Embed Size (px)
DESCRIPTION
Citation preview

Litigation in gynaecologySwati Jha MD FRCOG,a,* Sarah Rowland MA (Oxon)
b
aConsultant Obstetrician and Gynaecologist, and Honorary Senior Clinical Lecturer, Jessop Wing, Sheffield Teaching Hospitals NHSFT, Tree Root
Walk, Sheffield S10 2SF, UKbPartner, Medical Law and Patients’ Rights Team, Irwin Mitchell LLP, Riverside East, 2 Millsands, Sheffield S3 8DT, UK
*Correspondence: Swati Jha. Email: [email protected]
Accepted on 24 September 2013
Key content� Reasons for litigation and pitfalls in patient care.� Knowledge of civil law and basic Acts governing clinical negligence
in a medicolegal claim.� Specific problem areas relating to consent, sterilisation,
laparoscopy, colposcopy, hysteroscopy, urogynaecology
and hysterectomy.� Issues of education, training and clinical governance.
Learning objectives� To understand the anatomy of a claim.� How to avoid litigation.
� What to do when things go wrong.
Ethical issues� Increased litigation leads to clinicians practicing
defensive medicine.� Are patients being exposed to unnecessary investigations and
invasive procedures to prevent clinicians from being sued?� Litigation has an adverse impact on healthcare professionals and
affects recruitment to particular specialties.
Keywords: clinical negligence / litigation / medico-legal /
professional misconduct / risk management
Please cite this paper as: Jha S, Rowland S. Litigation in gynaecology. The Obstetrician & Gynaecologist 2014;16:51–57.
Introduction
Obstetrics and gynaecology has always had a reputation for
being a highly litigious specialty. It is estimated in the USA
that annually 11% of obstetricians and gynaecologists will
face a malpractice suit of which 2.5% will result in a
payout.1,2 The same study showed that over their medical
careers 100% of all obstetricians and gynaecologists will face a
claim for medical negligence.
Within the remit of gynaecology, claims should be brought
within 3 years of the injury or the date of knowledge of clinical
negligence. Where the injured person is a child, the 3-year
period does not begin until they reach their 18th birthday. So,
in effect, a child has until their 21st birthday to bring a claim.
No time limit applies to claimants who lack capacity, as is
often the case in birth injury cases. If an adult dies as a result of
their medical treatment, their personal representatives or
dependants may bring a claim within 3 years of the date of
their death.
Why do doctors get sued?
A study by Vincent et al.3 demonstrated that the four main
reasons for litigation are:
� Accountability: when things go wrong someone should be
held accountable for their actions.
� The need for an explanation: to know how the injury
happened and why.
� Concern with standards of care: the desire to prevent
similar accidents in the future.
� Compensation for actual losses, pain and suffering or the
provision of future care for an injured person.
However, Vincent et al. and several other studies have also
shown that the decision to take legal action is determined not
only by the original injury, but also by failure to provide
information, an explanation and an apology. Insensitive
handling of an injury and poor communication after the
original incident increases the risk of litigation and erodes the
patient–doctor relationship.
Anatomy of a claim
The various medical defence organisations (NHS Litigation
Authority [NHSLA], Medical Defence Union [MDU],
Medical Protection Society [MPS]) receive several thousand
new claims per year but very few reach court (1–2%).
Irrespective of outcomes, being sued is a distressing
experience. It is reassuring to know that the chances of
ending up in court are relatively slim and there is a 70%
chance that cases are successfully defended. A claim goes
through various stages before it will be dropped, settled out of
court, or successfully defended or claimed. It is usually up to
ª 2014 Royal College of Obstetricians and Gynaecologists 51
DOI: 10.1111/tog.12065
The Obstetrician & Gynaecologist
http://onlinetog.org
2014;16:51–57 Review

three years from the point a claim is made that cases will reach
a courtroom (trial). The stages of a claim leading up to and
different aspects of a trial are described in Table 1.
Key cases that have influencedmedico-legal rulings
Bolam v Friern Hospital Management Committee4
The Bolam principle formulated that a medical professional is
not considered negligent if his practice reflects that of an
accepted body of responsiblemedical opinion at that time. This
is in spite of other doctors at that time adopting a different
practice. This means that the standard of care is a matter of
medical judgement, even though the law imposes thedutyof care.
Bolitho v City and Hackney Health Authority5
The Bolitho principle subjects expert evidence to close judicial
scrutiny. The court is not bound to accept that a doctor
escapes liability for a treatment or diagnosis purely on the
grounds that other medical experts are of the opinion that
the defendant’s actions were in accordance with sound
medical practice. The court has to be satisfied that the
exponents of the body of opinion relied upon can
demonstrate that such opinion has a logical basis. The
experts must question comparative risks and benefits and
have reached a defensible conclusion on the matter.
Roe v Minister of Health6
The Roe ruling stated that a defendant may not be liable
provided he acted in accordance with medical knowledge
available at the timeof the incident rather than the timeof the trial.
Ashcroft v Mersey RHA7
The burden of proof lies with the claimant to prove that on
the balance of probabilities the defendant was negligent.
Hunter v Hanley8
Departure from routine practice does not automatically
constitute negligence.
Crawford v Board of Governors of Charing CrossHospital9
The standard of medical knowledge and its application
will not be judged on the basis of publication in isolated
medical journals.
Wilsher v Essex Area Health Authority10
The standard of care is reliant on the post occupied by a
doctor, not the level of training. Where multiple causes
resulted in an adverse outcome it is for the claimant to prove
that “But For” the defendant’s actions the damage would not
have occurred.
Chester v Afshar11
Patients should be told of any possible significant adverse
outcomes of a proposed treatment. A patient has a prima
facie right to be informed by a surgeon of a small, but
well-established, risk of serious injury as a result of surgery;
even if it would not have changed the claimant’s decision to
proceed with the treatment.
Janaway v Salford Health Authority12
Doctors who object to participating or being involved in the
process of termination of pregnancies should make these
opinions known to patients and give them an opportunity to
see another clinician without undue delay if that is what the
patient desires.
The definition of ‘participating’ has been subjected to
considerable scrutiny in this case. The General Medical
Council (GMC), in the current edition of Good Medical
Practice goes on to state ‘the doctor must ensure that
arrangements are made for another suitably qualified
colleague to take over this role so that the patient’s care
does not suffer’.
Gillick v West Norfolk & Wisbeach Area HealthAuthority13
This ruling meant that children under 16 years of age could
be deemed as competent if for a particular decision they
understood the problem and its implications, risks and
benefits of treatment, consequences if not treated, the
alternative options and implications on the family. They
need also to be able to retain (remember) the information,
weigh the pros and cons and communicate a reasoned
decision about their wishes.
Fraser ruling14
Lord Fraser, in his ruling of the the Gillick case in the House
of Lords produced guidelines with regard to contraceptive
Table 1. Anatomy of a claim
Pre-Trial Trials
Stage 1: Letter before action Practicalities and the mediaStage 2: Letter of claim Court proceedingsStage 3: The response JudgementStage 4: Formal proceedings begin Damages and costsStage 5: Track allocationa AppealsStage 6: Your witness statement A security blanketb
Stage 7: Exchange of expertwitness reports
Stage 8: Expert joint meetings
aCourts allocate a claim to one of three tracks. This depends oncomplexity of the case and its value. This could be small claims, afast track or a multi track. Most clinical negligence cases fall in thecategory of ‘multi-track’.bDefence organisations provide both financial indemnity andspecialist advice and support for doctors facing a trial.
52 ª 2014 Royal College of Obstetricians and Gynaecologists
Litigation in gynaecology

advice given by doctors. Doctors can proceed to advise
and treat patients provided they are satisfied by the
following criteria:
1. ‘that the girl (although under the age of 16 years of age) will
understand advice;
2. that they cannot persuade her to inform her parents or to
allow them to inform the parents that she is seeking
contraceptive advice;
3. that she is very likely to continue having sexual intercourse
with or without contraceptive treatment;
4. that unless she receives contraceptive advice or treatment her
physical or mental health or both are likely to suffer;
5. that her best interests require them to give her contraceptive
advice, treatment or both without the parental consent.’
Medical indemnity
Gynaecologists employed by the NHS receive indemnity
against claims for clinical negligence handled by the NHSLA.
Whereas NHS vicarious liability covers clinical negligence
claims, it would not cover coronal enquiry or GMC
proceedings so all active clinicians should still have defence
cover. Those working in the private sector will need
insurance through defence organisations such as the MDU
or MPS. The NHSLA manages clinical negligence and other
claims made against the NHS in England on behalf of its
member organisations. Other activities include improving
safety for patients and staff, sharing learning about risks and
standards in the NHS and resolving disputes fairly. The
NHSLA is also responsible for handling issues relating to
equal pay claims and investigating and advising the NHS on
human rights case law.
In 2011–12 the annual NHS bill for clinical negligence
claims reached £1.28 billion. This was a 45% rise from the
previous year’s total of £863 million. Though the total
number of claims for clinical negligence is the highest in
surgery, the value of payouts are greatest for obstetrics and
gynaecology of which the large proportion is related to
obstetric payouts.15
When a successful claim is made, two elements constitute
a compensation award. The first is financial compensation
for pain and suffering caused by the injury and is called
general damages. This may include an element to represent
a person’s inability to do things after the medical incident
that they could do before the incident. General damages
awarded are assessed using guidelines given to judges and
precedents from previous cases. The second element is
known as special damages and is compensation for past and
future losses and expenses. In a clinical negligence claim
compensation is based on outcomes had the treatment been
a success. Most often, clinical negligence cases are settled
out of court.
Aetiology of claims in gynaecology
A case of clinical negligence requires four elements are met:
� duty arising out of the physician–patient relationship,� a breach of that duty (i.e., deviation from the accepted
standard of care),
� a link between that breach of duty, and
� a specific harm that has occurred.
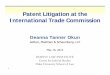
With regard to gynaecology, common causes of claims are
shown in Figure 1 and specific injuries leading to claims are
shown in Figure 2. These are NHSLA data for 2012 hence
exclude claims made to and defended by private insurers
such as the MDU or MPS. In 2012, 504 claims were coded
under gynaecology, 75 were closed with no payout and 51
were closed with payment. A total of £810,888.90 (excluding
costs) was paid in damages.
Common areas of litigation in gynaecology
ConsentWith the exception of cancer patients, in gynaecology most
patients are healthy with problems relating to quality of life.
Most surgery is elective. The expectations of these patients are
therefore high, and litigation is often related to whether these
expectations have been met. Both the GMC and the Royal
College of Obstetricians and Gynaecologists (RCOG) provide
guidance on obtaining consent.16,17 A signature on a consent
form does not equate to valid consent. The purpose is to record
the patient’s decision and also the discussions that have taken
place. Before seeking a woman’s consent for a test, treatment,
0 20 40 60 80 100 120
Wrong/failed/delayeddiagnosis
Number of claims
109
99
105
28
22
15
21
105
Intraoperative problems
Inappropriate/failed/delayed treatment
Failure to obtain informed consent
Failure to recognise complication
Foreign body left in situ
Failure to performoperation/ tests
Others
Figure 1. Gynaecological claims by cause between 01 January 2012and 31 December 2012. Unpublished data provided by Mr John Meadand Ms Esther Kaikai of the NHSLA.
ª 2014 Royal College of Obstetricians and Gynaecologists 53
Jha and Rowland

intervention or operation, it is important to ensure that she
understands the nature of the condition for which it is being
proposed, its prognosis, i.e. benefits and risks inherent to the
procedure, likely consequences and the risks of receiving no
treatment, what can realistically be expected following surgery
as well as any reasonable or accepted alternative treatments.16 A
discussion of the risks associated with a clinical decision is a
critical element of an informed decision. Research has not yet
identified best practices for communicating uncertainty about
harms and benefits of treatment to patients.18 Uncertainties
should be discussed. Litigation related to consent may also arise
from the performance of procedures that were not discussed
with the patient i.e. removal of both ovaries when consented to
removal of one or none.
SterilisationThe most common ground for litigation arising from a
sterilisation is conception post-sterilisation. This could be a
luteal phase pregnancy which was not identified at the time
of surgery or an actual failure because the procedure was
inappropriately or inadequately performed or recanalisation
of the fallopian tubes occurred after the procedure. If
pregnancy occurs within 12 months of sterilisation it is
likely to be a failure of the technique whereas after 12 months
it is more likely to be recanalisation. The shortest interval
between operation and conception was three months and the
longest 17 years.19 There are also recorded cases of litigation
because of failure to perform procedures concurrently for
which the patient has consented, such as removal of an
IUCD. More serious was non-consented tubal sterilisation
performed at caesarean section (CS), or regret related to
sterilisation done at the time of CS when the patient was
consented immediately before the procedure. Inadvertent
injury during the procedure or injury related to the method
of tubal occlusion, such as bowel injury due to cautery, are
other causes of litigation during sterilisation.
Medico-legal law relating to maintenance of the child born
after sterilisation is controversial. In the McFarlane20 ruling it
was held that parents of healthy children born after
sterilisation were not entitled to the costs of bringing up
the child. However, a valid claim can be made following the
birth of child with disabilities, based on the additional cost of
raising a child with those disabilities (Parkinson21).
LaparoscopyClaims arising from laparoscopic procedures may be related to
a variety of different issues. They may arise from an allegation
of a lack of training or because a case performed
laparoscopically would have been done by a more
experienced body of clinicians as a laparotomy and
complications arose as a result of the wrong choice of surgery.
But the most common cause of litigation related to
laparoscopy is internal injury or a delay in recognition of
these complications. The initial laparoscopic entry into the
peritoneal cavity remains the major contributor to bowel
injury anddelayed recognitionwas amajor factor in assessment
of liability.22 These cases can be difficult to defend, particularly
if the patient’smedical records do not document that they have
been closely monitored and any deterioration in their
condition managed in a timely and appropriate fashion. The
need to proceed to a laparotomy, particularly a midline
incision as opposed to a transverse incision, also increased the
risks of litigation. Unlike a laparotomy, where patients should
be seen to improve on a daily basis, in laparoscopic surgery they
should be improving on an hourly basis.
Management of patient expectations helps ensure that they
are satisfied with their care and there is early recognition of
warning signs of complications post-surgery.
Recommendations to avoid complications during
operative laparoscopy include the following:
� The best possible vision should be maintained at all times.
� The use of sharp instruments should be avoided unless
absolutely necessary.
� The use of diathermy, or ultrasonic devices require
knowledge of their use and utmost care. The tip of the
instrument may remain hot even if the power has been
switched off.
� Rule out bowel injury after primary trocar insertion.
� On completion of the procedure and when removing
trocars, check all areas where injury to tissue or bleeding
may have occurred.
� All trocar sites should be inspected after withdrawal by
lightly placing a finger over the skin wound at the time so
0 50 100 150 200
Bladder damage/94
64
80
32
14
24
19
177
Additional/unneces-sary operation(s)
Unnecessary pain
Bowel damage/dysfunction
Perforation
Cancer
Psychiatric/psy-chological damage
Others
Number of claims
Figure 2. Gynaecological claims by injury between 01 January 2012and 31 December 2012. Unpublished data provided by Mr John Meadand Ms Esther Kaikai of the NHSLA.
54 ª 2014 Royal College of Obstetricians and Gynaecologists
Litigation in gynaecology

that any bleeding will run into the abdominal cavity and
be identified.
� Use a drain when necessary.
� Patients should be given appropriate contact details and
instructed to contact the hospital if problems
occur postoperatively.
ColposcopyLitigation related to colposcopy can arise from physician
errors or laboratory errors. The common physician errors
that lead to claims of clinical negligence include improper
sampling, improper identification or failure to obtain a
complete history and incomplete follow-up. Laboratory
errors leading to litigation may be due to improper smear
processing including identification, staining and reviewing of
history of previous Pap smears as well as incorrect
interpretation by a cytologist. Lack of training and
supervision of a cytologist and improper recommendations
by a cytologist can also be causes of litigation.
HysteroscopyLitigation in part is related to a failure of clinicians to adapt to
the demands of newer technologies, lack of adequate expertise
when performing complicated procedures and failure to
recognise complications during relatively simple procedures.
Clinical negligence claims related tohysteroscopic procedures
include complications related to uterine perforation and
subsequent internal organ injury. The failure to recognise the
complication is the commonest cause of litigation.When there
has been internal organ damage, such as bowel, patients may
remain asymptomatic for 2–10 days before the nature of the
injury, often thermal, becomes apparent.
Factors that increase the risk of perforation include
cervical stenosis, acute anteversion or retroversion,
lower-segment fibroids or intrauterine synechiae and
operator inexperience.23,24 Uterine injury without the use
of an electrical source can usually be managed by observation
of signs of vaginal or intraperitoneal bleeding.23,25 However,
where an electrical source has been used, laparoscopy is
advised to rule out bowel injury.
Fatal complications to which the clinician should be alert
during hysteroscopy include:
� fluid overload causing hyponatraemia and subsequent
respiratory arrest and seizures,
� air embolism leading to collapse and death. Though
relatively rare, this has been recorded and both the surgeon
and anaesthetist must be alert to the signs suggestive of this
rare but fatal complication.
UrogynaecologyIncreasingly, litigation related to urogynaecology cases are
centred on the use of meshes and related complications.
Following the class action against Johnson & Johnson vaginal
mesh kits in the US, Johnson & Johnson publicly declared
their decision to withdraw their vaginal meshes by the first
quarter of 2013, and this was followed by a sharp decline in
the use of vaginal meshes elsewhere including the UK. With
the first cases now going to court in the US and already
worth several million pounds, this could well be a minefield
waiting to explode. Clinicians undertaking synthetic meshes
for the treatment of pelvic organ prolapse should familiarise
themselves with NICE guidance on the use of meshes
interventional procedure guidelines (IPG) 267, 280, 281, 282,
283 and 28426–31 and those performing urinary continence
procedures with IPG 138, 154, 133 and 262.32–35 Cases of
vaginal or abdominal mesh and all secondary prolapse
repairs should ideally be discussed at a multidisciplinary
team meeting and management of all patients undergoing
relatively new procedures should adhere to the principles of
clinical governance and risk management. This will serve to
protect clinicians against litigation related to the use of
meshes. However, the primary factor is adequate training of
clinicians performing these procedures.
General gynaecologists must also be aware that without a
sufficient workload, continuing to perform complicated
urogynaecology procedures is fraught with the risk of litigation.
HysterectomyUreteric injury is the most common cause of litigation related
to hysterectomy. Though a known complication of a difficult
hysterectomy, failure to detect these injuries often leads to a
successful claim. Damage to the bladder and bowel are
probably more common but are not generally considered to
be negligent, especially if the procedure is difficult due to
scarring from a previous surgery. It is important that the
injury is recognised and has been appropriately repaired. In
such cases, a successful claim for compensation is unlikely.
However if the injury to the bladder is missed, a
vesico-vaginal fistula may be formed and a missed bowel
injury could result in sepsis or peritonitis. These will
frequently be classed as negligent. It may be argued that
some occur because of ischaemic necrosis in the bladder base,
and these may be defensible. Therefore, timing of onset of the
leakage is important. Early leak is probably a result of direct
injury whereas later leak is a sequel of ischaemia.
Litigation may also be related to unnecessary hysterectomy
or an oopherectomy. Questions relating to the indication for
surgery can arise particularly when a hysterectomy is
associated with complications and less invasive options
such as an intrauterine contraceptive or an ablation have
not been offered or discussed.
Foreign bodyRetained foreign bodies are classified as SUIs (serious
untoward incidents) and inevitably result in a payment of a
ª 2014 Royal College of Obstetricians and Gynaecologists 55
Jha and Rowland

negligence claim. They can arise from a simple failure to count
swabs and instruments to forgotten pessaries or removal of one
pack where two were inserted. They have been shown to be a
particular problem after long and complicated procedures.
Ethical issues
A recent survey of MPS members demonstrated that 73% felt
their practice was defensive for fear of litigation.36 As a result
of increasing litigation additional and unnecessary tests are
performed.37 These can be invasive and potentially harmful
for the patient but also drive up healthcare costs as their need
is questionable.
The second aspect of litigation is the impact on the
healthcare professional. A malpractice suit can have the same
impact as a major illness, loss of a loved one or a severe career
setback.38 It has adverse emotional consequences and often
involves the stages of grief as described by K€ubler-Ross. It can
cause irritability, headache, insomnia, difficulty with
concentration, clinical depression and suicide.38
There has been an increasing reluctance to join specialities
prone to litigation and obstetrics and gynaecology is one of
these.39,40 The fear of litigation is even becoming a deterrent for
doctors to assist people involved in emergency situations such
as in an accidents or on a flight as the medical practitioner
is open to being sued by the affected or injured person if
the outcome is less than optimal. There is therefore a direct
conflict of professional obligations and a reluctance to be
involved in a situation that can land the clinician in a court
room.
Avoiding litigation
The basic principles of avoiding litigation include:
Good documentationThe old saying ‘if it’s not in the record, it didn’t happen’ still
holds true. Good record keeping includes:
� information provided by the patient that factored in to the
diagnoses or treatment decisions,
� the physical findings or laboratory results that factored in
to decisions,
� the treatment selected, and
� anticipated follow-up.
Restraints of time sometimes make such detailed
discussions difficult.
Good communicationPossibly more important than high standards of care is good
communication with the patient and valid informed consent.
Informed consent is a dialogue, not a lecture. It requires
physicians to discuss:
� risks of the treatment,
� benefits of the treatment, and
� alternatives to the treatment including doing nothing as
well as pros and cons of the individual treatment options.
Any risks associated with serious long-term sequelae,
must be discussed, even if the probability of the risk
occurring is remote.
Accurate representationIt is imperative that clinicians do not misrepresent their
experience. A doctor’s greatest asset is their advanced training
and experience, but it is important to work within that remit.
It is also important to give patients realistic expectations
about their outcomes.
Discharge instructionsIncreasingly, procedures are being performed as day cases
and inpatient stay is shorter than ever before. Discharge
instructions should therefore address all areas of potential
concern, including pain, wound care, and signs of infection.
There should also be information regarding whom to contact
if there is a change in condition or if there are any
further questions.
Saying sorryDoctors are human and errors will sometimes happen. Taking
responsibility doesn’t mean admitting negligence. It means
acknowledging a complication when it occurs and hopefully
minimising the consequences.41 This will sometimes involve
transferring care to another physician. When things go wrong
the vastmajority of people just want two things: an explanation
and an apology.
This is also one of the recommendations of the Francis
report.42 In keeping with a Duty of Candour the report states:
‘Every healthcare organisation and everyone working for
them must be honest, open and truthful in all their dealings
with patients and the public, and organisational and
personal interests must never be allowed to outweigh the
duty to be honest, open and truthful.’
IntegrityExpectations of physicians to act with integrity means that
higher standards of conduct are placed on the medical
profession. A physician should not allow their own interests
to influence a patient’s treatment.
Conclusion
Attention to issues such as continuing professional
development, audit of outcomes and complications,
supervision in theatres, preoperative safety checklists,
56 ª 2014 Royal College of Obstetricians and Gynaecologists
Litigation in gynaecology

effective risk management and attention to safety issues form
the basis of good clinical practice. These will be further
reinforced through the revalidation process.MacLennan et al40
described some key strategies to reduce litigation related to
cerebral palsy, however these measures are applicable to all
cases of litigation related to clinical negligence.
In spite of the best intentions, high standards of care,
and attention to all issues discussed, litigation claims may
still be made. Individual awareness and adequate support
is the basis of coming through these stressful situations
with one’s enthusiasm and zeal for continuing in the
profession intact.
Disclosure of interestsNone declared.
AuthorshipSJ conceived the article, acquired and analysed data, drafted
the article and revised it critically before final approval of the
version to be published. SR drafted the article and revised it
critically before final approval of the version to be published.
AcknowledgementsWe would like to thank Mr John Mead and Ms Esther Kaikai
of the NHSLA for providing the relevant data.
References
1 Jena AB, Seabury S, Lakdawalla D, Chandra A. Malpractice risk according tophysician specialty. N Engl J Med 2011;365:629–36.
2 Seabury SA, Chandra A, Lakdawalla DN, Jena AB. On average, physiciansspend nearly 11 percent of their 40-year careers with an open, unresolvedmalpractice claim. Health Aff (Millwood) 2013;32:111–9.
3 Vincent C, Young M, Phillips A. Why do people sue doctors? A study ofpatients and relatives taking legal action. Lancet 1994;343:1609–13.
4 Bolam v Friern Hospital Management Committee [1957] 1 WLR 5825 Bolitho v City and Hackney Health Authority [1997] 4 All ER 7716 Roe v Minister of Health [1954] 2 All ER 1317 Ashcroft v Mersey RHA [1983] 2 All ER 2458 Hunter v Hanley [1955] SC 2009 Crawford v Board of Governors of Charing Cross Hospital [1953] The Times,
8 December, CA.10 Wilsher v Essex Area Health Authority [1988] AC 107411 Chester v Afshar [2004] UKHL 41; [2005] 1 AC 134; [2004] 3 WLR 927;
[2004] 4 All ER 587; Times, October 19, 200412 Janaway v Salford Health Authority [1989] AC 53713 Gillick v West Norfolk & Wisbech Area Health Authority [1985] UKHL 714 National Society for the Protection of Cruelty to Children. Gillick
Competency and Fraser Guidelines. NSPCC Factsheet. London: NSPCC;2012 [http://www.nspcc.org.uk/inform/research/questions/gillick_wda61289.html].
15 NHS Litigation Authority. Ten Years of Maternity Claims. NHS LitigationAuthority: An Analysis of NHS Litigation Authority Data. London; 2012.
16 Royal College of Obstetricians and Gynaecologists. Obtaining ValidConsent. London: RCOG; 2008 [http://www.rcog.org.uk/files/rcog-corp/CGA6-15072010.pdf].
17 General Medical Council. Consent: Patients and Doctors Making DecisionsTogether. London: GMC; 2008 [http://www.gmc-uk.org/static/documents/content/GMC_Consent_0513_Revised.pdf].
18 Royal College of Obstetricians and Gynaecologists. Presenting Informationon Risk. London: RCOG; 2008 [http://www.rcog.org.uk/files/rcog-corp/CGA7-15072010.pdf].
19 Bender S. Grounds for litigation in regard to tubal sterilisation. TheObstetrician & Gynaecologist 2000;2:53–4.
20 McFarlane v Tayside HB [1999] 3 WLR 130121 Parkinson v St James’ [2001] 3 All ER 97.22 Vilos GA. Laparoscopic bowel injuries: forty litigated gynaecological cases in
Canada. J Obstet Gynaecol Can 2002;24:224–30.23 Cooper JM, Brady RM. Intraoperative and early postoperative complications
of operative hysteroscopy. Obstet Gynecol Clin North Am 2000;27:347–66.24 Jansen FW, Vredevoogd CB, van Ulzen K, Hermans J, Trimbos JB,
Trimbos-Kemper TC. Complications of hysteroscopy: a prospective,multicenter study. Obstet Gynecol 2000;96:266–70.
25 Isaacson KB. Complications of hysteroscopy. Obstet Gynecol Clin North Am1999;26:39–51.
26 National Institute for Health and Clinical Excellence. Surgical Repairof Vaginal Wall Prolapse Using Mesh (IPG 267). London: NICE; 2008 [http://www.nice.org.uk/nicemedia/live/11363/41024/41024.pdf].
27 National Institute for Health and Clinical Excellence. InfracoccygealSacropexy Using Mesh for Uterine Prolapse Repair (IPG 280). London: NICE;2009 [http://www.nice.org.uk/nicemedia/live/11913/42957/42957.pdf].
28 National Institute for Health and Clinical Excellence. InfracoccygealSacropexy Using Mesh for Vaginal Vault Prolapse Repair (IPG 281). London:NICE; 2009 [http://www.nice.org.uk/nicemedia/live/11163/42964/42964.pdf].
29 National Institute for Health and Clinical Excellence. Insertion of MeshUterine Suspension Sling (including Sacrohysteropexy) for Uterine ProlapseRepair (IPG 282). London: NICE; 2009 [http://www.nice.org.uk/nicemedia/live/11311/42862/42862.pdf].
30 National Institute for Health and Clinical Excellence. Sacrocolpopexy UsingMesh for Vaginal Vault Prolapse Repair (IPG 283). London: NICE; 2009[http://www.nice.org.uk/nicemedia/pdf/ipg283guidance.pdf].
31 National Institute for Health and Clinical Excellence. Sacrocolpopexy withHysterectomy Using Mesh for Uterine Prolapse Repair (IPG 284). London:NICE; 2009 [http://www.nice.org.uk/nicemedia/live/12054/42892/42892.pdf].
32 National Institute for Health and Clinical Excellence. Intramural UrethralBulking Procedures for Stress Urinary Incontinence in Women (IPG 138).London: NICE; 2005 [http://www.nice.org.uk/nicemedia/live/11182/31424/31424.pdf].
33 National Institute for Health and Clinical Excellence. Insertion of BiologicalSlings for Stress Urinary Incontinence in Women (IPG 154). London: NICE;2006 [http://www.nice.org.uk/nicemedia/live/11184/31431/31431.pdf].
34 National Institute for Health and Clinical Excellence. Insertion ofExtraurethral (Non-Circumferential) Retropubic Adjustable CompressionDevices for Stress Urinary Incontinence in Women (IPG 133). London: NICE;2005 [http://www.nice.org.uk/nicemedia/live/11183/31428/31428.pdf].
35 National Institute for Health and Clinical Excellence. Single-IncisionSub-Urethral Short Tape Insertion for Stress Urinary Incontinence in Women(IPG 262). London: NICE; 2008 [http://www.nice.org.uk/nicemedia/live/11858/40741/40741.pdf].
36 Williams S. On the defensive. Africa Casebook 2011;19(8–1):1.37 Bishop TF, Federman AD, Keyhani S. Physicians’ views on
defensive medicine: a national survey. Arch Intern Med 2010;170:1081–3.38 Kerr CD. The personal cost of medical litigation. Med J Aust 2004;181:384.39 Barber HR. The malpractice crisis in obstetrics and gynecology: is there a
solution? Bull N Y Acad Med 1991;67:162–72.40 MacLennan A, Nelson KB, Hankins G, Speer M. Who will deliver our
grandchildren? Implications of cerebral palsy litigation. JAMA2005;294:1688–90.
41 Robbennolt JK. Apologies and medical error. Clin Orthop Relat Res2009;467:376–82.
42 Francis R. The Mid Staffordshire NHS Foundation Trust Public Inquiry.London; The Stationery Office: 2013.
ª 2014 Royal College of Obstetricians and Gynaecologists 57
Jha and Rowland