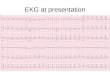
ST Elevation in Various Syndromes
Early Afterdepolarization vs ST-Elevation
Early After Depolarizations
QRS Morphology 1. Are there any pathological Q waves as a sign
of previous MI? Yes/No? 2. Are there signs of LV or RV Hypertrophy:
Yes/No? 3. Does the QRS complex show Microvoltage (< 5mV):
Yes/No? 4. Is the Conduction normal or prolonged ( > 0.12s):
Yes/No? 5. Is the R wave propagation normal? **(Normal R waves
become larger from V1-V5 (Max @ V5)) a. Is R-Wave amplitude @ V2
> R-Wave amplitude @ V3? Yes? could be a sign of a (previous)
posterior MI + others *If all these items are normal you can go on
to the next step: ST morphology
STT Elevation #1 = Acute Ischemia Early Repolarization Acute
Pericarditis: SE Elevation @ All Leads (Except AVR) Pulmonary
Embolism: St Elevation @ V1 + AVRr Hypothermia: St Elevation @ V3,
V4, V5, V6, II, III, + AVF HCM @ V3, V4, V5, (V6)
K (Hyperkalemia): @ V1, V2 (V3)
During Acute Neurologic Events: @ All Leads, (Primarily V1-V6)
Acute Sympathic Stress: @ Leads Leads, (Especially V1-V6) Brugada
Syndrome. Cardiac Aneurysm Cardiac Contusion LV-Hypertrophy
Idioventricular Rhythm Including Paced Rhythm
The T wave= morphologically variable but give hints
Flat T wave < 0.5 mm / Concordance @ Leads I, II, V3, V4, V5
or V6
Inverted T wave > 0.5 mm @ leads I, II, V3, V4, V5 or V6
Possible causes of T wave changes: Ischemia & MI
Pericarditis Myocarditis Cardiac Contusion Acute Neurologic event
(ex SAH) Mitral valve prolapse (MVP) Digoxin effect Straining
RV/LV-Hypertrophy
STT Depression #1 = Ischemia Reciprocal STsD (If one lead shows
STsE another must show STsD Straining LV-Hypertophy Digoxin effect
K, Mg
Post tachycardia) During acute neurologic events
P Wave Morphology can reveal RA-Hypertrophy, LA-Hypertrophy +
Atrial arrhythmias best determined @ leads II and V1 during sinus
rhythm.
Normal P-Wave: P-Wave max height = 2.5 mm @ leads II or III
P-Wave duration < 0.12 seconds P-Wave: Lead II: , AVF: , V1:
Biphasic
Abnormal P wave 1. Elevation or Depression of the PTa segment
PTa seg = between the p wave and QRS complex can result from atrial
infarction or pericarditis. 2. If the p-wave is enlarged, the Atria
are enlarged. 3. Inverted P-Wave = ectopic atrial rhythm
PTa seg = between the p wave and QRS complex Atrial infarction
or PericarditisElevation or Depression of the PTa segment
STT = ST Seg = ventricular repolarizationRepolarization follows
Contraction and Depolarization.
During Repolarization -Cardiomyocytes elongate and prepare for
the next heartbeat -Repolarization takes much more time than the
depolarization.
-Elongation is not passive Repolarization Starts @ J point, Ends
@ T wave. Normally the STs @ or near the isoelectric line **Minor
STT changes are not necessarily associated with cardiac
ischemia[1].
The T wave is usually "CONCORDANT" e.g. QRS = T-Wave for a given
lead
The T wave is normally in Lead I, II, AVL, AVF, V3-V6.
The T wave is normally in V1 & AVR.
The T wave is in V2 (in Blacks V3)
The T wave angle LV Endocardium repolarizes 22msec slower LV
Epicardium Repolarization = Current from the Endocardium
Epicardium
Interpreted as a signal on the ECG
Early repolarization = STE w/o without underlying
disease.Probably has nothing to do with actual early
repolarization. Commonly seen in young and understand that ER
Ischemia
EKG Morphology
P-Wave?PTa Seg?QRS?STT?T-Wave?
Denition of a pathologic Q wave Any Q-wave @ leads V2V3 0.02s or
QS complex in leads V2 and V3 Q-wave 0.03 s and > 0.1 mV deep or
QS complex in leads I, II, aVL, aVF, or V4V6 in any two leads of a
contiguous lead grouping (I, aVL,V6; V4V6; II, III, and aVF) R-wave
0.04 s in V1V2 and R/S 1 with a concordant positive T-wave in the
absence of a conduction defect