Embed Size (px)
Citation preview
LOWER LIMBLEARNING OBJECTIVE:Hip Bone: Ilium: identify - iliac crest, articular surface (for sacrum); Ischium: identify - ischial tuberosity; Pubis: identify - articular surface of symphysis pubis;Coxal bone: identify- acetabulum, obturator foramen.Femur: identify - head, neck, greater trochanter, lesser trochanter, medial condyle, lateral condyle, intercondylar fossa.Patella: know the general featuresTibia: identify - lateral condyle, medial condyle, tibial tuberosity, medial malleolus.Fibula: identify - head, lateral malleolus.Foot: identify - tarsals, metatarsals, & phalanges as groups; talus, calcaneus.Identify right from left: Hip bone femur, Patella, tibia, fibula, foot.Fracture and complications: Anatomical factors related to the fracture
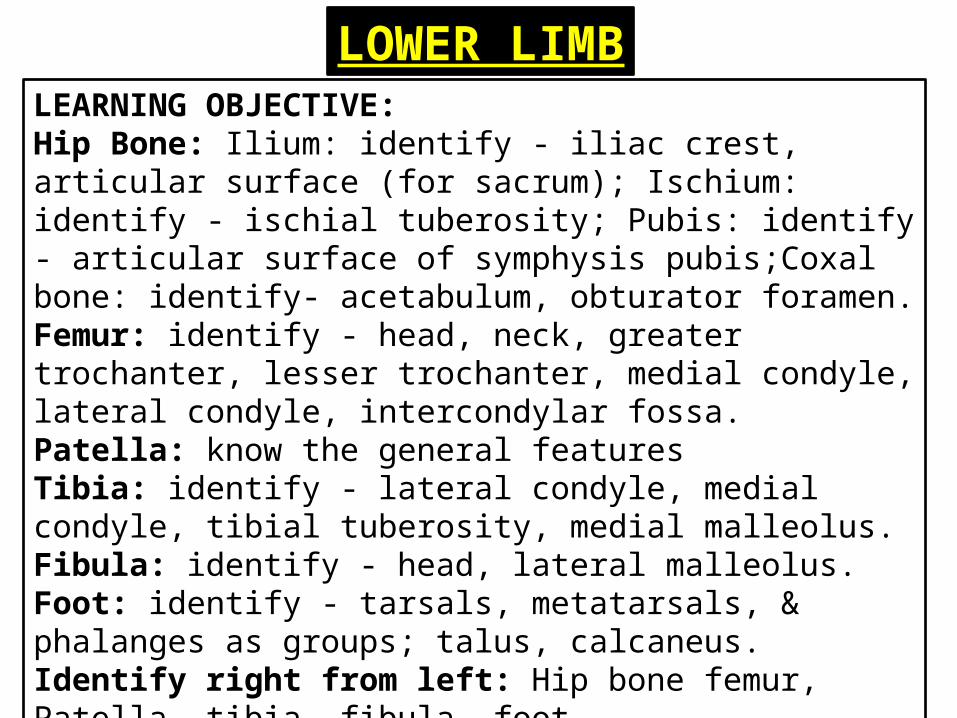
Bones of the Lower LimbDivided into two functional components:
The Pelvic Girdle
The bones of the Free Lower Limb .
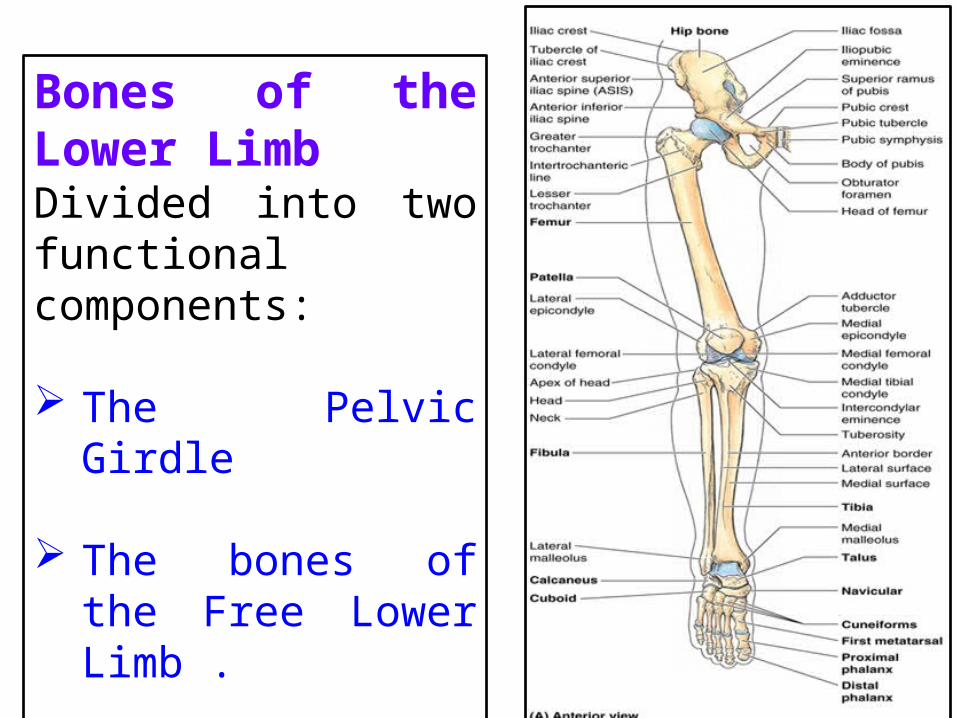
Bones of the Lower LimbPelvic girdle: composed of the sacrum and right and left hip bones joined anteriorly at the pubic symphysis.
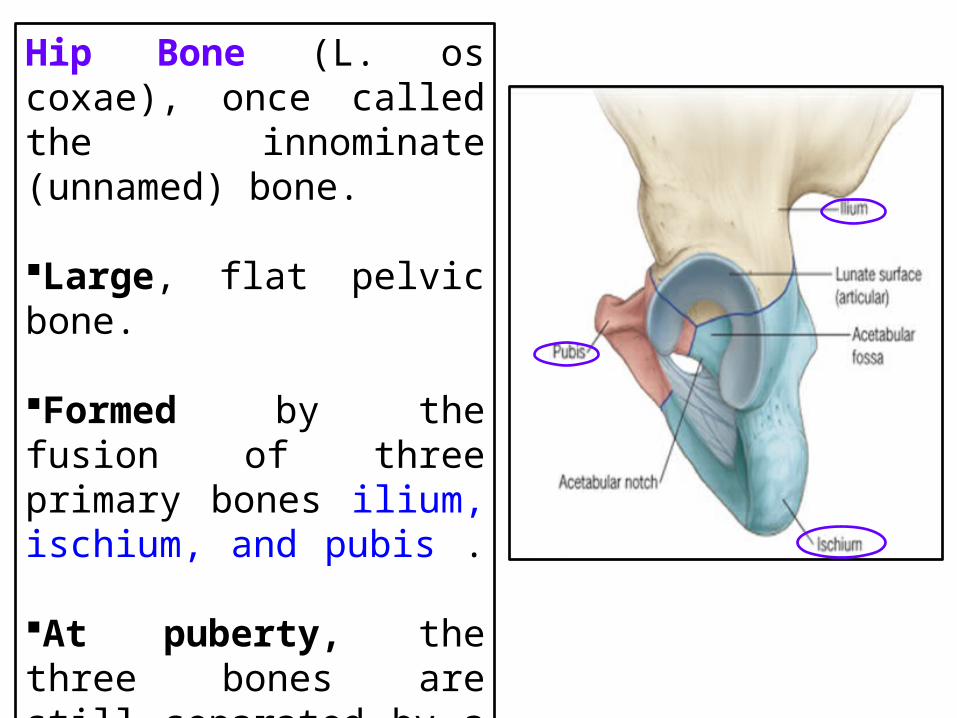
Hip Bone (L. os coxae), once called the innominate (unnamed) bone.
Large, flat pelvic bone.
Formed by the fusion of three primary bones ilium, ischium, and pubis .
At puberty, the three bones are still separated by a Y-shaped triradiate cartilage centered in the acetabulum.
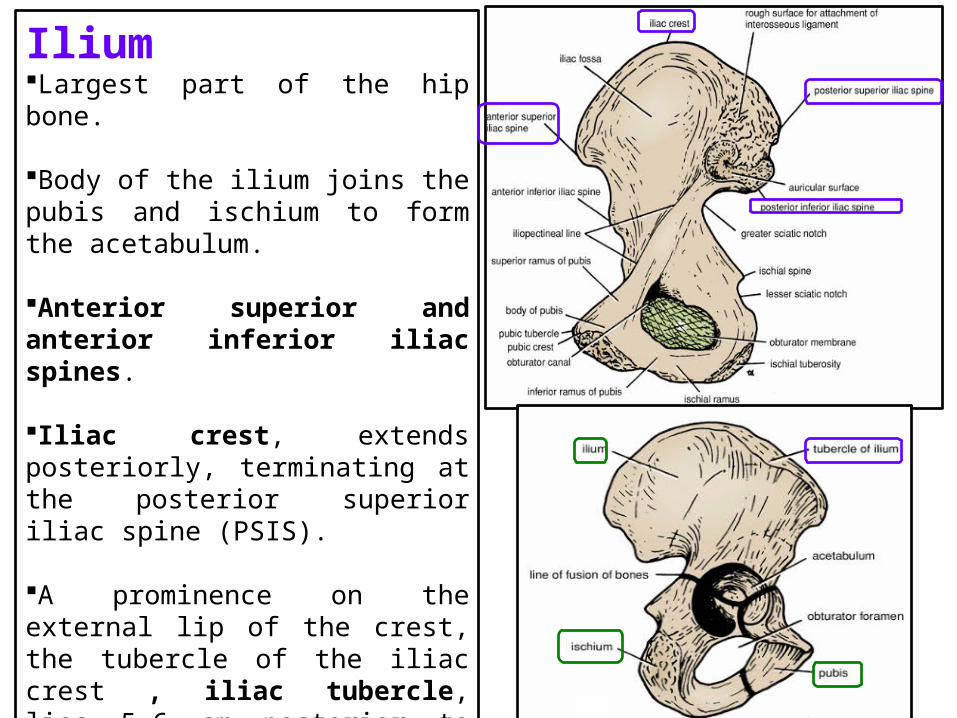
IliumLargest part of the hip bone.
Body of the ilium joins the pubis and ischium to form the acetabulum.
Anterior superior and anterior inferior iliac spines.
Iliac crest, extends posteriorly, terminating at the posterior superior iliac spine (PSIS).
A prominence on the external lip of the crest, the tubercle of the iliac crest , iliac tubercle, lies 5-6 cm posterior to the ASIS.
Posterior inferior iliac spine marks the superior end of the greater sciatic notch.
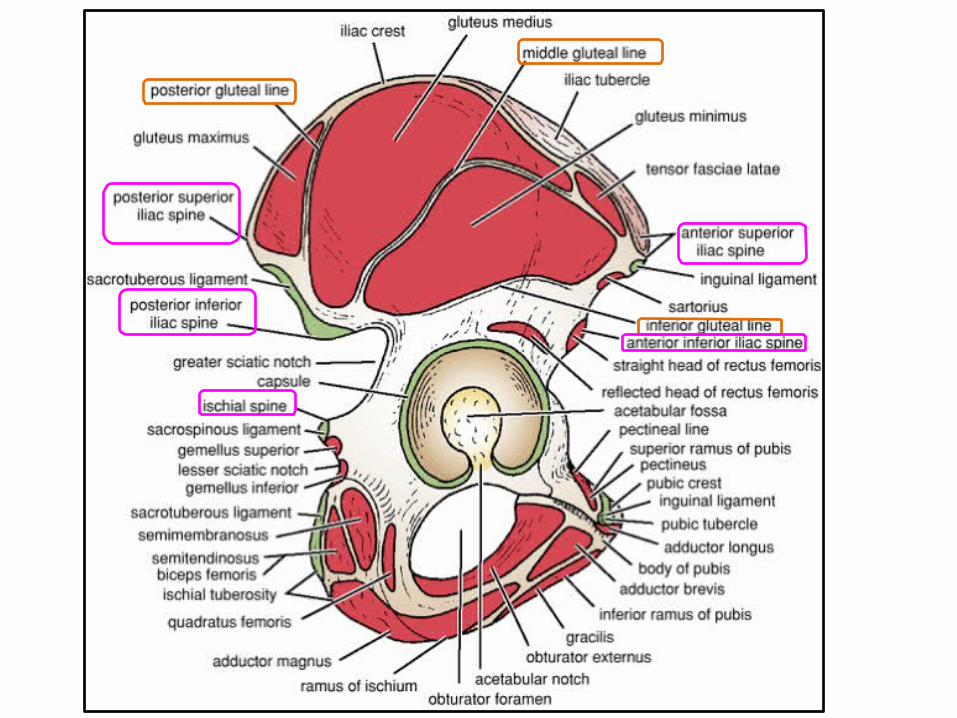
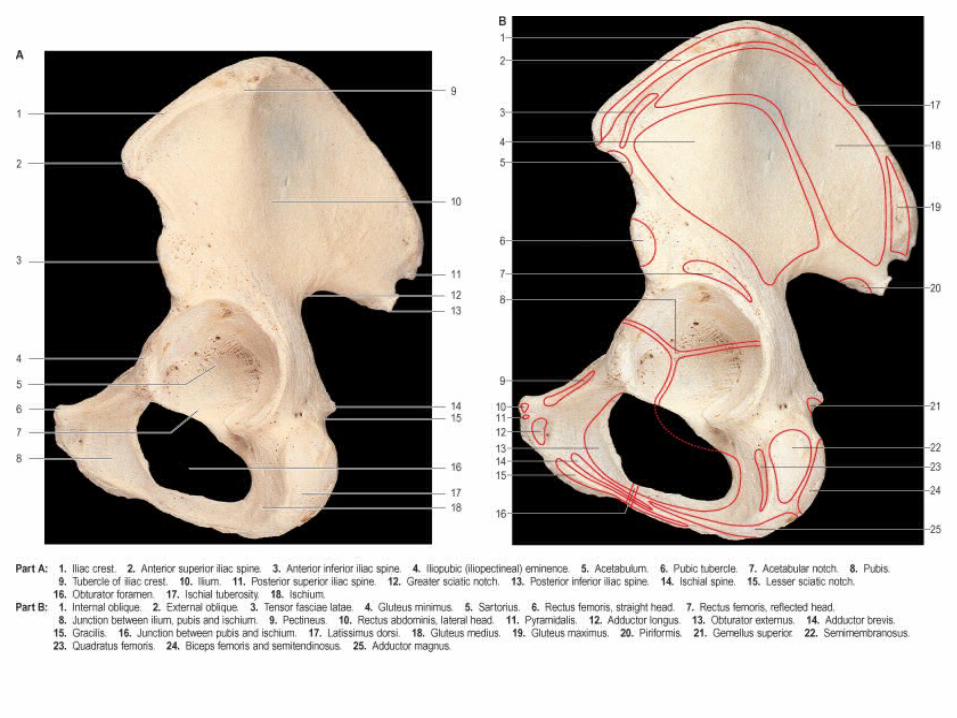
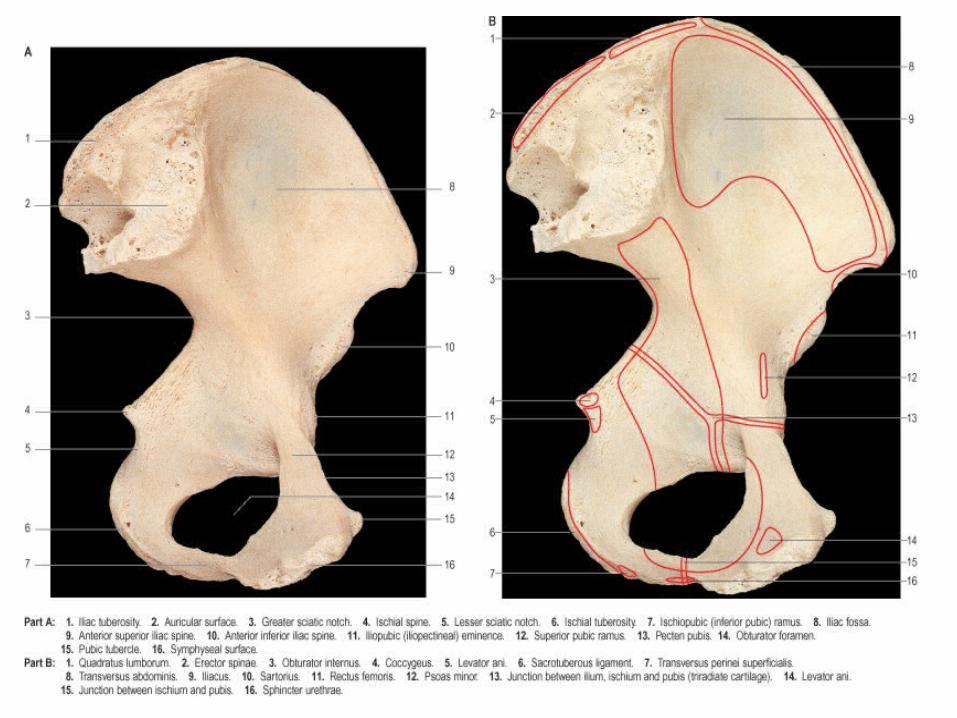
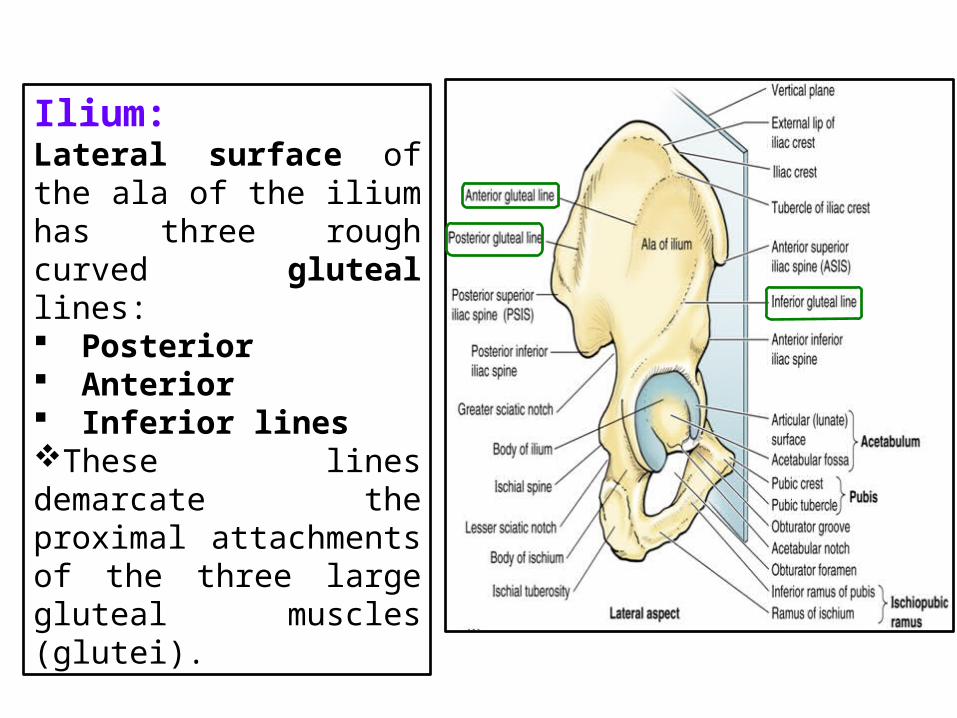
Ilium:Lateral surface of the ala of the ilium has three rough curved gluteal lines: Posterior Anterior Inferior lines These lines demarcate the proximal attachments of the three large gluteal muscles (glutei).
Ilium:
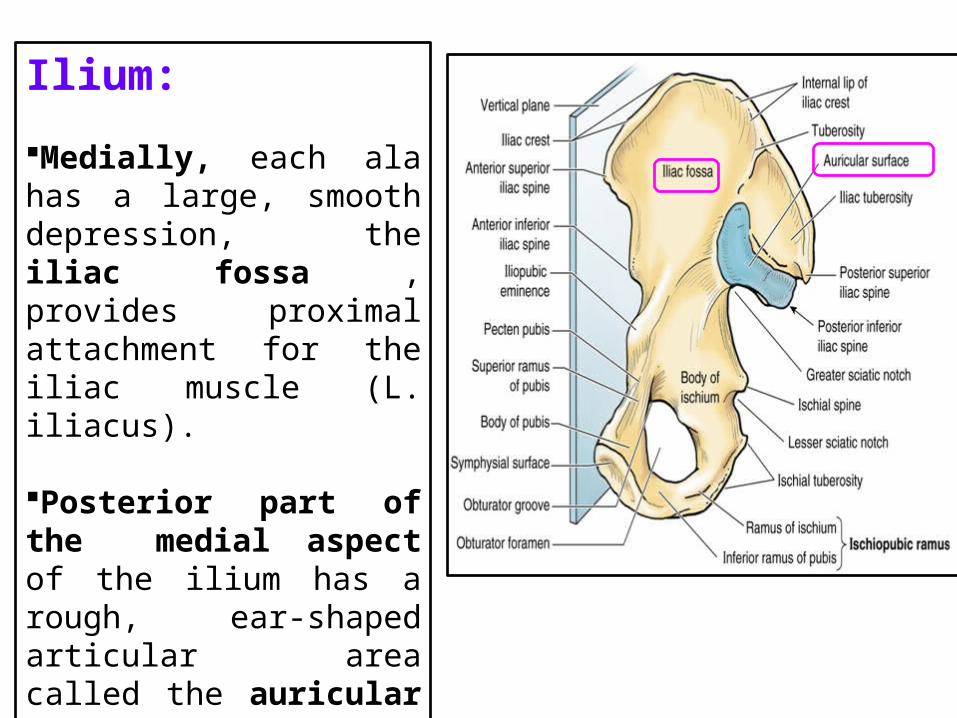
Medially, each ala has a large, smooth depression, the iliac fossa , provides proximal attachment for the iliac muscle (L. iliacus).
Posterior part of the medial aspect of the ilium has a rough, ear-shaped articular area called the auricular surface.
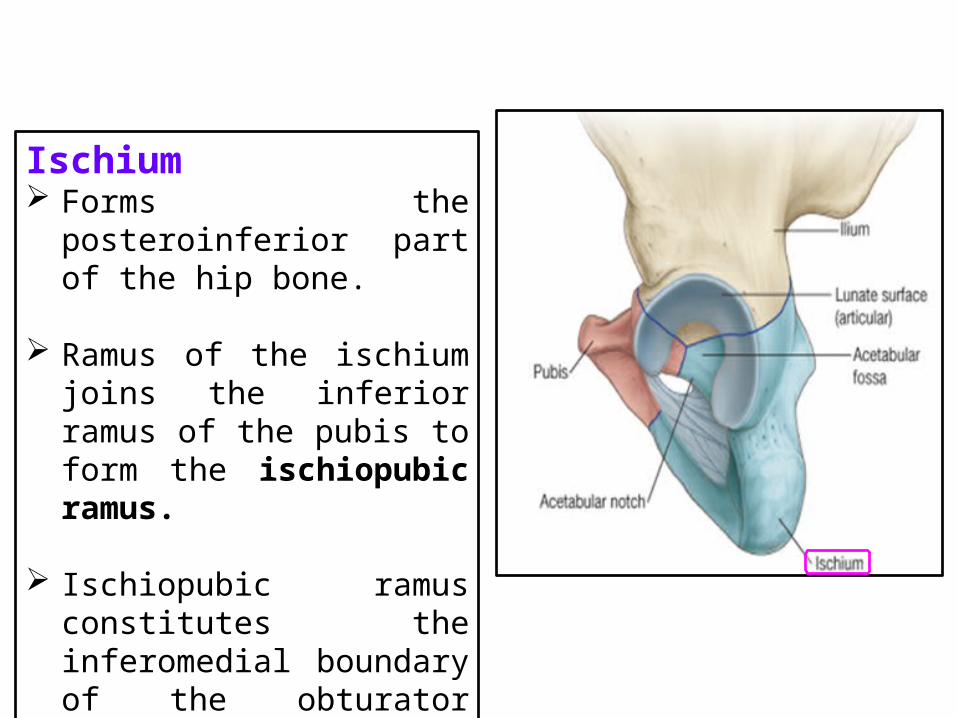
Ischium Forms the posteroinferior part
of the hip bone.
Ramus of the ischium joins the inferior ramus of the pubis to form the ischiopubic ramus.
Ischiopubic ramus constitutes the inferomedial boundary of the obturator foramen.
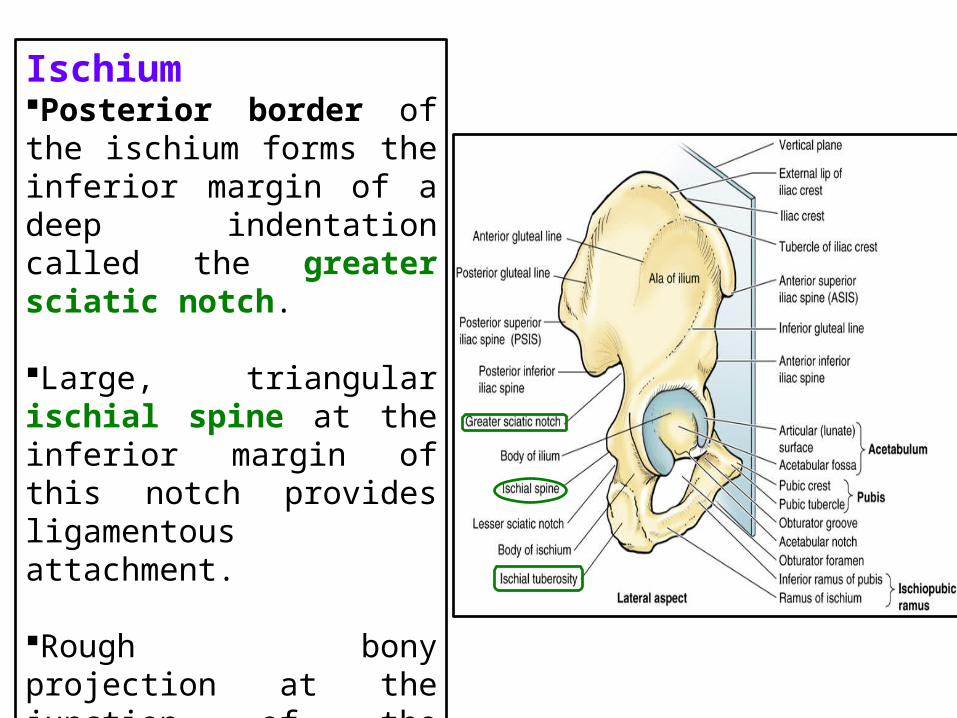
IschiumPosterior border of the ischium forms the inferior margin of a deep indentation called the greater sciatic notch.
Large, triangular ischial spine at the inferior margin of this notch provides ligamentous attachment.
Rough bony projection at the junction of the inferior end of the body of the ischium and its ramus is the large ischial tuberosity.
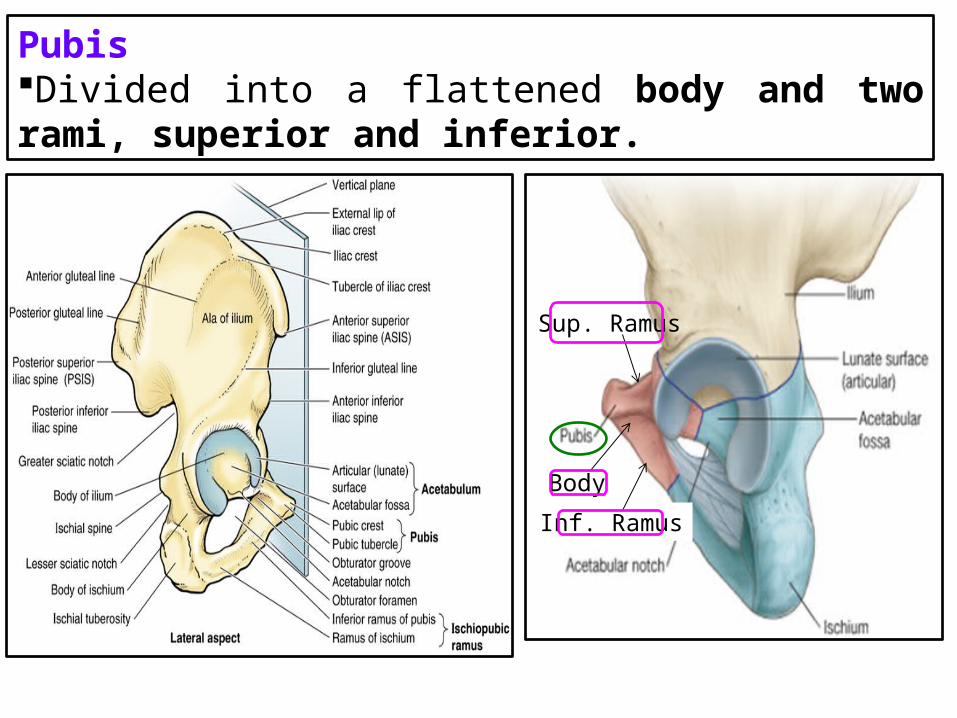
PubisDivided into a flattened body and two rami, superior and inferior.
Sup. Ramus
Inf. Ramus
Body
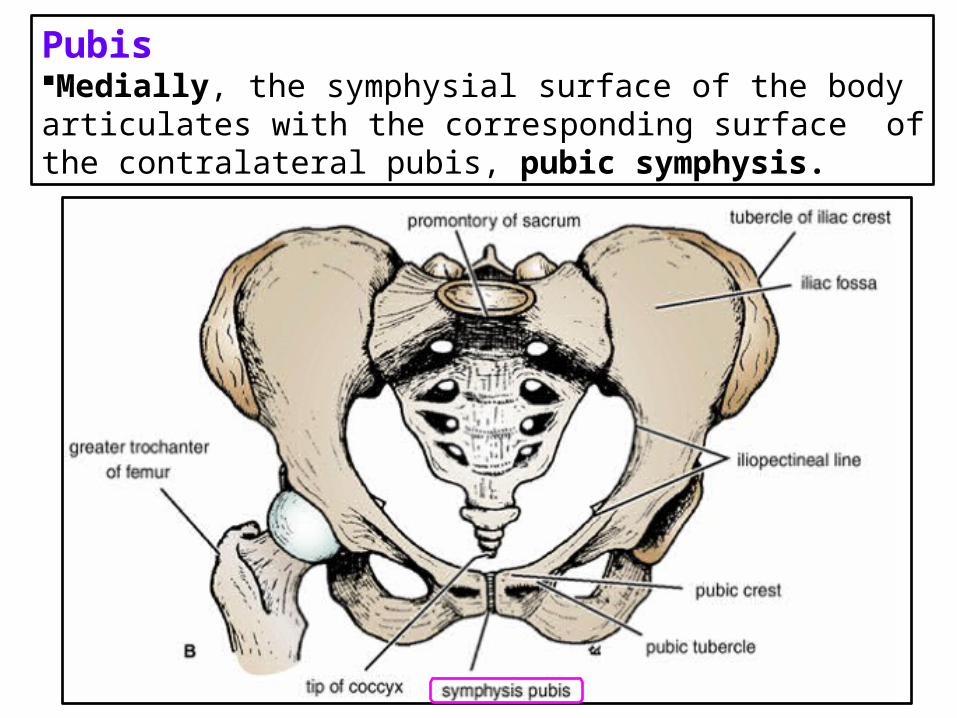
PubisMedially, the symphysial surface of the body articulates with the corresponding surface of the contralateral pubis, pubic symphysis.
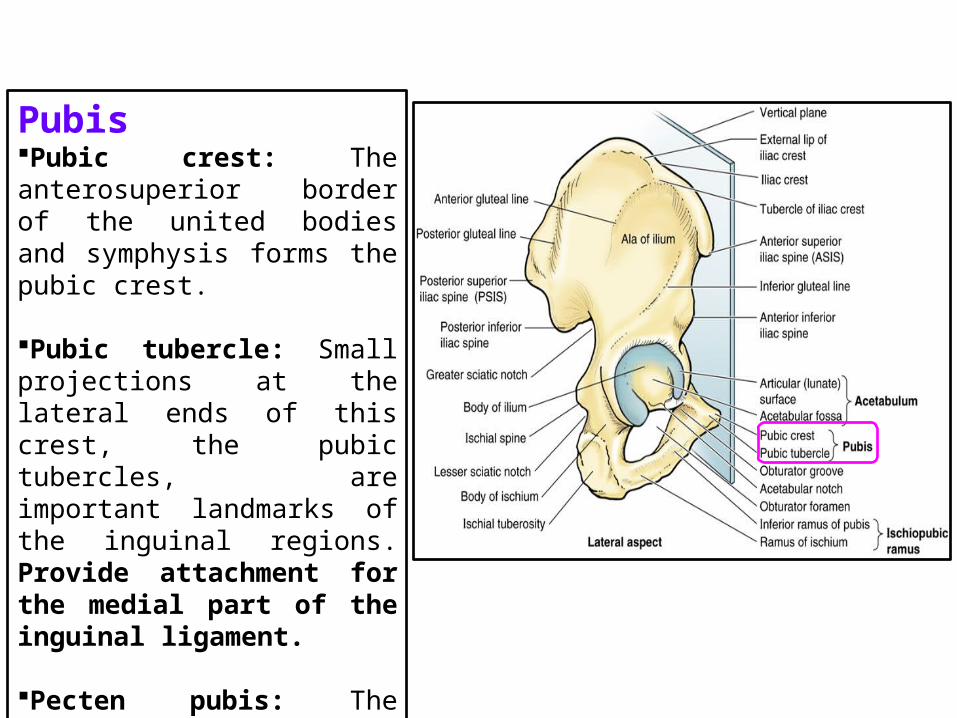
PubisPubic crest: The anterosuperior border of the united bodies and symphysis forms the pubic crest.
Pubic tubercle: Small projections at the lateral ends of this crest, the pubic tubercles, are important landmarks of the inguinal regions. Provide attachment for the medial part of the inguinal ligament.
Pecten pubis: The posterior margin of the superior ramus of the pubis has a sharp raised edge, the pecten pubis.
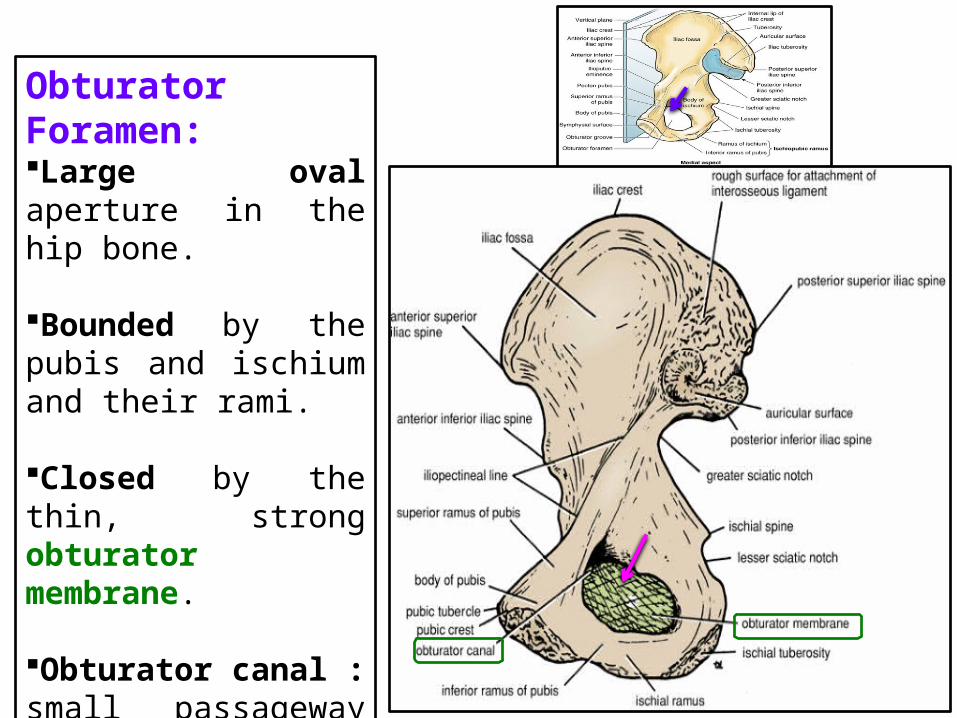
Obturator Foramen:Large oval aperture in the hip bone.
Bounded by the pubis and ischium and their rami.
Closed by the thin, strong obturator membrane.
Obturator canal : small passageway for the obturator nerve and vessels.
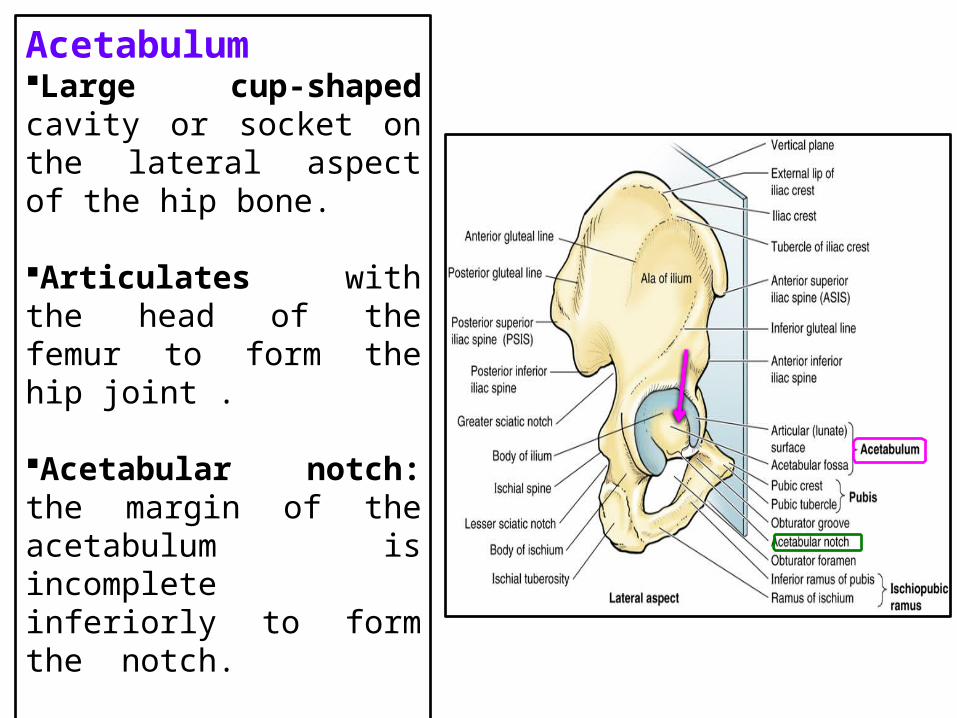
AcetabulumLarge cup-shaped cavity or socket on the lateral aspect of the hip bone.
Articulates with the head of the femur to form the hip joint .
Acetabular notch: the margin of the acetabulum is incomplete inferiorly to form the notch.
Acetabular fossa: a rough depression in the floor of the acetabulum.
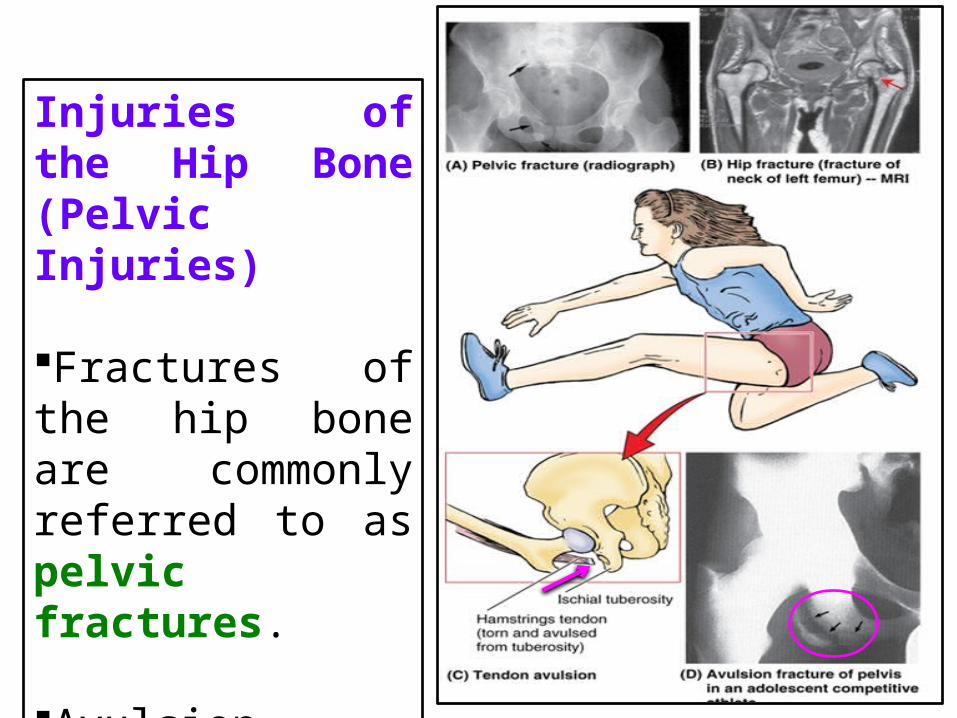
Injuries of the Hip Bone (Pelvic Injuries)
Fractures of the hip bone are commonly referred to as pelvic fractures.
Avulsion fractures of the hip bone may occur during sports.
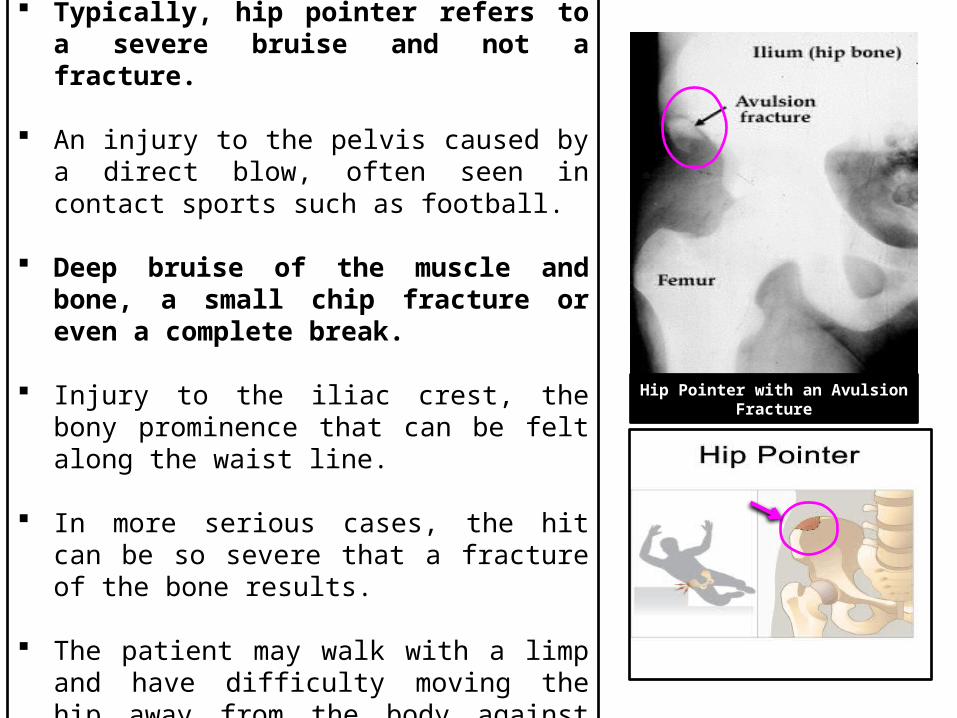
Hip Pointer Typically, hip pointer refers to a severe
bruise and not a fracture.
An injury to the pelvis caused by a direct blow, often seen in contact sports such as football.
Deep bruise of the muscle and bone, a small chip fracture or even a complete break.
Injury to the iliac crest, the bony prominence that can be felt along the waist line.
In more serious cases, the hit can be so severe that a fracture of the bone results.
The patient may walk with a limp and have difficulty moving the hip away from the body against resistance.
Hip Pointer with an Avulsion Fracture
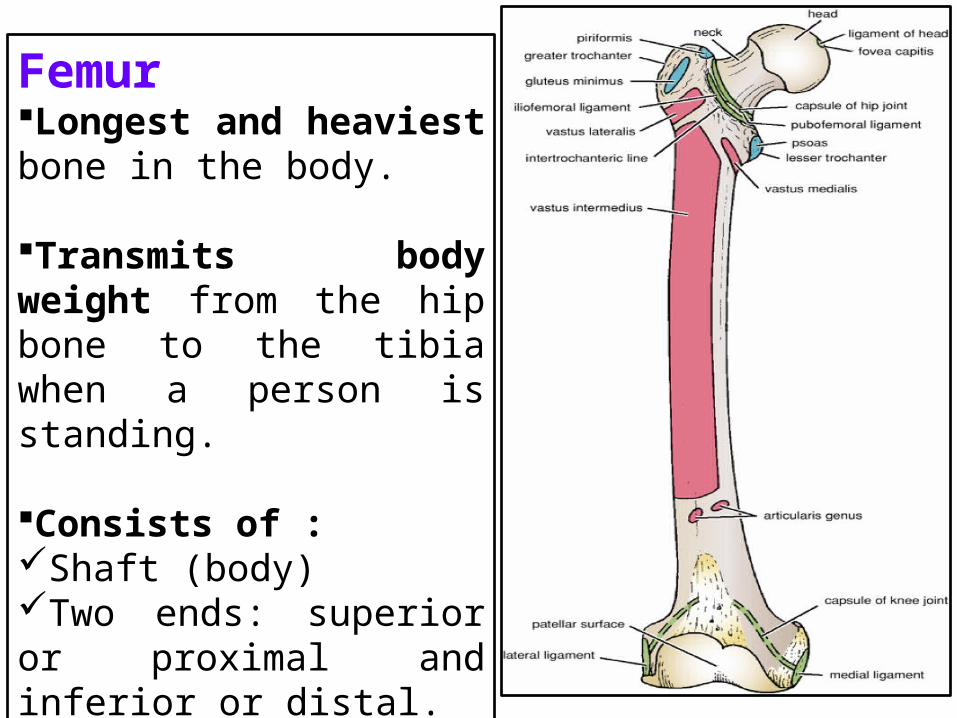
FemurLongest and heaviest bone in the body.
Transmits body weight from the hip bone to the tibia when a person is standing.
Consists of :Shaft (body)Two ends: superior or proximal and inferior or distal.
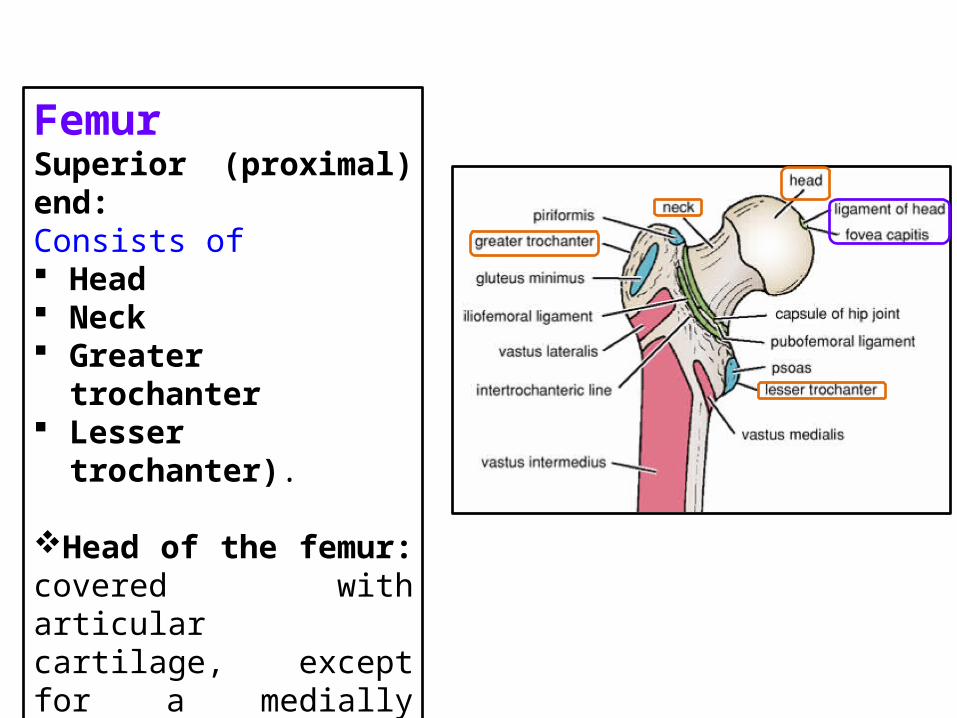
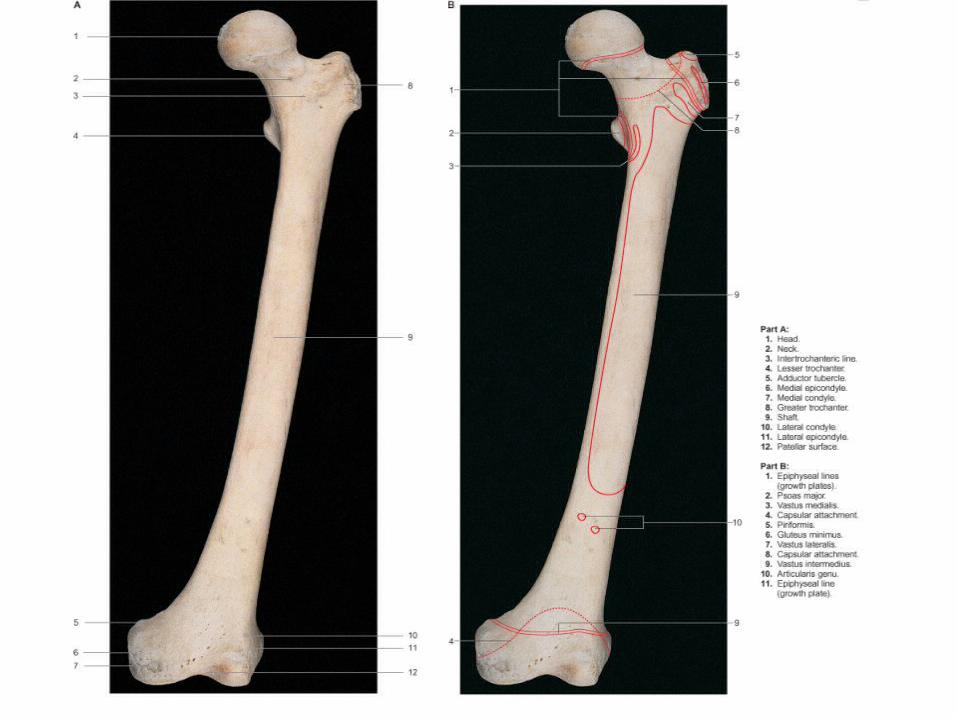
FemurSuperior (proximal) end:Consists of Head Neck Greater trochanter Lesser trochanter).
Head of the femur: covered with articular cartilage, except for a medially placed depression or pit, the fovea for the ligament of the head.
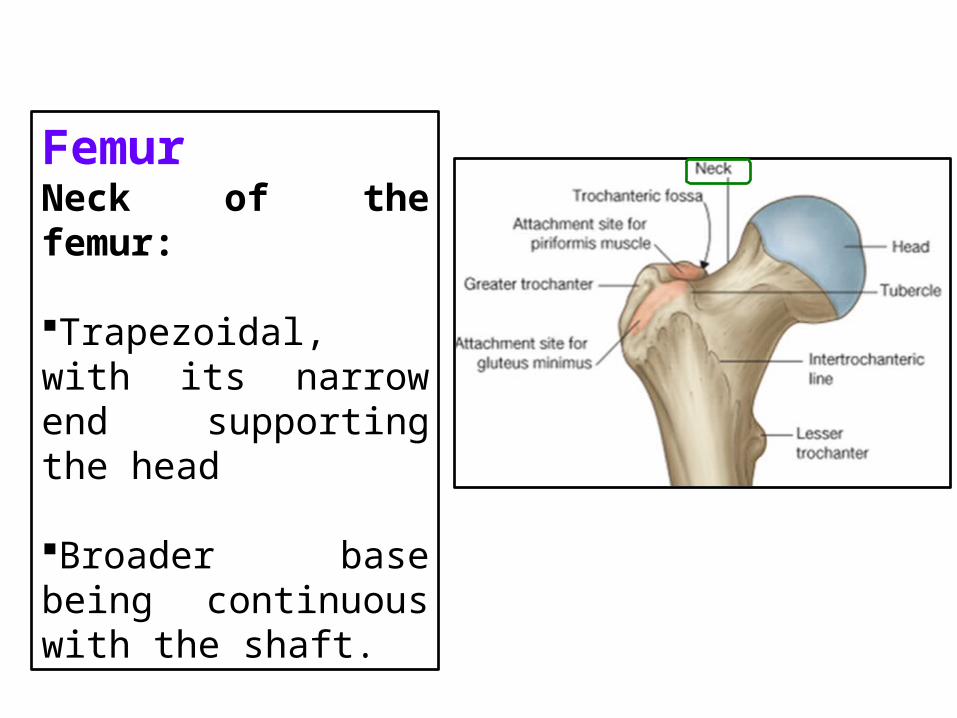
FemurNeck of the femur:
Trapezoidal, with its narrow end supporting the head
Broader base being continuous with the shaft.
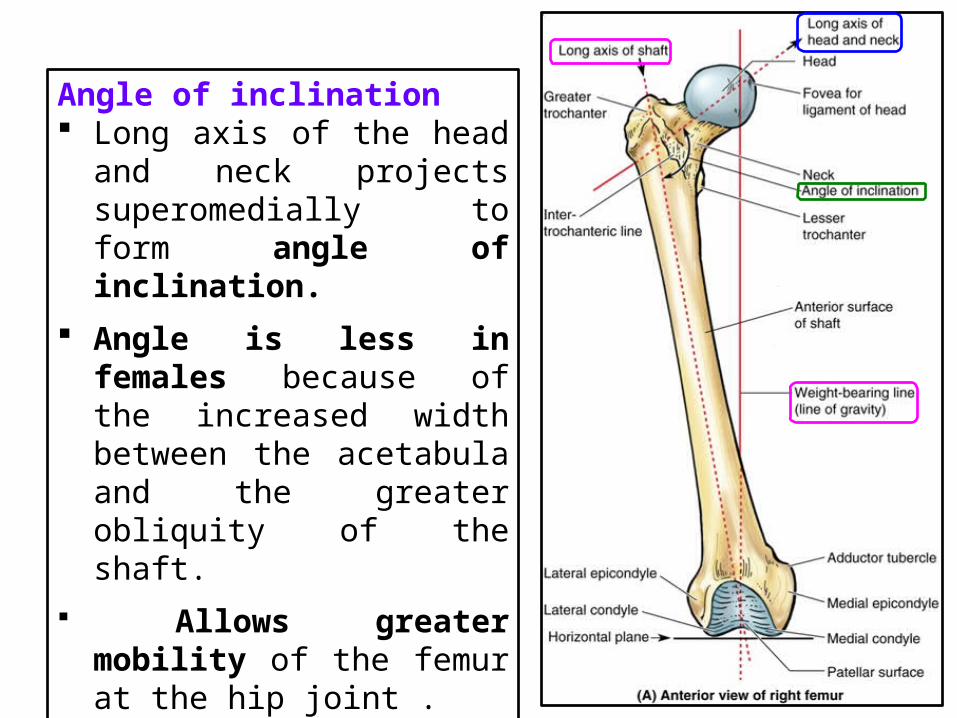
Angle of inclination Long axis of the head and neck
projects superomedially to form angle of inclination.
Angle is less in females because of the increased width between the acetabula and the greater obliquity of the shaft.
Allows greater mobility of the femur at the hip joint .
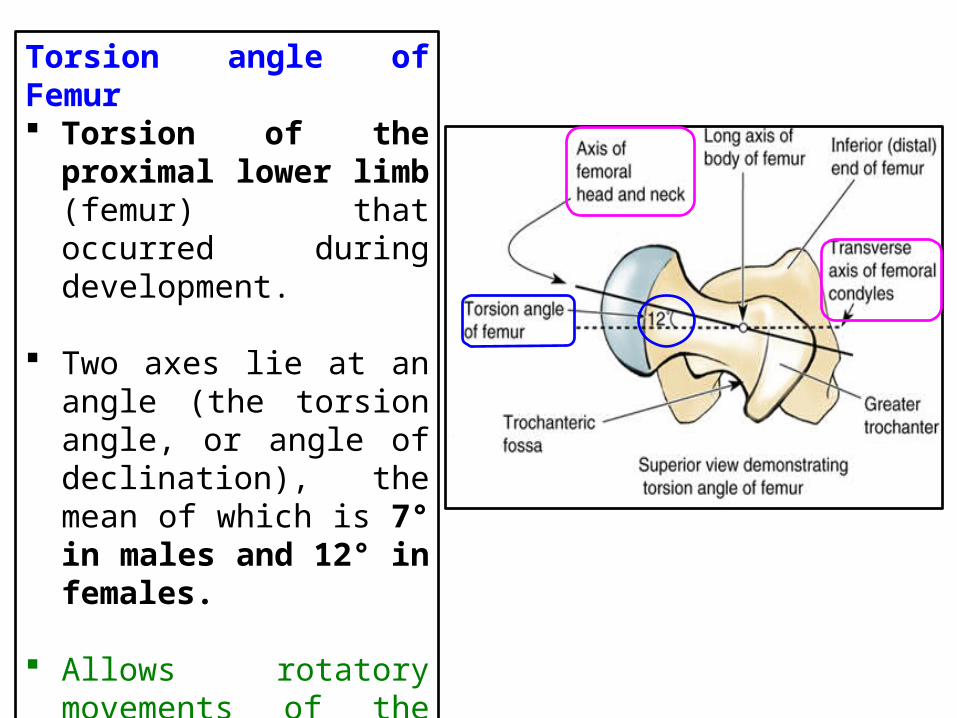
Torsion angle of Femur Torsion of the proximal
lower limb (femur) that occurred during development.
Two axes lie at an angle (the torsion angle, or angle of declination), the mean of which is 7° in males and 12° in females.
Allows rotatory movements of the femoral head.
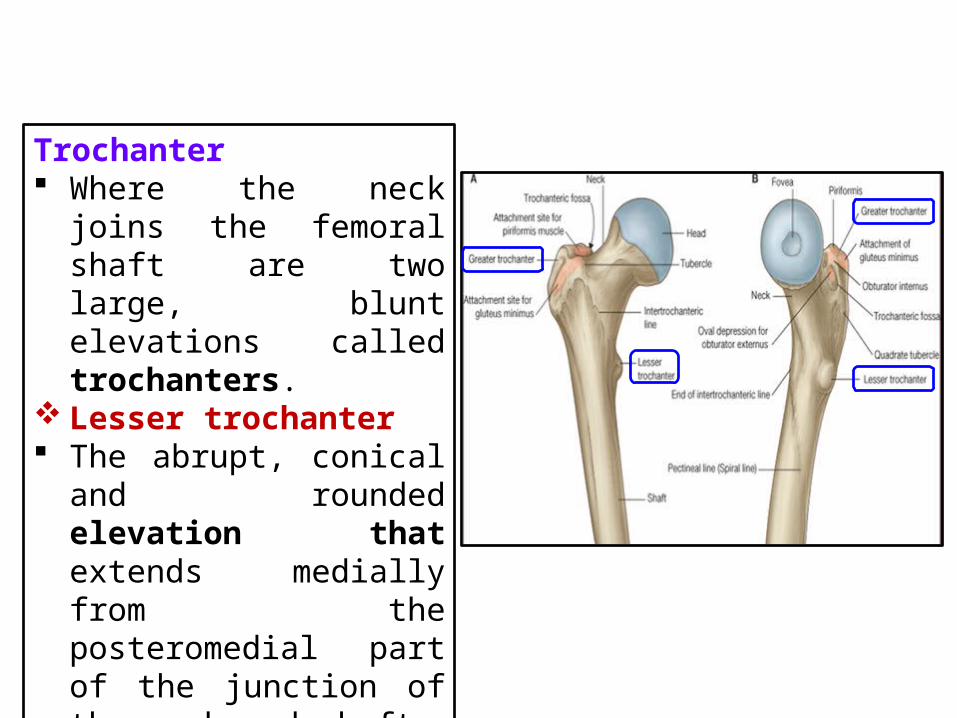
Trochanter Where the neck joins the
femoral shaft are two large, blunt elevations called trochanters.
Lesser trochanter The abrupt, conical and
rounded elevation that extends medially from the posteromedial part of the junction of the neck and shaft.
Attachment of the iliopsoas.
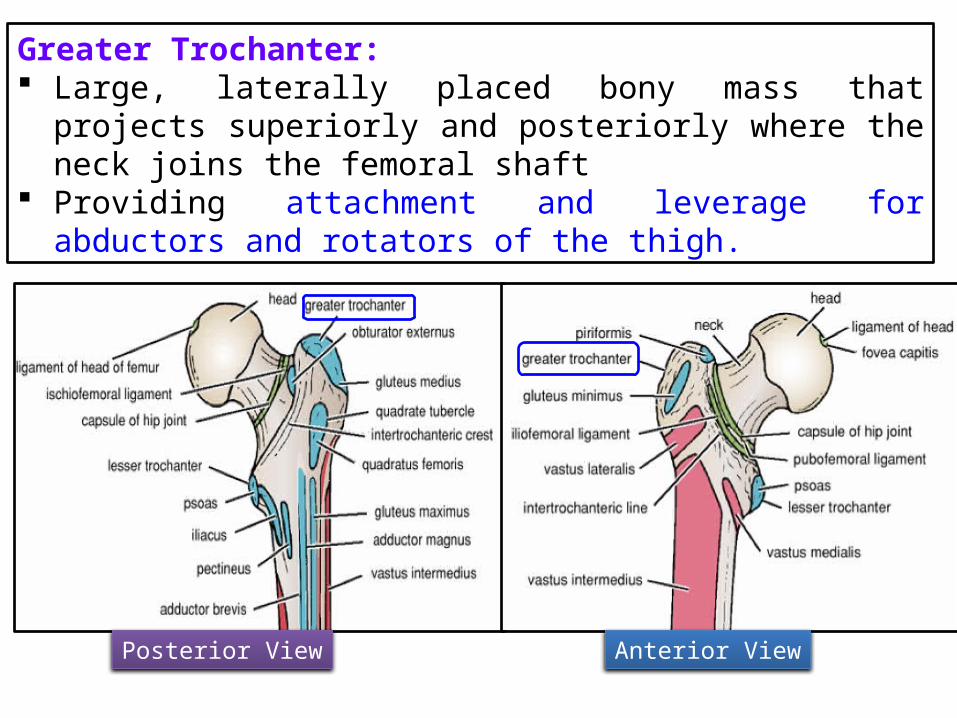
Greater Trochanter: Large, laterally placed bony mass that projects superiorly and
posteriorly where the neck joins the femoral shaft Providing attachment and leverage for abductors and rotators of
the thigh.
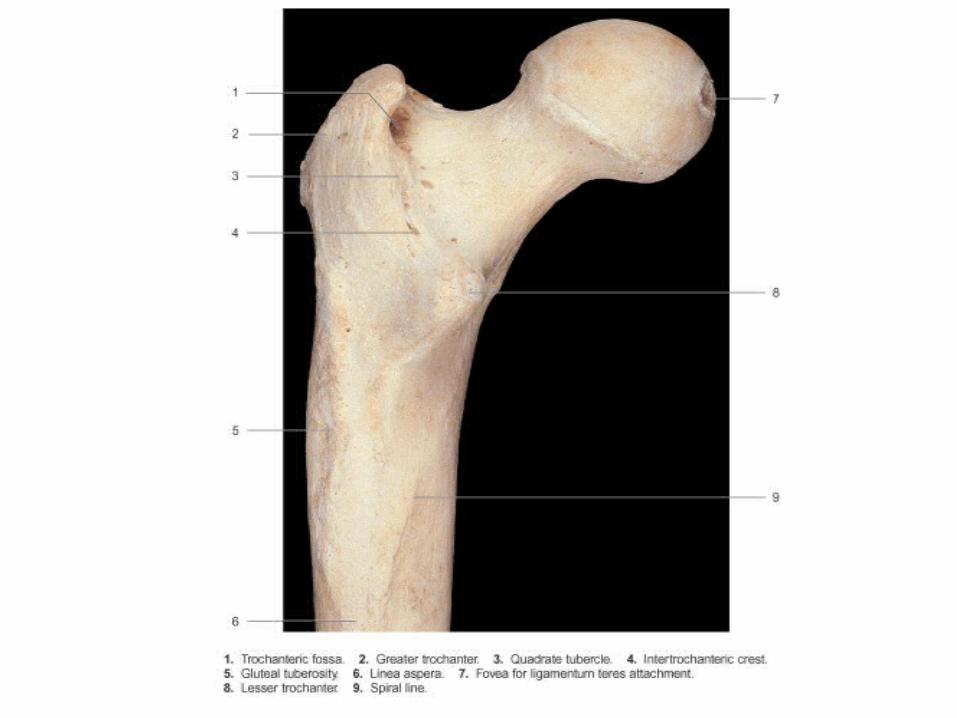
Anterior ViewPosterior View
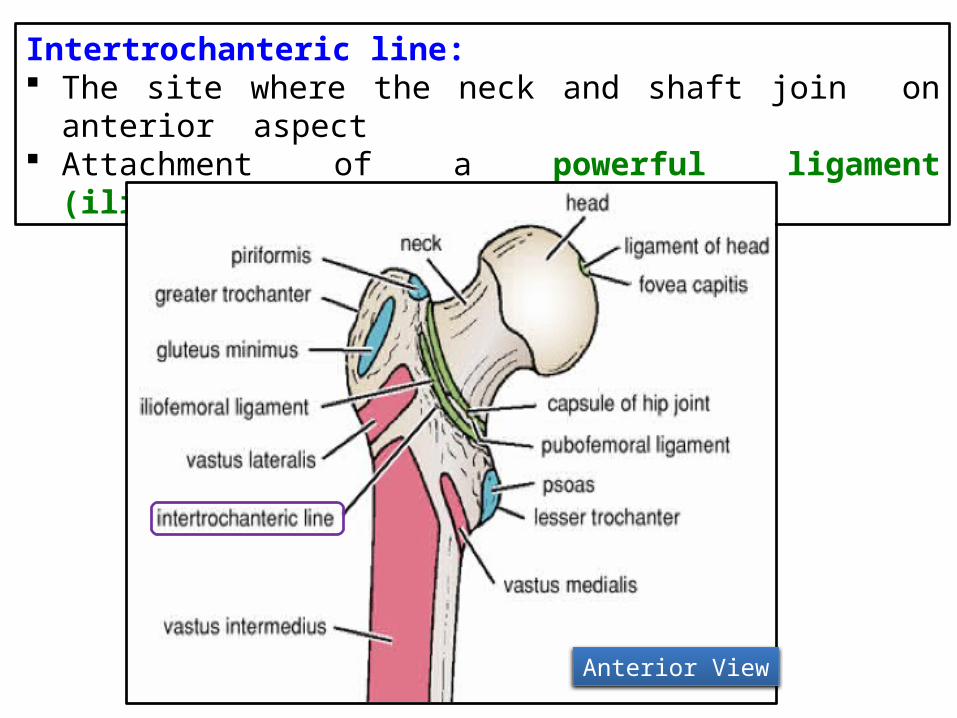
Intertrochanteric line: The site where the neck and shaft join on anterior aspect Attachment of a powerful ligament (iliofemoral ligament).
Anterior View
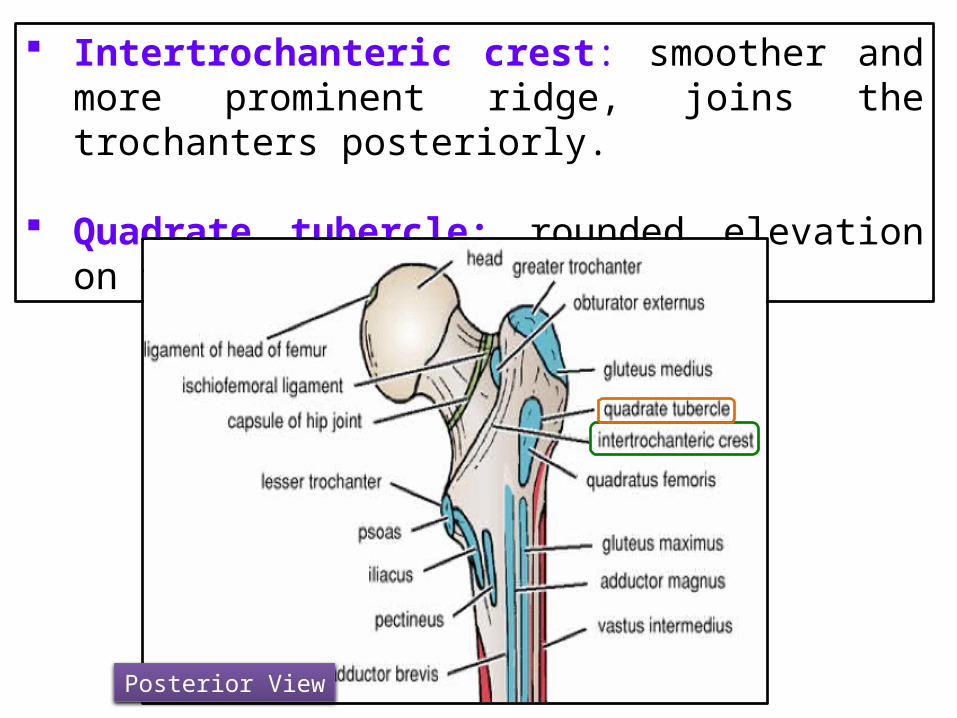
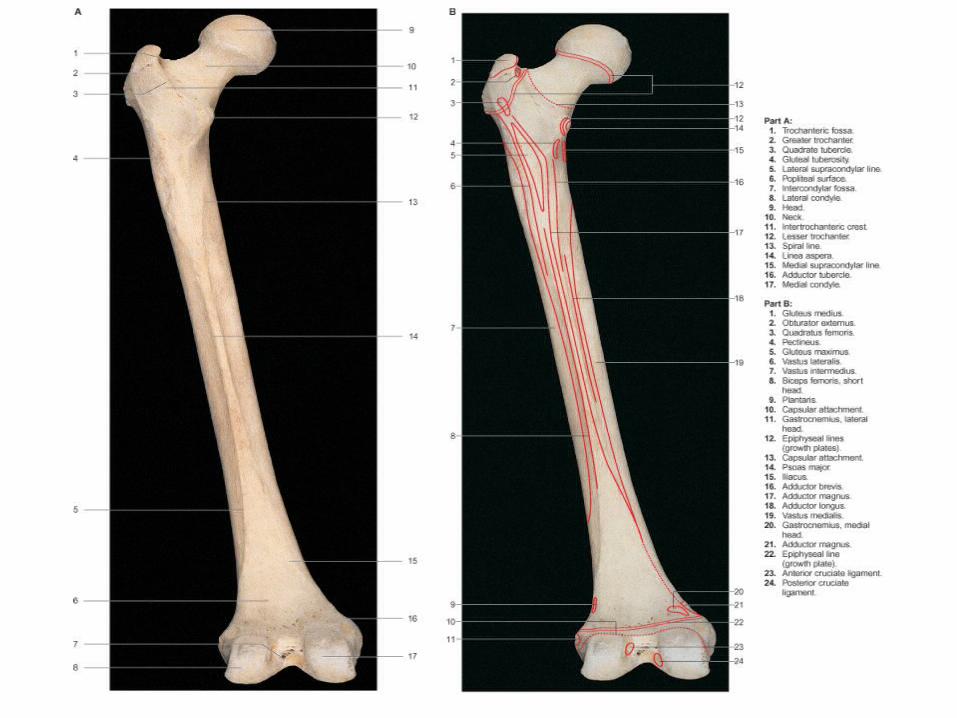
Intertrochanteric crest: smoother and more prominent ridge, joins the trochanters posteriorly.
Quadrate tubercle: rounded elevation on the crest
Posterior View
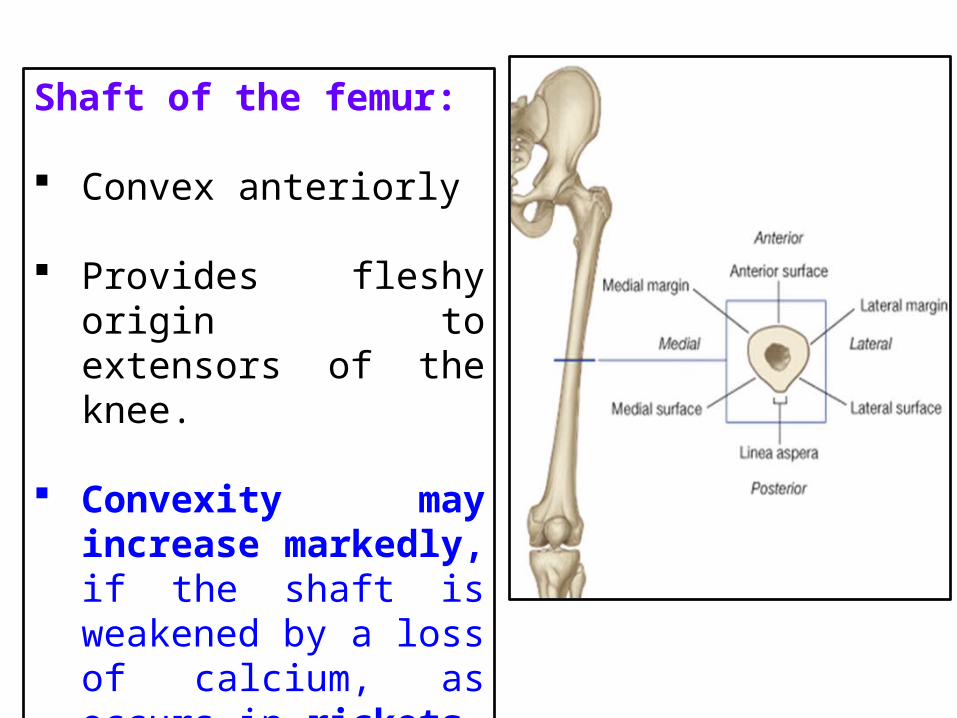
Shaft of the femur:
Convex anteriorly
Provides fleshy origin to extensors of the knee.
Convexity may increase markedly, if the shaft is weakened by a loss of calcium, as occurs in rickets.
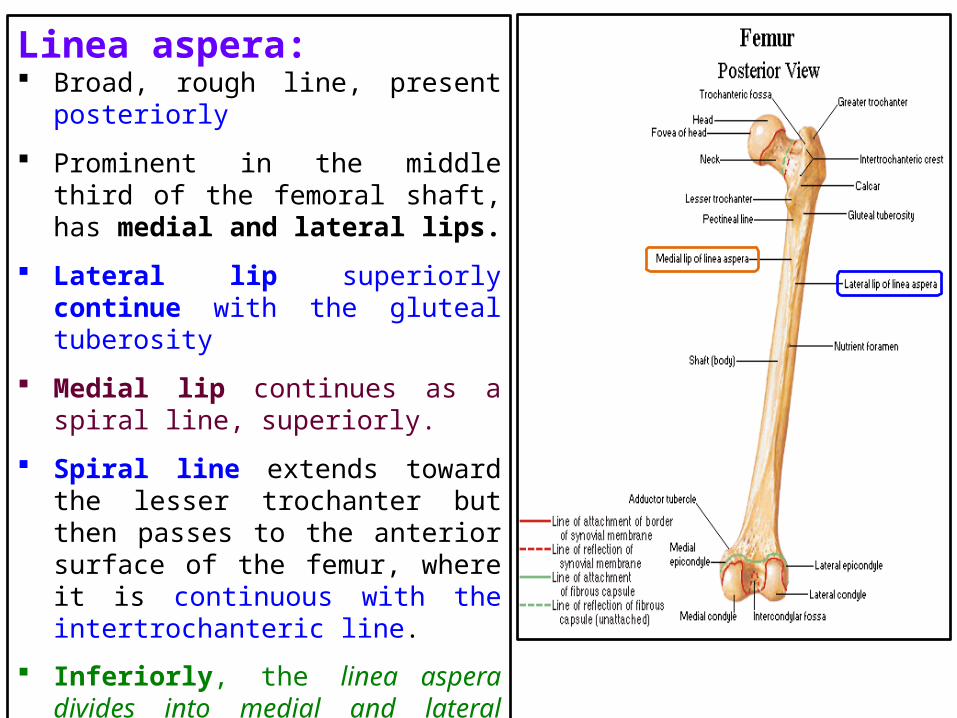
Linea aspera: Broad, rough line, present posteriorly
Prominent in the middle third of the femoral shaft, has medial and lateral lips.
Lateral lip superiorly continue with the gluteal tuberosity
Medial lip continues as a spiral line, superiorly.
Spiral line extends toward the lesser trochanter but then passes to the anterior surface of the femur, where it is continuous with the intertrochanteric line.
Inferiorly, the linea aspera divides into medial and lateral supracondylar lines.
Provides attachment for adductors of the thigh.
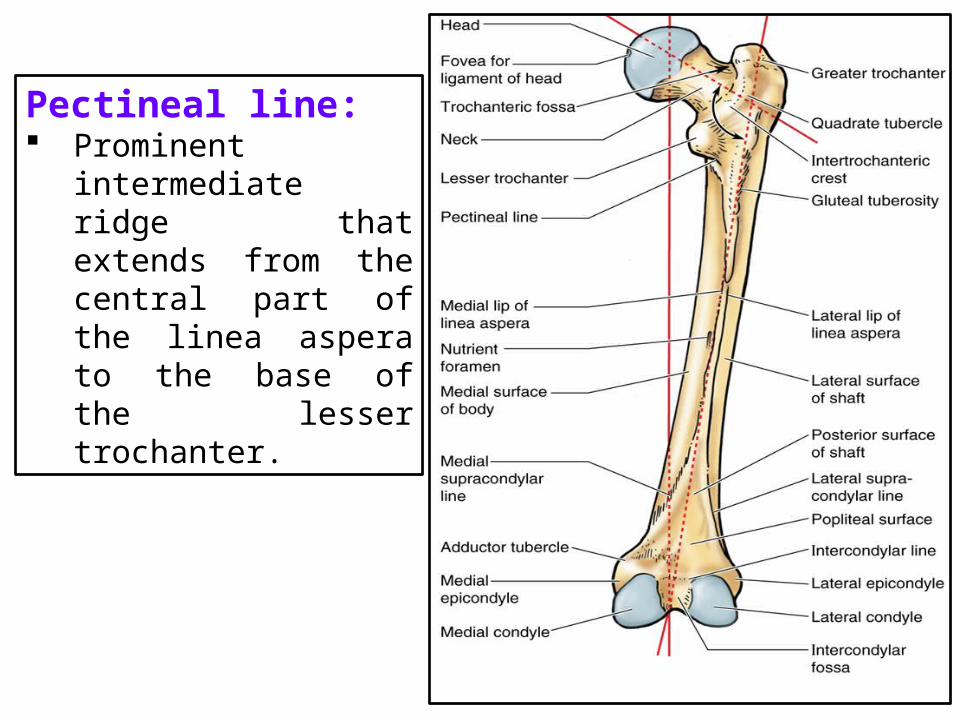
Pectineal line: Prominent intermediate
ridge that extends from the central part of the linea aspera to the base of the lesser trochanter.
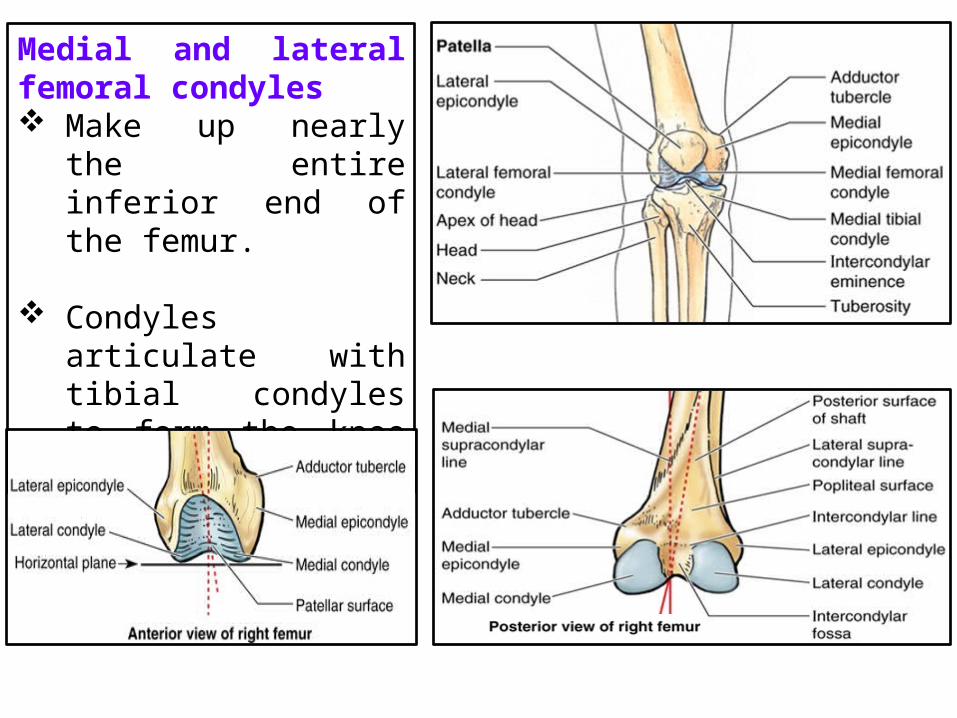
Medial and lateral femoral condyles Make up nearly the entire
inferior end of the femur.
Condyles articulate with tibial condyles to form the knee joint.
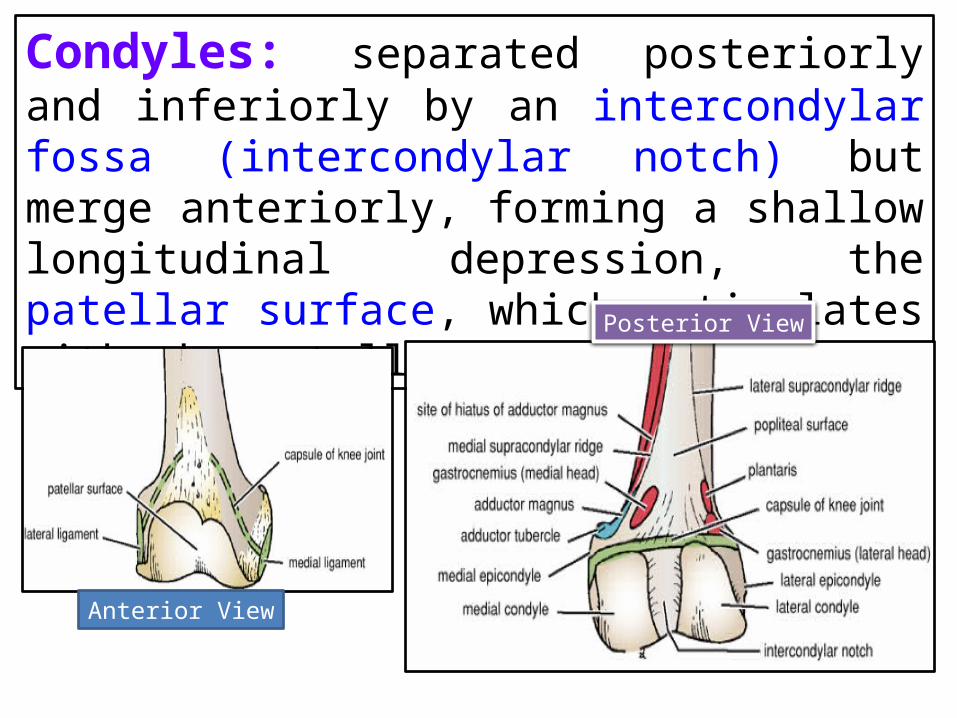
Condyles: separated posteriorly and inferiorly by an intercondylar fossa (intercondylar notch) but merge anteriorly, forming a shallow longitudinal depression, the patellar surface, which articulates with the patella.
Anterior View
Posterior View
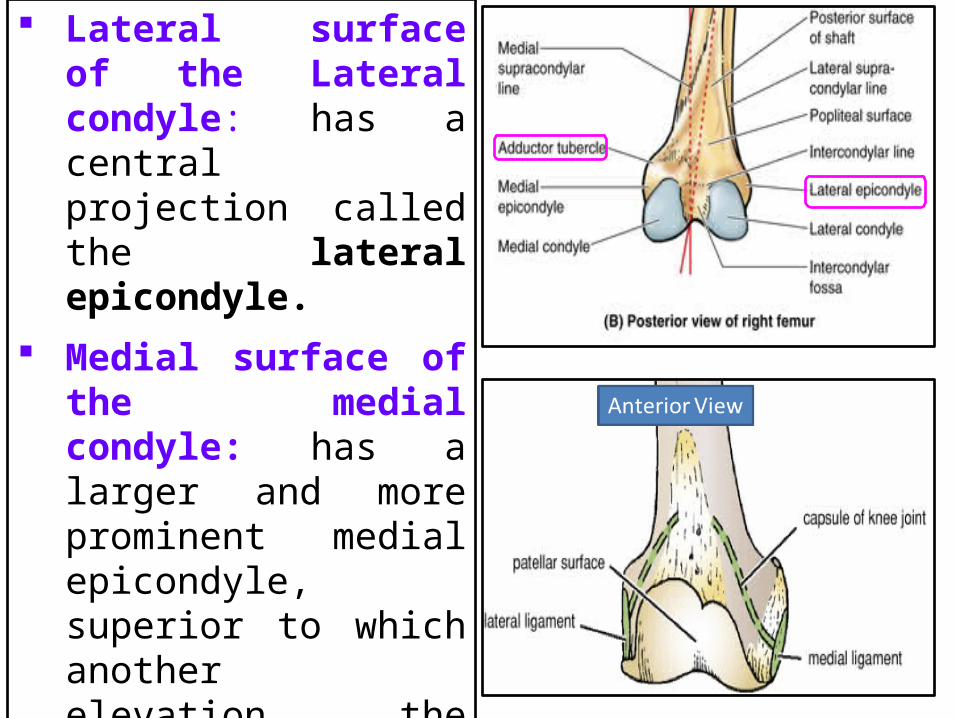
Lateral surface of the Lateral condyle: has a central projection called the lateral epicondyle.
Medial surface of the medial condyle: has a larger and more prominent medial epicondyle, superior to which another elevation, the adductor tubercle.
Epicondyles provide proximal attachment for the collateral ligaments of the knee joint.
Blood Supply to the Femoral Head and Neck Fractures
In the young, the epiphysis of the head is supplied by a small branch of the obturator artery, which passes to the head along the ligament of the femoral head.
The upper part of the neck of the femur receives a profuse blood supply from the medial femoral circumflex artery. These branches pierce the capsule and ascend the neck deep to the synovial membrane. As long as the epiphyseal cartilage remains, no communication occurs between the two sources of blood.
In the adult, after the epiphyseal cartilage disappears, an anastomosis between the two sources of blood supply is established.
Fractures of the femoral neck interfere with or completely interrupt the blood supply from the root of the femoral neck to the femoral head.
The scant blood flow along the small artery that accompanies the round ligament may be insufficient to sustain the viability of the femoral head, and ischemic necrosis gradually takes place.
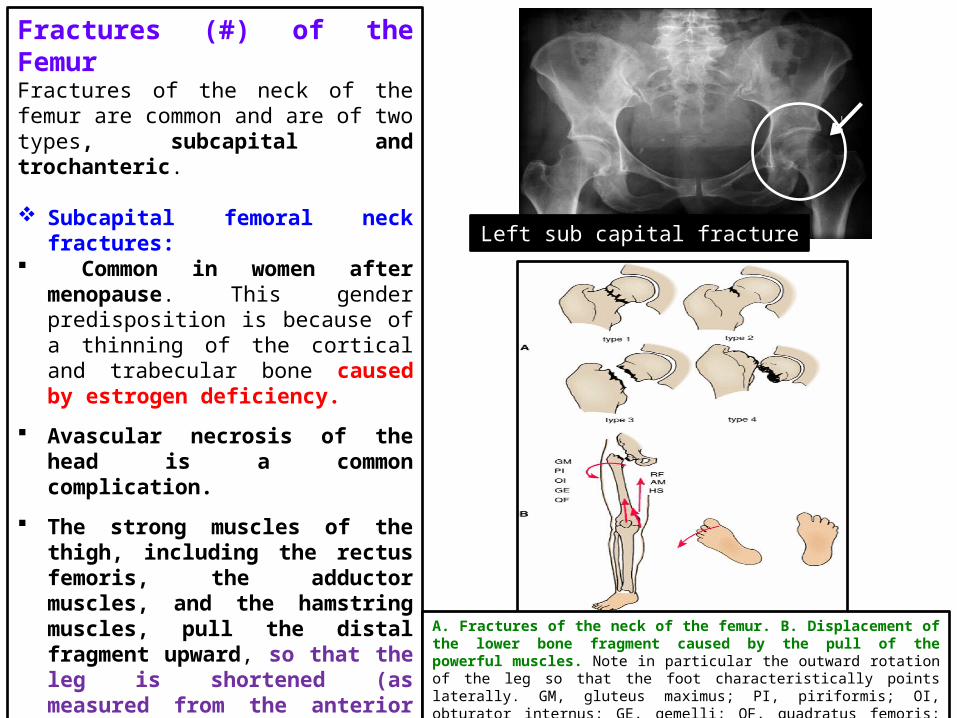
Fractures (#) of the FemurFractures of the neck of the femur are common and are of two types, subcapital and trochanteric.
Subcapital femoral neck fractures: Common in women after menopause.
This gender predisposition is because of a thinning of the cortical and trabecular bone caused by estrogen deficiency.
Avascular necrosis of the head is a common complication.
The strong muscles of the thigh, including the rectus femoris, the adductor muscles, and the hamstring muscles, pull the distal fragment upward, so that the leg is shortened (as measured from the anterior superior iliac spine to the adductor tubercle or medial malleolus).
The gluteus maximus, the piriformis, the obturator internus, the gemelli, and the quadratus femoris rotate the distal fragment laterally, as seen by the toes pointing laterally.
A. Fractures of the neck of the femur. B. Displacement of the lower bone fragment caused by the pull of the powerful muscles. Note in particular the outward rotation of the leg so that the foot characteristically points laterally. GM, gluteus maximus; PI, piriformis; OI, obturator internus; GE, gemelli; QF, quadratus femoris; RF, rectus femoris; AM, adductor muscles; HS, hamstring muscles.
Left sub capital fracture
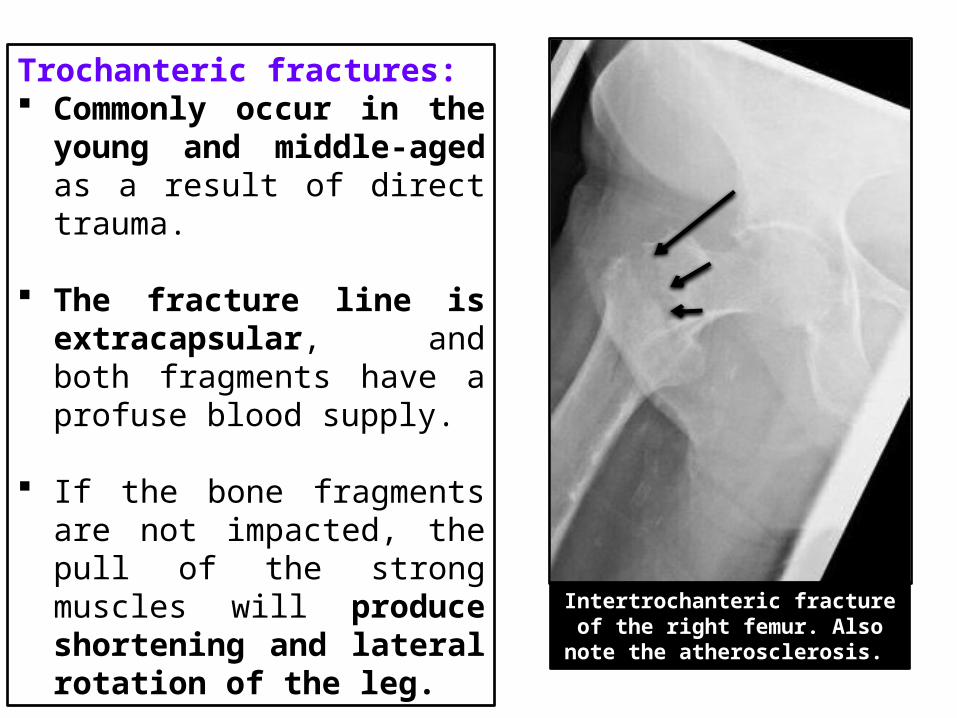
Trochanteric fractures: Commonly occur in the young
and middle-aged as a result of direct trauma.
The fracture line is extracapsular, and both fragments have a profuse blood supply.
If the bone fragments are not impacted, the pull of the strong muscles will produce shortening and lateral rotation of the leg.
Intertrochanteric fracture of the right femur. Also note the atherosclerosis.
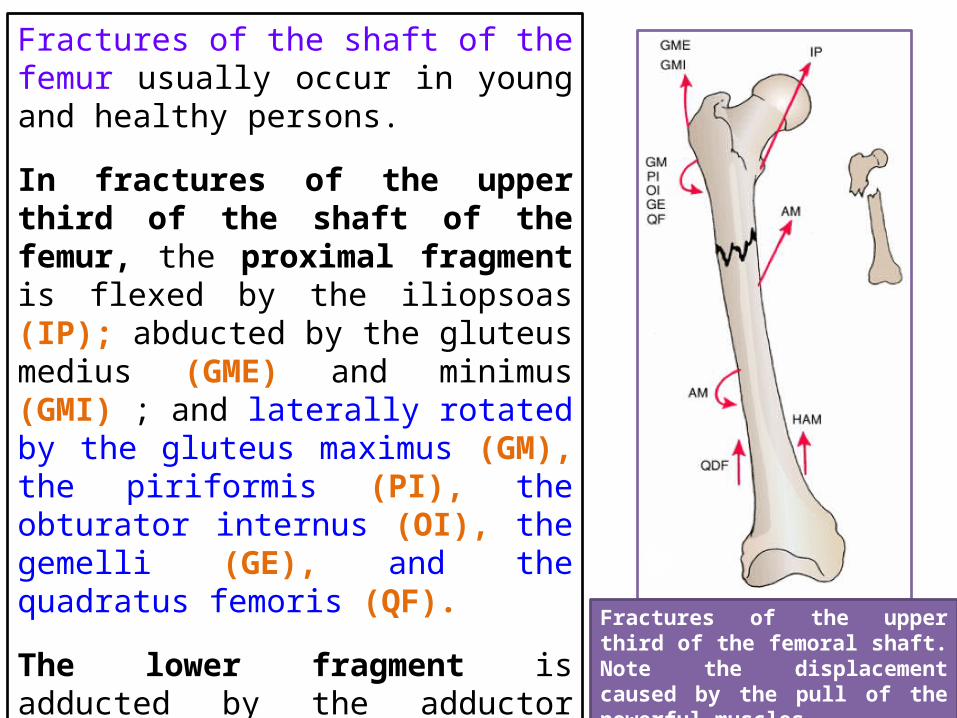
Fractures of the shaft of the femur usually occur in young and healthy persons.
In fractures of the upper third of the shaft of the femur, the proximal fragment is flexed by the iliopsoas (IP); abducted by the gluteus medius (GME) and minimus (GMI) ; and laterally rotated by the gluteus maximus (GM), the piriformis (PI), the obturator internus (OI), the gemelli (GE), and the quadratus femoris (QF).
The lower fragment is adducted by the adductor muscles (AM), pulled upward by the hamstrings (HAM) and quadriceps (QF), and laterally rotated by the adductors (AM) and the weight of the foot.
Fractures of the upper third of the femoral shaft. Note the displacement caused by the pull of the powerful muscles.
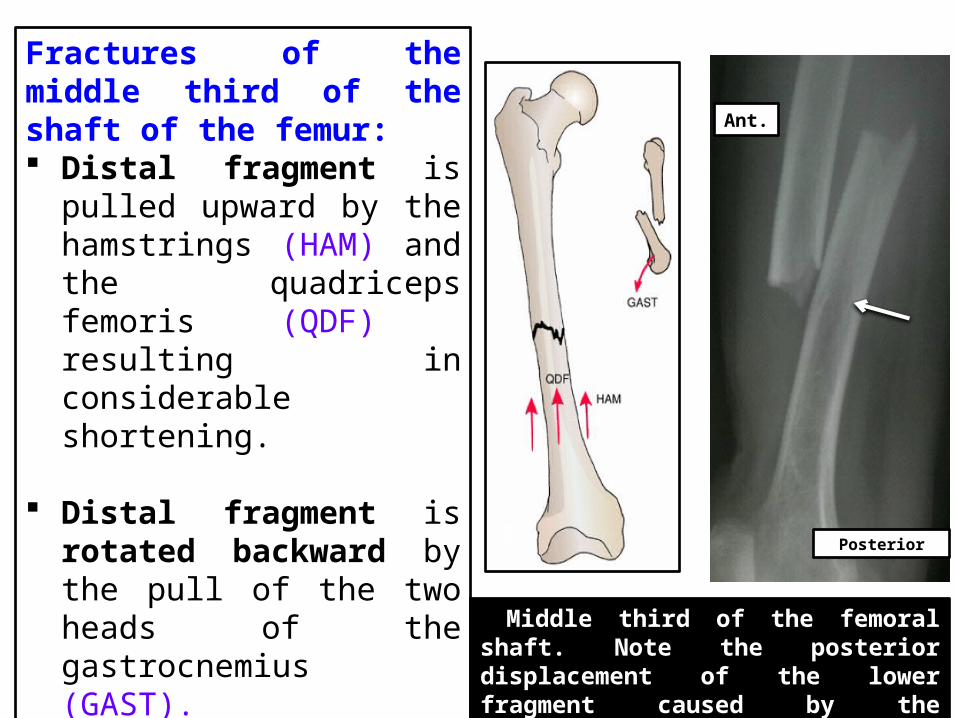
Fractures of the middle third of the shaft of the femur: Distal fragment is pulled
upward by the hamstrings (HAM) and the quadriceps femoris (QDF) resulting in considerable shortening.
Distal fragment is rotated backward by the pull of the two heads of the gastrocnemius (GAST).
Middle third of the femoral shaft. Note the posterior displacement of the lower fragment caused by the gastrocnemius muscle.
Ant.
Posterior
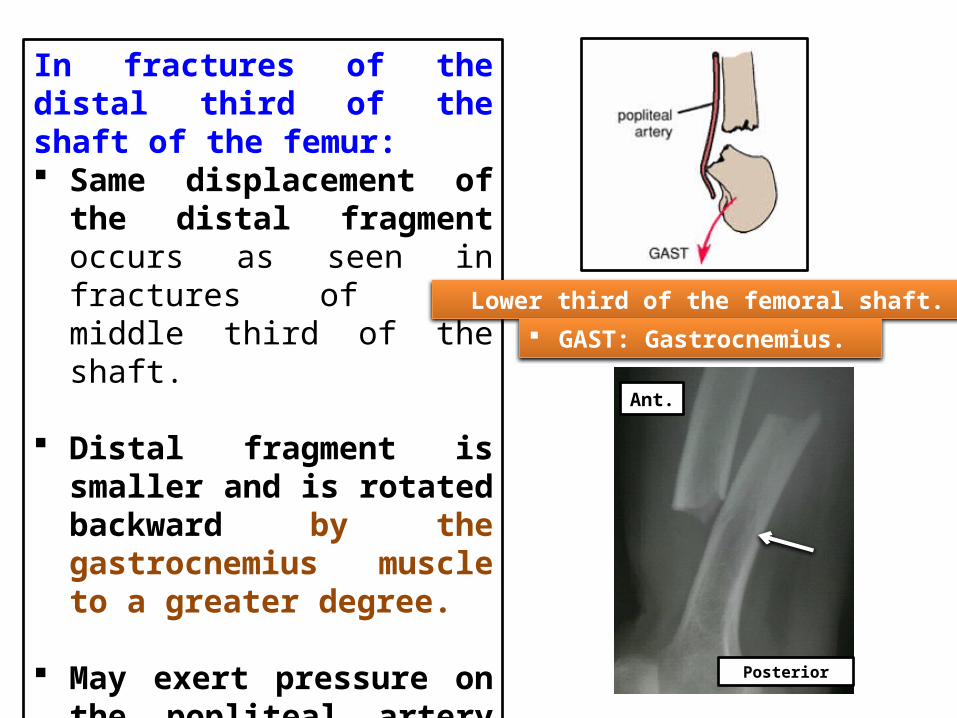
In fractures of the distal third of the shaft of the femur: Same displacement of the distal
fragment occurs as seen in fractures of the middle third of the shaft.
Distal fragment is smaller and is rotated backward by the gastrocnemius muscle to a greater degree.
May exert pressure on the popliteal artery and interfere with the blood flow through the leg and foot.
Lower third of the femoral shaft. GAST: Gastrocnemius.
Ant.
Posterior
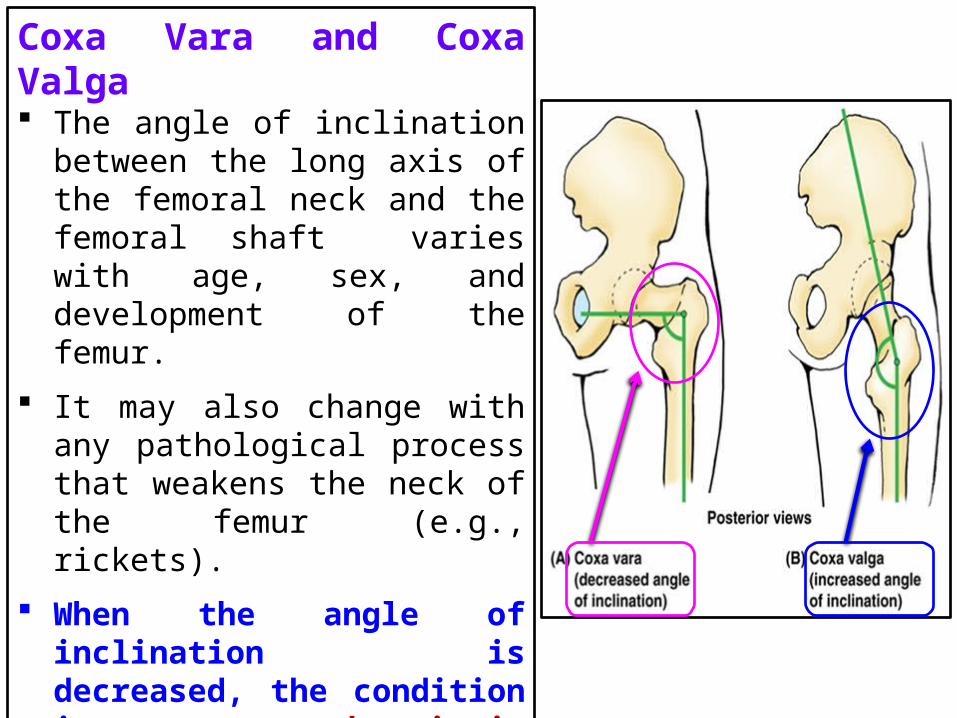
Coxa Vara and Coxa Valga The angle of inclination between
the long axis of the femoral neck and the femoral shaft varies with age, sex, and development of the femur.
It may also change with any pathological process that weakens the neck of the femur (e.g., rickets).
When the angle of inclination is decreased, the condition is coxa vara; when it is increased, it is coxa valga.
Coxa vara causes a mild shortening of the lower limb and limits passive abduction of the hip.
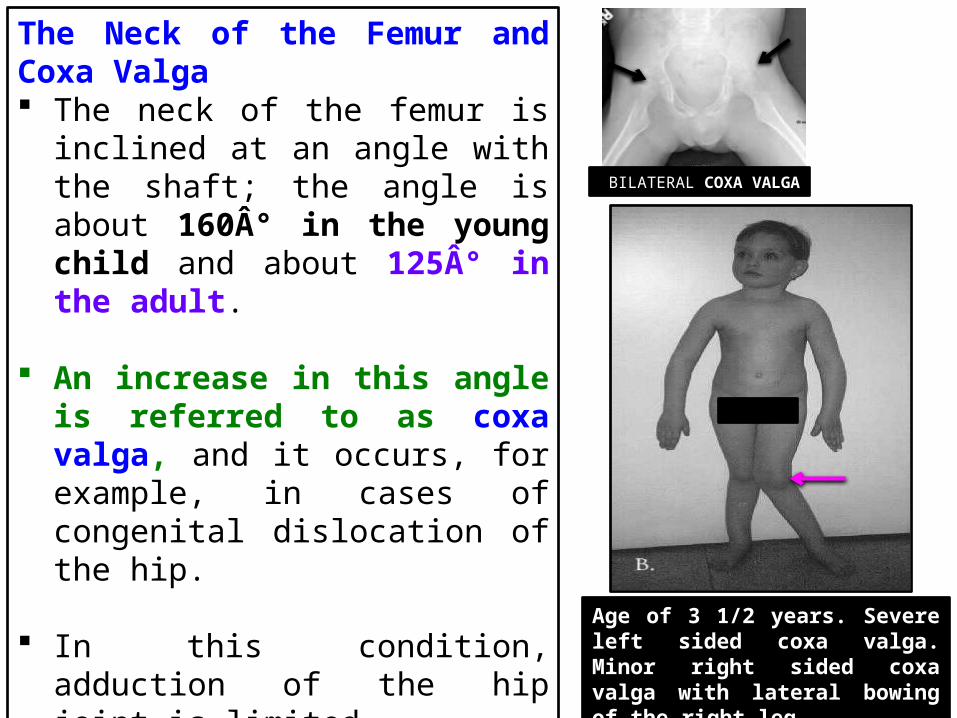
The Neck of the Femur and Coxa Valga The neck of the femur is inclined at an
angle with the shaft; the angle is about 160° in the young child and about 125° in the adult.
An increase in this angle is referred to as coxa valga, and it occurs, for example, in cases of congenital dislocation of the hip.
In this condition, adduction of the hip joint is limited.
Shenton's line is a useful means of assessing the angle of the femoral neck on a radiograph of the hip region
Age of 3 1/2 years. Severe left sided coxa valga. Minor right sided coxa valga with lateral bowing of the right leg.
BILATERAL COXA VALGA
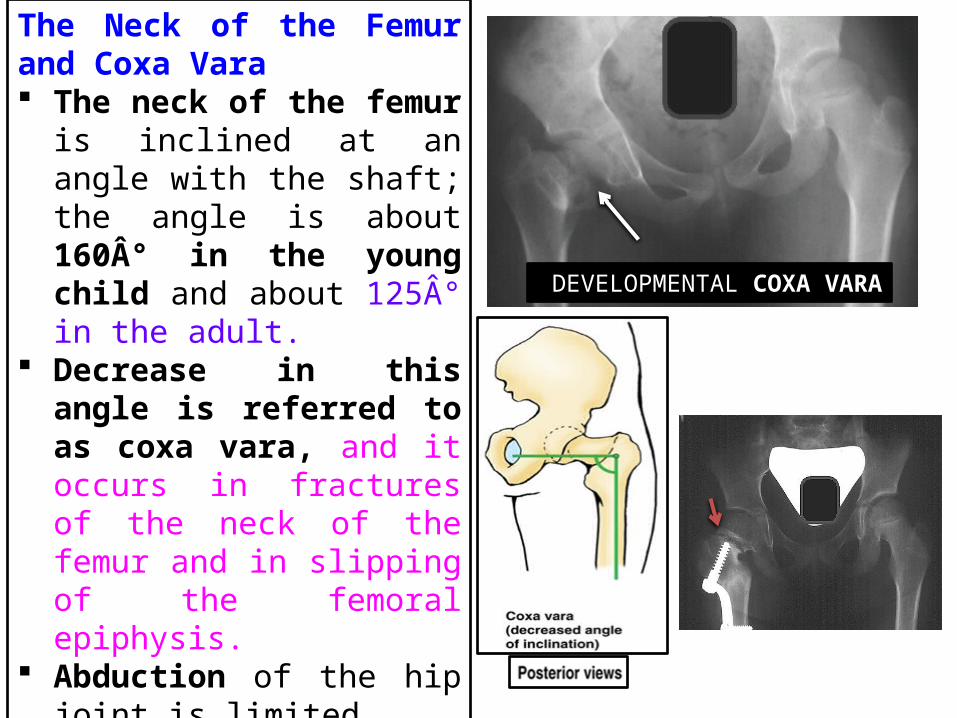
The Neck of the Femur and Coxa Vara The neck of the femur is
inclined at an angle with the shaft; the angle is about 160° in the young child and about 125° in the adult.
Decrease in this angle is referred to as coxa vara, and it occurs in fractures of the neck of the femur and in slipping of the femoral epiphysis.
Abduction of the hip joint is limited.
Shenton's line is a useful means of assessing the angle of the femoral neck on a radiograph of the hip region
DEVELOPMENTAL COXA VARA
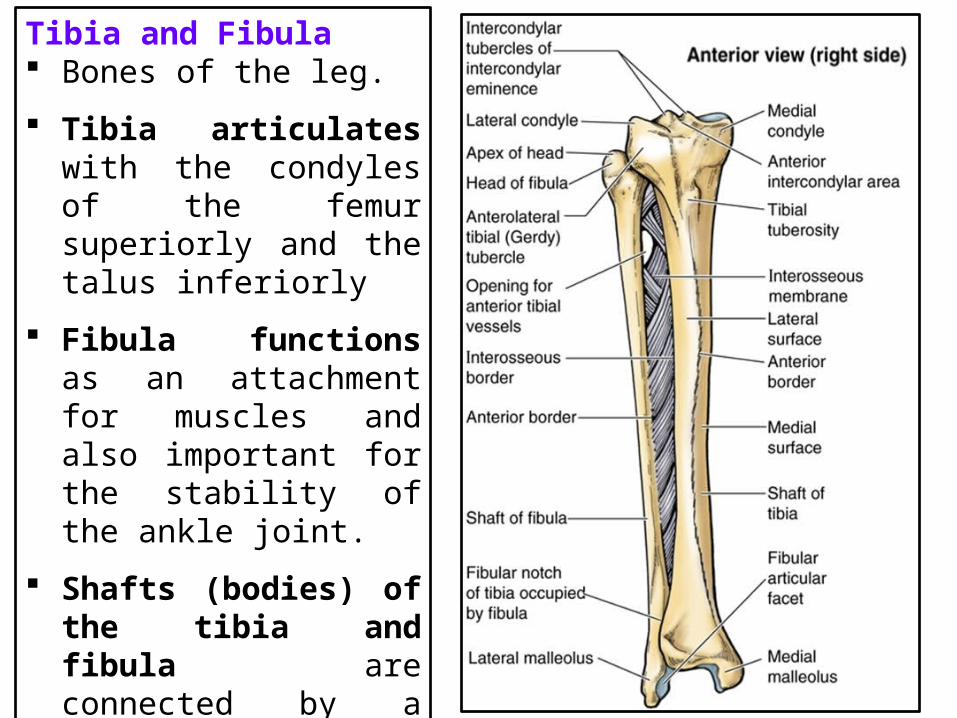
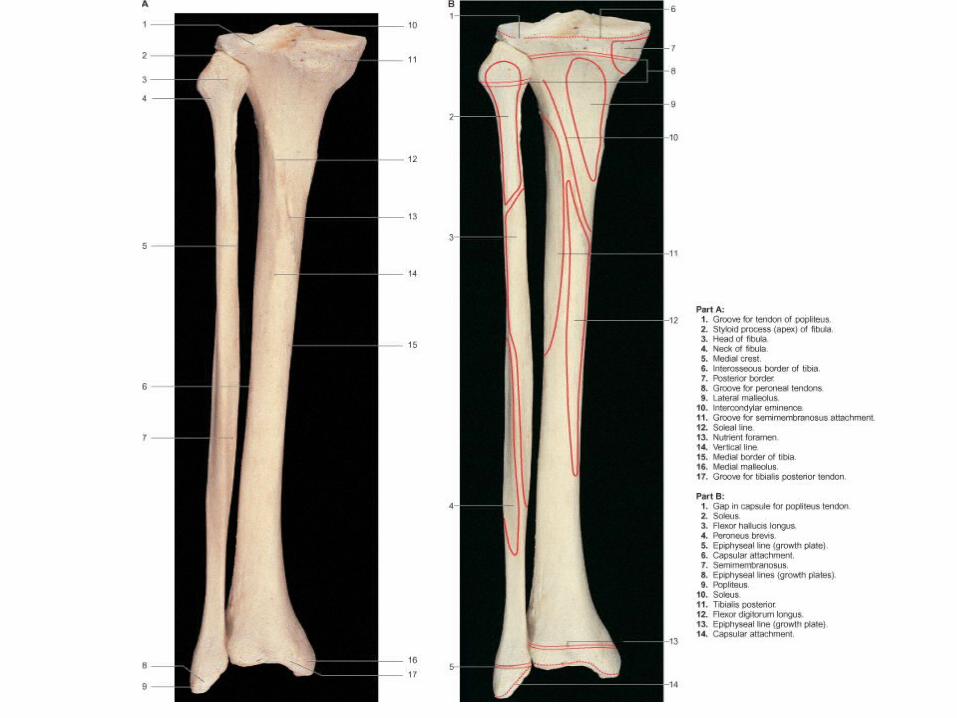
Tibia and Fibula Bones of the leg.
Tibia articulates with the condyles of the femur superiorly and the talus inferiorly
Fibula functions as an attachment for muscles and also important for the stability of the ankle joint.
Shafts (bodies) of the tibia and fibula are connected by a dense interosseous membrane composed of strong oblique fibers.
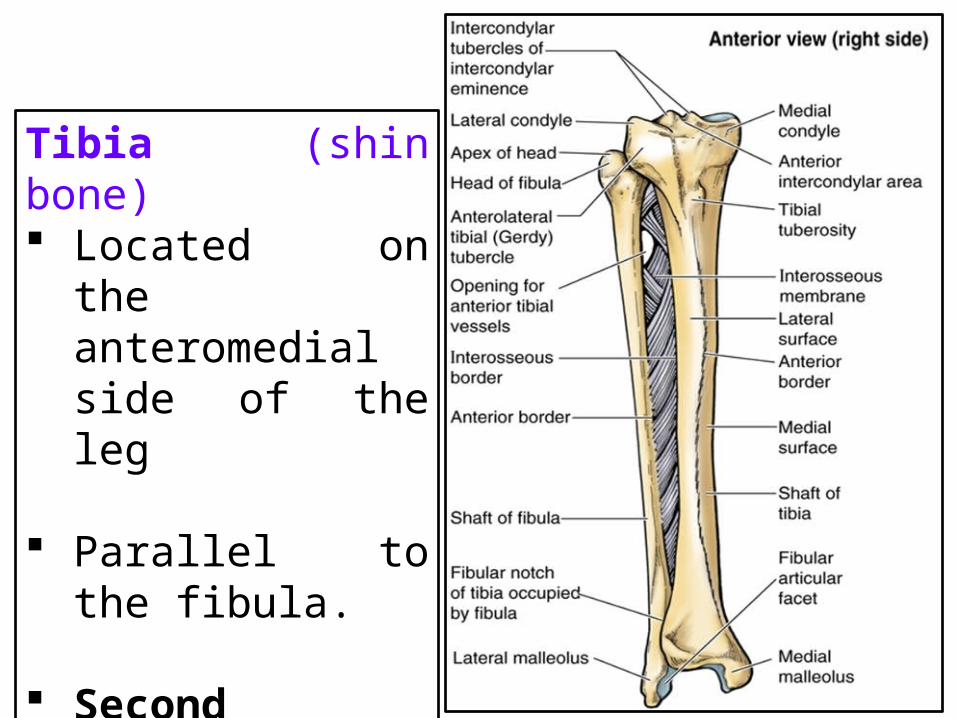
Tibia (shin bone) Located on the
anteromedial side of the leg
Parallel to the fibula.
Second largest bone in the body.
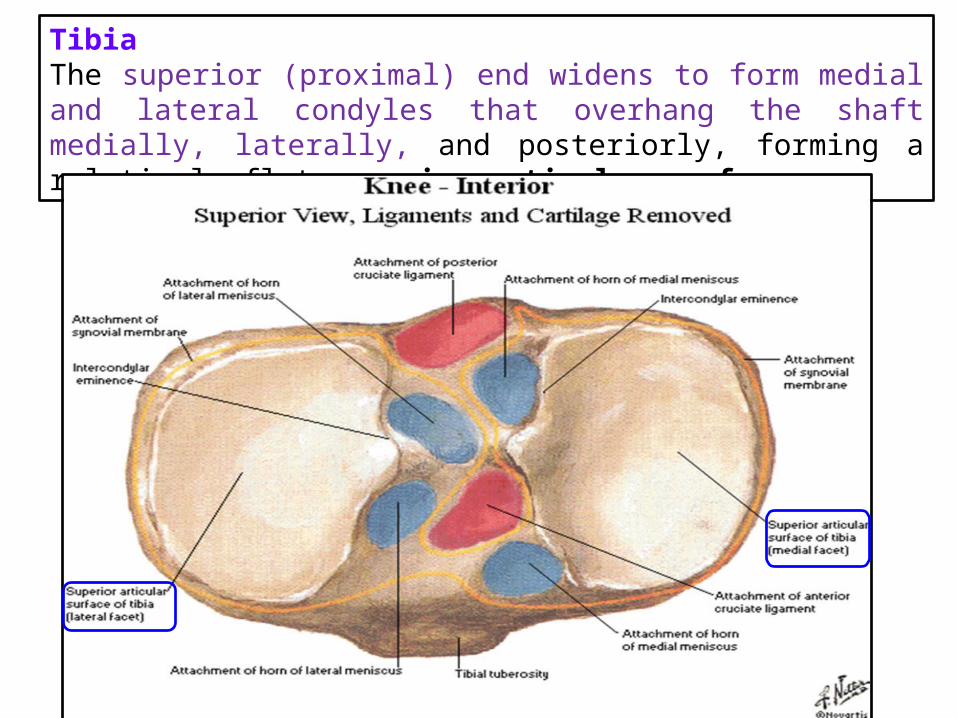
TibiaThe superior (proximal) end widens to form medial and lateral condyles that overhang the shaft medially, laterally, and posteriorly, forming a relatively flat superior articular surface.
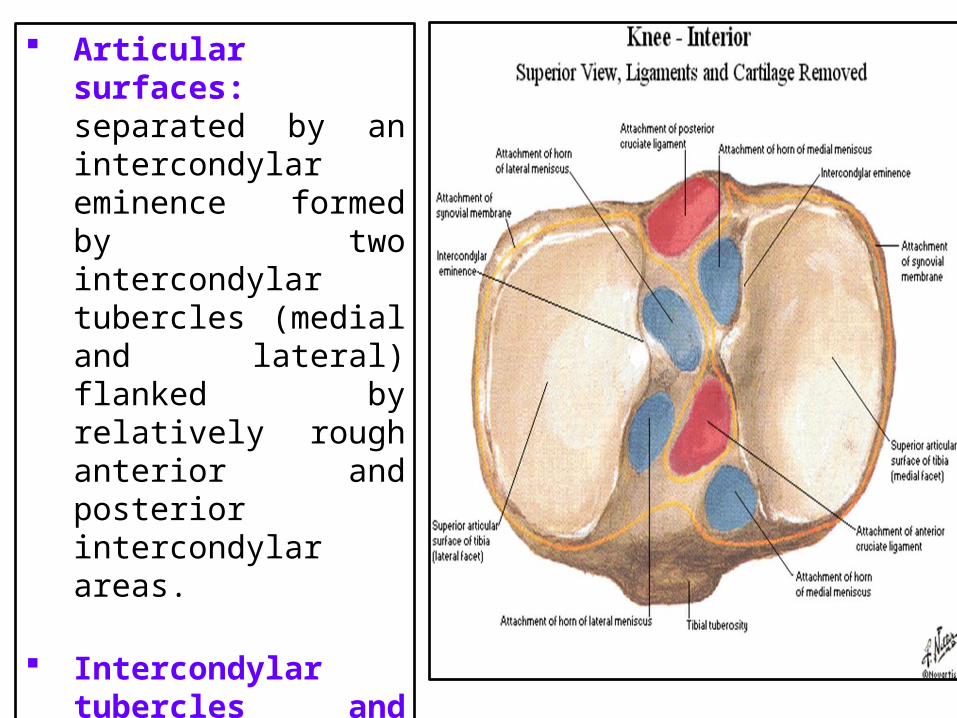
Articular surfaces: separated by an intercondylar eminence formed by two intercondylar tubercles (medial and lateral) flanked by relatively rough anterior and posterior intercondylar areas.
Intercondylar tubercles and areas: provide attachment for the menisci and principal ligaments of the knee.
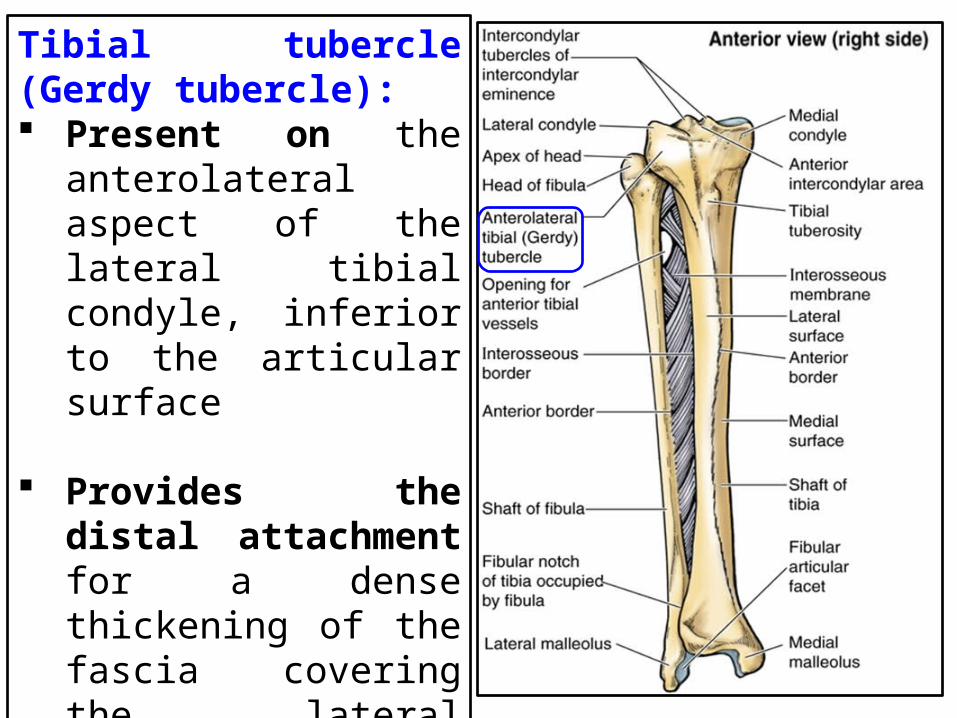
Tibial tubercle (Gerdy tubercle): Present on the
anterolateral aspect of the lateral tibial condyle, inferior to the articular surface
Provides the distal attachment for a dense thickening of the fascia covering the lateral thigh, adding stability to the knee joint.
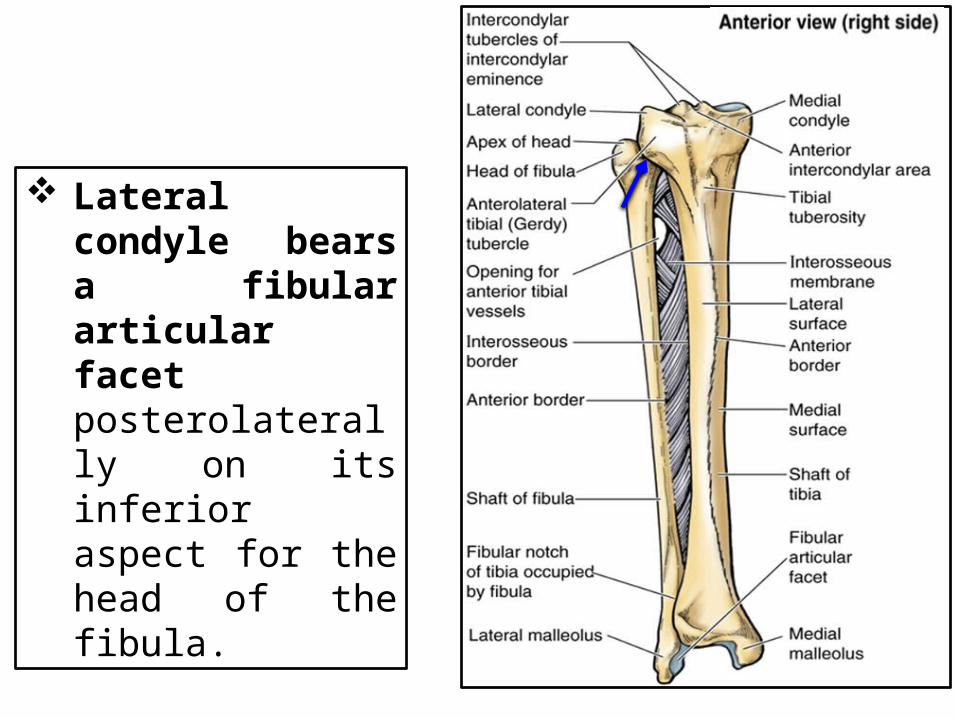
Lateral condyle bears a fibular articular facet posterolaterally on its inferior aspect for the head of the fibula.
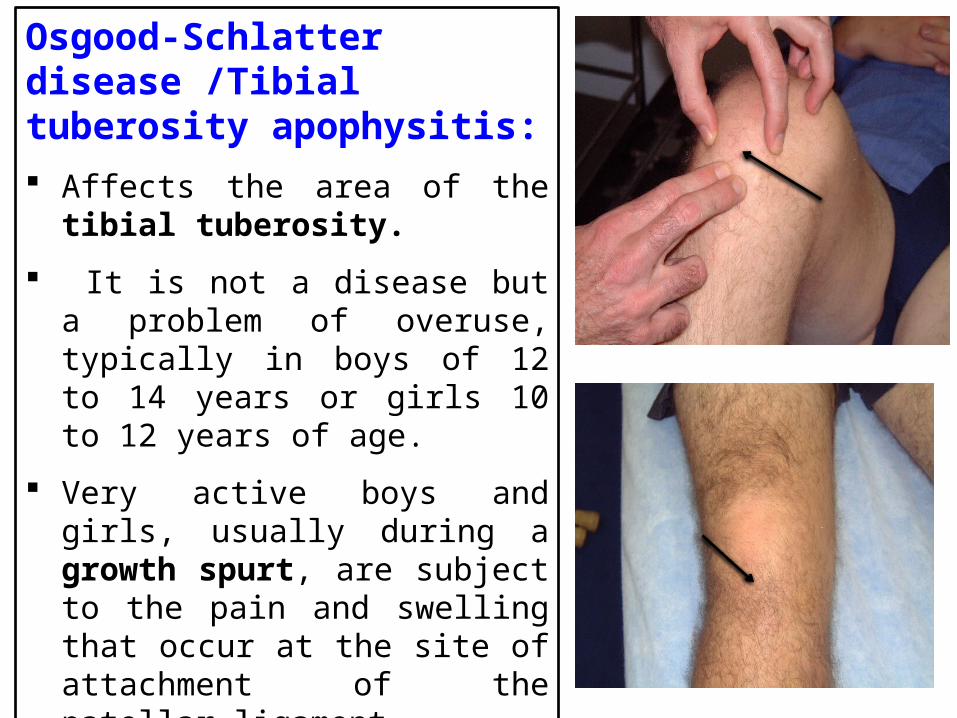
Osgood-Schlatter disease /Tibial tuberosity apophysitis: Affects the area of the tibial
tuberosity.
It is not a disease but a problem of overuse, typically in boys of 12 to 14 years or girls 10 to 12 years of age.
Very active boys and girls, usually during a growth spurt, are subject to the pain and swelling that occur at the site of attachment of the patellar ligament.
The ligament can tear, resulting in a long period of healing following treatment.
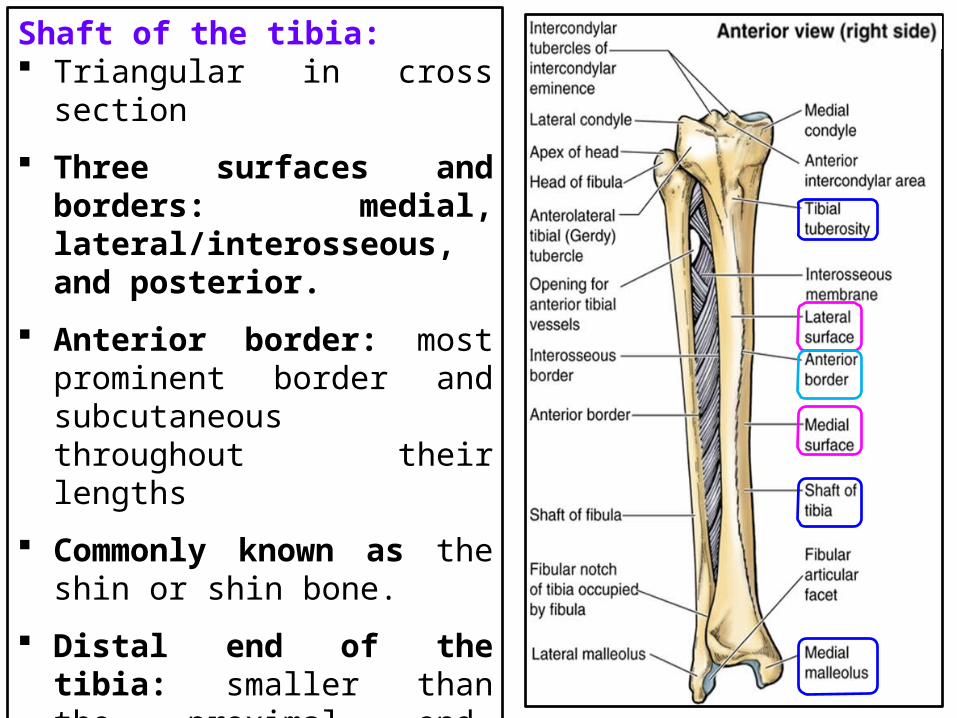
Shaft of the tibia: Triangular in cross section
Three surfaces and borders: medial, lateral/interosseous, and posterior.
Anterior border: most prominent border and subcutaneous throughout their lengths
Commonly known as the shin or shin bone.
Distal end of the tibia: smaller than the proximal end, flaring only medially; the medial expansion extends inferior to the rest of the shaft as the medial malleolus.
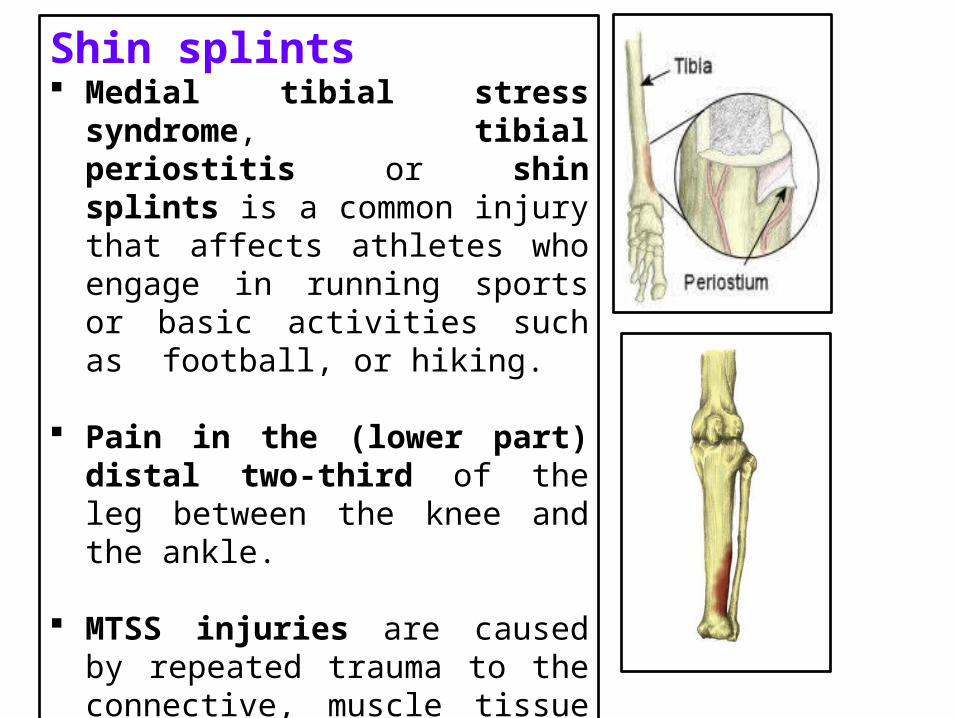
Shin splints Medial tibial stress syndrome, tibial
periostitis or shin splints is a common injury that affects athletes who engage in running sports or basic activities such as football, or hiking.
Pain in the (lower part) distal two-third of the leg between the knee and the ankle.
MTSS injuries are caused by repeated trauma to the connective, muscle tissue surrounding the tibia.
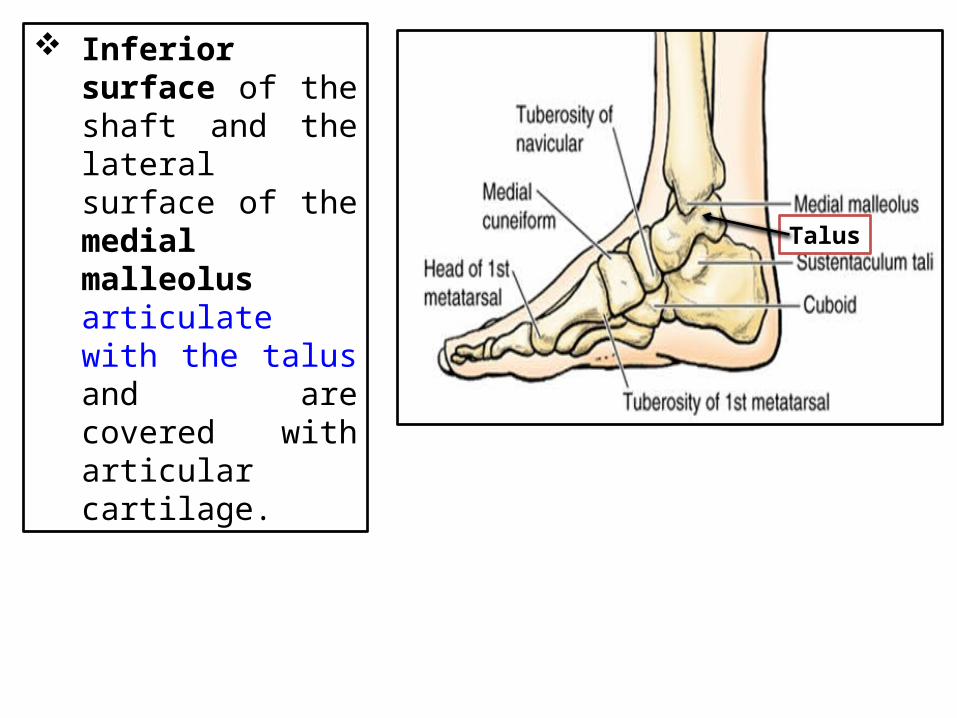
Inferior surface of the shaft and the lateral surface of the medial malleolus articulate with the talus and are covered with articular cartilage.
Talus
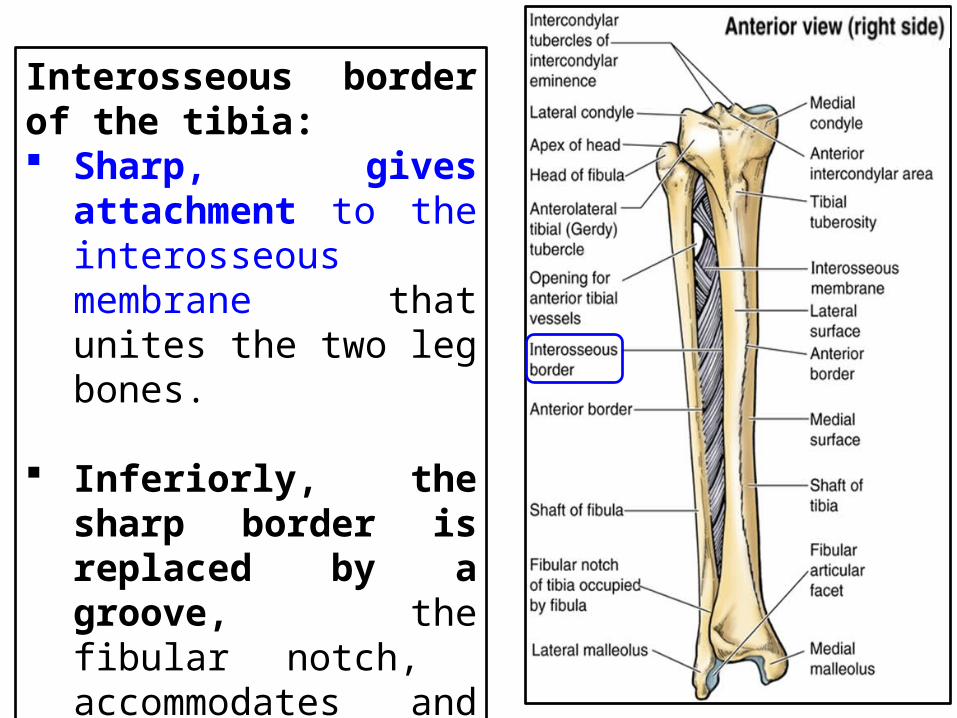
Interosseous border of the tibia: Sharp, gives attachment
to the interosseous membrane that unites the two leg bones.
Inferiorly, the sharp border is replaced by a groove, the fibular notch, accommodates and provides fibrous attachment to the distal end of the fibula.
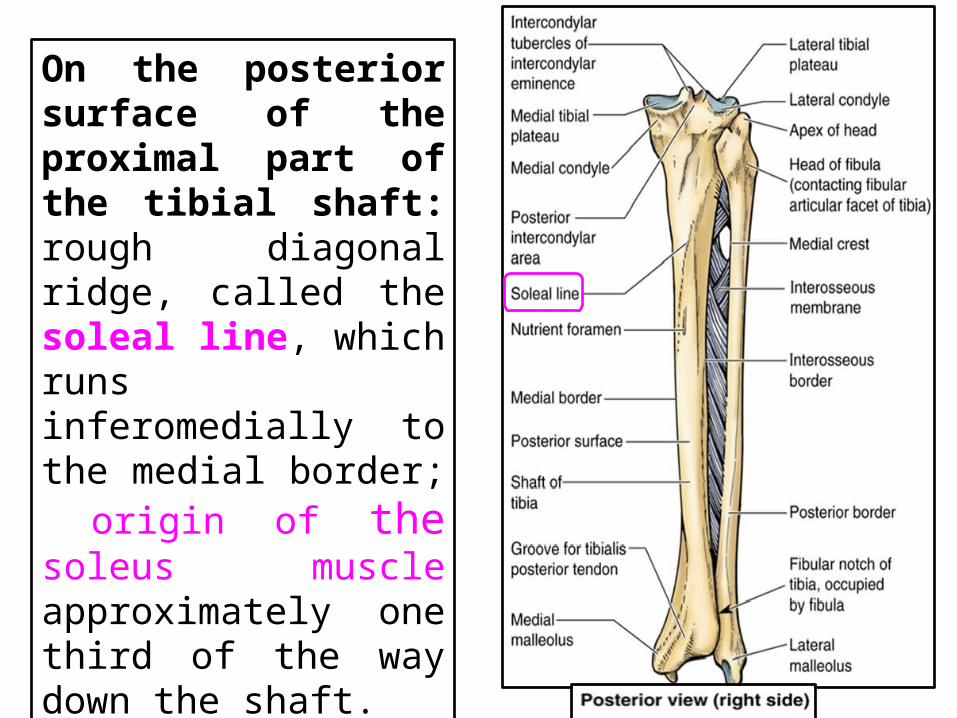
On the posterior surface of the proximal part of the tibial shaft: rough diagonal ridge, called the soleal line, which runs inferomedially to the medial border; origin of the soleus muscle approximately one third of the way down the shaft.
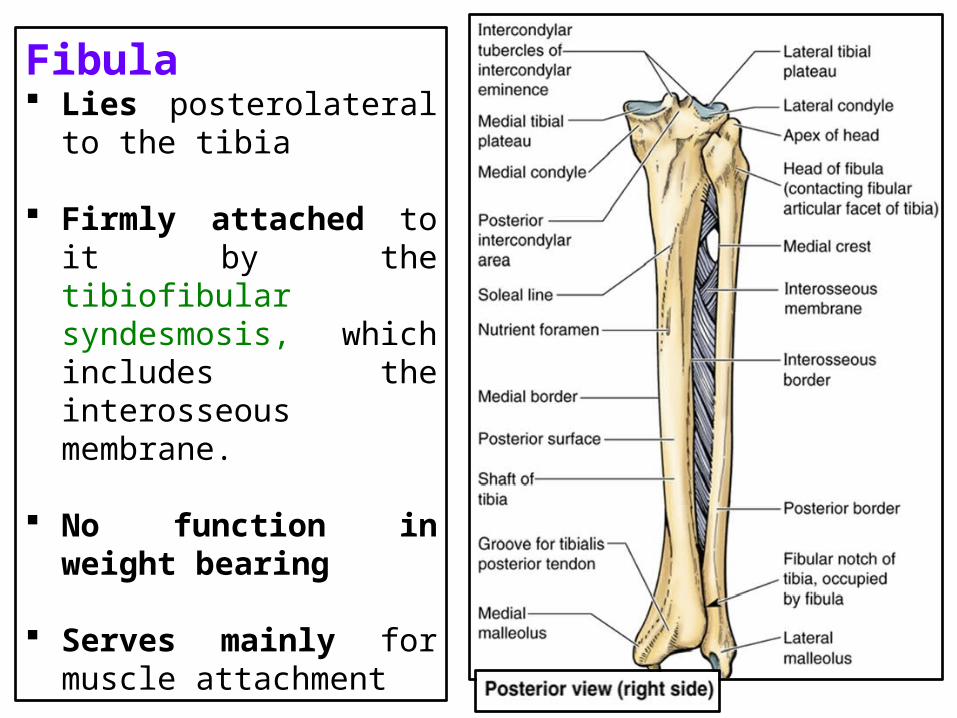
Fibula Lies posterolateral to the
tibia
Firmly attached to it by the tibiofibular syndesmosis, which includes the interosseous membrane.
No function in weight bearing
Serves mainly for muscle attachment
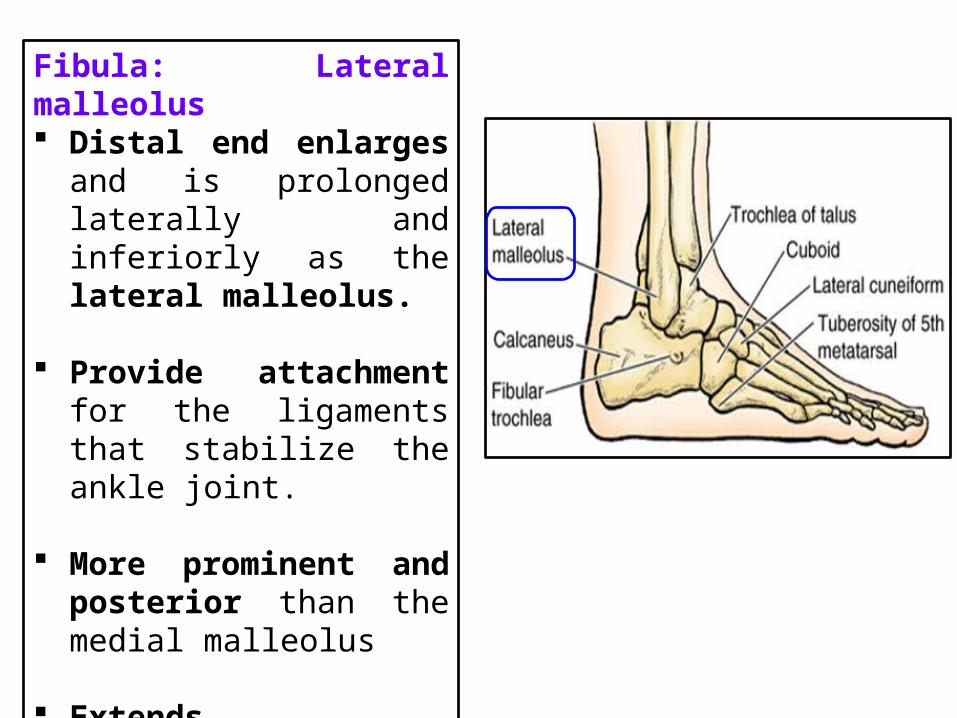
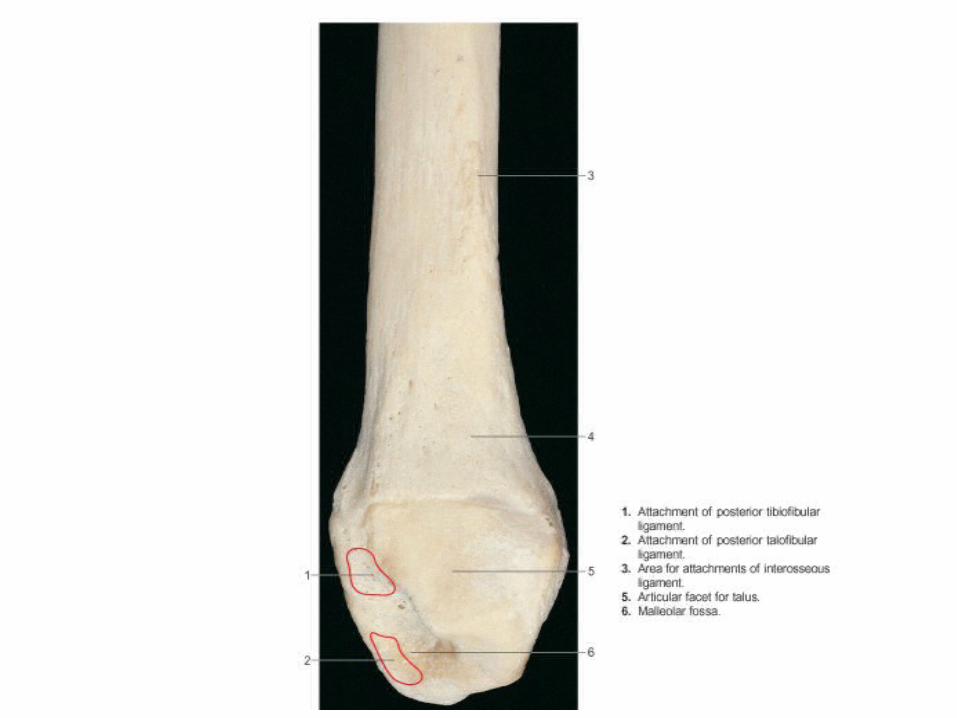
Fibula: Lateral malleolus Distal end enlarges and is
prolonged laterally and inferiorly as the lateral malleolus.
Provide attachment for the ligaments that stabilize the ankle joint.
More prominent and posterior than the medial malleolus
Extends approximately 1 cm more distally.
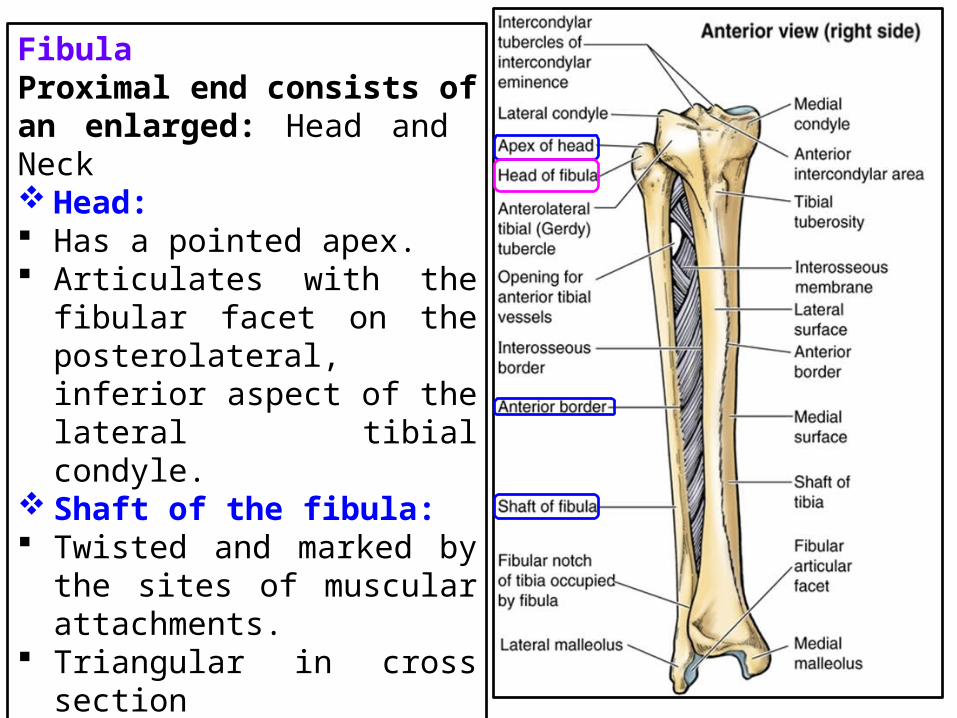
FibulaProximal end consists of an enlarged: Head and Neck Head: Has a pointed apex. Articulates with the fibular facet
on the posterolateral, inferior aspect of the lateral tibial condyle.
Shaft of the fibula: Twisted and marked by the sites
of muscular attachments. Triangular in cross section Has three borders (anterior,
interosseous, and posterior) and three surfaces (medial, posterior, and lateral).
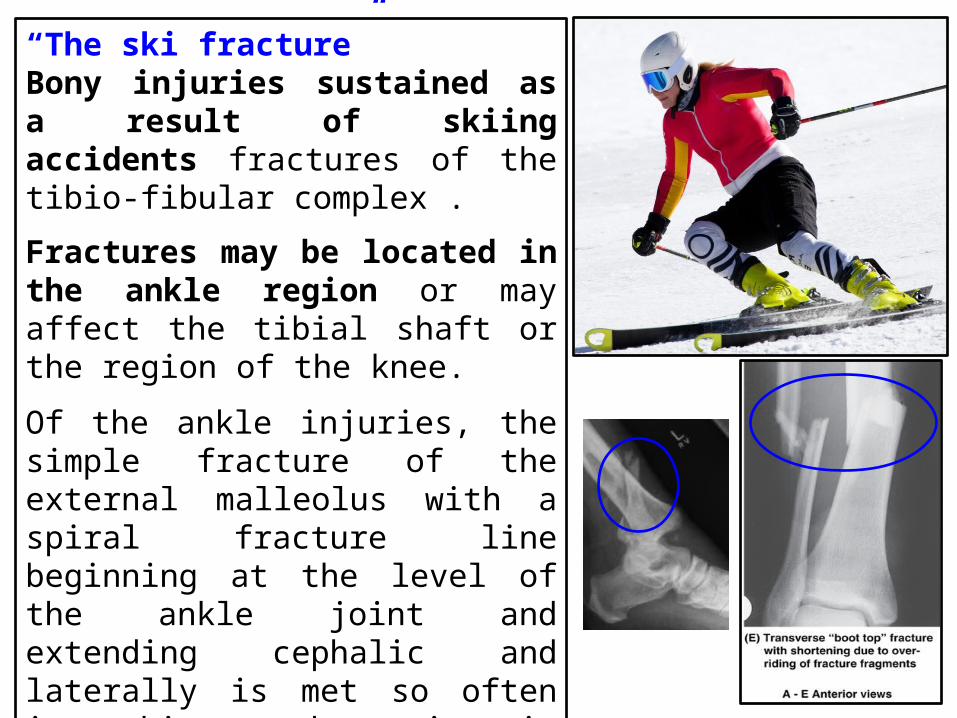
“The ski fracture”Bony injuries sustained as a result of skiing accidents fractures of the tibio-fibular complex .
Fractures may be located in the ankle region or may affect the tibial shaft or the region of the knee.
Of the ankle injuries, the simple fracture of the external malleolus with a spiral fracture line beginning at the level of the ankle joint and extending cephalic and laterally is met so often in skiers that it is sometimes called “The ski fracture”
(Btazntv 1957, Moritz 1959, Ellison, Carroll, Haddon & Wolf 1962, Spademan 1968).REF: Linden W. V. D. 1970):The Skiers’ Boot Top Fracture: Rising Incidence, Characteristics, Treatment; 40, 797-806: Acta orthop. Scandinav.
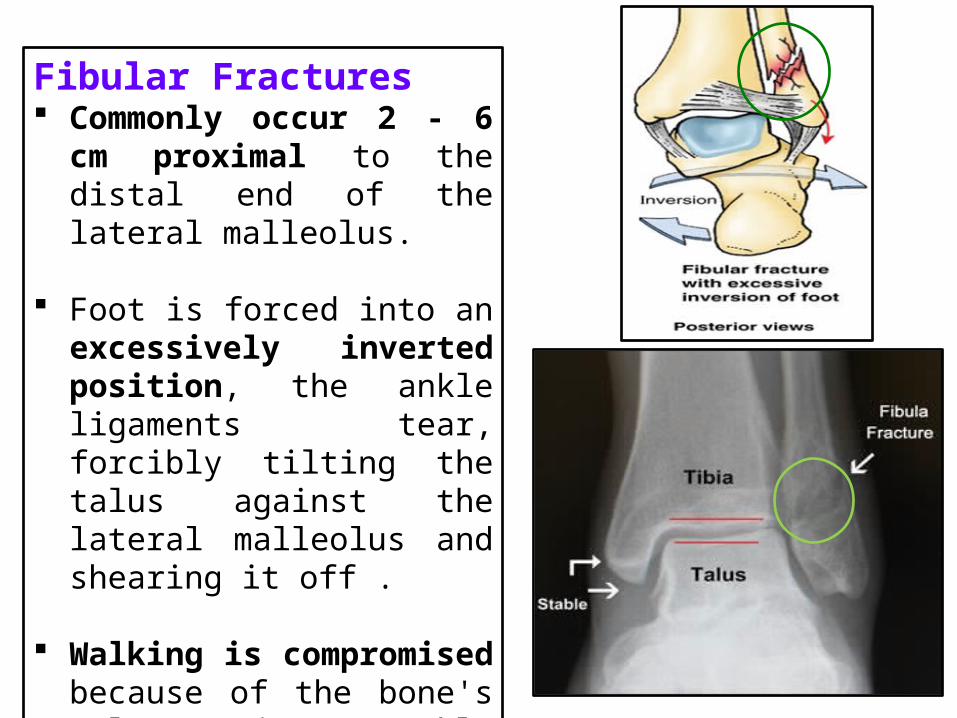
Fibular Fractures Commonly occur 2 - 6 cm
proximal to the distal end of the lateral malleolus.
Foot is forced into an excessively inverted position, the ankle ligaments tear, forcibly tilting the talus against the lateral malleolus and shearing it off .
Walking is compromised because of the bone's role in ankle stability.
Bone Grafts: The fibula is a common source of bone for grafting.
Even after a segment of shaft has been removed, walking, running, and jumping can be normal.
Free vascularized fibulas have been used to restore skeletal integrity to upper and lower limbs in which congenital bone defects exist and to replace segments of bone after trauma or excision of a malignant tumor.
Awareness of the location of the nutrient foramen is important when performing free vascularized fibular transfers. The foramen is located in the middle third of the fibula in most cases.
The graft must include a blood supply to the marrow cavity as well as to the compact bone of the surface (via the periosteum).
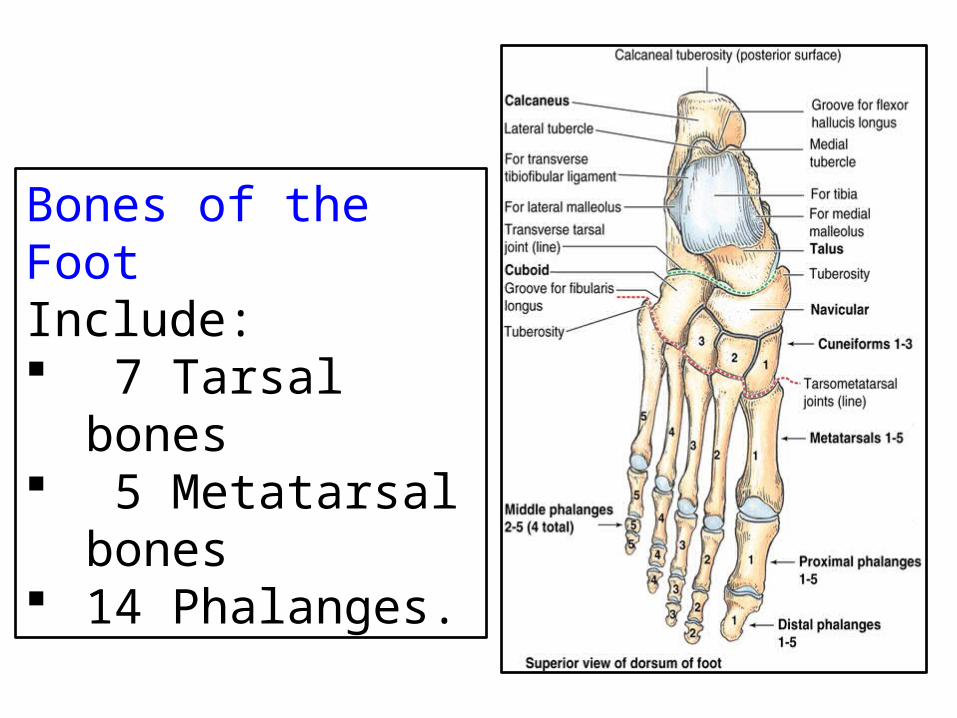
Bones of the FootInclude: 7 Tarsal bones 5 Metatarsal bones 14 Phalanges.
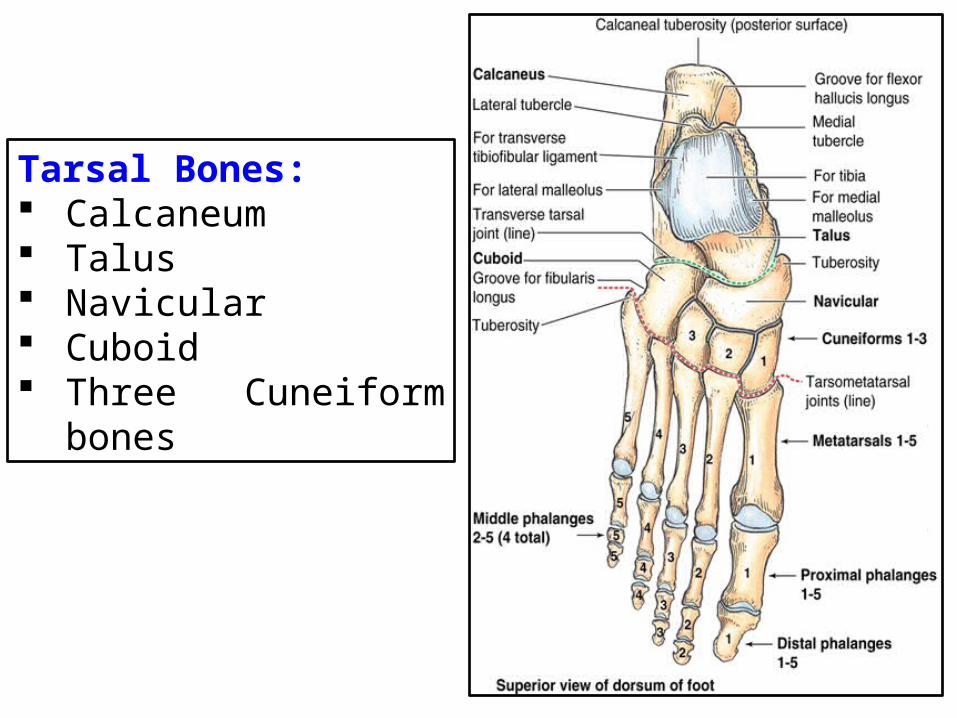
Tarsal Bones: Calcaneum Talus Navicular Cuboid Three Cuneiform bones
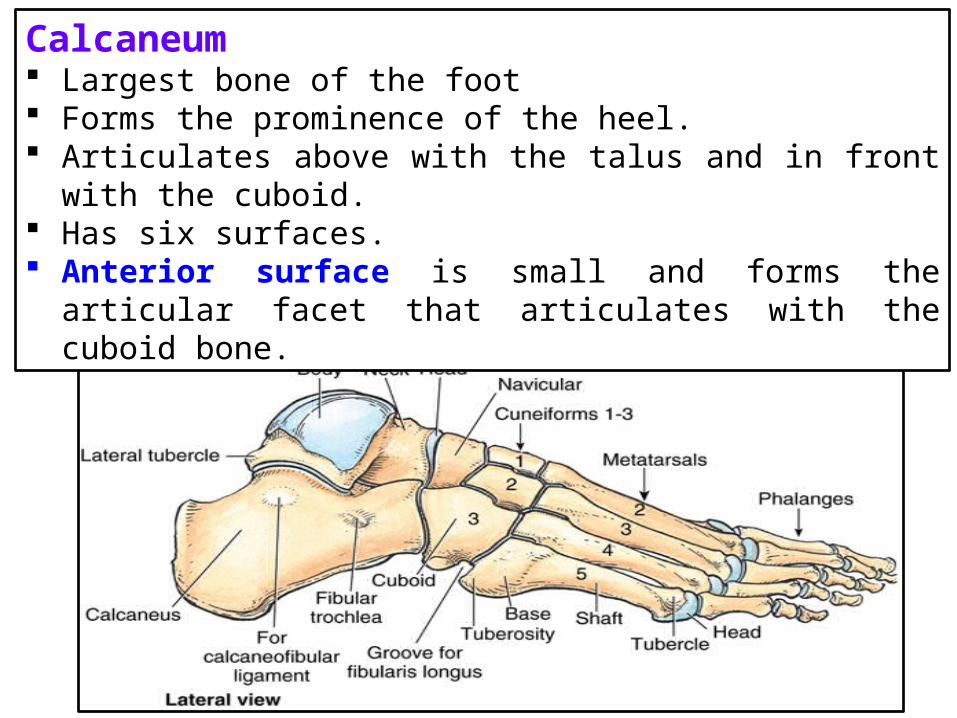
Calcaneum Largest bone of the foot Forms the prominence of the heel. Articulates above with the talus and in front with the cuboid. Has six surfaces. Anterior surface is small and forms the articular facet that
articulates with the cuboid bone.
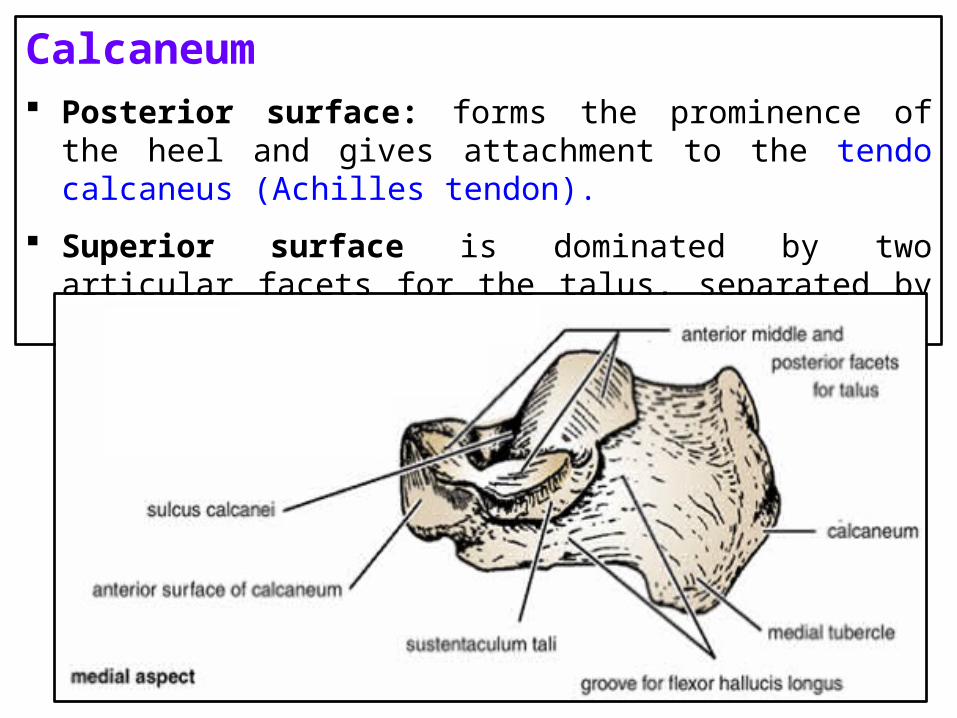
Calcaneum Posterior surface: forms the prominence of the heel and gives
attachment to the tendo calcaneus (Achilles tendon).
Superior surface is dominated by two articular facets for the talus, separated by a roughened groove, the sulcus calcanei.
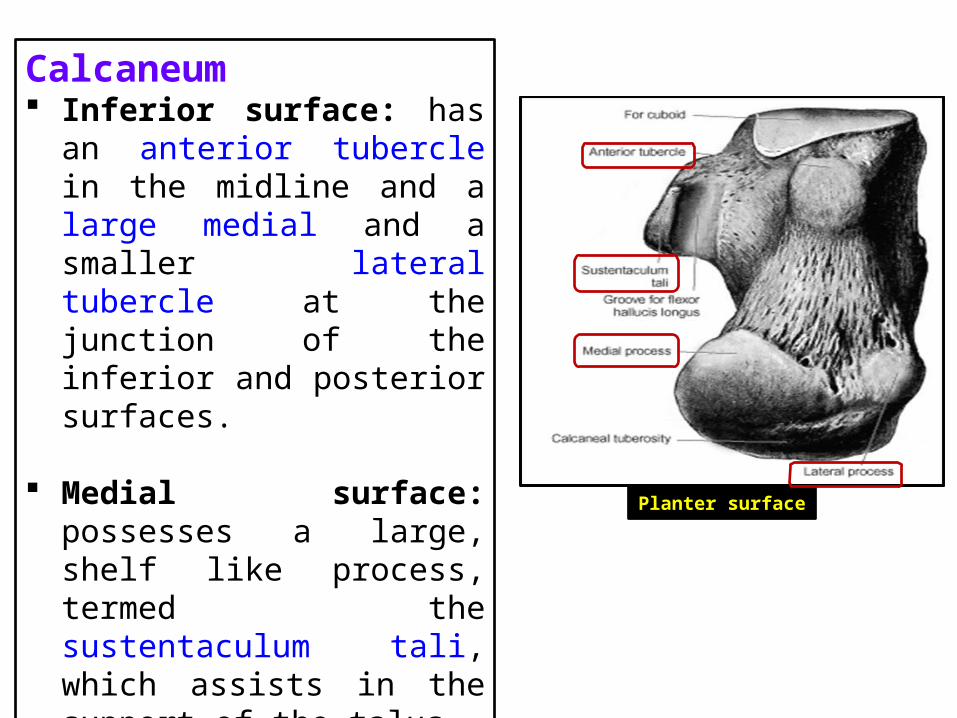
Calcaneum Inferior surface: has an anterior
tubercle in the midline and a large medial and a smaller lateral tubercle at the junction of the inferior and posterior surfaces.
Medial surface: possesses a large, shelf like process, termed the sustentaculum tali, which assists in the support of the talus.
Planter surface
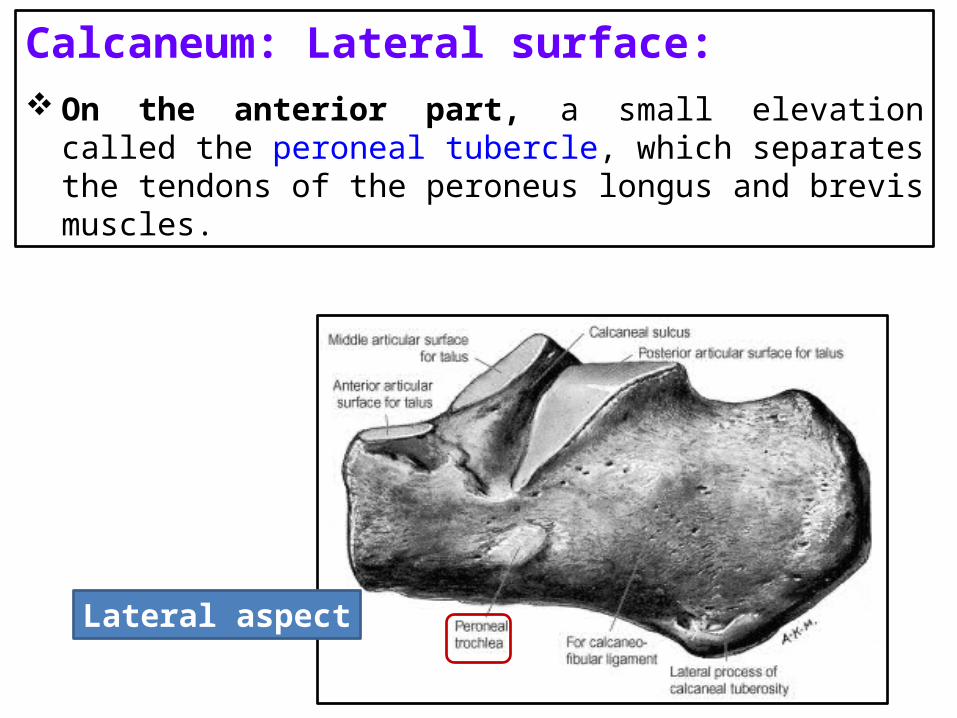
Calcaneum: Lateral surface: On the anterior part, a small elevation called the peroneal
tubercle, which separates the tendons of the peroneus longus and brevis muscles.
Lateral aspect
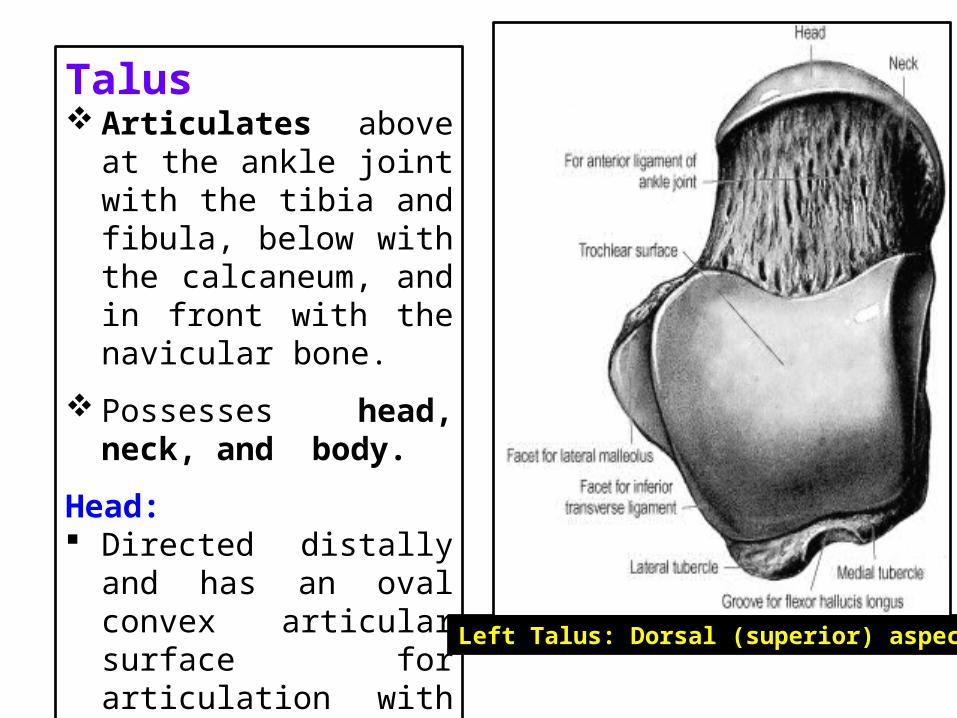
Talus Articulates above at the
ankle joint with the tibia and fibula, below with the calcaneum, and in front with the navicular bone.
Possesses head, neck, and body.
Head: Directed distally and has
an oval convex articular surface for articulation with the navicular bone.
Left Talus: Dorsal (superior) aspect
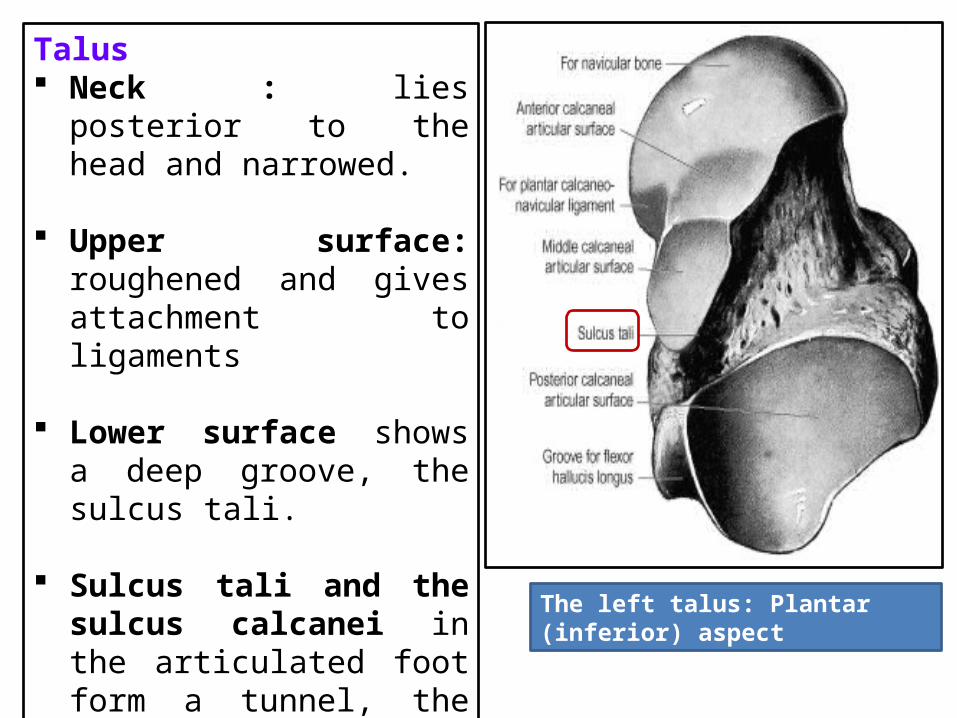
Talus Neck : lies posterior to the
head and narrowed.
Upper surface: roughened and gives attachment to ligaments
Lower surface shows a deep groove, the sulcus tali.
Sulcus tali and the sulcus calcanei in the articulated foot form a tunnel, the sinus tarsi, which is occupied by the strong interosseous talocalcaneal ligament.
The left talus: Plantar (inferior) aspect
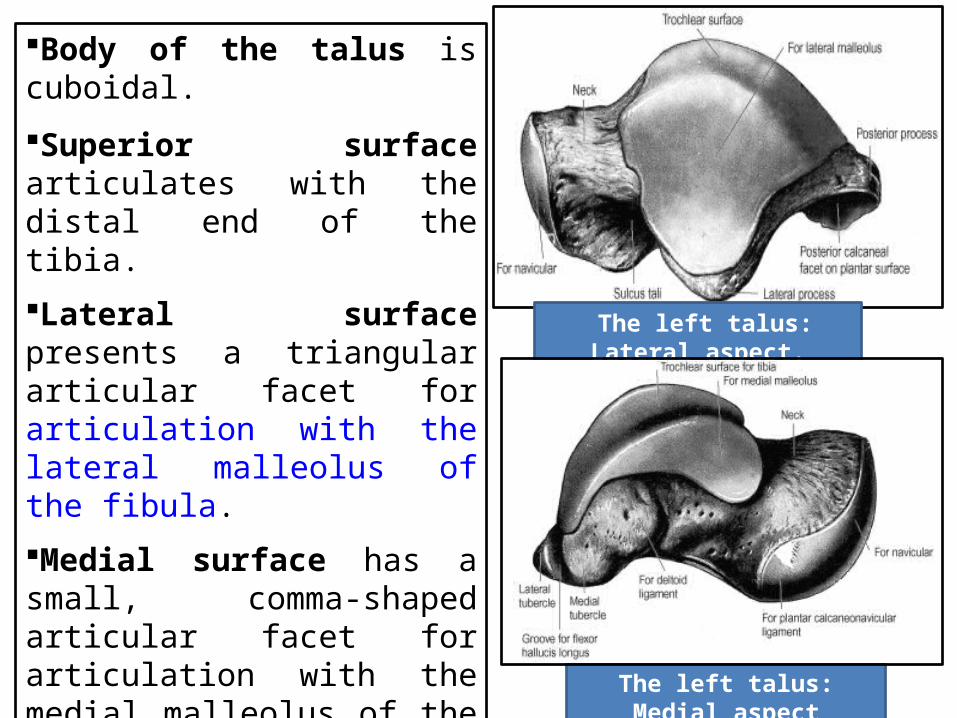
Body of the talus is cuboidal.
Superior surface articulates with the distal end of the tibia.
Lateral surface presents a triangular articular facet for articulation with the lateral malleolus of the fibula.
Medial surface has a small, comma-shaped articular facet for articulation with the medial malleolus of the tibia.
Posterior surface is marked by two small tubercles, separated by a groove for the flexor hallucis longus tendon.
The left talus: Lateral aspect.
The left talus: Medial aspect
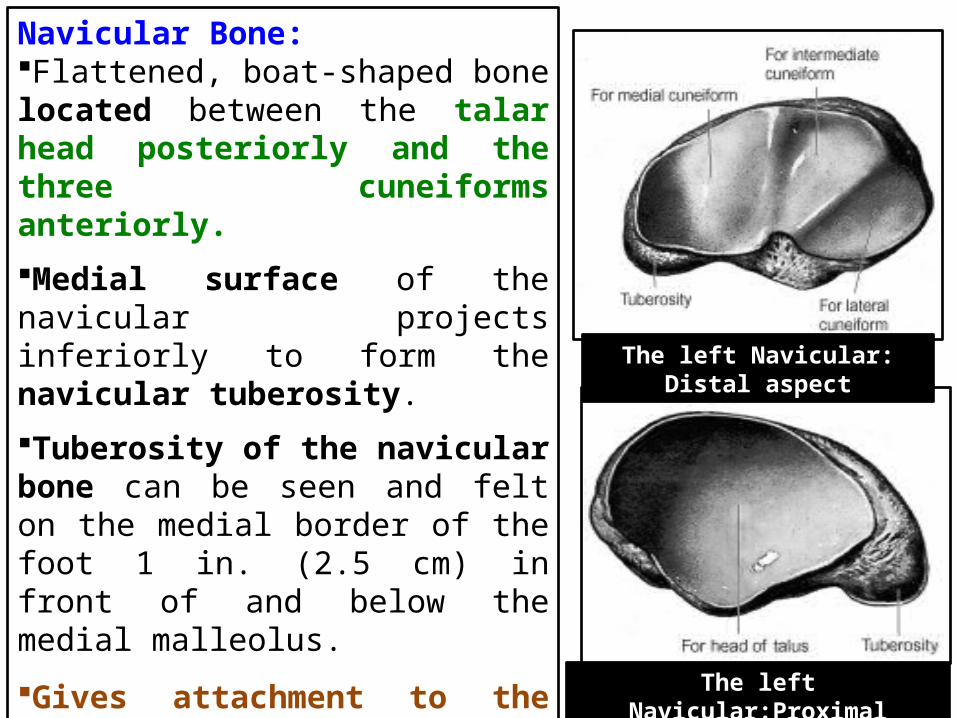
Navicular Bone:Flattened, boat-shaped bone located between the talar head posteriorly and the three cuneiforms anteriorly.
Medial surface of the navicular projects inferiorly to form the navicular tuberosity.
Tuberosity of the navicular bone can be seen and felt on the medial border of the foot 1 in. (2.5 cm) in front of and below the medial malleolus.
Gives attachment to the main part of the tibialis posterior tendon.
If this tuberosity is too prominent, it may press against the medial part of the shoe and cause foot pain.
The left Navicular: Distal aspect
The left Navicular:Proximal aspect.
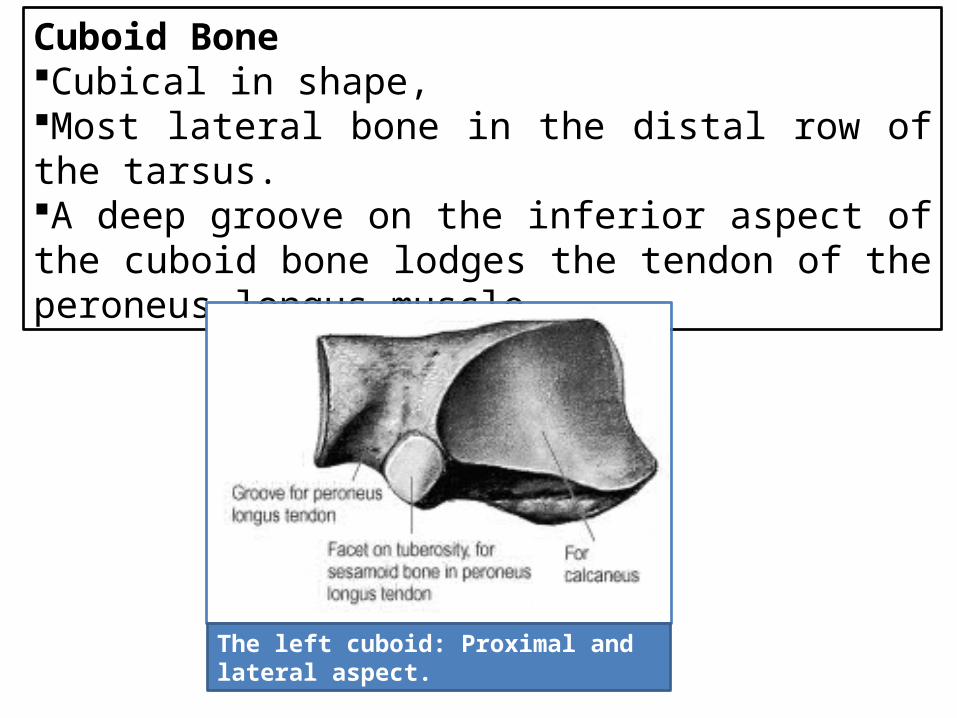
Cuboid BoneCubical in shape, Most lateral bone in the distal row of the tarsus. A deep groove on the inferior aspect of the cuboid bone lodges the tendon of the peroneus longus muscle.
The left cuboid: Proximal and lateral aspect.
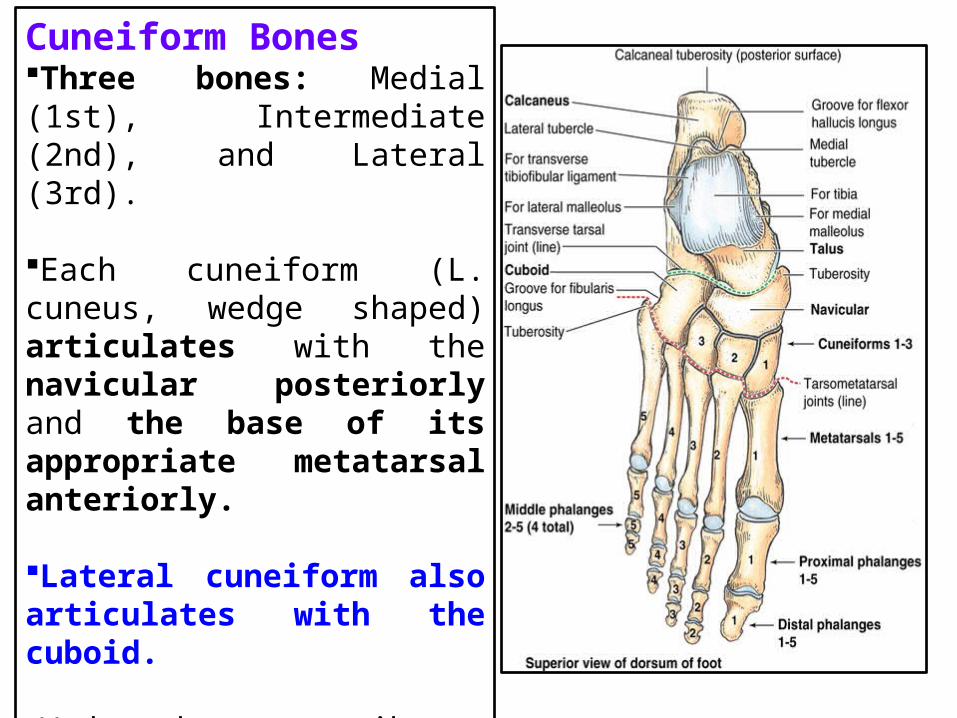
Cuneiform BonesThree bones: Medial (1st), Intermediate (2nd), and Lateral (3rd).
Each cuneiform (L. cuneus, wedge shaped) articulates with the navicular posteriorly and the base of its appropriate metatarsal anteriorly.
Lateral cuneiform also articulates with the cuboid.
Wedge shape contributes greatly to the formation and maintenance of the transverse arch of the foot.
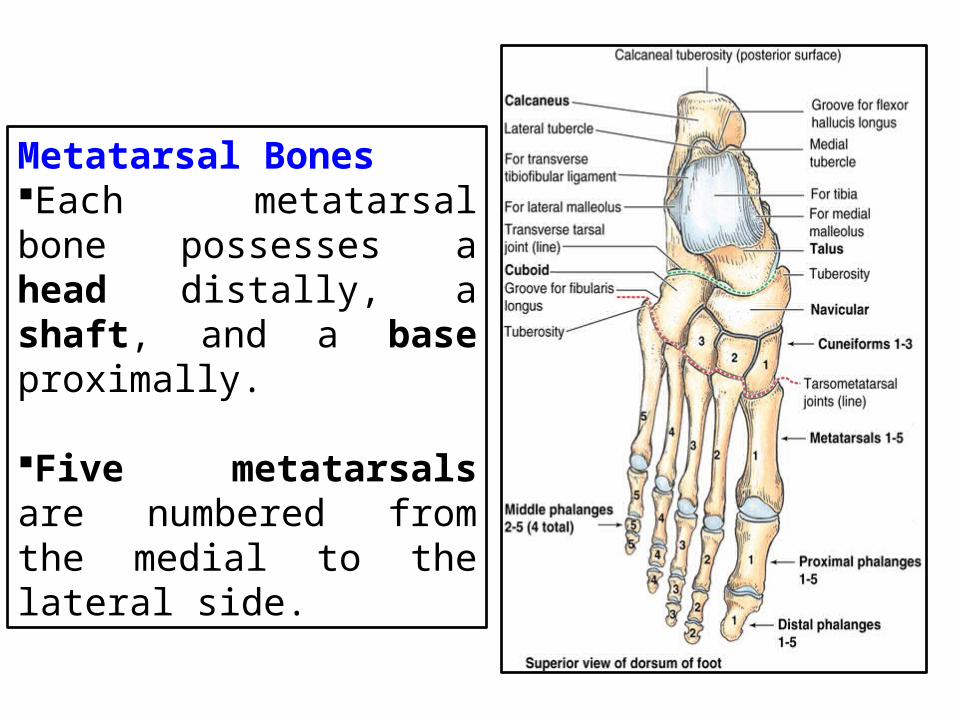
Metatarsal Bones Each metatarsal bone possesses a head distally, a shaft, and a base proximally.
Five metatarsals are numbered from the medial to the lateral side.
Metatarsal Bones
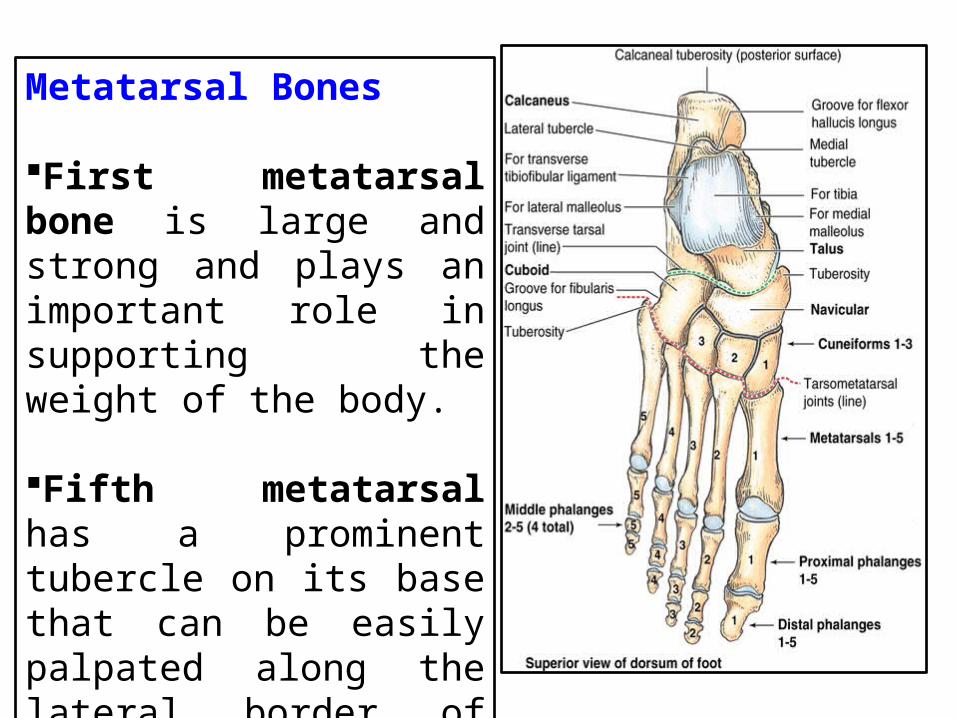
First metatarsal bone is large and strong and plays an important role in supporting the weight of the body.
Fifth metatarsal has a prominent tubercle on its base that can be easily palpated along the lateral border of the foot.
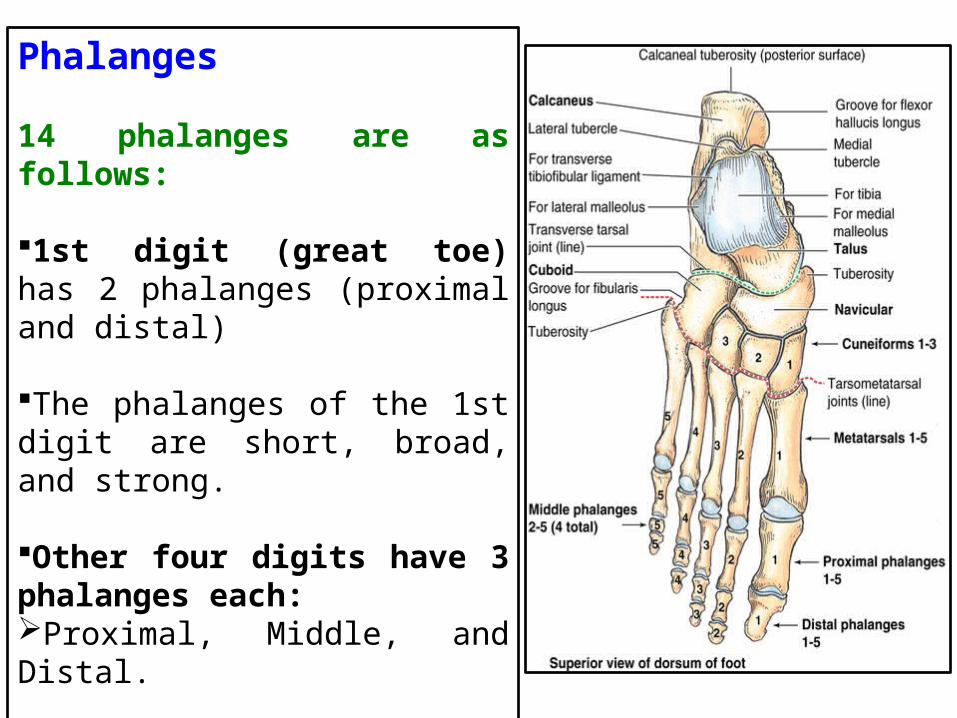
Phalanges
14 phalanges are as follows:
1st digit (great toe) has 2 phalanges (proximal and distal)
The phalanges of the 1st digit are short, broad, and strong.
Other four digits have 3 phalanges each: Proximal, Middle, and Distal.
Each phalanx has a base (proximally), a shaft, and a head (distally).
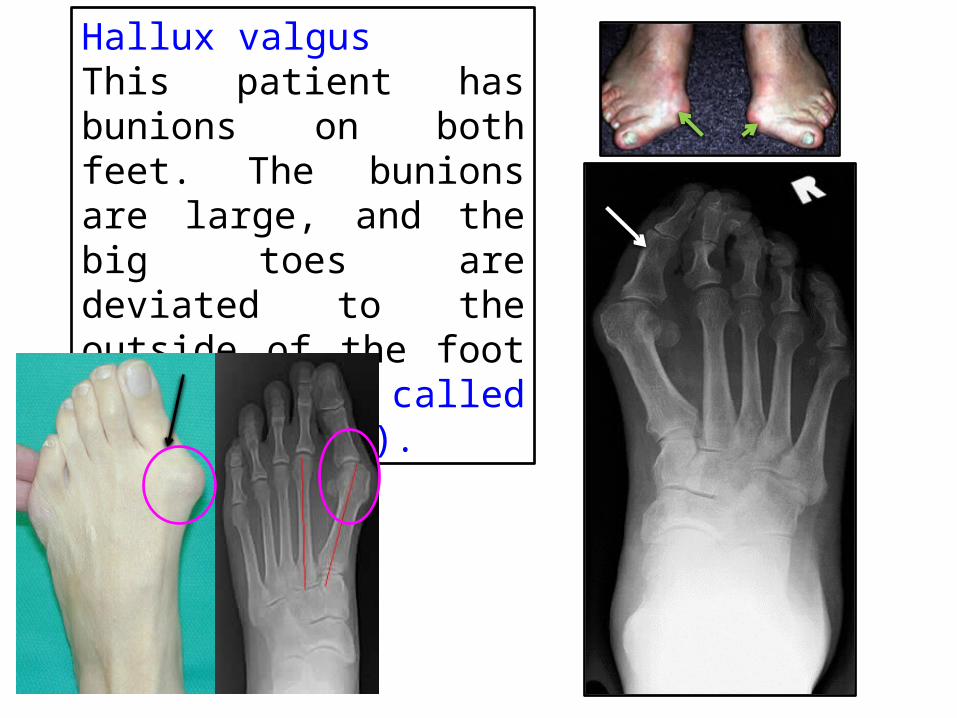
Hallux valgus This patient has bunions on both feet. The bunions are large, and the big toes are deviated to the outside of the foot (this is called hallux valgus).
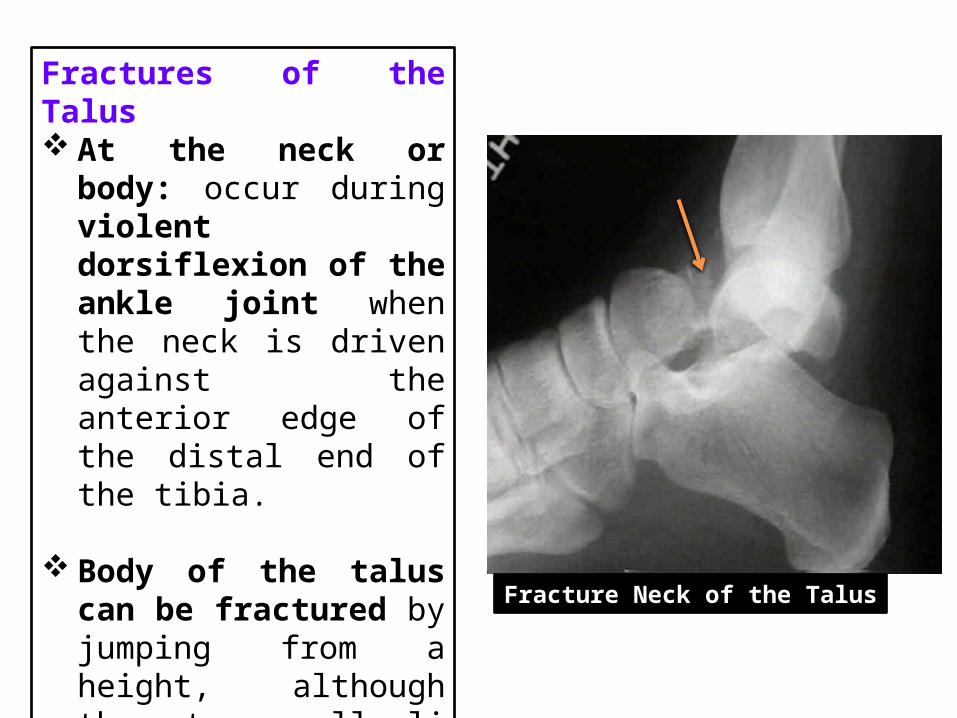
Fractures of the Talus At the neck or body: occur
during violent dorsiflexion of the ankle joint when the neck is driven against the anterior edge of the distal end of the tibia.
Body of the talus can be fractured by jumping from a height, although the two malleoli prevent displacement of the fragments.
Fracture Neck of the Talus
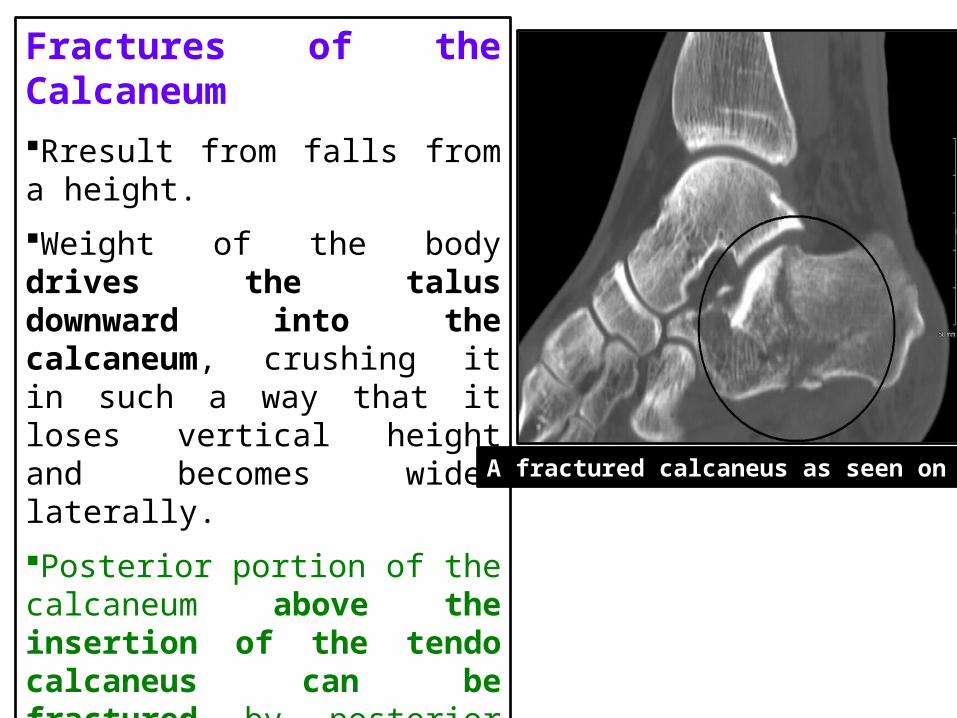
Fractures of the CalcaneumRresult from falls from a height.
Weight of the body drives the talus downward into the calcaneum, crushing it in such a way that it loses vertical height and becomes wider laterally.
Posterior portion of the calcaneum above the insertion of the tendo calcaneus can be fractured by posterior displacement of the talus.
Sustentaculum tali can be fractured by forced inversion of the foot.
A fractured calcaneus as seen on CT
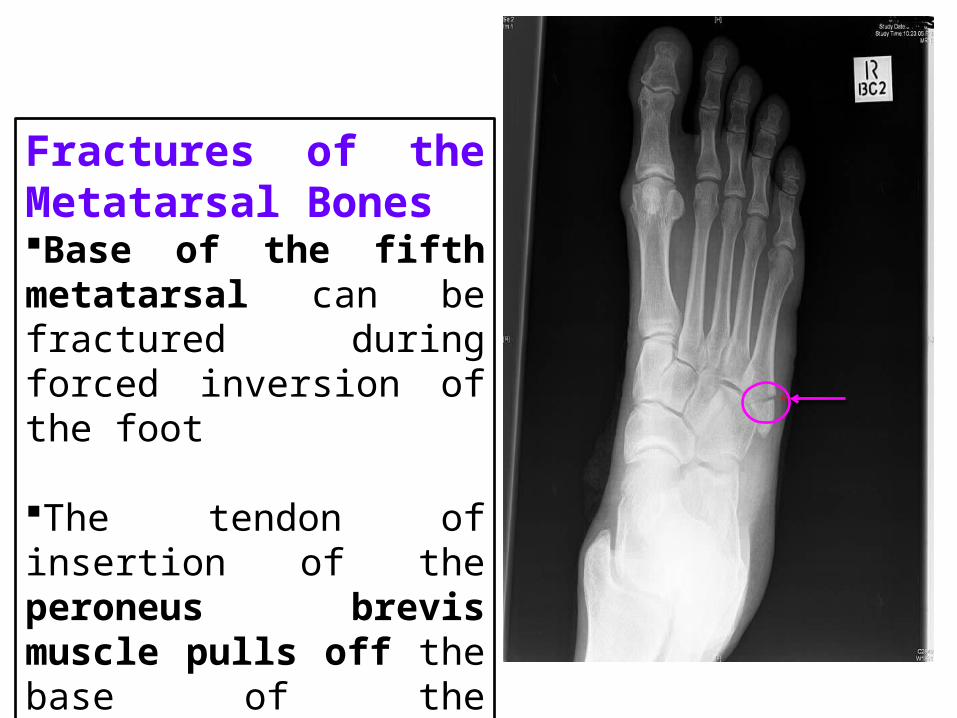
Fractures of the Metatarsal BonesBase of the fifth metatarsal can be fractured during forced inversion of the foot
The tendon of insertion of the peroneus brevis muscle pulls off the base of the metatarsal.
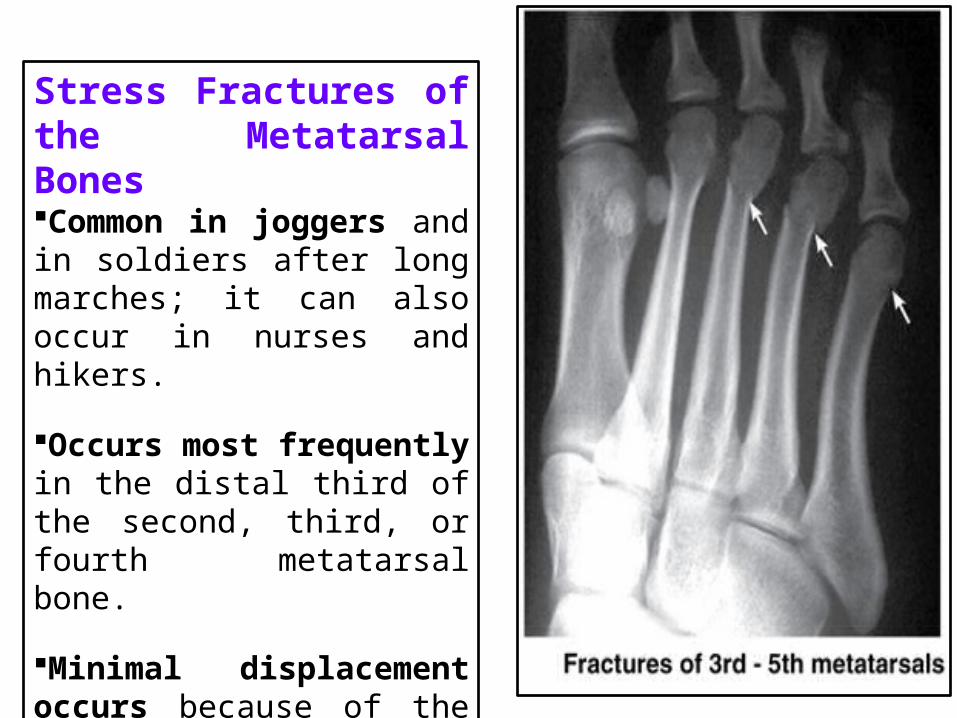
Stress Fractures of the Metatarsal BonesCommon in joggers and in soldiers after long marches; it can also occur in nurses and hikers.
Occurs most frequently in the distal third of the second, third, or fourth metatarsal bone.
Minimal displacement occurs because of the attachment of the interosseous muscles.
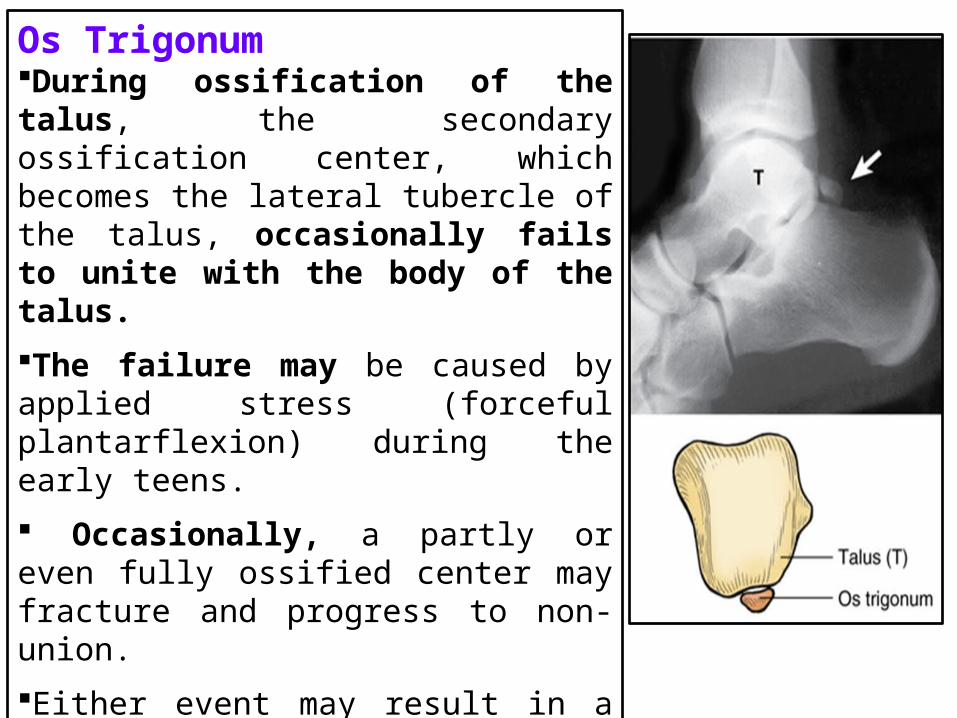
Os TrigonumDuring ossification of the talus, the secondary ossification center, which becomes the lateral tubercle of the talus, occasionally fails to unite with the body of the talus.
The failure may be caused by applied stress (forceful plantarflexion) during the early teens.
Occasionally, a partly or even fully ossified center may fracture and progress to non-union.
Either event may result in a bone (accessory ossicle) known as an os trigonum.
Patients with an os trigonum may be symptomatic or pain free.

Thank you