Embed Size (px)
Citation preview

Neonatal EKG Basics
Dr.Vinayak Vijay Kodur3rd year DM Neonatology Resident
L.T.Municipal Medical College,Mumbai




Normal Neonatal EKG

What is EKG?• The electrocardiogram (EKG) is a
representation of the electrical events of the cardiac cycle.
• Each event has a distinctive waveform• The study of waveform can lead to greater
insight into a patient’s cardiac pathophysiology.
• Electrocardiograph is a galvanometer which measures the potential difference between two points to which they are connected.

Events and EKG waveforms

Leads• The limb leads (leads I, II, III, aVR, aVL, and aVF)
provide information about the frontal projection (reflecting superior-inferior and right-to-left forces).
• The precordial leads (leads V1 through V6, V3R, and V4R) provide information about the horizontal plane, which reflects forces that are right-to-left and anterior–posterior.


Hexaxial System

Hexaxial System

Hexaxial System• The hexaxial reference system is made up by the six limb
leads and provides information about the superoinferior and right–left relationships of the electromotive forces.
• In this system, leads I and aVF cross at a right angle at the electrical center.
• The bipolar limb leads (I, II, and III) are clockwise with the angle between them of 60 degrees.
• The positive poles of aVR, aVL, and aVF are directed toward the right and left shoulders and the foot, respectively.

Hexaxial System• The positive pole of lead I is labeled as 0 degree, and the
negative pole of the same lead as Å}180 degrees. • The positive pole of aVF is designated as +90 degrees,
and the negative pole of the same lead as −90 degrees. • The positive poles of leads II and III are +60 and +120
degrees, respectively, and so on. • The hexaxial reference system is used in plotting the QRS
axis, T axis, and P axis.


Horizontal System• Consists of precordial leads (leads V1 through V6, V3R,
and V4R) and provides information about the anterior–posterior and the left–right relationship.
• The leads V2 and V6 cross approximately at a right angle at the electrical center of the heart. The V6 axis represents the left–right relationship, and the V2 axis represents the anterior–posterior relationship.
• The precordial leads V3R and V4R are at the mirror image points of V3 and V4, respectively, in the right chest.

Horizontal System• The R wave of V6 represents the leftward force and the R
wave of V2 the anterior force. • The S wave in V6 represents the rightward force and the
S wave of V2 the posterior force. • The R wave in V1, V3R, and V4R represents the
rightward and anterior force, and the S wave of these leads represents the leftward and posterior force.

Standardisation• With the full standardisation, one millivolt signal introduced
into the circuit causes a deflection of 10 mm on the record. • With the half standardisation, the same signal produces 5 mm
of deflection. • The amplitude of ECG deflections is read in millimeters
rather than in millivolts. • When the deflections are too big to be recorded, the
sensitivity may be reduced to 1 ⁄2. • With half standardisation, the measured height in millimetres
should be multiplied by 2 to obtain the correct amplitude of the deflection.

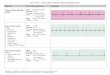
Simple Steps For Reading EKG
1. Rhythm (sinus or nonsinus) by considering the P axis2. Heart rate (atrial and ventricular rates, if different)3. The QRS axis, the T axis, and the QRS-T angle4. Intervals: PR, QRS, and QT5. The P wave amplitude and duration6. The QRS amplitude and R/S ratio; also abnormal Q waves7. ST-segment and T-wave abnormalities

Rhythm..• Sinus rhythm is the normal rhythm at any age and is
characterized by P waves preceding each QRS complex and a normal P axis (0 to +90 degrees); the latter is an often neglected criterion.
• The requirement of a normal P axis is important in discriminating sinus from nonsinus rhythm.
• In sinus rhythm, the PR interval is regular but does not have to be of normal interval. (The PR interval may be prolonged as seen in sinus rhythm with first-degree atrioventricular [AV] block.)

Rhythm• SA node is located in the right upper part of the atrial mass,
so the direction of atrial depolarisation is from the right upper part toward the left lower part, with the resulting P axis in the lower left quadrant (0 to +90 degrees) (Fig A ).
• Some atrial (nonsinus) rhythms may have P waves preceding each QRS complex, but they have an abnormal P axis (Fig B)
• For the P axis to be between 0 and +90 degrees, P waves must be upright in leads I and aVF or at least not inverted in these leads; simple inspection of these two leads suffices.
• A normal P axis also results in upright P waves in lead II and inverted P waves in aVR.

Rhythm

Heart Rate• There are many different ways to calculate the heart rate, but
they are all based on the known time scale of ECG papers. • At the usual paper speed of 25 mm/sec, 1 mm = 0.04
second, and 5 mm = 0.20 second. 1. Count the R-R cycle in six large divisions (1/50 minute)
and multiply it by 50.2. Count the number of large divisions between two R waves
and divide that into 300 (because 1 minute = 300 large divisions). or small divisions between two R waves and divide that into 1500.
3. Measure the R-R interval (in seconds) and divide 60 by the R-R interval.

Heart Rate• When the ventricular and atrial rates are different, as in
complete heart block or atrial flutter, the atrial rate can be calculated using the same methods as described for the ventricular rate; for the atrial rate, the P-P interval rather than the R-R interval is used.

Heart Rate

QRS axis• For the determination of the QRS axis (as well as T axis),
one uses only the hexaxial reference system (or the six limbs leads), not the horizontal reference system.
• Method 1: Best approach is to plot QRS axis is using lead 1 and lead avF.
• Method 2: Among the remaining four limb leads, find a lead with an equiphasic QRS complex (in which the height of the R wave and the depth of the S wave are equal). The QRS axis is perpendicular to the lead with an equiphasic QRS complex in the predetermined quadrant.

QRS axis

QRS axis

QRS axisAge QRS axis
0-1 day 60-200
1-3 days 64-197
3-7 days 75-185
7-30 days 65-160
1-3 months 31-115

QRS axis• Normal ranges of QRS axis vary with age. Newborns
normally have RAD compared with the adult standard. By 3 years of age, the QRS axis approaches the adult mean value of +50 degrees.
• The normal full-term neonate has an axis between 60-200 but by 1 month, the normal upper limit has fallen to 160 or less.
• The QRS axis in the premature newborn ECG ranges between 65 and 174.
• Abnormal QRS axis: ventricular depolarization abnormalities.

QRS axis1. Left axis deviation (LAD) is present when the QRS axis is
less than the lower limit of normal for the patient’s age. LAD occurs with LVH, LBBB, and left anterior hemiblock. Also in atrioventricular septal defect, VSD, tricuspid atresia, and WPW syndrome, but may be occasionally observed in otherwise normal infants.
2. RAD is present when the QRS axis is greater than the upper limit of normal for the patient’s age. RVH and RBBB.
3. “Superior” QRS axis is present when the S wave is greater than the R wave in aVF. Left anterior hemiblock (in the range of –30 to –90 degrees is seen in congenital heart diseases such as endocardial cushion defect and tricuspid atresia) or with RBBB.

Are you with me !!

T Axis• The T axis is determined by the same methods used to
determine the QRS axis. • In normal newborns/children/adults, the mean T axis is +45
degrees(0 to +90 degrees)• T waves must be upright in leads I and aVF. • The T waves can be flat but must not be inverted in these
leads. • The T axis outside of the normal quadrant is seen in severe
ventricular hypertrophy with “strain,” ventricular conduction disturbances, and myocardial dysfunction of a metabolic or ischemic nature

QRS-T Angle• The QRS-T angle is formed by the QRS axis and the T
axis. A QRS-T angle of greater than 60 degrees is unusual, and one greater than 90 degrees is certainly abnormal.
• The QRS-T angle outside of the normal quadrant suggests conditions with myocardial dysfunction similar to those listed for abnormal T axis.

Intervals• Three important intervals are routinely measured in the
interpretation of an ECG: PR interval, QRS duration, and QT interval.

PR interval
The normal PR interval varies with age and heart rate. The PR interval is longer in older individuals and with a slower heart rate. Prolongation of the PR interval (i.e., first-degree AV block) is seen in digitalis or quinidine toxicity, CHD (endocardial cushion defect, atrial septal defect, Ebstein’s anomaly), myocardial dysfunction, hyperkalemia, and otherwise normal heart with vagal stimulation.

PR interval• A short PR interval is present in Wolff-Parkinson-White
(WPW) preexcitation, Lown- Ganong-Levine syndrome, myocardiopathies of glycogenosis, Duchene’s muscular dystrophy (or relatives of these patients), Friedrich’s ataxia, and otherwise normal children.
• Variable PR intervals are seen in the wandering atrial pacemaker and the Wenckebach phenomena (Mobitz type I second-degree AV block).

Normal PR interval
Age PR interval
0-1 day 0·08–0·16 (0·11)
1-3 days 0·08–0·14 (0·11)
3-7 days 0·08–0·14 (0·10)
7-30 days 0·07–0·14 (0·10)
1-3 months 0·07–0·13 (0·10)

QRS Duration• “Ventricular depolarization.”• QRS duration is short in newborn and increases with age. • Prolonged QRS duration:• RBBB, LBBB, preexcitation (e.g., WPW preexcitation),
and intraventricular block (as seen in hyperkalemia, toxicity from quinidine or procainamide, myocardial fibrosis, and myocardial dysfunction of a metabolic or ischemic nature).
• Ventricular arrhythmias (e.g., premature ventricular contractions, ventricular tachycardia, implanted ventricular pacemaker)

QRS Duration• Because QRS duration varies with age, the definition of
bundle branch block (BBB) or other ventricular conduction disturbances vary with age.(>0.08 abnormal)
Age Normal QRS Duration0-1 day 0·02–0·08 (0·05)1-3 days 0·02–0·07 (0·05)3-7 days 0·02–0·07 (0·05)
7-30 days 0·02–0·08 (0·05)1-3 months 0·02–0·08 (0·05)

QT Interval• The QT interval varies primarily with heart rate. The
heart rate–corrected QT (QTc) interval is calculated by the use of Bazett’s formula,
• QTc = QT/ RR interval
Age QTc Interval1st week 0.47
1wk- 6 months 0.45>6 months 0.44

QT Interval• Long QT intervals may be seen in long QT syndrome
(e.g., Jervell and Lange-Nielsen syndrome, Romano-Ward syndrome), hypocalcemia, myocarditis, diffuse myocardial diseases (including hypertrophic and dilated cardiomyopathies.
• A short QT interval is a sign of a digitalis effect or of hypercalcemia. It is also seen with hyperthermia and in short QT syndrome (a familial cause of sudden death with QTc ≤ 300 millisecond).

P wave Amplitude and Duration• The P-wave duration and amplitude are important in the
diagnosis of atrial hypertrophy. Normally, the P amplitude is less than 3 mm. The duration of P waves is shorter than 0.09 second in children and shorter than 0.07 second in infants.
Age Normal p wave Amplitude0-1 day 2.81-3 days 2.83-7 days 2.97-30 days 3.0
1-3 months 2.6

P wave Abnormalities• Abnormal P waves may be seen in infants with atrial
enlargement or non-sinus origin of the P wave. • Ectopic atrial rhythms originate most commonly from the
low right atrium (0 to 90), high left atrium (+90 to +180) or the low left atrium (+180 to +270).
• Right atrial enlargement and/or hypertrophy typically produces increased P wave amplitude with a normal P wave duration. The P wave axis usually remains normal so the effect is usually best seen in lead II.

P wave Abnormalities• Left atrial enlargement and/or hypertrophy typically
produces an increased and prolonged negative terminal deflection of the P wave in lead V1 (generally accepted as >40 ms in duration and 0·1 mV in amplitude). Left atrial enlargement also causes exaggerated notching of the P wave in lead II although this is not a specific sign.

T wave in Rightward Leads• During the 1st days of life, right axis deviation, large R
waves and upright T waves in the right precordial leads (V3R or V4R and V1) are the norm.
• As the pulmonary vascular resistance decreases in the 1st few days after birth, the right precordial T waves become negative, In the majority of instances, this change occurs with in 48 hours of life.
• Upright T waves that persist in lead V3R , V4R or V1 beyond 1 week of life are abnormal finding indicating right ventricular strain, even in the absence of QRS voltage criteria.
• The T wave in V1 should never be positive before 6 years of age and may remain negative into adolescence.

R voltages and S voltages • Voltages in mV (1mV = 10 mm on ECG paper)

ST segment and T wave• ST segment elevations >1 mm above the isoelectric line
are uncommon in the newborn. • In neonates and infants it is better to consider as the
isoelectric line the TP segment instead of the PQ segment.
• T waves are normally quite variable in the first week of life. After 1 week, the T wave is negative in lead V1 and positive in V5–V6.

Adult Vs Neonatal• RV dominance is most noticeable in newborns, and it
gradually changes to LV dominance of adults. • By 3 years of age, the child’s ECG resembles that of
young adults. • The age-related difference in the ECG reflects an age-
related anatomic differences; the RV is thicker than the LV in newborns and infants, and the LV is much thicker than the RV in adults.

Adult Vs Neonatal• Right ventricular dominance of infants is expressed in the
ECG by right axis deviation (RAD) and large rightward or anterior QRS forces (i.e., tall R waves in lead aVR and the right precordial leads [V4R, V1, and V2] and deep S waves in lead I and the left precordial leads [V5 and V6]) compared with an adult ECG.

Adult Vs Neonatal

Adult Vs Neonatal

Age Related Changes• HR decreases• All durations and intervals increases• RV dominance gradually changes to LV dominance• QRS axis- less rightward shift• R wave in RPLs decreases and in LPLs it increases. This
is reverse for S wave

LV/RV Mass ratio
Age LV/RV mass
30 weeks 1.2:1
33 weeks 1:1
Birth 0.8:1
6Months 2:1
Adult 2.5:1

Preterm Newborns• Low voltages of QRS • Low T wave voltages• Less RV dominance• Left Axis deviation • Short PR, QRS and QT intervals• More ECG variability

Artefacts
• Can be random as with hiccoughs or limb movement.• Normal complexes are seen along with the artefacts,
and the intrinsic rhythm of the patient is not affected. • Fine, often irregular undulation of the baseline from
muscle tremors or jitteriness. Again, the intrinsic rhythm is not affected.
• The size of the QRS complex and the baseline may wander in a cyclic fashion with respirations.

Artefacts

Points To Remember!!
• ECG machine should we well earthed.• Rub good conducting gel before applying electrodes.• Use guide on electrodes while placing them.• Make sure gel applied for one chest electrode does not
spread to the adjacent one, this might cause uniform tracing in all chest leads.
• Feed the baby few mins before the procedure.• Sedate sos. (Trichlofos 50mg/kg)

Points To Remember!!
• Use 14 lead ECG (additional leads V3R and V4R) • Whenever suspecting a conduction abnormality get a
long lead 2 and V1.• As soon as done, record the name, age, sex, date and
time of ECG.• Always report the ECG in systematic manner.• Always check if baby is on cardiac medication specially
digoxin before embarking on a diagnosis.

Thank you