Embed Size (px)
Citation preview

M A J O R A R T I C L E
T2 Magnetic Resonance Assay for the RapidDiagnosis of Candidemia in Whole Blood:A Clinical Trial
Eleftherios Mylonakis,1 Cornelius J. Clancy,2 Luis Ostrosky-Zeichner,3 Kevin W. Garey,4 George J. Alangaden,5
Jose A. Vazquez,6 Jeffrey S. Groeger,7 Marc A. Judson,8 Yuka-Marie Vinagre,9 Stephen O. Heard,10 Fainareti N. Zervou,1
Ioannis M. Zacharioudakis,1 Dimitrios P. Kontoyiannis,11 and Peter G. Pappas12
1Infectious Diseases Division, Rhode Island Hospital, Warren Alpert Medical School of Brown University, Providence; 2Veterans Affairs PittsburghHealthcare System, Division of Infectious Diseases, University of Pittsburgh, Pennsylvania; 3Division of Infectious Diseases, University of Texas MedicalSchool at Houston and Memorial Hermann Texas Medical Center; 4University of Houston College of Pharmacy, Texas; 5Division of Infectious Diseases,Henry Ford Health System, Detroit, Michigan; 6Department of Medicine, Medical College of Georgia at Georgia Regents University, Augusta; 7Urgent CareService, Memorial Sloan Kettering Cancer Center, New York, New York; 8Division of Pulmonary and Critical Care Medicine, Albany Medical College,New York; 9Department of Critical Care Medicine, St Vincent Hospital; 10Department of Anesthesiology, UMass Memorial Medical Center, Worcester,Massachusetts; 11Department of Infectious Diseases, Infection Control and Employee Health, The University of Texas MD Anderson Cancer Center,Houston; and 12Division of Infectious Diseases, University of Alabama at Birmingham
Background. Microbiologic cultures, the current gold standard diagnostic method for invasive Candida infec-tions, have low specificity and take up to 2–5 days to grow. We present the results of the first extensive multicenterclinical trial of a new nanodiagnostic approach, T2 magnetic resonance (T2MR), for diagnosis of candidemia.
Methods. Blood specimens were collected from 1801 hospitalized patients who had a blood culture ordered forroutine standard of care; 250 of them were manually supplemented with concentrations from <1 to 100 colony-forming units (CFUs)/mL for 5 different Candida species.
Results. T2MR demonstrated an overall specificity per assay of 99.4% (95% confidence interval [CI], 99.1%–99.6%) with a mean time to negative result of 4.2 ± 0.9 hours. Subanalysis yielded a specificity of 98.9% (95% CI,98.3%–99.4%) for Candida albicans/Candida tropicalis, 99.3% (95% CI, 98.7%–99.6%) for Candida parapsilosis,and 99.9% (95% CI, 99.7%–100.0%) for Candida krusei/Candida glabrata. The overall sensitivity was found to be91.1% (95% CI, 86.9%–94.2%) with a mean time of 4.4 ± 1.0 hours for detection and species identification. The sub-group analysis showed a sensitivity of 92.3% (95% CI, 85.4%–96.6%) for C. albicans/C. tropicalis, 94.2% (95% CI,84.1%–98.8%) for C. parapsilosis, and 88.1% (95% CI, 80.2%–93.7%) for C. krusei/C. glabrata. The limit of detectionwas 1 CFU/mL for C. tropicalis and C. krusei, 2 CFU/mL for C. albicans and C. glabrata, and 3 CFU/mL for C. para-psilosis. The negative predictive value was estimated to range from 99.5% to 99.0% in a study population with 5% and10% prevalence of candidemia, respectively.
Conclusions. T2MR is the first fully automated technology that directly analyzes whole blood specimens to iden-tify species without the need for prior isolation of Candida species, and represents a breakthrough shift into a new eraof molecular diagnostics.
Clinical Trials Registration. NCT01752166.
Keywords. T2 magnetic resonance; T2MR; Candida; fungal infections; clinical trial.
Few advances have occurred in the past decades to ad-equately address the most severe and costly infectiousdiseases affecting hospitalized patients, such as invasivefungal infections. Candida species infections represent-ed 6% of all hospital-acquired infections in the UnitedStates in 2011, and ranked first among causes of pri-mary bloodstream infections [1]. Despite antifungal
Received 18 September 2014; accepted 22 November 2014.Correspondence: Eleftherios Mylonakis, MD, PhD, FIDSA, Infectious Diseases
Division, Warren Alpert Medical School of Brown University, Rhode Island Hospital,593 Eddy St, 3rd Floor, Ste 328/330, Providence, RI 02903 ([email protected]).
Clinical Infectious Diseases®
© The Author 2015. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected]: 10.1093/cid/ciu959
T2MR for Diagnosis of Candidemia • CID • 1
Clinical Infectious Diseases Advance Access published January 12, 2015 at M
cMaster U
niversity Library on January 27, 2015
http://cid.oxfordjournals.org/D
ownloaded from

therapy, candidemia has an associated mortality that is as highas 40% or more [2, 3].Along with timely control of the source ofthe infection [4], early initiation of appropriate treatment is animportant intervention to improve prognosis, particularlyamong patients with septic shock [5, 6]. For example, patientswho receive appropriate antifungal therapy within the firstday after blood is drawn for culture have an estimated mortalityof 24%, with the corresponding figures for treatment 1 and 2days later being 37% and 41%, respectively [6].
Automated blood cultures, the current “gold standard” fordiagnosis of candidemia, take 2–5 days to finalize, leading toa significant delay in the implementation of culture-driventherapy [7, 8]. In contrast, emerging methods, such as matrix-assisted laser desorption/ionization time-of-flight mass spec-trometry, require the time necessary for culture to isolate thepathogen before species identification [9], whereas molecularmethods, in particular polymerase chain reaction methodolo-gies, have limited clinical adoption to date [10]. The com-mercially available (1,3)-β-D-glucan assay is not specific forCandida, and high rates of false-positive results in high-riskpopulations have been reported [11].
The lack of diagnostic tools has led to the current clinical re-ality, where the administration of antifungal agents remainsmerely a “best guess” based on the local epidemiology and theindividual patient’s risk factors and clinical picture [7, 12]. Thisoveruse of the few available antifungal agents is concerning, inlight of the side effects [13] and the excess cost [14], as well asthe association of antifungal treatment with the rise of resistantpathogens [15–17]. Thus, diagnostic methods that directly testwhole clinical samples and provide rapid, sensitive, and specificresults are long awaited [8, 11, 18–21].
A new nanodiagnostic method using manual application of T2magnetic resonance (T2MR) to detect Candida species was pre-viously found to have high sensitivity and specificity and a time toresult of <3 hours [22]. This technology was used to develop anautomated instrument platform, T2Dx, to provide a “patientsample-to-answer” clinical diagnostic test, T2Candida, which iscurrently approved by the US Food and Drug Administration(FDA). By augmenting the T2MR technology with on-boardsample handling technology, the fully automated T2Dx increasesthroughput while also enabling multiplex detection of 5 Candidaspecies on a single blood sample. Herein, we present the results ofthe first extensive clinical trial to validate the sensitivity and spe-cificity of the new approach to diagnose candidemia.
METHODS
T2Dx InstrumentThe T2Dx instrument automatically completes all steps in theT2Candida panel after specimen loading. Specifically, T2Dxlyses the red blood cells, concentrates the pathogen cells and
cellular debris, lyses the Candida cells by mechanical bead beat-ing, amplifies Candida DNA using a thermostable polymerase(T2Biosystems, Inc) and pan-Candida primers for the interven-ing transcribed spacer 2 region within the Candida ribosomalDNA operon, and finally, detects amplified product by ampli-con-induced agglomeration of supermagnetic particles andT2MR measurement. The internal control, a synthetic DNA tar-get, monitors the integrity of the T2Candida results and is pro-cessed with each clinical specimen. If the internal control isinvalid and there are no positive T2MR signals, an “invalid” re-sult is displayed, indicating that the specimen could contain in-hibitors that would interfere with Candida detection. Thereadout of the test is positive or negative without any quantifiabledata report. Also, positive and negative T2Candida external con-trols were run each day before loading clinical specimens forquality-control checks of the reagents and the T2Dx instrument.
Patients and Data CollectionThe clinical trial was conducted from 31 July 2013 to 24 April2014 at 12 centers (Supplementary Table 1). The institutionalreview board of each center approved the study protocol. Writ-ten informed consent was obtained from all patients. Patientsaged 18–95 years with a blood culture ordered per routine stan-dard of care during their current hospitalization were enrolled(ClinicalTrials.gov identifier: NCT01752166).
Sample Collection and OutcomesA set of aerobic and anaerobic blood cultures and 3 whole bloodT2MR specimens were collected. T2MR clinical specimens werecollected in prelabeled and de-identified K2 ethylenediaminetet-raacetic acid plastic blood collection vacutainers. Tube A wasstored at room temperature (20°C–25°C) and was analyzedwithin 12 hours of collection, whereas tubes B and C weremaintained in frozen storage (−70°C to −80°C).
A total of 300 samples (also collected from patients referredfor a blood culture per routine standard of care) were used forthe contrived arm of the study. More specifically, 250 were man-ually supplemented (contrived samples) with clinically relevanttiters of the 5 Candida species targeted by the T2MR technology(C. albicans, C. glabrata, C. parapsilosis, C. tropicalis, and C.krusei), and 50 were used as negative controls. Different clinicalisolates were used for each specimen. The contrived arm of thestudy was developed in collaboration with the FDA prior to thebeginning of the study due to the expectation that the prospec-tive arm would not recruit candidemic patients representative ofthe full range of titer levels in infected patients, and due to thelimitations of blood culture as a comparator, including its poorsensitivity. Contrived specimens were spiked at known concen-trations of the targeted Candida species based on FDA inputregarding the range of clinically relevant concentrations. Colo-ny-forming units (CFUs) were confirmed by culture on yeast
2 • CID • Mylonakis et al
at McM
aster University L
ibrary on January 27, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

peptone dextrose agar media. Contrived specimens were de-identified as to the Candida species and concentration, andwere shipped under refrigerated conditions (2°C–8°C) to eachtest site. Each specimen was analyzed within 48 hours of receipt,after having been placed at room temperature for 1–12 hours toequilibrate. This incubation at room temperature for up to 12hours was previously shown to have no effect on the CFUsper milliliter of the specimens (data not shown). The specimensof the contrived arm of the study were randomly inserted intothe clinical specimens with which they were tested at the sametime. Finally, the limit of detection (LOD) for the assay was de-termined by 10 different isolates (2 each from the 5 differentCandida species) using quantified spiked samples. The LODwas defined as the lowest CFU per milliliter of Candida speciesin a specimen that was detected with ≥95% positive detectionfor ≥20 replicates. When a different LOD was observed acrossthe 2 tested strains, the higher level of CFUs per milliliter wasdetermined as the LOD for that species.
T2Candida panel results are grouped on the basis of antifun-gal resistance patterns of different Candida species [7], and 3results are reported: C. albicans/C. tropicalis, C. krusei/C. glab-rata, and C. parapsilosis. The blood culture specimens werepromptly processed in accordance with routine institutionalpractice for a period of 5–7 days, using one of the followingFDA-cleared methods: BacT/Alert 3D system (bioMérieux,Durham, North Carolina), BacTec FX system (BD Diagnostics,Sparks, Maryland), and Versatrek system (TREK DiagnosticSystems, Cleveland, Ohio).
Statistical AnalysisThe sensitivity and specificity of the T2MR technology, both perpatient and per assay, were examined by comparing the T2Can-dida results to the blood culture results and the known Candidastate of the contrived specimens. For the calculation of the sen-sitivity and specificity per patient, each patient was consideredpositive or negative based on all 3 results of the T2Candidapanel, whereas for the per-assay estimations, the 3 results ofeach patient were considered separately. The sensitivity and spe-cificity along with the 2-sided 95% confidence intervals (CIs)were calculated using the exact Clopper–Pearson method. Con-tinuous variables were presented as means and standard devia-tions, and categorical data as relative frequencies. Time to resultof T2MR technology and automated blood cultures was com-pared using the Student t test. Statistical significance was setat P = .05.
RESULTS
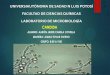
Study PatientsOverall, 2264 patients were enrolled and 463 were excludedfrom the final analysis. In 245 of 463 cases, T2MR yielded an
indeterminate result due to either a technical error (90 cases)or an invalid result (155 cases) (Figure 1). Therefore, 1801 re-sults were included in the final analysis. Specifically, 1501 pa-tients had blood cultures drawn concurrently and from thesame anatomical sites as the T2MR specimens, 250 gave sam-ples that were spiked with known and clinically relevant con-centrations of different Candida species, and 50 providedCandida-negative control samples for the contrived arm ofthe study. Table 1 shows the demographic characteristics ofpatients.
Sensitivity and SpecificityResults of the primary analysis are shown in Table 2. Among the250 specimens spiked at concentrations from <1 CFU/mL to100 CFU/mL for the 5 different Candida species and the 6 pro-spectively collected specimens that had positive blood cultureresults for Candida species, the T2MR technology had an over-all sensitivity per assay of 91.1% (95% CI, 86.9%–94.2%) andper patient of 91.0% (95% CI, 86.8%–94.2%). The subgroupanalysis showed a sensitivity of 92.3% (95% CI, 85.4%–96.6%)for C. albicans/C. tropicalis, 94.2% (95% CI, 84.1%–98.8%) forC. parapsilosis, and 88.1% (95% CI, 80.2%–93.7%) for C. krusei/C. glabrata. The LOD was found to be 1 CFU/mL for C. tropi-calis and C. krusei, 2 CFU/mL for C. albicans and C. glabrata,and 3 CFU/mL for C. parapsilosis (Supplementary Table 2).
The overall specificity was found to be 99.4% (95% CI,99.1%–99.6%) per assay and 98.1% (95% CI, 97.3%–98.7%)per patient. Subanalysis on different Candida species showeda specificity of 98.9% (95% CI, 98.3%–99.4%) for C. albicans/C. tropicalis, 99.3% (95% CI, 98.7%–99.6%) for C. parapsilosis,and 99.9% (95% CI, 99.7%–100.0%) for C. krusei/C. glabrata.The mean time to negative result, among the prospectively col-lected samples, was 4.2 ± 0.9 hours compared with ≥120 hoursfor blood cultures per institutional protocols. With an overallsensitivity of 91.0% and specificity of 98.1% per patient, the pos-itive predictive value of T2MR technology is estimated to rangefrom 71.6% to 84.2% in a study population with 5% and 10%prevalence of candidemia, respectively. The corresponding fig-ures for the negative predictive value (NPV) are 99.5% and99.0% in respective settings (Table 3).
Among the prospectively collected samples, there were 4patients characterized as candidemic with the same Candidaspecies both from T2MR and the companion blood cultures.The mean time to species identification was 4.4 ± 1.0 hoursfor T2MR and 129.9 ± 26.3 hours for the blood cultures(P < .001). One patient presented with a coinfection of C. albi-cans and C. parapsilosis in blood culture, and both species weredetected by T2MR technology in a single test.
There were 31 discordant cases (1.7%) between the T2MRand blood cultures. In 2 cases, the blood cultures identifiedthe patients as candidemic and the T2Dx instrument did not;
T2MR for Diagnosis of Candidemia • CID • 3
at McM
aster University L
ibrary on January 27, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

in 29 cases Candida was detected by the T2Dx instrument butnot by routine blood cultures. Both cases of discordant T2MR-negative blood culture–positive results were in oncology pa-tients with central lines who were on antifungal agents prior toblood draw. In both cases, the identified species was C. albicans.In the 29 discordant T2MR-positive, blood culture–negativesamples, 18 C. albicans/C. tropicalis, 12 C. parapsilosis, and 1C. krusei/C. glabrata were identified. Among these cases, therewas 1 with proven candidiasis based on the European Organi-zation for the Treatment of Cancer (EORTC) criteria [23]. Morespecifically, the patient had intra-abdominal C. albicans infec-tion, which was detected by the T2MR technology and wasproven later with culture of tissue obtained during surgeryafter >12 negative blood cultures. Finally, in 4 of 29 cases, Can-dida species was isolated from other clinical samples (respirato-ry secretions [3 patients] and urine [1 patient]), but thesepatients did not meet established criteria for invasive candidia-sis. Another 6 patients were receiving systemically antifungaltherapy but had no other evidence of fungal infection.Among the remaining 18 patients, 5 had a central line, 4 had
undergone stem cell or solid organ transplant (1 patient alsohad a central line), and 3 were oncology patients (1 was also atransplant recipient). The individual characteristics of the pa-tients with T2MR-positive, blood culture–negative results arepresented in Supplementary Table 3.
Reproducibility of T2MRTwo individual samples spiked with each one of C. albicans,C. parapsilosis, and C. glabrata, one at a concentration of 1–2times the LOD and one at 3–4 times the LOD, as well as 1 neg-ative sample, were tested in triplicate, twice daily for a total of 6days across 3 different sites. Overall, T2MR was found to be98.5% reproducible (Table 4).
DISCUSSION
Candida species infections are increasing [24], currently ac-counting for 6% of all hospital-acquired infections [1]. TheT2MR technology was able to correctly characterize 98.1% ofpatients as noncandidemic, with a mean time to negative result
Figure 1. Enrollment and outcomes for the prospective and the contrived arm of the study. *Subjects are counted only once within each main protocoldeviation category, but may be counted multiple times across protocol deviation categories. **Contrived samples delayed by weather or delivery service,personnel not available to run the specimens, T2Dx instrument not available due to a performance issue, contrived specimen did not load into the sampleinlet due to a clot, or T2 enrollment closed. †Indeterminate results were due to invalid internal controls (149), instrument malfunction (82), invalid T2 channel(6), failure of external control (3), sample inlet failure (4), and T2Dx drawer error (1). Abbreviation: CFUs, colony-forming units.
4 • CID • Mylonakis et al
at McM
aster University L
ibrary on January 27, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

of 4.2 hours. In a patient population with 6% prevalence ofCandida infections [1], this estimation would correspond toan NPV of 99.4%. The ability to rapidly and accurately excludethe possibility of candidemia can have significant implicationsin clinical practice, by decreasing the number of patients whoneed to be on empiric antifungal therapy [7, 12], and thus de-creasing the incidence of resistant strains [15–17], the potentialof side effects of antifungal treatment [13], and substantialhealthcare costs [14, 20].
In 29 cases, T2Candida panel results were in discordancewith negative blood cultures. This discordance can represent ei-ther false-positive T2MR, or false-negative blood culture results.Blood culture methods, although currently the gold standardfor candidemia diagnosis, are known to have poor sensitivityin clinical samples and are shown to be positive in only 38%
of proven and probable cases of invasive candidiasis [10], as de-fined by the EORTC criteria [23]. These discordant results
Table 1. Baseline Characteristics of Study Participants
Characteristic
ProspectiveCohort
(n = 1501)
ContrivedCohort(n = 300)
Demographic characteristics
Male sex 840 (56.0%) 180 (60.0%)Female sex 661 (44.0%) 120 (40.0%)
Age, y, mean ± SD 55.4 ± 15.7 56.9 ± 17.0
Race/ethnicityWhite 1170 (77.9%) 251 (83.7%)
Black 302 (20.1%) 26 (8.7%)
Other 29 (1.9%) 23 (7.7%)Medical history
Immunocompromised subjects 720 (48.0%) 102 (34.0%)
Cancer 379 (52.6%) 62 (60.8%)Transplant 302a (41.9%) 20 (19.6%)
Stem cell 130 (43.0%) 2 (10.0%)
Solid organ 171 (56.7%) 17 (85.0%)Otherb 2 (0.7%) 1 (5.0%)
HIV/AIDS 51 (7.1%) 12 (11.8%)
On steroid therapy 306 (42.5%) 36 (35.3%)Other IC states 41 (5.7%) 2 (2.0%)
Nonimmunocompromisedsubjects
781 (52.0%) 198 (66.0%)
Diabetes mellitus 270 (34.6%) 66 (33.3%)
Abdominal surgeryc 129 (16.6%) 8 (4.0%)
Renal failurec 100 (12.8%) 32 (16.2%)Cardiovascular 490 (62.7%) 124 (62.6%)
Burnsc 6 (0.8%) 0 (0.0%)
Data are presented as No. (%) unless otherwise indicated.
Abbreviations: HIV, human immunodeficiency virus; IC, immunocompromised;SD, standard deviation.a 1 patient had both solid organ and bone marrow transplant.b 2 patients with islet cell transplant (prospective cohort), 1 patient with rightiliac crest bone graft (contrived cohort).c During current hospitalization.
Table 2. Overall Sensitivity and Specificity of the T2 MagneticResonance Method
Sensitivity No. % 95% CI
Overall per patienta 233/256 91.0 86.8–94.2
Overall per assaya 234/257 91.1 86.9–94.2Per Candida speciesa
C. albicans/tropicalis 96/104 92.3 85.4–96.6
C. parapsilosis 49/52 94.2 84.1–98.8C. krusei/glabrata 89/101 88.1 80.2–93.7
Per Candida species and per CFU/mLb
C. albicans<1 CFU/mL 8/10 80.0 44.4–97.5
1–10 CFU/mL 18/18 100.0 81.5–100.0
11–30 CFU/mL 17/17 100.0 80.5–100.031–100 CFU/mL 5/5 100.0 47.8–100.0
Overall 48/50 96.0 86.3–99.5
C. tropicalis<1 CFU/mL 8/10 80.0 44.4–97.5
1–10 CFU/mL 16/18 88.9 65.3–98.6
11–30 CFU/mL 17/17 100.0 80.5–100.031–100 CFU/mL 5/5 100.0 47.8–100.0
Overall 46/50 92.0 80.8–97.8
C. parapsilosis<1 CFU/mL 8/10 80.0 44.4–97.5
1–10 CFU/mL 17/18 94.4 72.7–99.9
11–30 CFU/mL 17/17 100.0 80.5–100.031–100 CFU/mL 5/5 100.0 47.8–100.0
Overall 47/50 94.0 83.5–98.7
C. krusei<1 CFU/mL 6/10 60.0 26.2–87.8
1–10 CFU/mL 18/18 100.0 81.5–100.0
11–30 CFU/mL 17/17 100.0 80.5–100.031–100 CFU/mL 5/5 100.0 47.8–100.0
Overall 46/50 92.0 80.8–97.8
C. glabrata<1 CFU/mL 5/10 50.0 18.7–81.3
1–10 CFU/mL 16/18 88.9 65.3–98.6
11–30 CFU/mL 16/17 94.1 71.3–99.831–100 CFU/mL 5/5 100.0 47.8–100.0
Overall 42/50 84.0 70.9–92.8
SpecificityOverall per patienta 1516/1545 98.1 97.3–98.7
Overall per assaya 5114/5146 99.4 99.1–99.6
Per speciesa
C. albicans/tropicalis 1679/1697 98.9 98.3–99.4
C. parapsilosis 1736/1749 99.3 98.7–99.6
C. krusei/glabrata 1699/1700 99.9 99.7–100.0
Abbreviations: CFU, colony-forming unit; CI, confidence interval.a Based on the prospective and the contrived arm of the study.b Based only on the results of the spiked samples.
T2MR for Diagnosis of Candidemia • CID • 5
at McM
aster University L
ibrary on January 27, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

motivated a post hoc analysis of the individual patients’ notes.This analysis showed that there was 1 case with later proven in-vasive candidiasis, and 4 cases with Candida species isolation
from other clinical samples, but these patients did not meet es-tablished criteria for invasive candidiasis. The above findingsindicate that at least some of these discordant results may rep-resent cases of Candida species infections that were missed bythe blood culture. Importantly, cultures can be inhibited by an-tifungal agents, and some Candida species may need more thanthe typical 5-day culture time to grow [25, 26]. In contrast,T2MR technology performance has not been shown to be al-tered by antifungal agents [22].
A significant percentage of the cohort had high-risk hostfactors for invasive Candida infections, such as current canceror neutropenia, steroid therapy, solid or stem cell transplant,or current abdominal surgery (Table 1) [23, 27]. Of note,there were no clinical or mycological inclusion criteria, otherthan a blood culture order per routine standard of care. There-fore, the anticipated prevalence of Candida infections inour population was low. This allowed the evaluation of NPVof the new technology to be done with high precisionamong a population with high-risk characteristics. The low
Table 3. Positive and Negative Predictive Values of T2 MagneticResonance Method for a Range of Prevalence of Candidemia
Prevalence ofDisease
91.0% Sensitivity/98.1%Specificity
PPV NPV
1% 32.6% 99.9%
2% 49.4% 99.8%5% 71.6% 99.5%
10% 84.2% 99.0%
20% 92.3% 97.8%35% 96.3% 95.3%
50% 98.0% 91.6%
Abbreviations: NPV, negative predictive value; PPV, positive predictive value.
Table 4. Results of the Reproducibility Study
Candida Species Concentration Test Site No. Detected No. Not Detected % Agreement With Expected
C. parapsilosis 1–2× LOD Site 1 36 0 108/108 (100%)
Site 2 36 0Site 3 36 0
All sites 108 0
3–4× LOD Site 1 36 0 108/108 (100%)Site 2 36 0
Site 3 36 0
All sites 108 0C. glabrata 1–2× LOD Site 1 35 1 105/108 (97.2%)
Site 2 34 2
Site 3 36 0Total 105 3
3–4× LOD Site 1 36 0 106/108 (98.1%)
Site 2 35 1Site 3 35 1
Total 106 2
C. albicans 1–2× LOD Site 1 35 1 103/108 (95.4%)Site2 35 1
Site 3 33 3
Total 103 53–4× LOD Site 1 35 1 107/108 (99.1%)
Site 2 36 0
Site 3 36 0Total 107 1
Negative NA Site 1 0 36 108/108 (100%)
Site 2 0 36Site 3 0 36
Total 0 108
Abbreviations: LOD, limit of detection; NA, not defined.
6 • CID • Mylonakis et al
at McM
aster University L
ibrary on January 27, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

anticipated prevalence and the limitations of blood culture as agold standard comparator created the need to investigate con-trived samples for determining the sensitivity of the T2MRtechnology.
The T2MR technology was found to have an overall sensitiv-ity per patient of 91.0%, with a mean time to species identifi-cation of only 4.4 hours, compared to the 2–5 days typicallyneeded by the automated blood culture systems [8]. This differ-ence in time of identification could impact the mortality of can-didemic patients [5, 6]. Another important aspect of the rapidspeciation is the potential for appropriate choice of antifungaltherapy, as the 5 target Candida species of the T2MR technol-ogy account for >95% of cases of candidemia [28], and have dis-tinct antifungal susceptibility profiles [29, 30]. Notably, T2MRtechnology was found to have an LOD as low as 1 CFU/mLfor 2 Candida species. This may prove specifically useful inthe diagnosis of candidemia coming from the gastrointestinaltract, where the burden of organisms is low, especially amongpatients on antifungals [31]. Also, T2MR has the potential ofsimultaneously identifying >1 species, a unique characteristic,and particularly interesting in the light of 2%–5% prevalenceof mixed candidemia [32]. However, this high yield needs tobe verified in prospective samples and in comparison with acombination of clinical, imaging, and autopsy results [23].
Importantly, this new technology has a high sensitivity inidentifying non-albicans Candida species. During recentyears, there has been a shift in the Candida epidemiology,with non-albicans species representing >50% of clinical isolates[29]. Among them, C. glabrata is reported to be isolated in asmany as 26% of candidemic patients [33, 34]. Although culturemethods are shown to identify some Candida species in spikedblood samples with an adequate sensitivity [35–38], this has notbeen the case for C. glabrata, with reported sensitivities as lowas 60% in samples spiked with 100 CFU/mL [35–37, 39]. Thismight be explained by its slow growth in the blood/broth mix-ture, which results in a long time to culture positivity, frequentlybeyond the typical 5-day culture period [25, 26]. The T2MRtechnology was shown to be able to detect C. glabrata at an un-precedented LOD of 2 CFU/mL with an overall sensitivity of84.0%.
As a limitation of this study, it should be noted that in 245cases the T2MR result was indeterminate. We can assumethat rerunning the sample could be a reasonable fix in the36.7% (90/245) of cases that were due to a technical error. How-ever, further studies are needed to clarify if this will also happenin the cases where the T2MR result was invalid. Also, due to thelimited number of candidemic patients who were enrolled inour study, the clinical sensitivity of T2MR should be assessedin future studies.
This study presents the results of the first extensive clinicaltrial using the T2MR technology. This technology represents
an example of the emerging era of molecular diagnostics,where rapid, accurate, and species-specific diagnosis directlyon the clinical sample is feasible. A key advantage of T2MRover other biosensors is that it does not require culture and sam-ple purification or preparation, making T2MR a promising can-didate for point-of-care diagnostics of infectious pathogens andcertain noninfectious diseases [9]. T2MR managed to identify91% of Candida-positive samples and >98% of noncandidemicpatients. Because mortality due to invasive candidiasis has re-mained high and unchanged for the past 2 decades [29], andearly initiation of appropriate antifungal therapy has been re-ported to reduce mortality by at least two-thirds [5], the rapidand accurate diagnostic capability offered by this novel technol-ogy has the potential to change the management and prognosisof the disease.
Supplementary Data
Supplementary materials are available at Clinical Infectious Diseases online(http://cid.oxfordjournals.org). Supplementary materials consist of data pro-vided by the author that are published to benefit the reader. The posted ma-terials are not copyedited. The contents of all supplementary data are thesole responsibility of the authors. Questions or messages regarding errorsshould be addressed to the author.
Notes
Acknowledgments. The authors acknowledge Drs Robert Langer andTom Lowery for helpful discussions.Financial support. This work was supported by T2 Biosystems.Potential conflicts of interest. E. M. has received grant support from
Boehringer Ingelheim, T2 Biosystems, and Astellas and has served on an ad-visory board for Astellas. C. J. C. has received investigator-initiated researchfunding fromMerck, Pfizer, and CSL-Behring. L. O.-Z. has received researchgrants, consulting, and speaking honoraria fromMerck, Pfizer, and Astellas,and research grants from Associates of Cape Cod and T2 Biosystems.K. W. G. has received grant support from T2 Biosystems. J. A. V. has servedon the speakers’ bureaus for Astellas and Pfizer, as a consultant for Astellasand Miravista, and on the advisory board of Astellas, and has receivedhonoraria from Astellas and research grants from Merck. J. S. G. is on theclinical advisory board of T2 Biosystems. M. A. J. is a consultant for Celgene,Novartis, Mitsubishi-Tanabe, Questcor, and Janssen and has received royal-ties from Springer and UpToDate. D. P. K. is on the advisory board of Merckand has received research support from Merck, Pfizer, and Astellas andhonoraria from Merck, Astellas, Gilead, and Pfizer. P. G. P has receivedgrants/research support from T2 Biosystems, Astellas, Gilead, and Merckand is on an ad hoc scientific advisory committee for T2 Biosystems,Merck, Astellas, and Gilead. All other authors report no potential conflicts.All authors have submitted the ICMJE Form for Disclosure of Potential
Conflicts of Interest. Conflicts that the editors consider relevant to the con-tent of the manuscript have been disclosed.
References
1. Magill SS, Edwards JR, Bamberg W, et al. Multistate point-prevalencesurvey of health care-associated infections. N Engl J Med 2014;370:1198–208.
2. Andes DR, Safdar N, Baddley JW, et al. Impact of treatment strategy onoutcomes in patients with candidemia and other forms of invasive can-didiasis: a patient-level quantitative review of randomized trials. ClinInfect Dis 2012; 54:1110–22.
T2MR for Diagnosis of Candidemia • CID • 7
at McM
aster University L
ibrary on January 27, 2015http://cid.oxfordjournals.org/
Dow
nloaded from

3. Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, EdmondMB. Nosocomial bloodstream infections in US hospitals: analysis of24,179 cases from a prospective nationwide surveillance study. ClinInfect Dis 2004; 39:309–17.
4. Kollef M, Micek S, Hampton N, Doherty JA, Kumar A. Septic shockattributed to Candida infection: importance of empiric therapy andsource control. Clin Infect Dis 2012; 54:1739–46.
5. Morrell M, Fraser VJ, Kollef MH. Delaying the empiric treatment ofCandida bloodstream infection until positive blood culture results areobtained: a potential risk factor for hospital mortality. AntimicrobAgents Chemother 2005; 49:3640–5.
6. Garey KW, Rege M, Pai MP, et al. Time to initiation of fluconazole ther-apy impacts mortality in patients with candidemia: a multi-institutionalstudy. Clin Infect Dis 2006; 43:25–31.
7. Pappas PG, Kauffman CA, Andes D, et al. Clinical practice guidelinesfor the management of candidiasis: 2009 update by the InfectiousDiseases Society of America. Clin Infect Dis 2009; 48:503–35.
8. Arvanitis M, Anagnostou T, Fuchs BB, Caliendo AM,Mylonakis E. Mo-lecular and nonmolecular diagnostic methods for invasive fungal infec-tions. Clin Microbiol Rev 2014; 27:490–526.
9. Marklein G, Josten M, Klanke U, et al. Matrix-assisted laser desorptionionization-time of flight mass spectrometry for fast and reliable identi-fication of clinical yeast isolates. J Clin Microbiol 2009; 47:2912–7.
10. Avni T, Leibovici L, Paul M. PCR diagnosis of invasive candidiasis: sys-tematic review and meta-analysis. J Clin Microbiol 2011; 49:665–70.
11. Clancy CJ, Nguyen MH. Finding the “missing 50%” of invasive candi-diasis: how nonculture diagnostics will improve understanding of dis-ease spectrum and transform patient care. Clin Infect Dis 2013; 56:1284–92.
12. Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: in-ternational guidelines for management of severe sepsis and septic shock:2012. Crit Care Med 2013; 41:580–637.
13. Walsh TJ, Teppler H, Donowitz GR, et al. Caspofungin versus liposomalamphotericin B for empirical antifungal therapy in patients with persis-tent fever and neutropenia. N Engl J Med 2004; 351:1391–402.
14. Arnold HM, Micek ST, Shorr AF, et al. Hospital resource utilization andcosts of inappropriate treatment of candidemia. Pharmacotherapy 2010;30:361–8.
15. Garnacho-Montero J, Diaz-Martin A, Garcia-Cabrera E, et al. Risk fac-tors for fluconazole-resistant candidemia. Antimicrob Agents Chemo-ther 2010; 54:3149–54.
16. Beyda ND, Lewis RE, Garey KW. Echinocandin resistance in Candidaspecies: mechanisms of reduced susceptibility and therapeutic ap-proaches. Ann Pharmacother 2012; 46:1086–96.
17. Alexander BD, JohnsonMD, Pfeiffer CD, et al. Increasing echinocandinresistance in Candida glabrata: clinical failure correlates with presenceof FKS mutations and elevated minimum inhibitory concentrations.Clin Infect Dis 2013; 56:1724–32.
18. Kontoyiannis DP. Invasive mycoses: strategies for effective manage-ment. Am J Med 2012; 125(1 suppl):S25–38.
19. Pappas PG. Opportunistic fungi: a view to the future. Am J Med Sci2010; 340:253–7.
20. Aitken SL, Beyda ND, Shah DN, et al. Clinical practice patterns in hos-pitalized patients at risk for invasive candidiasis: role of antifungal stew-ardship programs in an era of rapid diagnostics. Ann Pharmacother2014; 48:683–90.
21. Leon C, Ostrosky-Zeichner L, Schuster M. What’s new in the clinicaland diagnostic management of invasive candidiasis in critically ill pa-tients. Intensive Care Med 2014; 40:808–19.
22. Neely LA, Audeh M, Phung NA, et al. T2 magnetic resonance enablesnanoparticle-mediated rapid detection of candidemia in whole blood.Sci Transl Med 2013; 5:182ra154.
23. De Pauw B, Walsh TJ, Donnelly JP, et al. Revised definitions of invasivefungal disease from the European Organization for Research and Treat-ment of Cancer/Invasive Fungal Infections Cooperative Group and theNational Institute of Allergy and Infectious Diseases Mycoses StudyGroup (EORTC/MSG) Consensus Group. Clin Infect Dis 2008;46:1813–21.
24. Miceli MH, Diaz JA, Lee SA. Emerging opportunistic yeast infections.Lancet Infect Dis 2011; 11:142–51.
25. Huang L, Zhang YY, Sun LY. Time to positivity of blood culture canpredict different Candida species instead of pathogen concentrationin candidemia. Eur J Clin Microbiol Infect Dis 2013; 32:917–22.
26. Lai CC, Wang CY, Liu WL, Huang YT, Hsueh PR. Time to positivity ofblood cultures of different Candida species causing fungaemia. J MedMicrobiol 2012; 61(pt 5):701–4.
27. Guinea J. Global trends in the distribution of Candida species causingcandidemia. Clin Microbiol Infect 2014; 20(suppl 6):5–10.
28. Pfaller MA, Jones RN, Castanheira M. Regional data analysis of Candi-da non-albicans strains collected in United States medical sites over a 6-year period, 2006–2011. Mycoses 2014; 57:602–11.
29. Pfaller MA, Diekema DJ. Epidemiology of invasive candidiasis: a persis-tent public health problem. Clin Microbiol Rev 2007; 20:133–63.
30. Pfaller MA, Messer SA, Woosley LN, Jones RN, Castanheira M. Echino-candin and triazole antifungal susceptibility profiles for clinical oppor-tunistic yeast and mold isolates collected from 2010 to 2011: applicationof new CLSI clinical breakpoints and epidemiological cutoff values forcharacterization of geographic and temporal trends of antifungal resis-tance. J Clin Microbiol 2013; 51:2571–81.
31. Kontoyiannis DP, Reddy BT, Hanna H, Bodey GP, Tarrand J, Raad II.Breakthrough candidemia in patients with cancer differs from de novocandidemia in host factors and Candida species but not intensity. InfectControl Hosp Epidemiol 2002; 23:542–5.
32. Jensen J, Munoz P, Guinea J, Rodriguez-Creixems M, Pelaez T, Bouza E.Mixed fungemia: incidence, risk factors, and mortality in a general hos-pital. Clin Infect Dis 2007; 44:e109–14.
33. Horn DL, Neofytos D, Anaissie EJ, et al. Epidemiology and outcomes ofcandidemia in 2019 patients: data from the prospective antifungal ther-apy alliance registry. Clin Infect Dis 2009; 48:1695–703.
34. Pfaller MA, Diekema DJ, Gibbs DL, et al. Results from the ARTEMISDISK Global Antifungal Surveillance study, 1997 to 2005: an 8.5-yearanalysis of susceptibilities of Candida species and other yeast speciesto fluconazole and voriconazole determined by CLSI standardizeddisk diffusion testing. J Clin Microbiol 2007; 45:1735–45.
35. Horvath LL, Hospenthal DR, Murray CK, Dooley DP. Detection ofsimulated candidemia by the BACTEC 9240 system with plus aero-bic/F and anaerobic/F blood culture bottles. J Clin Microbiol 2003;41:4714–7.
36. Horvath LL, George BJ, Murray CK, Harrison LS, Hospenthal DR. Di-rect comparison of the BACTEC 9240 and BacT/ALERT 3D automatedblood culture systems for Candida growth detection. J Clin Microbiol2004; 42:115–8.
37. Riedel S, Eisinger SW, Dam L, Stamper PD, Carroll KC. Comparison ofBD Bactec Plus Aerobic/F medium to VersaTREK Redox 1 blood cul-ture medium for detection of Candida spp. in seeded blood culturespecimens containing therapeutic levels of antifungal agents. J Clin Mi-crobiol 2011; 49:1524–9.
38. Horvath LL, George BJ, Hospenthal DR. Detection of fifteen species ofCandida in an automated blood culture system. J Clin Microbiol 2007;45:3062–4.
39. Beyda ND, Alam MJ, Garey KW. Comparison of the T2Dx instrumentwith T2 Candida assay and automated blood culture in the detection ofCandida species using seeded blood samples. Diagn Microbiol InfectDis 2013; 77:324–6.
8 • CID • Mylonakis et al
at McM
aster University L
ibrary on January 27, 2015http://cid.oxfordjournals.org/
Dow
nloaded from