Embed Size (px)
Citation preview

Laboratory DiagnosisOf
Tuberculosis
Tarun Prudvi B
MBBS 3RD PROFESSSIONAL

A complete medical evaluation for tuberculosis(TB) must include a medical history, a physical
examination, a chest X-ray and microbiological
examination (of sputum or some other appropriate
sample). It may also include a tuberculin skin test,
other scans and X-rays, surgical biopsy
Tuberculosis is diagnosed by finding Mycobacterium
tuberculosis bacteria in a clinical specimen taken from the
patient. While other investigations may strongly suggest
tuberculosis as the diagnosis, they cannot confirm it.

Diagnosis // MEDICAL HISTORY
Productive prolonged cough of three or more weeks, chest pain, and haemoptysis.
Systemic symptoms
Low grade remittent fever, chills, night sweats,
Appetite loss, weight loss, easy fatigability, and
Production of sputum that starts out mucoid but changes to purulent.
Other parts of the medical history include prior TB exposure, infection or disease;
past TB treatment;
demographic risk factors for TB;
and medical conditions that increase risk for TB disease such as HIV infection.
• Tuberculosis should be suspected when a pneumonia-like illness has persisted longer than three weeks, or when a respiratory illness in an otherwise healthy individual does not respond to regular antibiotics.

A definitive diagnosis of tuberculosis can only be made by culturing Mycobacterium tuberculosis organisms from a specimen taken from the patient (most often sputum, but may also include pus, CSF, biopsied tissue, etc.).
A diagnosis made other than by culture may only be classified as "probable" or "presumed".
For a diagnosis negating the possibility of tuberculosis infection, most protocols require that two separate cultures both test negative
Diagnosis // Microbiological studies

SAMPLE SOURCES // Sputum
Sputum smears and cultures should be done for acid-fast bacilli if the patient is producing sputum.
In cases where there is no spontaneous sputum production, a sample can be induced, usually by nebulized inhalation of a saline or saline with bronchodilator solution.
A comparative study found that inducing three sputum samples is more sensitive than three gastric washings

Alternative sample sources
Gastric washings,
Laryngeal swab,
Bronchoscopy (with bronchoalveolar lavage, bronchial washings, and/or transbronchial biopsy),
FNAC (transtracheal or transbronchial).
In some cases, a more invasive technique is necessary, including tissue biopsy during mediastinoscopy or thoracoscopy

Concentration methods
Petroff’s method
N acetyl cysteine is used, NaOH kills contaminating bacteria.Sputum is incubated w/ 4% sodium hydroxide at 37 degrees with frequent shaking till it becomes clear. Then centrifuged at 3000rpm for 20 min and sediment neutralized with N/10 HCL.
NALC combined with 2% NaOH

Microscopy
Ziehl-Neelsen staining
After smears are dried then stained using Ziehl-Neelsen technique and are observed under oil immersion for the presence of acid fast bacilli

Auramine rhodamine
Smears are stained with Auramine phenol or Auramine fluorescent dyes and examined under ultraviolet illumination.
Seen as bright rods against dark background.

AFB Report as per RNTCP Guidelines:
Result Grading No. of fields
>10/field positive 3+ 20
1-10/fiield Positive 2+ 50
10-99/field Positive 1+ 100
1-9/field
No bacilli
Positive
Negative
Scanty 100
1000

CultureSolid media: Lowenstein-Jensen (LJ) medium.
Colonies are dry, rough, raised, irregular with wrinkled surface.
They are creamy white or buff colored.
They may take 3-8 weeks to develop.
Liquid media: middle brooke 7H10/7H11

Automated systems
Radiometric BACTEC 460 TB method:
This system detects the presence of mycobacteria based on their metabolism rather than visible growth.
When the 14C labelled substrate present in the medium is metabolised, 14Co2 is produced and measured by the BACTEC system instrument and reported in terms of the growth index(GI) value.
The BACTEC system is also useful in the identification of M. tuberculosis using a specific inhibitor, para-nitro-a-acetyl-amino-B-hydroxypropiophenone.
Using the same system, drug susceptibility tests can also be performed for all the anti-tuberculosis drugs when sufficient GI is observed.
Mycobacteria in clinical samples can be detected in half the time compared to conventional culture methods

MGIT 960 (Mycobacteria Growth Indicator Tube):
Growth detection is based on the AFB metabolic O2 utilization.
MB/BacT system:
This is a non-radiometric continuous monitoring system with computerised database management. The system is based on colorimetric detection of CO2.
ESP culture system II:
This is a fully automated continuous monitoring system based on the detection of pressure changes within the headspace above the broth culture medium in a sealed bottle, i.e. either gas production or gas consumption due to microbial growth.
A special detection algorithm is present in this system for the detection of very slowly growing mycobacteria.

Resistant testing.
Phenotypic methods
Absolute concentration method,
Resistance ratio method
Proportion method.
Recently developed phenotypic methods are E-test (commercially available as AB BIODISK), micro-well alamar blue assay and micro plate tetrazoliumreduction assay, mycolic acid index susceptibility testing.
Microscopic observation of broth cultures for drug susceptibility assay, micro-colony detection, Pha B assay and luciferase reporter phage assay, etc., are also being developed37.

Important genotypic methods include Automated DNA sequencing, PCR SSCP, PCR HDF, Line probe assay or LiPA (solid phase hybridisation assay).
Mycobacteria usually acquire resistance either by alteration of the drug target by mutation or by titration of drug through over production of the target. MDR-TB usually results from an accumulation of individual target genes

Demonstration of Mycobacteria Directly from Clinical Samples
Genotypic methods:
Nucleic-acid Amplification Assays (NAA)
PCR
Phenotypic methods:
FAST Plaque TB

Serological Diagnosis
stages or types of TB infection Antigen (epitope)
Contacts and tuberculin convertors 38 KDa (TB 71,72), 14 KDa (TB 68)
Radiologically healed or less extensive disease
14 KDa (TB 68
Radiologically extensive disease 38 KDa (TB 71, 72)
Miliary TB LAM (ML 34)
TB meningitis adults LAM (ML 34)children 17 KDa (HBT2)
Human immuno-deficiency virus (HIV) infection-
38 KDa, LAM, 17KDa
It is important to remember that different antibody specificities are stimulated in various stages or types of TB infection

Tests.
Sandwich ELISA, inhibition ELISA, latex agglutination and reverse passive haemagglutination tests are various methods used for their detection
Newer tests are the TB STAT-PAK, enzyme Immuno-assay for detection of anti-mycobacterial superoxide dismutase antibody, and the Insta test TB

Test to detect latent infection.
• The Heaf test was used in the United Kingdom until 2005, and is graded on a four point scale. The Mantoux test is now used.
• The equivalent Mantoux test positive levels done with 10 TU PPD (0.1 ml 100 TU/ml, 1:1000) are
• 0–4 mm induration (Heaf 0 to 1)
• 5–14 mm induration (Heaf 2)
• Greater than 15 mm induration (Heaf 3 to 5)



IFN-gamma produced by T lymphocytes in whole blood after stimulation with PPDs obtained from M. tuberculosis, M. avium, and
M. bovis- QauntiFERON-Gold test for TB.

RNTCP PROTOCOL



Radiography
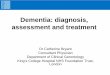
• In active pulmonary TB, infiltrates or consolidations and/or cavities are often seen in the upper lungs with or without mediastinal or hilar lymphadenopathy or pleural effusions ( tuberculous pleurisy).
• However, lesions may appear anywhere in the lungs. In disseminated TB a pattern of many tiny nodules throughout the lung fields is common - the so-called miliary TB.
• In HIV and other immunosuppressed persons, any abnormality may indicate TB or the chest X-ray may even appear entirely normal.
• Abnormalities on chest radiographs may be suggestive of, but are not necessarily diagnostic of, TB. However, chest radiographs may be used to rule out the possibility of pulmonary TB in a person who has a positive reaction to the tuberculin skin test and no symptoms of the disease.
• Cavitation or consolidation of the apexes of the upper lobes of the lung or the tree-in-bud sign may be visible on an affected patient's chest X-ray.
• The tree-in-bud sign may appear on the chest CTs of some patients affected by tuberculosis, but it is not specific to tuberculosis

Diffuse bilateral, largely upper lobe, consolidation and pulmonary infiltrates. Suggestion of small area of cavitation at the left lung apex

left upper lobe cavitation




STOP TB