Embed Size (px)
Citation preview

FORENSIC ANATOMY OF SKELETON OF LIMBS

BONES OF THE UPPER LIMB
Humerus
• The humerus, the largest
bone in the upper limb.
• Articulates with the
scapula at the
glenohumeral joint and
the radius and ulna at the
elbow joint.
• It is composed of proximal
end, body (shaft )& distal
end.

• The proximal end of the humerus has a head,
surgical and anatomical necks, and greater and
lesser tubercles.
• Head- less than ½ sphere is directed medially,
upward &posteriorly and articulates with the
glenoid cavity of the scapula.
• The anatomical neck- a groove separates head
from the greater and lesser tubercles
• surgical neck- It is the narrow part distal to the
head and tubercles (common site of fracture).

• The junction of the head and neck with the shaft of the
humerus is indicated by the greater and lesser tubercles,
which provide attachment and leverage to some
scapulohumeral muscles.
• The intertubercular (bicipital) groove separates the tubercles
and provides passage for tendon of the long head of the
biceps muscle
• The shaft: upper ½ of the shaft is cylindrical while the lower
½ is like a prism.
• It has two prominent features:
the deltoid tuberosity for attachment of the deltoid
muscle.
the oblique radial groove groove for radial nerve

• The inferior end formed from
(from medial lateral)
medial epicondyle,
trochlea, capitulum&
lateral epicondyle.
• With 2 fossae anteriorly
(coronoid & radial)
one fossa posteriorly
(olecranon).

BONES OF FOREARM

Ulna
• The ulna is the stabilizing bone of the
forearm.
• It is the medial and longer of the two
forearm bones.
• Its proximal end - articulation with the
humerus.
• The ulna has two prominent
projections: the olecranon, which
projects proximally from its posterior
aspect (forming the point of the elbow)
• The coronoid process projects
anteriorly.
• Inferior to the coronoid process is the
tuberosity of the ulna attachment of
tendon of the brachialis muscle

• The shaft of the ulna is thick and cylindrical
proximally.
• It tapers, diminishing in diameter, as it continues
distally.
• At the narrow distal end of the ulna is a small but
abrupt enlargement, the disc-like head of the ulna
with a small, conical ulnar styloid process.

Radius
• The radius is the lateral and shorter of the
two forearm bone.
• It consist of thin narrow upper end ,body &
thick expanded lower end .

The upper end consist of :
• The head- it is disc like
with 2 articular surfaces :
• the upper surface
articulate with the
capitulum of the Humerus
.
• Lateral surface with the
radial notch of the ulna
• The neck - constricted
part below the head .
• The radial tuberosity -
below the medial part of
the neck .

• The shaft of the radius, in contrast to that of the
ulna, gradually enlarges as it passes distally.
• The distal end of the radius is essentially four sided
when sectioned transversely.
• Its medial aspect forms a concavity, the ulnar notch
which accommodates the head of the ulna.
• Its lateral aspect becomes increasingly ridge-like,
terminating distally in the radial styloid process.

BONES OF HAND
•The skeleton of the hand
is subdivided into three
segments-
•The carpus or wrist
bones
•The metacarpus or
bones of the palm
•The phalanges or bones
of the digits

THE CARPUS
• The carpal bones- eight in number
• They are arranged in two rows.
• Proximal row, from the radial ulnar
scaphoid, lunate, Triquetrum, and pisiform.
• Distal row, radial ulnar
Trapezium, trapezoid, capitate, and hamate.

SCAPHOID
• A boat-shaped bone
• Has a prominent scaphoid tubercle
• It is the largest bone in the proximal row of
carpals.
• articulates with five bones: the radius
proximally, trapezium and trapezoid distally,
and capitate and lunate medially.

LUNATE
• A moon-shaped bone between the scaphoid
and the triquetral bones.
• It is broader anteriorly than posteriorly.
• articulates with five bones: the radius
proximally, capitate and hamate distally,
Scaphoid laterally, and triquetral medially.

TRIQUETRUM
• A pyramidal bone on the medial side of the
carpus;
• Articulates with three bones: the lunate laterally,
the pisiform in front, the hamate distally; and
with the triangular articular disk which
separates it from the lower end of the ulna

Pisiform:
• A small, pea-shaped bone
• It lies on the palmar surface of the triquetrum.

Trapezium:
• A four-sided bone on the lateral side of the carpus.
• It articulates with the 1st and 2nd metacarpals,
scaphoid, and trapezoid bones.
Trapezoid:
• A wedge-shaped bone
• It resembles the trapezium.
• It articulates with the 2nd metacarpal, trapezium,
capitate, and scaphoid bones.

Capitate:
• A head-shaped bone with a rounded extremity
• The largest bone in the carpus.
• It articulates primarily with the 3rd metacarpal
distally and with the trapezoid, scaphoid, lunate,
and hamate.

Hamate:
• A wedge-shaped bone on the medial side of the hand.
• It articulates with the 4th and 5th metacarpal,
capitate, and triquetral bones.
• It has a distinctive hooked process, the hook of the
hamate, that extends anteriorly.

METACARPUS
• The metacarpus forms the skeleton of the palm
of the hand between the carpus and the
phalanges.
• It is composed of five metacarpal bones
(metacarpals).
• Each metacarpal consists of a base, shaft, and
head.
• The proximal bases of the metacarpals
articulate with the carpal bones, and the distal
heads of the metacarpals articulate with the
proximal phalanges and form the knuckles.

• The 1st metacarpal (of the
thumb) is the thickest and
shortest of these bones.
• The 3rd metacarpal is
distinguished by a styloid
process on the lateral side of
its base

PHALANGES
• Each phalanx has a base proximally, a shaft (body), and a
head distally.
• The proximal phalanges are the largest, the middle ones are
intermediate in size, and the distal ones are the smallest.
• The shafts of the phalanges taper distally.
• Each digit has three phalanges except for the first (the
thumb), which has only two
• The terminal phalanges are flattened and expanded at their
distal ends, which underlie the nail beds.
• The phalanges are convex on their dorsal and flat on their
volar surfaces.

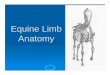
BONES OF LOWER LIMBThe femur
• The femur, or thigh bone is
the longest and heaviest
bone in the body.
• Its length varies from one
fourth to one third of that of
the body
• The femur is well covered
with muscles, so that only its
superior and inferior ends
are palpable.
• It is formed of upper end ,
shaft (body) & lower end.

THE UPPER END
• It consists of the head , the neck ,the greater
trochanter & the lesser trochanter .
• The round head of the femur makes up two thirds of
a sphere that is covered with articular cartilage,
except for a medially placed depression or pit, the
fovea for the ligament of the head.
• In early life, the ligament gives passage to an artery
supplying the epiphysis of the head

THE NECK
• It is trapezoidal,
• Its narrow end supporting the head and its
broader base is continuous with the shaft.
• Its average diameter is three quarters that of
the femoral head.
• The proximal femur is “bent” (L-shaped) so that
the long axis of the head and neck projects
superomedially at an angle to that of the
obliquely oriented shaft.
• The angle of inclination-helps to maintain
bipedal walking.

• Where the neck joins the femoral shaft are two large,
blunt elevations called trochanters.
• Lesser trochanter –
abrupt, conical and rounded
extends medially from the posteromedial part of the
junction of the neck and shaft.
• The greater trochanter –
large
laterally placed bony mass that projects superiorly
and posteriorly where the neck joins the femoral
shaft.

Shaft
• It is cylindrical in shape
• flattened posteriorly & downward.
• It is very slightly curved (convex) anteriorly.
• linea aspera -Along the middle of the shaft
posteriorly there is rough ridge
• The lateral lip of linea aspera superiorly join the
gluteal tuberosity which extends upward to the base
of greater trochanter.
• The medial lip of linea aspera passes above to form
the spiral line & ends in the intertrochanteric line.

The lower end of femur
• consist of two condyles.
• The medial and lateral femoral condyles
• The two condyles are on the same horizontal level when
the bone is in its anatomical position
• isolated femur is placed upright with both condyles
contacting the floor or tabletopthe femoral shaft will
assume the same oblique position it occupies in the
living body (about 9° from vertical in males and slightly
greater in females).
• The femoral condyles articulate with menisci (crescentic
plates of cartilage) and tibial condyles to form the knee
joint.

The Patella
• The patella is a flat & the largest sesamoid bone located in
the tendon of quadriceps femoris
• It is triangular in shape
• A base (upper border )
• An apex (rounded lower tip )
• 2 borders (medial & lateral)
• 2 surfaces (ant. & post.)
• The lower 1/3 of the posterior surface is rough
• The upper 2/3 is smooth. articular surface as it articulates
with the patellar surface of the femur.

THE BONES OF THE LEG
•The tibia and fibula are
the bones of the leg.
•The shafts of the tibia
and fibula are connected
by a dense interosseous
membrane

TIBIA
• Located on the antero-medial side of the leg.
• The proximal end widens to form medial and
lateral condyles
• Tibial plateau -This plateau consists of two smooth
articular surfaces.
• The medial one slightly concave and the lateral
one slightly convex.
• It articulate with the large condyles of the femur.
• The articular surfaces are separated by an
intercondylar eminence formed by two
intercondylar tubercles.

• The shaft of the tibia is vertical within the leg
• It is triangular in cross-section, having three surfaces and
borders: medial, lateral/interosseous, and posterior.
• The anterior border of the tibia is the most prominent border.
• It and the adjacent medial surface are subcutaneous “shin”.
• Their periosteal covering and overlying skin are vulnerable to
bruising.
• At the superior end of the anterior border, a broad, oblong
tibial tuberosity - distal attachment for the patellar ligament.
• On the posterior surface of the proximal part of the tibial
shaft is a rough diagonal ridge, called the soleal line, which
runs inferomedially to the medial border

• The distal end of the tibia is smaller than the
proximal end, flaring only medially.
• The medial expansion extends inferior to the
rest of the shaft as the medial malleolus.
• The inferior surface of the shaft and the
lateral surface of the medial malleolus
articulate with the talus and are covered with
articular cartilage.
• Helps in weight bearing.

FIBULA
• The slender fibula lies
posterolateral to the tibia
• It is firmly attached to Tibia
by the Tibio-fibular
syndesmosis.
• The fibula has no function in
weight-bearing.
• It serves mainly for muscle
attachment.

• The proximal end of the fibula consists of an
enlarged head superior to a small neck.
• The head has a pointed apex.
• The head of the fibula articulates with the fibular
facet on the posterolateral, inferior aspect of the
lateral tibial condyle.

• The shaft of the fibula is twisted
• It is marked by the sites of muscular
attachments.
• It is also important for the stability of the
ankle joint.
• It is triangular in cross-section
• It has three borders anterior, interosseous,
and posterior.
• Three surfaces medial, posterior, and
lateral.

• The distal end enlarges
• It is prolonged laterally and inferiorly as the
lateral malleolus.
• The lateral malleolus is more prominent and
posterior than the medial malleolus and
extends approximately 1 cm more distally.

BONES OF FOOT
• The bones of the foot include The Tarsus,
Metatarsus, and Phalanges.
7 tarsal bones,
5 metatarsal bones
14 phalanges


THE TARSUS
• Consists of seven bones
• talus, calcaneus, cuboid, navicular, and
three cuneiforms.
• Only one bone, the talus, articulates with
the leg bones.

THE CALCANEUS• It is the largest and strongest bone in the foot.
• When standing, the calcaneus transmits the majority of the
body's weight from the talus to the ground.
• The anterior two thirds of the calcaneus's superior surface
articulates with the talus and its anterior surface
articulates with the cuboid.
• The posterior part of the calcaneus has a massive, weight-
bearing prominence, the calcaneal tuberosity, which has
medial, lateral, and anterior tubercles.
• Only the medial tubercle contacts the ground during
standing.

Talus
• The talus has a body, neck, and head.
• The superior surface, or trochlea of the talus, is gripped by the two
malleoli.
• It receives the weight of the body from the tibia. The talus
transmits that weight in turn, dividing it between the calcaneus,
on which the body of talus rests, and the forefoot, via an
osseoligamentous “hammock”.
• Most of its surface is covered with articular cartilage.
• The talar body bears the trochlea superiorly and narrows into a
posterior process that features a groove
• This groove is for the tendon of the flexor hallucis longus, flanked
by a prominent lateral tubercle and a less prominent medial
tubercle.

The Navicular
• It is a flattened, boat-shaped bone.
• It is located between the head of the talus
posteriorly and the three cuneiforms anteriorly.
• The medial surface of the navicular projects
inferiorly to form the navicular tuberosity.
• It is an important site for tendon attachment
• It forms a longitudinal arch of the foot, which must
be supported centrally.
• If this tuberosity is too prominent, it may press
against the medial part of the shoe and cause foot
pain.

The Cuboid
• Cuboid is approximately cubical in shape.
• It is the most lateral bone in the distal row of the
tarsus.
• It lies between the calcaneus and the lateral 2
metatarsals.

Cuneiform bones
• The three cuneiform bones are the medial (1st),
intermediate (2nd), and lateral (3rd).
• The medial cuneiform is the largest bone.
• The intermediate cuneiform is the smallest.
• Each cuneiform articulates with the navicular
posteriorly and the base of its appropriate
metatarsal anteriorly.
• The lateral cuneiform articulates with the cuboid.

Metatarsus
• Consists of five metatarsals that are numbered from the
medial side of the foot.
• The 1st metatarsal is shorter and stouter than the
others.
• The 2nd metatarsal is the longest.
• Each metatarsal has a base proximally, a shaft, and a
head distally.
• The base of each metatarsal is the larger, proximal end.
• The bases of the metatarsals articulate with the
cuneiform and cuboid bones, and the heads articulate
with the proximal phalanges.

Phalanges
• The 14 phalanges are as follows-
the 1st digit (great toe) has 2 phalanges (proximal
and distal).
the other four digits have 3 phalanges each:
proximal, middle, and distal.
• Each phalanx has a base (proximally), a shaft, and a
head (distally).
• The phalanges of the 1st digit are short, broad, and
strong.
• The middle and distal phalanges of the 5th digit may
be fused in elderly people

MEDICO-LEGAL IMPORTANCE OF BONES OF LIMBS.
• Identification- age, sex, race, stature, and
specific identification factors
• Time since death
• Trauma analysis

AGE
• the appearance and union of epiphyses and
other ossification centers,
• Remodeling,
• Bone Loss,
• Arthritic Changes,
• Shifts in chemical composition

OSSIFICATION CENTER APPEARANCE AND EPIPHYSEAL
UNION
• appearance and
union of
ossification centres
are used to
estimate age
during
development and
growth from the
immature to adult
stage.

BONE REMODELING-
• Kerley histological technique
• Circular fields located adjacent to the periosteal
edge of the bone on its anterior, posterior, medial,
and lateral surfaces are measured.
• the numbers of primary osteons, secondary osteons,
and osteon fragments must be counted
• with increasing age, the percentage of
circumferential lamellar bone and the number of
primary osteons decrease while the number of
secondary osteons and osteon fragments increases

RADIOLOGICAL METHOD (BONE LOSS)
• Bone density observed on
radiographs to assess bone loss
with age and disease.
• height of the apex of the
medullary cavity, structure of
trabecular bone, cavity
formation in the major
tubercles, and the thinning of
the cortex are observed.

• Arthritic Changes
• General changes associated with arthritis provide an
additional source of age information from bones
• Generalized changes provide clues to advancing age,
but pathological conditions can produce such evidence
prematurely or with varied expressions in different
anatomical areas.
• Chemical Changes
• Racemization is a chemical reaction whereby the L-
forms of amino acids change to D-forms, and this
change correlates highly with the age of the protein. D-
L ratio increases with the age.

SEXThere are two methodological approaches to
sexing in adults:
• Morphological- focus on shape, the bony
configurations that are macroscopically
visible.
• Metric – based on bone dimensions

Morphological differences between
male (left) and female (right)
humerus:
(a) trochlear constriction: less
pinched in males, more pinched in
females;
(b) trochlear symmetry: assymetrical
in males, symmetrical in females;
(c) olecranon fossa shape: triangular
in males, oval in females;
(d) angle of medial epicondyle:
horizontal in males, angled in females

• Femur
• the vertical diameter of head is greater than
45 mm in the male and less than 41 mm in
the female,
• angle that the shaft makes with the
vertical- 76deg in females and 80 deg in
males
• collodiaphyseal angle- < 40 deg in males and
>50 deg in females

STATURE
• The most common method used- linear regression.
• With this technique, the known statures of adults in a given
population are plotted against the lengths of skeletal elements
and the best lines are fitted to the scatter plots
• Various regression formulae for calculating height have been
compiled, based on a number of different populations and sex.
• Karl pearson’s formula: a constant factor is to be added to the
product of the length of the bone with the multiplying factor
• femur- (Males) 81.306 +1.880 x length of femur,
(F)72.884+1.945 x length
• Tibia – (M)78.664 + 2.376 x length, (F) 74.774 +2.352 X length
• Humerus – 70.641+2.891 x length, (F)71.745+ 2.754 x length

• Trotter and Gleser formula- Different formulae were
calculated for the three major race types (white, negro
and mongoloid) and extensievely used.
• As such, these formulae cannot be satisfactorily used
on all populations and people from different regions
bear different morphology.
• Some of different formulae available for different
parts of india are
• Pan’s formula- Bihar Bengal and Orissa
• Nat’s formula – UP
• Siddiqui and Shah’s formula- Punjab

STATURE FROM FRAGMENT OF LONG BONES
• The most common approach is to use a
fragment of a long bone to estimate its
total length and then to employ this in
an existing formula.
• Alternatively, the length of the
fragment can be used directly to
estimate stature.
• They defined a number of landmarks
establishing few segments in the bones
like 4 in femur, five in the tibia, and
four in the humerus. Each segment is
defined as the distance between two
consecutively numbered points

RACE
• with respect to ancestry, postcranial
differences are largely nonexistent
• However Differences in the anterior
curvature of the diaphysis of femur can be
assessed for race determination.

PERSONAL IDENTITY
• Discrete abnormalities such as healing
fractures, metal prostheses, bone disease or
congenital defects. Some artefacts, such as
drill holes or wire can be used in
identification.

TIME SINCE DEATH
Based on physical appearance
• If soft tissues are still attached : 2weeks to 2
months
• No soft tissue but greasy : 1-3months
• Completely dry but foul smell : 3months to 1 year
• After 1yr unpreserved bones get destroyed

• Physical tests: silvery-blue fluorescence in
ultraviolet light
• From 3 to 80 years, greatly depending upon the
environmental conditions, the outer zone and
the zone around the marrow cavity
progressively lose fluorescence
• After a century or more, the residual
fluorescence contracts to a narrowing central
sandwich
• By second century fluorescence completely
vanishes

• Chemical tests: diminishing of amino acids
• Radio nucleotide method: radiocarbon (C-14)
analysis (this method is, however, insufficient for a
PMI of less than 100 years)
• strontium-90 and plutonium is used for shorter
PMI.

CAUSE OF DEATH
• It can be made out if there are fractures or
marks of deep cuts in bones, or marks of
burns or evidence of firearm injuries or any
disease. Metallic poisons can be found in
bones long after death.

NATURE OF INJURY• identification of the skeletal defects and establishment of
the timing of injury into ante-mortem peri-mortem and
postmortem
• Antemortem injury- signs of healing like grooves around
the fracture, active bone remodeling, callus formation,
and edge resorption are seen
• Perimortem injury- no evidence of healing on the bone.
characterized by a “green bone response” where the
collagen fibres in living bone allow some bending or
bowing to take place
• Postmortem injury- Transverse fractures and right-
angled edges