Embed Size (px)
Citation preview

PHARMACOKINETICS & PHARMACODYNAMICS
Mario Wilmath

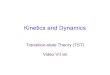
BASIC PK PARAMETERS
LIBERATION
ABSORPTION
DISTRIBUTION
METABOLISM
ELIMINATION
DOSAGE FORM, STABILITY, QUALITY
ROUTE, DOSE
DRUG TARGET, EFFICACY
HALF-LIFE, SAFETY
DURATION, FREQUENCY

Cardiovascular : Lidocaine, procainamide, digoxin
Infectious Disease: Aminoglycosides, vancomycin
Neurology: Phenytoin, carbamazepine, phenobarbital, valproic acid
Oncology: Methotrexate
Pulmonary: Theophylline, aminophylline
Transplant: Cyclosporine, tacrolimus, sirolimus
CLINICAL DRUG MONITORING
Thankful for my healing.com

DOSE & DOSING INTERVALS Intravenous: X0 = C0/Vd
Single IV: Ct future = C0* e-ket Ct past = C0 / e-ket
Multiple IV: Dose= (Cp *Vd)(1-e-nkeτ /1-e-keτ)e-ket
Short-term Infusion (0.5 h), Multiple Dosing:
› R0= CL*Cmax{1-e-keτ /1-e-keT} e-ket 1
› Cmin= Cmax*e-ke(τ -T)
Continuous Infusion (1 h): › R0= CL*Cpss*[1-e-keτ]/1-e-keT 1 ] e-ket 1
› Cmin= Cpss*e-ke(τ -T)
› 2R0/(C1+C2) + 2Vd (C1-C2) )/(C1+C2) (t1-t2)
Loading Dose: LD = Vd*Css / SF
Intermittent IV Bolus: Dose/τ = CL*Cp{1-e-keτ/1-e-keT}*e-ke(τ -T)
Maintenance Dose: MD =CL*Css* τ / SF Oral:
› Multidose: Cave steady state = [LD/Vd*(1-e-keτ)]
› Dose = C*(ka-ke)*Vd/SF*ka* (e-ket-e-kat) Steady State: Multiple doses cause term 1-e-nket 1
Ansel. Dosage Forms.
australianprescriber.com

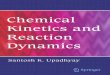
EMPIRIC DOSING - NOMOGRAMS
DIGOXIN
AMINOGLYCOSIDES
THEOPHYLLINERxkinetics.org
A review of clinical use of theophylline in acute asthma: Factors influencing kinetic disposition and drug interactionsOhnishi, A./Methods Find Exp Clin Pharmacol 2000, 22(4): 253ISSN 0379-0355 Copyright 2000 Prous Science CCC: 0379-0355 DOI: 10.1358/mf.2000.22.4.584459
Loading Dose 25 mg/kgMaintenance Dose 19 mg/kg
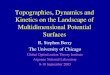
VANCOMYCIN
IBW Ht
Creatinine Clearance

PHYSIOLOGIC PARAMETERS FOR INDIVIDUALIZED THERAPY
1. Body Compartment: Central vs Peripheral2. Body Surface Area3. Weight & Body Composition
• Actual body weight – All Tissues• Ideal body weight - Muscle• Adjusted body weight – Intermediate Distribution
4. Adjustments to PK:• Age• Gender• Disease• Food• Drug Interactions
5. Clinical Endpoint, Surrogate Marker, Lab Measures
6. Toxicity

REFERENCES
1. Allen L, Ansel H, Popovich N. Ansel’s Pharmaceutical Dosage Forms and Drug Delivery Systems. Lippincott Williams & Wilkins. Baltimore, MD, USA. 2005.
2. Bauman JL, et al. “A Method of Determining the Dose of Digoxin for CHF in the Modern Era.” Archives of Internal Medicine. Vol 166, Dec 11/25, 2006.
3. Derendorf H, Hochhaus G, Winkler J. “How the Lung Handles Drugs. Pharmacokinetics and Pharmacodynamics of Inhaled Corticosteroids.” Proceedings of the American Thoracic Society, Vol 1. pp 356-363, 2004.
4. Hendeles L, et al. “Food-induced "dose-dumping" from a once-a-day theophylline product as a cause of theophylline toxicity.” Chest 87.6.758 Vol. 87no. 6 758-765. June 1985.
5. DiPiro JT. Concepts in Clinical Pharmacokinetics.6. Hammerlein, et al. “Age-Related Changes in Drug Metabolism and
Effect.” Clinical Pharmacokinetics, Jul:35(1), 1998.7. Tomlin ME. Pharmacology and Pharmacokinetics- A Basic Reader.
Elsavier, 2010. 8. Images as noted and courtesy of Wikipedia Commons
Bike friendlyarlington.com