Embed Size (px)
Citation preview
LESION STERLIZATION
&TISSUE REPAIR
By
Ahmed Mohsen Fawzy
Dentist in
Zagazig General HospitalEgypt

Dental caries is the greatest challenge to
the oral health of children especially
among low socioeconomic status
population.
Dental caries leads to irreversible damage
of pulp by exposing of the dental pulp to
microorganisms results in the
development of pulpal and periradicular
pathosis.

How do we fight back caries
invaded the pulpal tissues
..??
Pulpotomy
Pulpectomy
RCTExtraction

Is that an equivalent war ?!
No

What is LSTR ?Lesion Sterilization & Tissue Repair is simply
placing of antibiotic combination inside the
infected pulp chamber.
The therapy aims to eliminate causative bacteria
from lesions by sterilizing the lesions promoting
tissue repair & regeneration by the host's natural
tissue recovery process.
The Antiabiotic Combination 3 types of antibiotics are combined together to
ensure the complete eradication of all pathogenic
microbes in the periapical lesions.
The triple antibiotic paste (TAP) is formed by
mixing the powder of the antibiotics with
Macrogol & Propylene glycol which act as a
vehicle for the antimicrobial compound by their
penetrating ability to control the infection as far
as it extend.
So, it’s also called 3 Mix-MP

Triple Antibiotic Paste
TAP
Ciprofloxacin
Metronidazole
Minocycline
Nitroimidazole
compound that
exhibits a broad
spectrum of
activity against
protozoa and
anaerobic bacteria.
Synthetic
fluoroquinolone
& has
a bactericidal
mode of action.
Semisynthetic
derivative of
tetracycline
with a similar
spectrum of
activity.
Ratio 1 : 3 : 3 by wt

The Clinical Proceduresaccording to Rishi Nanda
Rubber dam Isolation
LA is not required as the pulp is necrotic
Caries Removal
Access Cavity
Extirpation of necrotic coronal pulp
Irrigation with normal saline (0.9%) and drying with cotton pellets to ensure visualization
Enlarging the canal orifices 1 mm in diameter and 2 mm deep to receive medicament (Medication Cavity)
Fill the medication cavities with 3 Mix and teeth restored with Glass Ionomer cement
S.S Crown
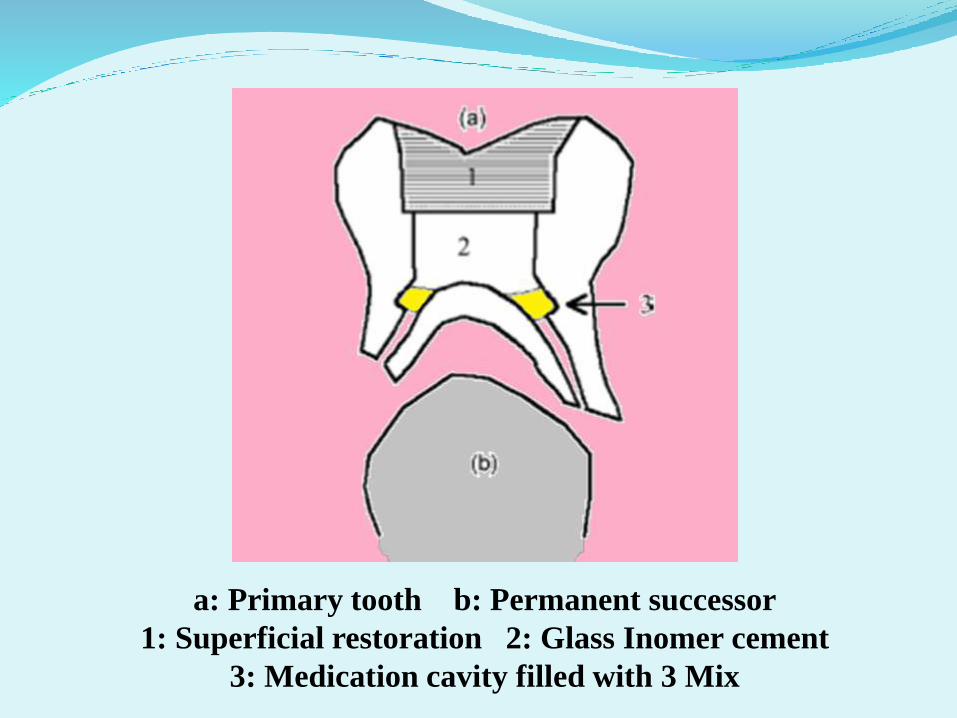
a: Primary tooth b: Permanent successor
1: Superficial restoration 2: Glass Inomer cement
3: Medication cavity filled with 3 Mix
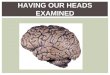
The Cariology Research Unit of the Niigata University
School of Dentistry was the first to introduce the concept
in 1988.

In Vitro evaluation of 3-Mix - Ibrahim Khalil et al
(2012) proved that the 3Mix (Ciprofloxacin, Minocycline, Metronidazole) has the best results when compared with each one alone & Ca(OH)2 againstEnterococcus faecaliswhich is considered as the most resistant strain in the radicular colonies.

In Vivo Studies on LSTR
Jaya et al (2012) evaluated and compared the clinical
and radiographic effectiveness of Ciprofloxacin,
Minocycline, Metronidazole combination with
Ciprofloxacin, Minocycline and Tinidazole
combination in primary teeth.
Tinidazole a second generation synthetic
nitroimidazole, is more effective than metronidazole
and produces fewer and milder side-effects and is
recommended as drug of choice in single dose therapy
and is preferred to metronidazole.

Jaya et al2012
Method:- 25 healthy children, aged between 6 – 9 years who were having
30 infected primary teeth with pain, tenderness &
symptoms of abscess were selected and divided into 2 groups.
- In Group A a mixture of 3mix-MP (Ciprofloxacin,
Metronidazole and Minocycline) was placed on the floor
of the pulp chamber covering the root canal orifices.
- In Group B a mixture of Ciprofloxacin, Tinidazole and
Minocycline was placed as a layer on the floor of the pulp
chamber.
- The procedure was completed in a single visit.

Jaya et al2012
- Post operative clinical evaluation was done after 1,6,12 and 24
months.
- Postoperative radiographic evaluation was done at 6,12 and 24
months.
- Both Groups showed :
Absence of pain & Tenderness
subsidence of Abscess
- They observed no significant difference between both the
groups and thus a combination of Ciprofloxacin, Minocycline
and Tinidazole antibacterial drugs can be used on teeth
pulpally involved with physiologic root resorption.
Divya et alMar. 2014
Conducted a study on 3 cases to ensure the
capability of the TAP to eliminate causative
bacteria from lesions, assuming that lesions will
be repaired or regenerated by the host's natural
tissue recovery process & softened dentin will re-
calcify, so both softened dentin as well as carious
dentin can be intentionally left so, an inflamed
pulp, even with spontaneous pain, will recover
after LSTR treatment.

Divya et alCase 1 :
- A 6-year old female child
with the chief complaint
of increasing pain in the
lower left back tooth
region for past two
weeks.
- On clinical examination
deep proximal caries
with pulpal exposure
was seen in the lower
left D.
- Patient had severe pain
on percussion on first
molar when compared to
the second molar.
- The radiograph showed
periapical radiolucency
Case 2:
- A six and a half year old male child with the chief complaint of pain and swelling in the lower left back tooth region & history of swelling for past two days.
- On clinical examination, patient had dentoalveolar abcsessrelated to the lower left E.
- The periapical radiograph showed radiolucencyinvolving the furcationand circumscribing the mesial root of the second primary molar
Case 3 :
- A five year old male
child with the chief
complaint of pain in
the lower left back
tooth region for 2
weeks.
- On clinical
examination left lower
D had caries with
pulpal exposure.
There was
dentoalveolar abscess
related to the same
tooth.
- The radiograph
showed mild furcation
involvement.

Divya et al
Preoperative After 3 months
Case 1

Divya et al
Preoperative After 3 months
Case 2

Divya et al
Preoperative After 3 months
Case 3

Divya et alConclusion:
The Lesion sterilization and tissue repair therapy is simple,
painless, time-saving, and with less burden to patients
physically and mentally.
Thus, patient compliance and cooperation of patients is
predicable which is of great concern in the management of
Pediatric patients.
This procedure might disinfect the severely infected
deciduous teeth and allow it to function as a space
maintainer until the eruption of its permanent successor.

Burrs et al
Children’s Hospital of Wisconsin
They published 2-case report in May 2014 to provide dental practitioners an ensured alternative treatment to pulpectomies and extractions for nonvital pulp therapy in primary teeth.
Modifications on 3-Mix have been acquired in this case report.

CHW’s 3-Mix 2-part system
- 1. Dry powder :
Metronidazole
Ciprofloxacin
Clindamycin (To avoid
discoloration of the tooth
and gums induced by
Minocycline)
Iodoform (To make the
product radiopaque)
- 2. Liquid component :
Polyethylene Glycol 300
MW liquid
Propylene Glycol
- That is mixed with the
powder in the dentist’s
office immediately prior to
use
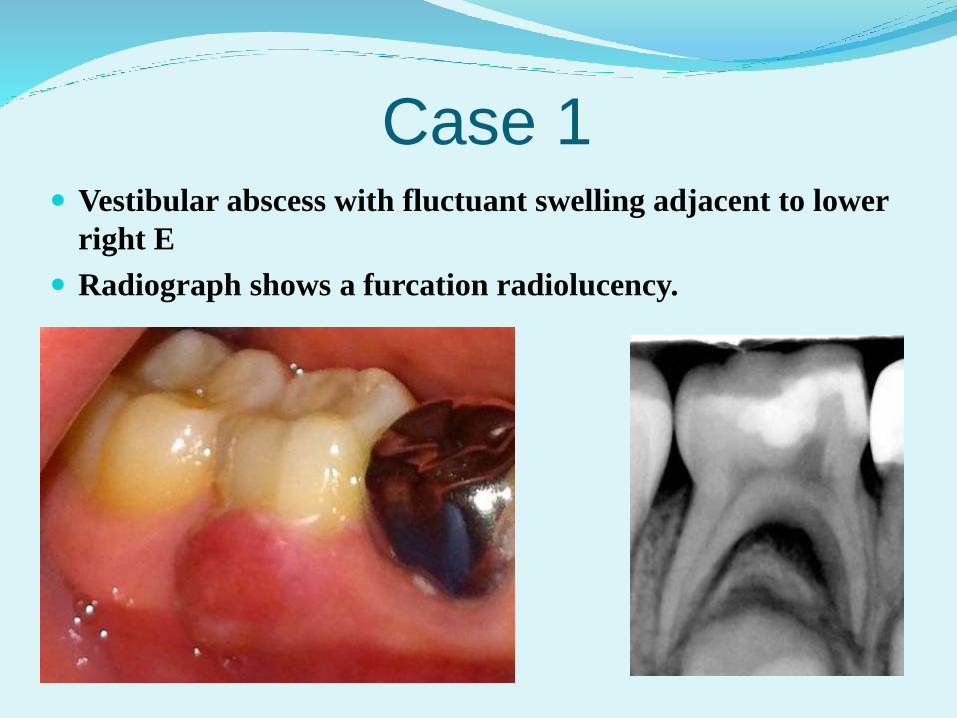
Case 1 Vestibular abscess with fluctuant swelling adjacent to lower
right E
Radiograph shows a furcation radiolucency.

Case 14 Months postoperative patient continues to be symptom free.
Furcal bone shows continued healing and increase in
trabeculation.

Case 2- Vestibular abscess with fluctuant swelling adjacent to the
lower right D.
- Clinically the tooth was depressible and class III mobile.
- Radiograph shows a furcation radiolucency.
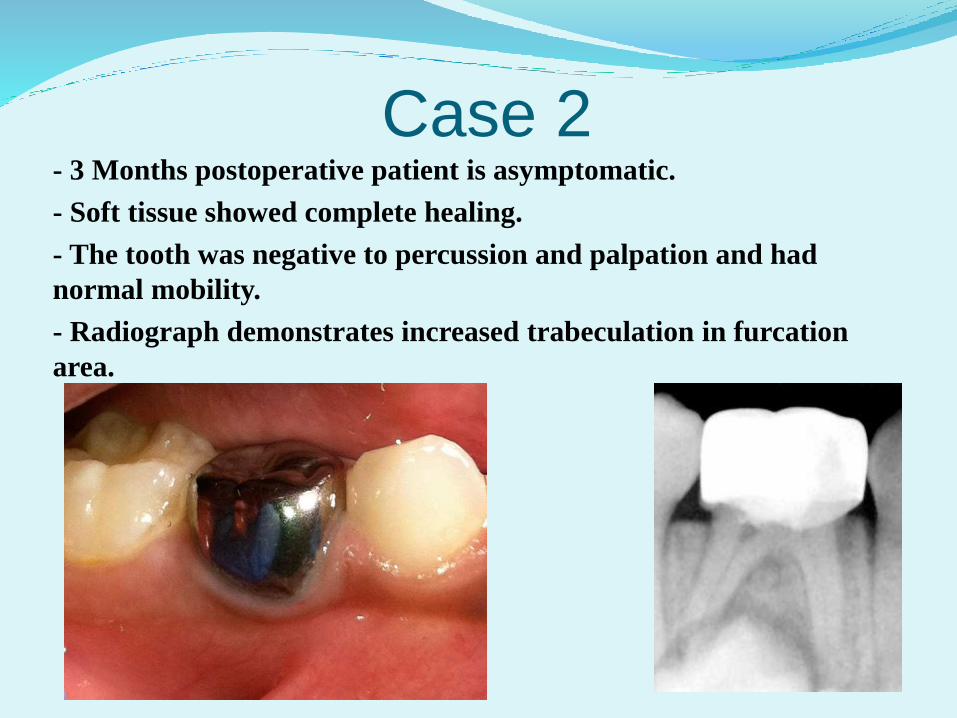
Case 2- 3 Months postoperative patient is asymptomatic.
- Soft tissue showed complete healing.
- The tooth was negative to percussion and palpation and had
normal mobility.
- Radiograph demonstrates increased trabeculation in furcation
area.

Rishi Nanda et alAug. 2014
- Conducted a study on 40 teeth of healthy children were
randomly divided into two groups.
- In Group A 20 teeth, using (ciprofloxacin, metronidazole,
and minocycline) 3 Mix
- Group B 20 teeth, using (ciprofloxacin, ornidazole, and
minocycline) Other Mix.
- Ornidazole has been reported to have a longer
duration of action, with better efficacy and slower
metabolism compared with metronidazole.

Rishi Nanda et al2014
Clinical and radiographic evaluation was done at 3, 6 and 12
months.
Both of the groups showed 100% clinical success
Radiographic success rate was 81% with 3 Mix and
92% with Other Mix.

Rishi Nanda et al2014
Using Ciprofloxacin, Minocycline, Metronidazole (3mix)
A: preoperative B: after 3 months
C: after 6 months D: after12 months
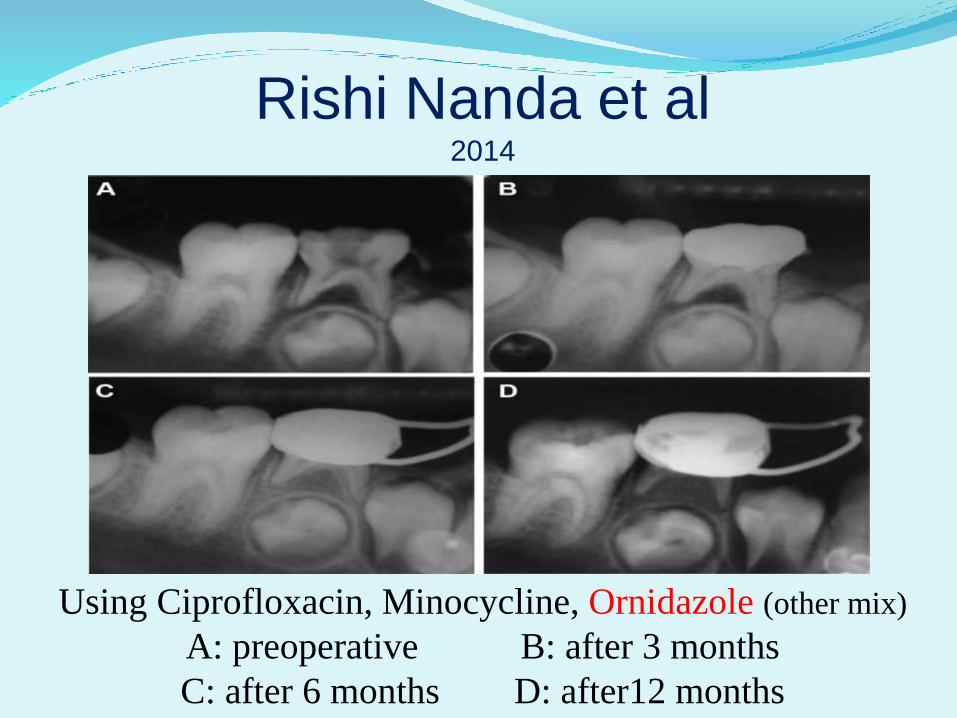
Rishi Nanda et al2014
Using Ciprofloxacin, Minocycline, Ornidazole (other mix)
A: preoperative B: after 3 months
C: after 6 months D: after12 months

Rishi Nanda et al2014
Wang et al2011
Performed 2 case report to present
conservative treatment for immature
premolars with apical periodontitis
using triple antibiotic paste (TAP) to
disinfect the root canal systems for
revascularization.

Wang et al2011
Case 1 :
- 11-year-old boy
- Swelling on the buccal
vestibule related to the lower
right 5
- Sensitive to palpation and
percussion.
- Radiograph : immature open
apex.
Case 2 :
- 14-year-old girl.
- sinus tract on the buccal
gingiva of the mandibular
right second premolar.
- Percussion sensitivity existed.
- 5 mm of probing depth on the
mesial surface of the root.
- Radiograph : immature open
apex.

Wang et al2011
Case Management :
- Rubber dam isolation
- Access cavity preparation without anesthesia.
- Hemorrhage observed.
- A gutta-percha cone size # 30 was gently inserted into
the canal and the patient reported sensitivity,
potentially indicating the survival of residual vital
pulp tissue.

Wang et al2011
- Irrigation with 10 mL of 3% NaOCl, without
instrumentation.
- The canal was dried with paper points.
- 3 mix placed into the canal with an endodontic plugger to
a depth of 10 mm.
- The access cavity was sealed with 4-mm thickness of
intermediate restorative materials (IRM)
- After 21 days no clinical symptoms.
- The tooth was then re-opened & the canal irrigated with
10 mL of 3% NaOCl.

Wang et al2011
- An endodontic explorer was introduced into the canal until apical tissue was detected.
- The explorer was used to irritate the tissue gently to create some bleeding into the canal.
- The bleeding was stopped at a level of 3 mm apical to the CEJ and left for 10 minutes.
- 3 mm thickness of MTA was carefully placed over the blood clot followed by a wet cotton pellet & IRM.
- 3 days later the IRM and cotton pellet were removed and replaced with bonded composite resin restoration.
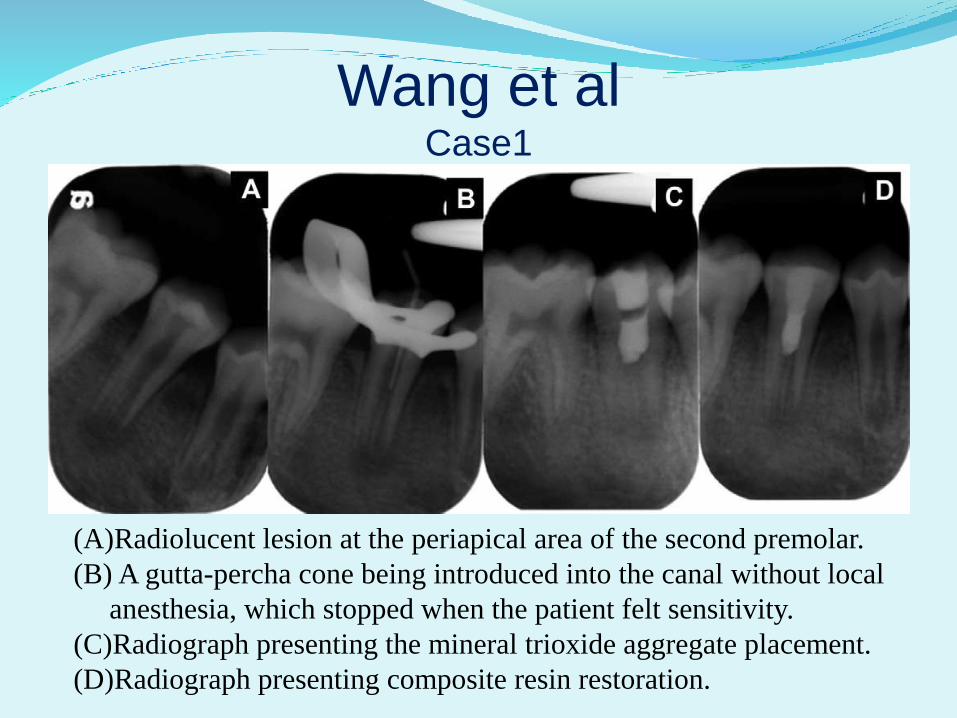
Wang et alCase1
(A)Radiolucent lesion at the periapical area of the second premolar.
(B) A gutta-percha cone being introduced into the canal without local
anesthesia, which stopped when the patient felt sensitivity.
(C)Radiograph presenting the mineral trioxide aggregate placement.
(D)Radiograph presenting composite resin restoration.

Wang et al
(A)6 month follow-up radiograph showing complete resolution of radiolucency.
(B)One-year follow-up radiograph revealing an increase in the thickness of the
root canal wall and continual development of the apex.
(C)17 month follow-up radiograph depicting continual root development.
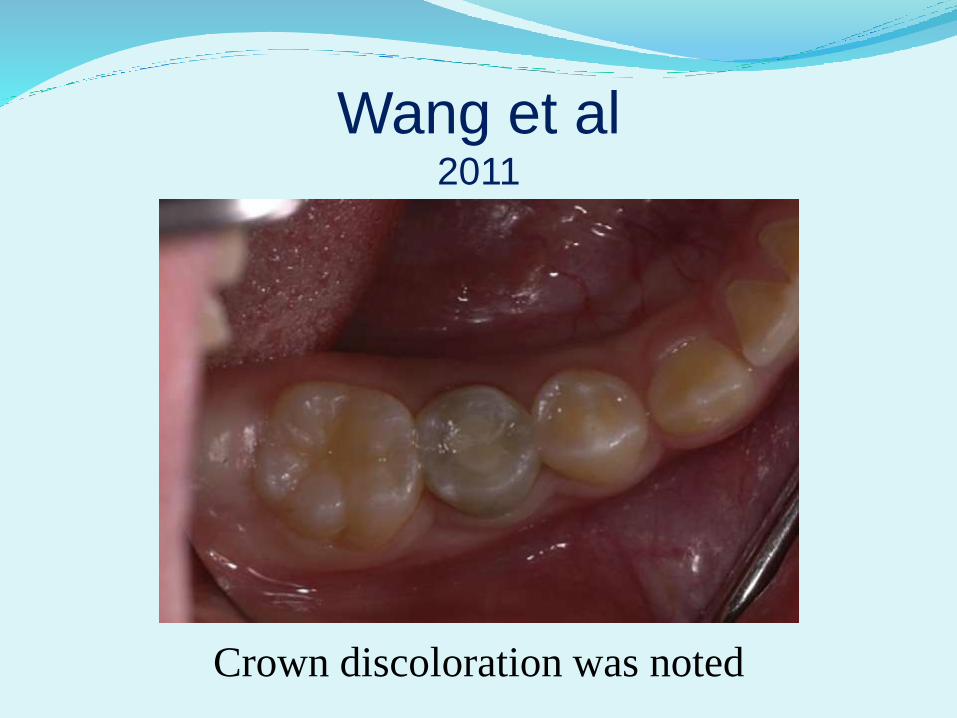
Wang et al2011
Crown discoloration was noted

Wang et alCase 2
(A) A sinus tract on the alveolar mucosa between 1st & 2nd premolars.
(B) Periradicular radiolucency of 2nd premolar with a wide open apex.
(C) Radiograph showing the sinus tract tracing to the periradicular radiolucency of
the affected tooth.
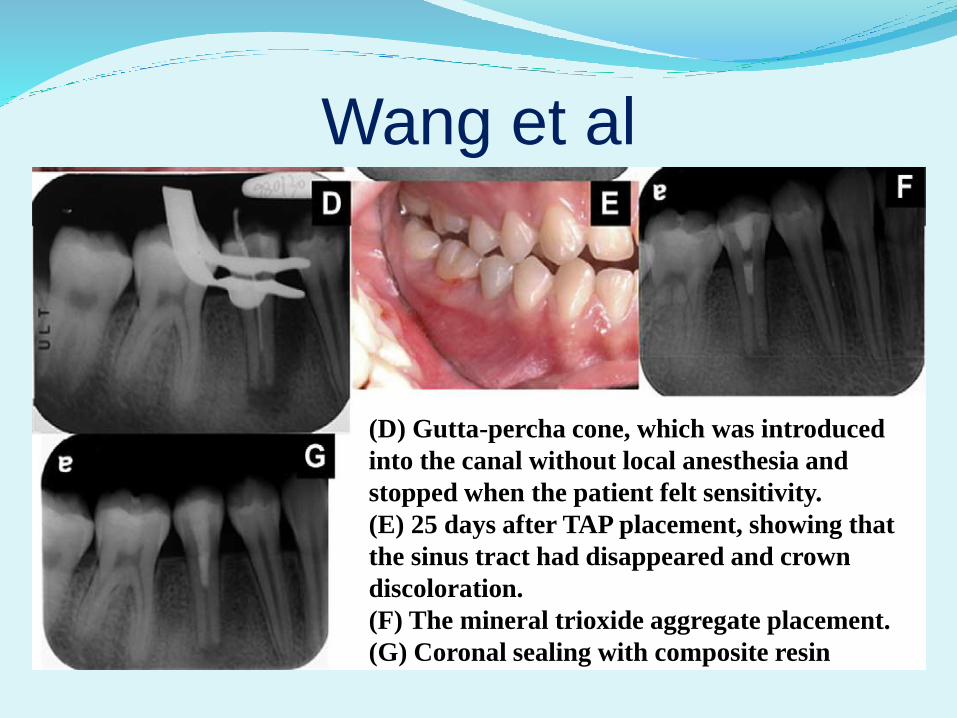
Wang et al
(D) Gutta-percha cone, which was introduced
into the canal without local anesthesia and
stopped when the patient felt sensitivity.
(E) 25 days after TAP placement, showing that
the sinus tract had disappeared and crown
discoloration.
(F) The mineral trioxide aggregate placement.
(G) Coronal sealing with composite resin
LSTR indications1- All indications of pulpectomy
2- 1ry affected teeth associated with pain &
tender to percussion
3- Presence of mobility (grade I, II)
4- Presence of abscess
5- Presence of sinus tract
6- Presence of radiolucency in furcation area
LSTR indications7- Restorable crown
8- Pulpless 1ry teeth in hemophilic patient
9- Strategic importance for space
maintaining especially when space
maintainer fabrication is difficult (e.g.:
Handicapped & uncooperative patients)
10- Immature permanent tooth with
incomplete root formation
LSTR contraindication
1- Sensitive & allergic patient to any of the antibiotic componants
2- Radiographic evidence of excessive internal or external root resorption
3- Primary tooth about to exfoliate
4- Perforated pulpal floor
5-Excessive bone loss in furcation area involving underlying tooth germ
6- Unrestorable crown of permanent tooth as post placement & core build up are not allowed in revitalized pulp

Advantages of LSTR1- Easy & simple technique
2- One short visit technique
3- Economic
4- Painless
5- No instrumentation needed
6- No irritation of periapical tissues
7- No obturation needed
8- No use of formocresol

Disadvantages of LSTR1- Minocycline discoloration effect
(Solved by replacing Minocycline with
Clindamycine) by CHW
2- Radiolocent in radiograph
(Solved by adding Iodoform) by CHW
3- Inability of post placement & core build up in
badly destructed permanent teeth
Thank You