

Twelve-lead electrocardiogram in a patient with ventricular preexcitation during AF with a rapid preecited ventricular response

Typical characteristics of Torsade des Pointes. The initiation of the first ventricular ectopic beat of hte tachycardia tends to occur following a pause.
The QRS of this first beat initiates on the T wave making it difficult to appreciate where the T wave ends. There is a beat-to-beat change in the QRS
axis in a sinusoidal pattern. The rate of hte tachycardia tends to be slower than the polymorphic VT seen ischemia

Malignant Arrhythmias in Critically Ill
Arr. Underling Pathology Adverse effect
Sinus tachy. Acute MI. Worseing ishcemia
AF WPW Pseudo V. Tachy.
HOCM Hypotenion
Valvular HD P. Edema
AF. Flutter
PACs Hypokalemia Forerunners of AF
PVCs Hyopkalemia Frequency, Salvos
Hypomognesion Salvos
AVNRT Fast slow pathway Incessant form

Malignant Arrhythmias in Critically Ill
Arr. Underling Pathology Adverse effect
Automatic AT Atrial Disease Incessant form
Slow V. Tachycardia Reperfusion Arr. ?
V. Tachycardia Acute MI rerperfusion VF
Poly morphic VT Long QT Torsade de points

The presence of frequent PVCs appears to
be associated with an increased risk of SCD in
patients with substantial LVdysfunction (e.g.
LV (LVEF < 0.4) but not in those without heart
disease.

Lown and Wolf classified PVCs into simple and
complex forms, with examples of the latter being pairs,
and early-cycle PVCs or the R-on-T phenomenon.
Complex PVCs were considered warning arrhythmias,
i.e. arrhythmias that presaged the appearance of VF or
VT.

Subsequent studies showed the
shortcomings of warning arrhythmias. For
example, 155 (59%) of 262 patients with an
acute MI had warning arrhythmias, yet only
12 (7%) had primary VF, and 8 (40%) of 20
with primary VF had no warning arrhythmias.

Furthermore, most recorded episodes of VT
result from midcycle rather than R-on-T PVCs,
and R-on-T PVCs initiated VT in only 14 (15%)
of 94 episodes in 1 study. Event in 47 patients
with a history of VT, introduction of PVCs onto
the T wave at EP testing, did not initiate sustained
VT or VF.

Malignant Arrhythmias in Critically Ill
It is the combination of Nonsustained VT or
frequent PVCs in patients with substantial
LVdysfunction (LVEF < 0.4) that identifies a
high risk group for subsequent SCD, not the
morphological aspects of the PVC itself.

Malignant Arrhythmias in Critically Ill
The problem of sudden cardiac death (SCD)
resulted in the development of a device by
Mirowski and Colleagues in the late 1960s,
with initial reports in the 1970s and the first
human implantation in 1980s.
History

Malignant Arrhythmias in Critically Ill
The limitations of Antiarrhythmic Drug
Therapy, recently amplified by data from the
Cardiac Arrhythmia Suppression Trial
(CAST) study, provided further support to
the need for a Non Pharmacologic approach.

Malignant Arrhythmias in Critically Ill
Arrhythmia Surgery is restricted to those
who have discrete aneurysms and is usually
not performed in those with diffuse
aneursymal ventricles.

Cardiac Arrest due to VF or VT and not due to a
transient or reversible cause
Syncope of Undetermined Origin with clinically
relevant hemodynamically significant sustained VT or
VF induced at EPS testing, when prior drug therapy is
ineffective, not tolerated, or not preferred .
ACC/NASPE Guidelines, 1998

Spontaneous Sustained VT.
Nonsustained VT with CAD, prior LV
dysfunction, inducible VF, or sustained VT at
EPS testing that is not suppressible by a class-1
antiarrhythmic drug.
ACC/NASPE Guidelines, 1998

Pre-Event Trials
Post-Event Trials

I) The AVID (Antiarrhythmics Versus Implantable
Defibrillator) Trial: is a multicenter trial intended
to compare the results of best medical therapy
(Amiodarone or Sotalol) to a Transvenous ICD.
The patient group targeted was the most seriously ill
ventricular arrhythmia patient.
Post-Event Trials:

Not surprisingly, the ICD showed a survival
advantage for the patient population as a whole.
Over a mean follow-up of 18.2 months the accrued
death rates were 15.8+3.2% in the ICD group and
24+3.7% in the drug group.
ICD: Clinical Trials

The Multicenter Automatic Defibrillator
Implantation Trial (1996). A multicenter trial that
studied a very carefully selected group of post MI
patients who were at high risk for a future event.
I) MADIT
ICD: Clinical Trials

� Three weeks removed from myocardial infarction,
� Had Nonsustained VT on Holter (3-30 beats),
� An EF of less than or equal to 35%,
� NSVT was inducible into Sustained Monomorphic
VT or VF and
� Not suppressed with procainamide.
Coronary artery disease patients
ICD: Clinical Trials

196 patients enrolled and randomized to either an ICD
or conventional therapy.
At a mean follow up of 27 months the trial was
terminated prematurely at a time at which the ICD
showed marked survival benefit over conventional
therapy (39 deaths in the conventional therapy arm and
15 deaths in the ICD arm).
ICD: Clinical Trials

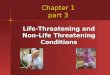
The Kaplan-Meier survival curve for the Mutlicenter Automatic Defibrillator implantation Trial population shows the clear-cut advantage of the Implantable cardivoerter defibrillator
over conventional therapy. Total mortality rate was reduced by 46% in the ICD group.
Defibrillator
ConventionalTherapy
0 1 2 3 4 5
0.0
0.2
0.4
0.6
0.8
1.0P
rob
abili
ty o
f S
urv
ival
Patients, nDefibrillator 95 80 53 31 17 3Conventional therapy 101 67 48 29 17 0
Year

Malignant Arrhythmias in Critically Ill
Patients in whom VT or VF is related to:
Acute myocardial infarction,
Transient electrolyte abnormalities, or
Drug toxicity
CONTRAINDICATIONS
Implantable Cardioverter Defibrillators

Malignant Arrhythmias in Critically Ill
Those with psychological conditions who
would not be able to adapt to this type of
therapy,
Those with a short life expectancy due to
terminal illness.
Who Should not be offered an ICD?
1.
2.

Malignant Arrhythmias in Critically Ill
Those with incessant VT due to their poor
prognosis and continuous triggering of the ICD
if sinus rhythm is restored intermitently.
Patients with frequent long runs of nonsustained
VT would also trigger frequent ICD discharges.
Who Should not be offered an ICD?
3.
4.

Malignant Arrhythmias in Critically Ill
Ventricular Tachycardia can be modified not
only by Drugs but also by pacing or
Cardioversion. This phenomonenon is familiar to
every electrophysiologist who has attempted
overdrive pacing of induced VT.
ICD Related Prblems
Exacerbation of the Arrhythmia:

Malignant Arrhythmias in Critically Ill
Occasionally the tachycardia acclerates or degenerates into VF. For this reason, Antitachycardia Pacemakers without backup Defibrillator Capability were abandoned.
Even during electrical cardivoersion, there is a similar risk of exacerbating the arrhythmia.
Exacerbation of the arrhythmia:

Malignant Arrhythmias in Critically Ill
Initially, when the ICD was investigational, the
patients viewed this device with some skepticism.
Most of the patients had few other options,
therapy with antiarrhythmic drugs having failed
while symptomatic arrhythmias continued.
Psychosocial Aspects of The ICDs

Malignant Arrhythmias in Critically Ill
Once the ICD was implanted, however, their outlook on life changed dramatically, becoming hopeful once again.
They dervied a tremendous sense of security from the ICD, knowing that if the arrhythmia recurred, they would be rescued.
Psychosocial Aspects of The ICDs

Malignant Arrhythmias in Critically Ill
What does the patient sense when the ICD discharges?
If the patient has a hemodynamically compromising arrhythmia, collapses, and immediately loses consciousness, there is no sensation of the discharge.
Psychosocial Aspects of The ICDs

Malignant Arrhythmias in Critically Ill
Some patients note very little discomfort and are barely aware that the device fired.
Some patients report a very noticeable and sometimes painful shock. Most patients describe a somewhat uncomfortable or unpleasant internal twitch or shock.
Psychosocial Aspects of The ICDs

Malignant Arrhythmias in Critically Ill
Psychologically, Patients are disappoointed that they had recurrence of the arrhythmia but also glad to be alive.
Patients with frequent discharges find them not only annoying but disconcerting. This situation requires revision of the antiarrhythmic regimen.
Psychosocial Aspects of The ICDs

Malignant Arrhythmias in Critically Ill
Kim et al., (1991) observed a total mortality ratet of 17% at 1 year, and 29% at 3 years.
Winkle et al., (1989) reported a total mortality rate of 8%, 16% and 26% after 1, 2, and 5 years of follow-up respectively.
Effect on Prognosis

Malignant Arrhythmias in Critically Ill
Some investigators have questioned the therapeutic value of ICD therapy as a whole. ICD merely changes the mode of death, converting a “Sudden Death” into a “Nonsudden” Death, resulting in little or no prolongation of life. (Conversion Hypothesis).
Effect on Prognosis

Malignant Arrhythmias in Critically Ill
The defibrillator is superior to antiarrhythmic-
drug therapy in prolonging survival among patiens
resuscitated after symtpomatic, sustained
ventricualr tachycardia or ventricular fibrillation
causing hemodynamic compromise. It should be
offered as first-line therapy to such patients.

Malignant Arrhythmias in Critically Ill
It would be unethical to withhold any therapy with potential benefit from patients at very high risk. Thus, physicians continued recommending implantable cardioverter-defibrillator therapy for high risk patients but were uncertain about the magnitude of benefit.
ICD: Clinical Bi-Impact