Embed Size (px)
Citation preview

Late Post-operative Late Post-operative Spinal InfectionsSpinal Infections
(fol lowing instrumentation)(fol lowing instrumentation)
G.S. SapkasG.S. Sapkas
1st Orthopaedic Department 1st Orthopaedic Department University Hospital “ATTIKON”University Hospital “ATTIKON”
Medical SchoolMedical SchoolAthens UniversityAthens University

Post-operative spinal infection Post-operative spinal infection
following instrumentation and following instrumentation and fusion is a potentially fusion is a potentially
devastating complication, devastating complication, reporting in the literature from reporting in the literature from
0.7% to 11.9% 0.7% to 11.9%
Infection places the patient at Infection places the patient at risk for:risk for:– PseudarthrosisPseudarthrosis– Adverse neurologic sequelaeAdverse neurologic sequelae– Poor outcome - Death Poor outcome - Death Abey DM et al J. Spinal Disord. 1995
Glassman SD et al Spine 1996Levi ADO et al J. Neurosurg. 1997
Roberts FJ et al Spine 1998

The administration ofof prophylactic prophylactic antibiotics decreases the infection antibiotics decreases the infection rate in spinal surgeryrate in spinal surgery
The use of instrumentation The use of instrumentation increases the risk for infectionincreases the risk for infection
Rimoldi RL et al Orthop. Clin North Am 1996Rubinstein E. et al J.B.J.S. (B) 1994
Cappen DA et al Orthop. Clin North Am 1996Massie JB et al C. O. R.R., 1992Knapp DR et al C. O. R.R. 1988

DiabetesDiabetes MalignancyMalignancy Tobacco use Tobacco use Obesity Obesity Cardiovascular Cardiovascular
problemsproblems Age Age ≥ 70 yrs≥ 70 yrs
Pre-operative medical conditions and Pre-operative medical conditions and risk factors are reported to be:risk factors are reported to be:
Weinstein MA et al J. Spin. Disord. 2000Weinstein MA et al J. Spin. Disord. 2000O.K.U. A.A.O.S. Spine 2 2002O.K.U. A.A.O.S. Spine 2 2002

Steroid use Steroid use ImmunosuppressionImmunosuppression Myelodysplasia Myelodysplasia Post - radiationPost - radiation
Pre-operative medical conditions and Pre-operative medical conditions and risk factors are reported to be:risk factors are reported to be:
Weinstein MA et al J. Spin. Disord. 2000Weinstein MA et al J. Spin. Disord. 2000O.K.U. A.A.O.S. Spine 2 2002O.K.U. A.A.O.S. Spine 2 2002

Length of pre-operative hospitalization Length of pre-operative hospitalization Revision surgery Revision surgery Time of surgery Time of surgery The number of fused segmentsThe number of fused segments Bone graft or methylmethacrylateBone graft or methylmethacrylate Blood loss and transfusionBlood loss and transfusion
Weinstein MA et al J. Spin. Disord. 2000Weinstein MA et al J. Spin. Disord. 2000O.K.U. A.A.O.S. Spine 2 2002O.K.U. A.A.O.S. Spine 2 2002
Pre- and intra-operative riskPre- and intra-operative risk factors are reported to be:factors are reported to be:

The use of instrumentationThe use of instrumentationThe type of implantsThe type of implants
SteelSteel TitaniumTitanium Cross linksCross links
Weinstein MA et al J. Spin. Disord. 2000Weinstein MA et al J. Spin. Disord. 2000O.K.U. A.A.O.S. Spine 2 2002O.K.U. A.A.O.S. Spine 2 2002
Intra-Post-operative riskIntra-Post-operative risk factors are reported to be:factors are reported to be:

Type of procedureType of procedureMinimal invasiveMinimal invasiveExtensiveExtensive
Weinstein MA et al J. Spin. Disord. 2000Weinstein MA et al J. Spin. Disord. 2000O.K.U. A.A.O.S. Spine 2 2002O.K.U. A.A.O.S. Spine 2 2002
Intra-Post-operative riskIntra-Post-operative risk factors are reported to be:factors are reported to be:

There is a wide There is a wide
variety of implant variety of implant designs including:designs including:
Segmental and Segmental and non-segmental non-segmental constructsconstructs
Rigid and Rigid and semi-rigid semi-rigid connectorsconnectors
Different materials Different materials and surface and surface treatments.treatments.

Spinal implantsSpinal implants
Factors of corrosion Factors of corrosion
1) 1) Combination of different metallic materialsCombination of different metallic materials2) 2) Surfaces’ composition and irregularitySurfaces’ composition and irregularity 3) 3) Micro-movements between the parts of the Micro-movements between the parts of the
spinal instrumentation spinal instrumentation 4) 4) Ions of ClIons of Cl -- from the plasma and from the plasma and
intercellular areaintercellular area5) 5) pHpH6) 6) Different concentration of ODifferent concentration of O22 ions ions
in free and covered metallic areasin free and covered metallic areas

Metal corrosionMetal corrosion galvanic corrosion different metals
frett ing corrosion same metals in micro-movement
crevice corrosion metals in different electrolytic fluids

Galvanic corrosion different metals
Accelerated Accelerated decay due to neighboring of dissimilar decay due to neighboring of dissimilar metallic implants in a corrosivemetallic implants in a corrosiveelectrolitic invironmentelectrolitic invironment
Electrochemical dissimilarity Electrochemical dissimilarity
It is possible to take placeIt is possible to take placeeven between the same typeeven between the same typeof materials in different end-plate of materials in different end-plate surfacessurfaces
It is common in articulated spinal implantsIt is common in articulated spinal implants

Frett ing corrosionFrett ing corrosion same metals in micro-movement

Crevice corrosionCrevice corrosionmetals in different electrolytic f luids
OH-
OH-
OH- OH-
O2
O2
O2

Approximately these Approximately these
metalic constructs metalic constructs are made of:are made of:
35% stainless steel35% stainless steel 65% (Ti64) alloy 65% (Ti64) alloy
titaniumtitanium aluminium – 6aluminium – 6 vanadium - 4vanadium - 4

Mechanical damage Mechanical damage from from frettingfretting can compromise can compromise passivated surfaces passivated surfaces and result in:and result in:
ionic debrisionic debris from from corrosion corrosion and and
particulate debris particulate debris from mechanical from mechanical damagedamage..

Ionic debrisIonic debris
is additive is additive to the influences to the influences of of particulate debrisparticulate debris and and can have a significant can have a significant impact on impact on local cytotoxicity.local cytotoxicity.

The use of metal The use of metal
instrumentation, instrumentation, particularly titanium,particularly titanium, for spinal fusion has introduced for spinal fusion has introduced the possibility the possibility of generating of generating microscopic metal particles microscopic metal particles that may be deposited :that may be deposited :
in the paraspinal soft tissues in the paraspinal soft tissues
or oron the neural elements.on the neural elements.

In vitro studies have In vitro studies have shown that these shown that these metal particles can be metal particles can be phagocytizedphagocytized intracellularlyintracellularly leading leading to release of to release of inflammatory inflammatory cytokinescytokines
Betts F. et al, Clin Orth., 1992Lee JM et al, J.B.J.S. 1992

This This
inflammatory inflammatory cascade may cascade may lead in turn to: lead in turn to:
resoption of resoption of bone and bone and
cellular deathcellular death
Hallab NJ, Cunnigham B et al, Spine 2003

The potential The potential
for for bonebone resorptionresorption is particularly is particularly distressing distressing in spinal surgery in spinal surgery because much of the because much of the operation’s success operation’s success depends on depends on obtaining obtaining a spinal fusion.a spinal fusion.

The toxic effects The toxic effects
of these metal of these metal particles particles also are of great also are of great concern because concern because the the neural elementsneural elements are widely exposed are widely exposed during spinal during spinal decompressions.decompressions.

TitaniumTitanium
TitaniumTitanium generally is generally is regarded as safe for regarded as safe for an organism, but it is an organism, but it is reported that titanium reported that titanium has a biochemical has a biochemical action of increasing: action of increasing:
prostagladin E2 prostagladin E2 or or
interleukin 1interleukin 1Tsustui T., et al, J. Orthop. Science 1999

Stainless steelStainless steel
Increased resistant to Increased resistant to corrosion with the corrosion with the addition :addition :
Chromium Chromium NikeliumNikeliumMolybdenum Molybdenum

Original procedureOriginal procedure It is clear that the type of spinal surgery It is clear that the type of spinal surgery
affects the risk for post-operative affects the risk for post-operative infectioninfection
Infection rate for:Infection rate for: Discectomy ~ 0.85 %Discectomy ~ 0.85 %
Decompression laminectomy ~ 1.5 %Decompression laminectomy ~ 1.5 %
Fusion added ~ 2.4 %Fusion added ~ 2.4 % Fusion without instrumentation ~ Fusion without instrumentation ~ 0.4%0.4% Fusion with hardware ~ Fusion with hardware ~ 3.2% (2.4% - 8.5%)3.2% (2.4% - 8.5%)
Operative treatment with instrumentation Operative treatment with instrumentation for metastatic disease ~ 20%for metastatic disease ~ 20%
Heller JG The spine 1992Abbey DM et al J. Spin. Disord 1995
Roibert FG et al Spine 1998Weinstein MA et al J. Spin. Disord. 2000

Type of Type of procedureprocedure
Anterior Anterior Posterior Posterior

Type of Type of procedureprocedure
Single Single Combined Combined

Level of Level of procedureprocedure
Cervical Cervical Thoracic - Lumbar Thoracic - Lumbar

Treatment of Treatment of post – operative infectionpost – operative infection
Early and decisive Early and decisive treatment should be treatment should be initiated on diagnosisinitiated on diagnosis
As medical management is As medical management is likely to fail, aggressive likely to fail, aggressive surgical intervention surgical intervention typically is suggested for typically is suggested for post-operative infectionspost-operative infections
O.K.U. A.A.O.S. Spine 2 2002

The debridement should proceed The debridement should proceed in a systematic fashionin a systematic fashion– Each layer is debrided and cultured Each layer is debrided and cultured
before advancing deeper with the before advancing deeper with the dissection dissection
– If subfacial involvement is believed to If subfacial involvement is believed to exist because of subfacial aspiration exist because of subfacial aspiration or gross deep drainageor gross deep drainage
Deep debridement is performed

Meticulous wound lavage with Meticulous wound lavage with
N/S-vancomycin N/S-vancomycin If there is evidence of pyogenic If there is evidence of pyogenic
infection it is necessary to infection it is necessary to insert a suction irrigation insert a suction irrigation system once moresystem once more
The bone graft poses a bit of a The bone graft poses a bit of a dilemma. Many authors will allow it to dilemma. Many authors will allow it to remain in place especially if it is remain in place especially if it is adherent. Others recommend removal adherent. Others recommend removal of loose graft and washing or of loose graft and washing or replacementreplacement
Hemostastis must be meticulous to Hemostastis must be meticulous to prevent formation of hematoma prevent formation of hematoma seeded with bacteriaseeded with bacteria

Although instrumentation is Although instrumentation is typically left in place in the typically left in place in the early post-operative period, early post-operative period, all other foreign bodies suchall other foreign bodies such as :as :
Bone waxBone wax Absorbable gelatin spongeAbsorbable gelatin sponge
Must be removedMust be removed

Hardware removal Hardware removal is appropriate:is appropriate:
if the instrumentation if the instrumentation has failed has failed in refractory infections in refractory infections in cases of late in cases of late hematogenous infection hematogenous infection occurring after a fusion occurring after a fusion has healed has healed

Gentamycin beeds- chain

Primary wound closure over Primary wound closure over drains, often with retention drains, often with retention sutures to prevent dehiscence sutures to prevent dehiscence is favoured when possibleis favoured when possible
Routine redebridements often Routine redebridements often are required (after 48 hours)are required (after 48 hours)
Simple wound infections may Simple wound infections may be packed open and allowed to be packed open and allowed to close by secondary intentionclose by secondary intention
More complex wound More complex wound infections may require infections may require musculocutaneous flapsmusculocutaneous flaps
Wound closureWound closure

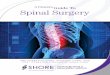
Courtesy K. Soultanis
Adolescent idiopathic scoliosis
Pre-op Post-op

1 year post-op1 year post-op


Implant removal - debridement New implants

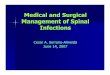
Severe surgical site infection after posterior thoracolumbar fusionSevere surgical site infection after posterior thoracolumbar fusion
Extensive granulation tissue(use of the VAC system)
Rotational muscle flap

Antibiotic therapy is required for at least Antibiotic therapy is required for at least 10 to 14 days in the face of soft tissue and 10 to 14 days in the face of soft tissue and wound infectionswound infections
Six weeks of parenteral antibiotic treatment is Six weeks of parenteral antibiotic treatment is preferred if:preferred if:- bony involvement - bony involvement - deep infection- deep infection- foreign bodies (metal, graft and so forth) - foreign bodies (metal, graft and so forth)
remain remain
Antibiotic therapy

Retrospective study of 850 patients, who were operated with spinal fusion
Posterior instrumentation Combined anterior-posterior instrumentation
Sapkas G, Eur. J. Orth. Surg. Traum. 2006

The init ial diagnosis was:
Degenerative spondyloarthrit is - 553 Scoliosis - 198 Kyphosis - 50 Spinal tumors ( Primary Benign and
Malignant/ Metastatic ) - 49

A retrospective analysis was performed to identify :Init ial diagnosisDemographic characterist ics Pre-operative risk factorsType of spinal surgeryOnset of the symptoms Clinical presentation Management ( laboratory test, imaging, treatment)

InvestigationsInvestigations
X-raysX-rays M.R.I.M.R.I. C.T. scanC.T. scan Scanning TC99 MDPScanning TC99 MDP Scanning Ga 67Scanning Ga 67

The incidence of Postoperative Spinal
Infection (PSI) was
2,47%21/850 pts
9 male /12 female Mean age 49 years (23-76)

RESULTSRESULTS
Early PSI (<3 months post-op)19 patients14 superficial - 5 deep Onset: 19th day (7-85)Symptoms: fever, low back pain, swelling, drainage(90%)
Late PSI (>3 months post-op)2 patientsOnset: 1,5 and 2 years post-opSymptoms: low back pain, swelling, drainage

RISK FACTORSRISK FACTORS
All patients had at least 1 risk factor (mean: 1,87)
DiabetesDiabetes Mellitus 7 Immunosuppression-Malignancy 6 Obesity 6 Tabacco use 6 Revision spine surgery 4 Long time hospitalization 2 Prolonged time of surgery 3

Early deep infectionsWBC 8900-11000WBC 8900-11000 ESR: ~ 100 1 s t hourCRP increasedBlood culture posit ive 11/19
Late infectionsWBC 8900-11000WBC 8900-11000 ESR: 40-60 1 s t hour CRP mild, <3μg/dlWound culture posit ive 2/2 Staph. EpidStaph. Epid ..
LABORATORY DIAGNOSTIC LABORATORY DIAGNOSTIC STUDIESSTUDIES

Early infections
Staph. Aureus methicil l in resistanceStaph. Aureus methicil l in resistance 1010 patients – 53%patients – 53%
Staph. EpidermidisStaph. Epidermidis 4 patients – 22%4 patients – 22%
Enterobacter – BacteroidesEnterobacter – Bacteroides 3 patients – 15%3 patients – 15%
More than oneMore than one 22 patients – 10%patients – 10%
OFFENDING BACTERIAOFFENDING BACTERIA

TREATMENTTREATMENT
Superficial wound infections •Surgical Debridement •Antibiot ic Chemotherapy i.v. 12/52
Deep infections•Routine Surgical Redebridement•Delayed wound closure •Antibiot ic Chemotherapy i.v. 12/52 per os ~ 6 months
Instrumentat ion Removal 3 patients (14,3%) 1 patient required re-operation ( for spine instabil i ty )

RESULTSRESULTS
12 months after init iat ion of the treatment
Free of symptoms 18 patients - 86% (pain relief-neurological improvement-no disabil i t ies)
Eradication of the infection (ESR-CRP)in al l patients 100%
Solid spinal fusion was achieved in 19 patients (90%)
2 patients with early deep infection eventually developed pseudarthrosis

Conclusions Conclusions

The incidence The incidence of PSI after of PSI after instrumentation instrumentation is high (2.47%)is high (2.47%)

Most important Most important risk factors are risk factors are malnutrit ion, malnutrit ion, smoking, smoking, obesity obesity and and extended extended perioperative perioperative hospital stayhospital stay

MRI MRI is very is very useful for early useful for early diagnosis-diagnosis-managementmanagement

Surgical Surgical debridement and debridement and antibiotics antibiotics administration for administration for at least 12 weeks at least 12 weeks is the gold is the gold standardstandard

Hardware removal Hardware removal is controversial is controversial because of their because of their importance for importance for stabil ization of the stabil ization of the spine (solid fusion spine (solid fusion - eradication of - eradication of infection)infection)

University Hospital “ATTIKON”