Embed Size (px)
Citation preview

KCIAPM SLIDE SEMINAR
ANAND DIAGNOSTIC LABORATORYANAND DIAGNOSTIC LABORATORY26/01/2014
CASE 1
35/F, LEFT HEMITHYROIDECTOMY35/F, LEFT HEMITHYROIDECTOMY
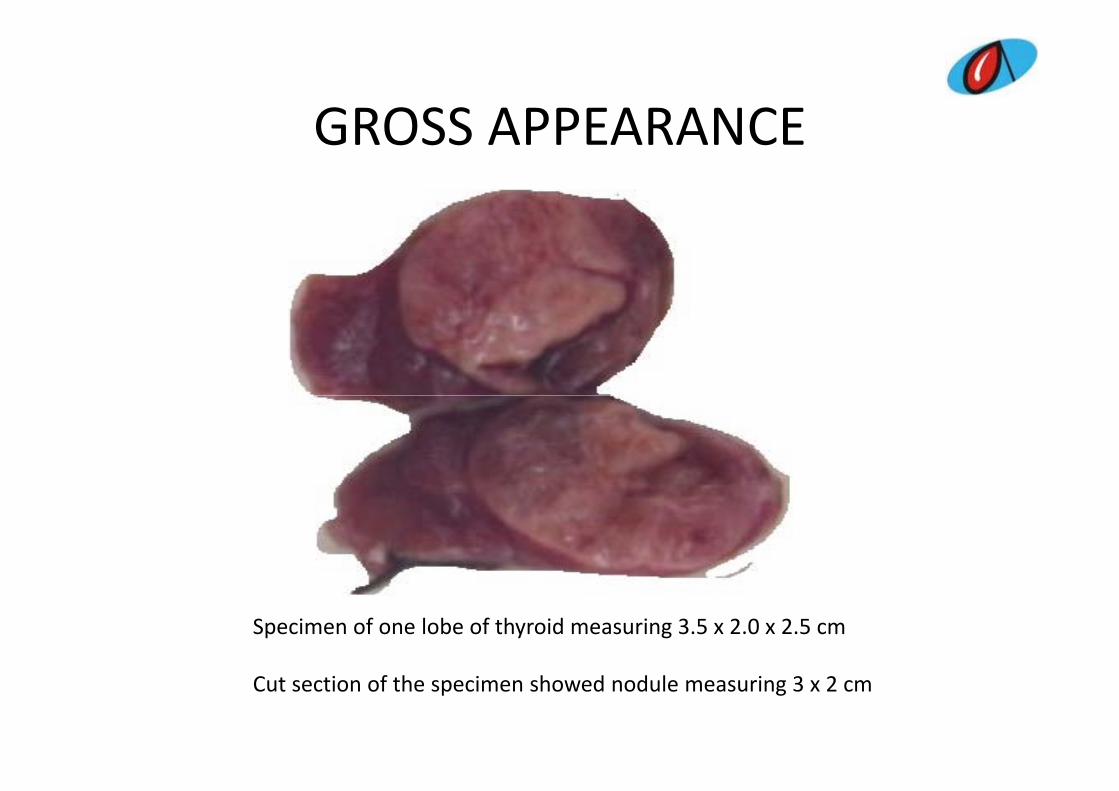
GROSS APPEARANCEGROSS APPEARANCE
Specimen of one lobe of thyroid measuring 3.5 x 2.0 x 2.5 cm
Cut section of the specimen showed nodule measuring 3 x 2 cm
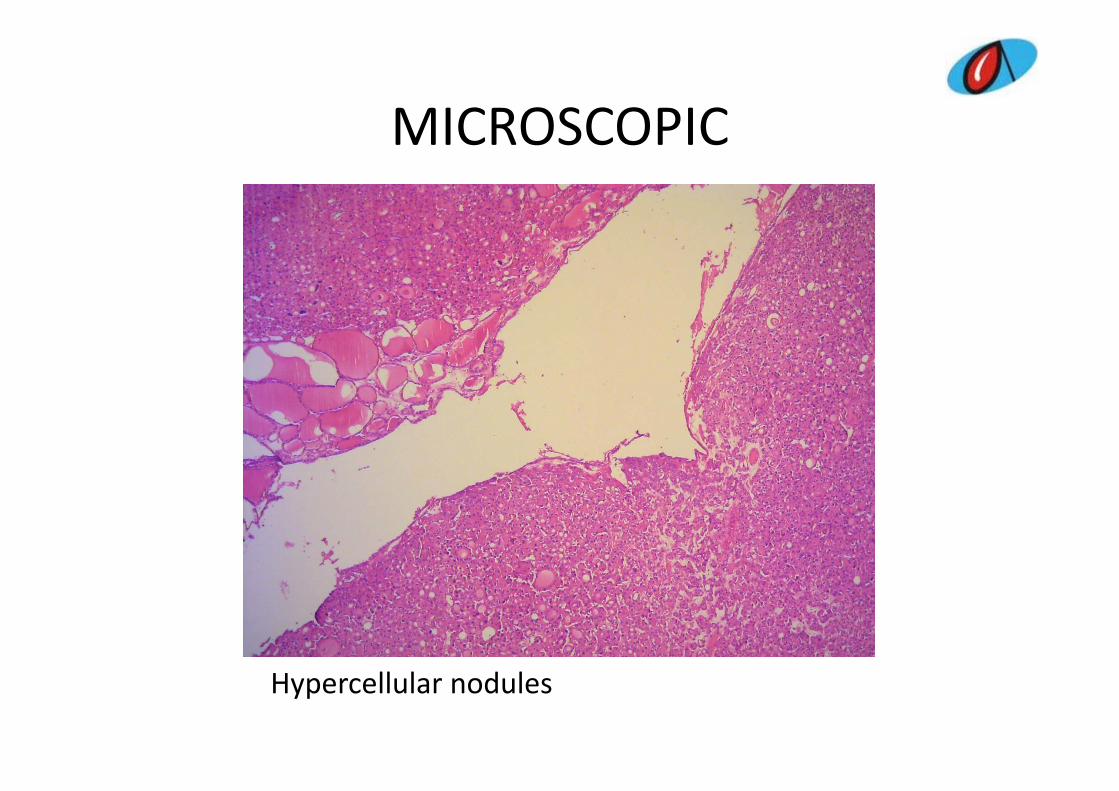
MICROSCOPICMICROSCOPIC
Hypercellular nodules
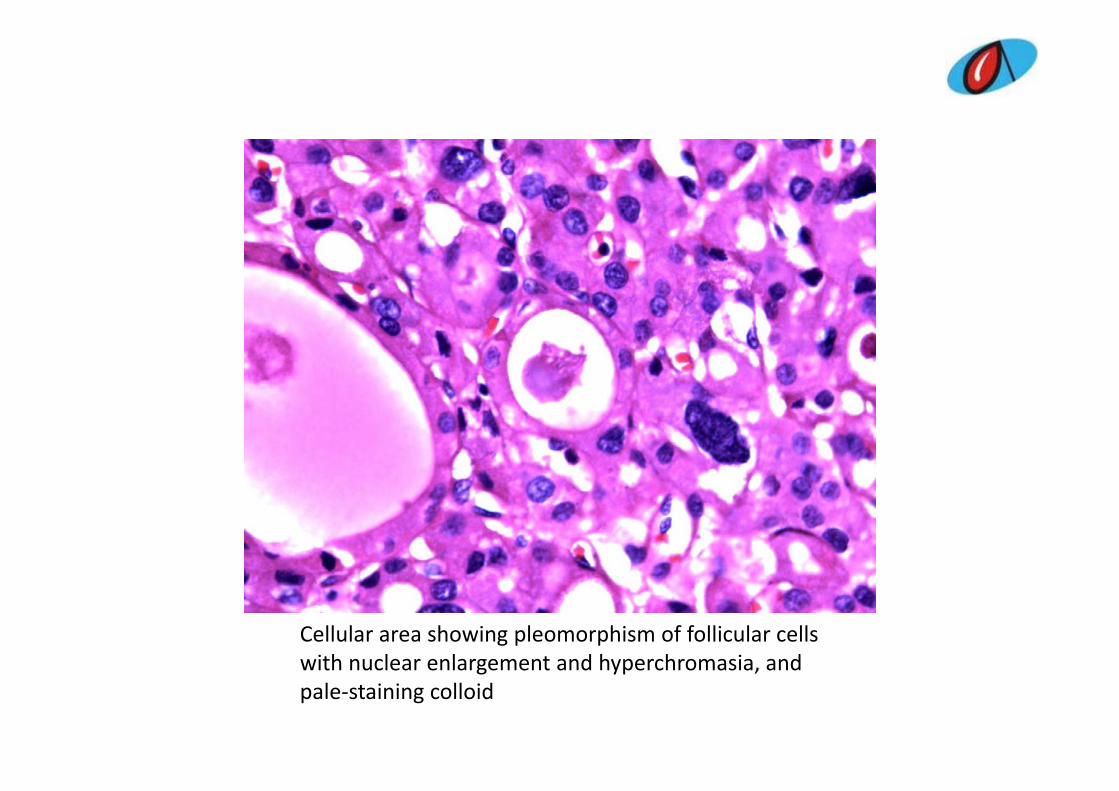
Cellular area showing pleomorphism of follicular cells with nuclear enlargement and hyperchromasia andwith nuclear enlargement and hyperchromasia, andpale‐staining colloid
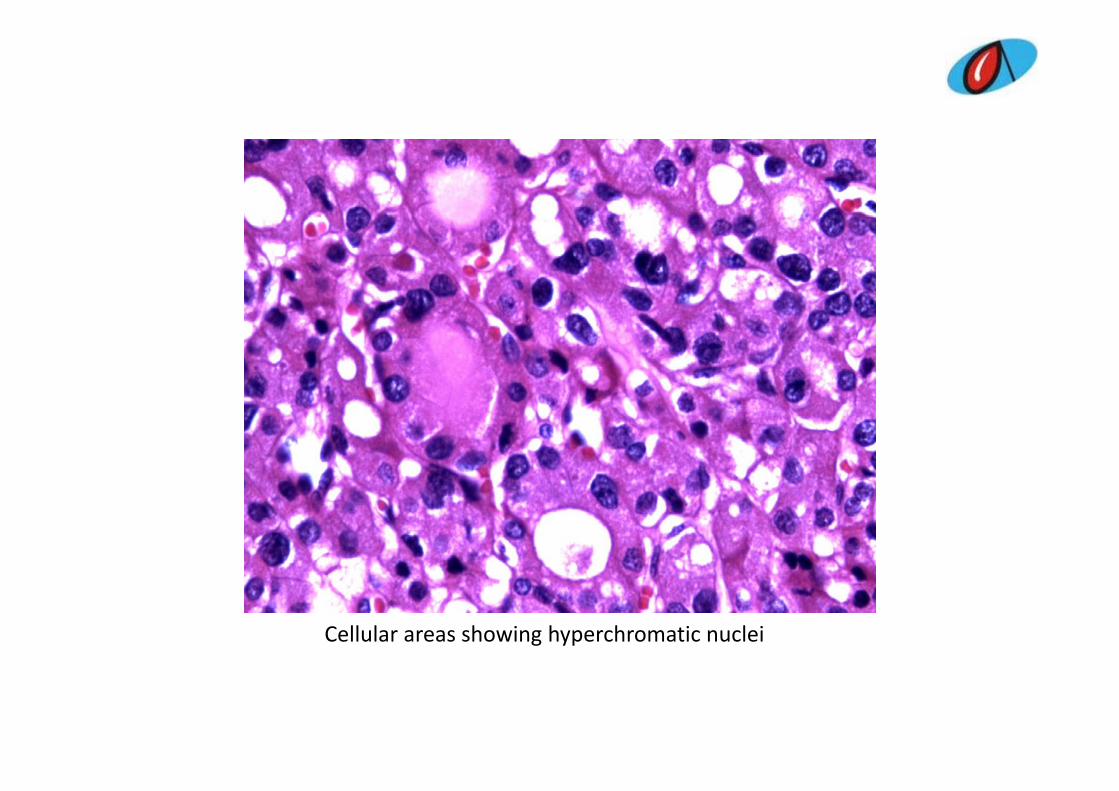
Cellular areas showing hyperchromatic nuclei
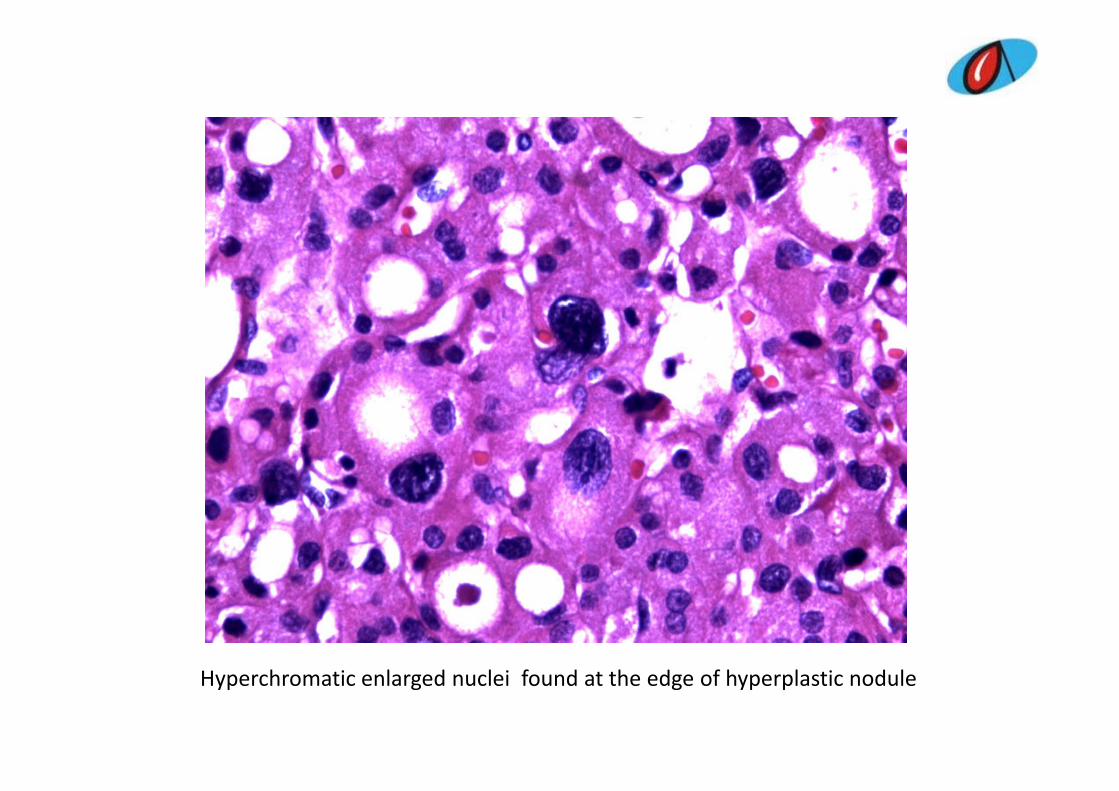
Hyperchromatic enlarged nuclei found at the edge of hyperplastic nodule
Differential diagnosisDifferential diagnosis • F lli l l ith h thl ll h• Follicular neoplasm with hurthle cell change• Hurthle cell neoplasm of unknown malignant potential• Papillary carcinoma (Hurtle/Follicular variant)• Nodular hyperplasia• Nodular goitre with atypical adenoma• Dyshormonogenetic goitre• Dyshormonogenetic goitre• Oncocytic parathyroid adenoma with atypia• Nodular goitre with adenomatous hyperplasia and radiation
hchanges• Follicular adenoma with bizarre nuclei• Parathyroid adenomay• MNG with atypical adenoma• Hurthlized colloid adenoma with bizarre nuclei
DIAGNOSIS OFFERED
DIAGNOSIS OFFERED Why it is ruled outFollicular neoplasm with Hurthle changes
No neoplasm, multiple nodules, no capsuleNo neoplasm multipleHurthle cell neoplasm / Unknown No neoplasm, multiple nodules, no capsule
Hurthle cell neoplasm / Unknown malignant potential Papillary carcinoma (Hurthle / N l fPapillary carcinoma (Hurthle / Follicular type) No nuclear features
More colloid, should show Nodular hyperplasia focal hyperplasia, no bizarre,
hyperchromatic nuclei.
Final diagnosisFinal diagnosis
• Dyshormonogenetic goitre
DIAGNOSISDIAGNOSIS
DYSHORMONOGENETIC GOITREDYSHORMONOGENETIC GOITRE• Hypercellular nodules with presence of cells
d i d i f lli l t b larranged in cords, microfollicular trabecular pattern.
• Presence of pale staining colloid• Presence of pale staining colloid• Nuclear pleomorphism, hyperchromatic and bizzare nucleibizzare nuclei.
• Presence of pleomorphism at the edge of the hyperplastic nodules and not in the entire glandhyperplastic nodules and not in the entire gland.
• Focal areas of fibrosis.
DYSHORMONOGENETIC GOITREDYSHORMONOGENETIC GOITRE
• Rare, inherited usually autosomal recessive disorder C i bl k i T3 /T4 th• Causing block in T3 /T4 pathway
• Defects involve TSH unresponsiveness– TSH unresponsiveness
– Defective iodine transport– Abnormal thyroid peroxidase y p– Formation of abnormal iodoprotein and defective deiodination of monoiodotyrosine and diiodotyrosineAbnormal th roglob lin s ntheses and e cretion– Abnormal thyroglobulin syntheses and excretion
• Rarely associated with deafness (Pendred’s syndrome)
DYSHORMONOGENETIC GOITREDYSHORMONOGENETIC GOITREMICROSCOPICMICROSCOPIC• Hypercellularity resulting from TSH stimulation of the gland• Cellular nodules of trabeculae, cords, with solid or microfollicular pattern
of epithelial cells with pale colloidof epithelial cells with pale colloid. • May have papillary foci, marked cellular pleomorphism . • Presence of pleomorphism at the edge of the hyperplastic nodules and
not in the entire glandnot in the entire gland.• Mitosis, bizarre hyperchromatic nuclei are seen.• True invasion is rare.
IMMUNOHISTOCHEMISTRY• Thyroglobulin positive• Calcitonin negativeRef :Vittal S, Chandrasekaran M, Bijai Kumar K, et al.DyshormonogeneticGoitre. JR Coll Surg Edinb;1993;38:205‐207
CASE 2
40/F, MASTECTOMY SPECIMEN/ ,CLINICAL DIAGNOSIS OF PHYLLODES TUMOR
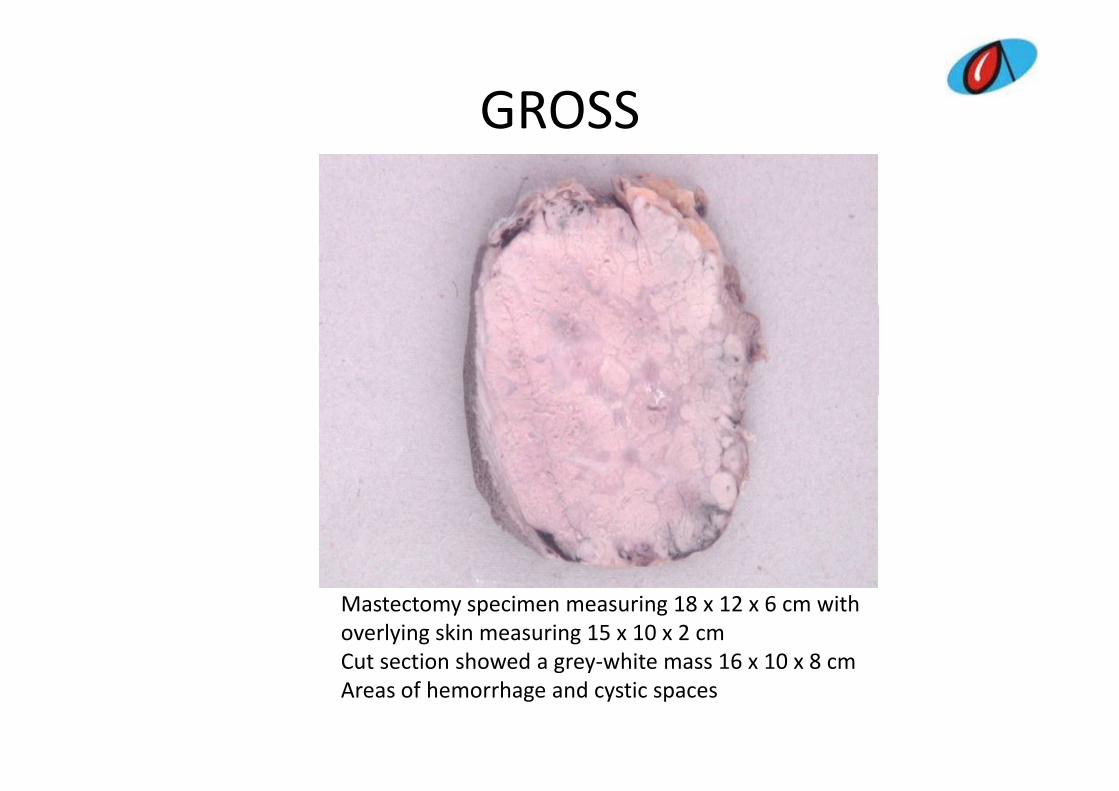
GROSSGROSS
Mastectomy specimen measuring 18 x 12 x 6 cm withoverlying skin measuring 15 x 10 x 2 cmCut section showed a grey‐white mass 16 x 10 x 8 cmCut section showed a grey white mass 16 x 10 x 8 cm Areas of hemorrhage and cystic spaces
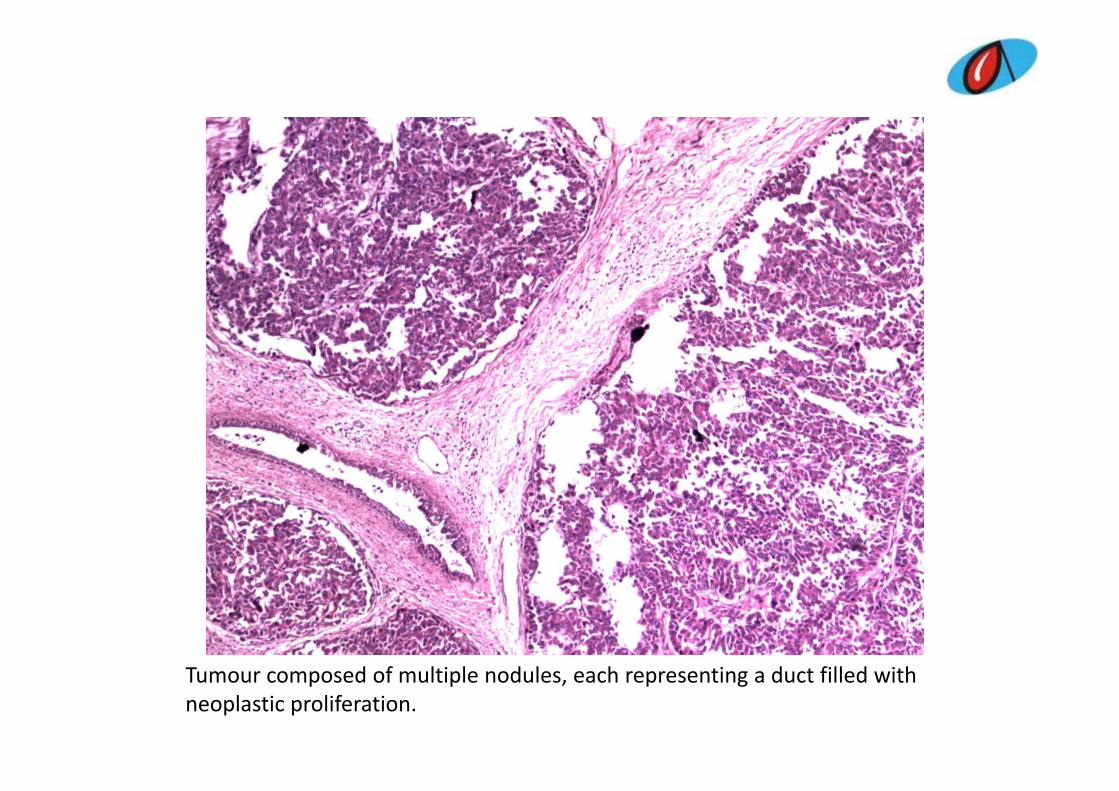
Tumour composed of multiple nodules, each representing a duct filled with neoplastic proliferation.
MICROSCOPICMICROSCOPIC
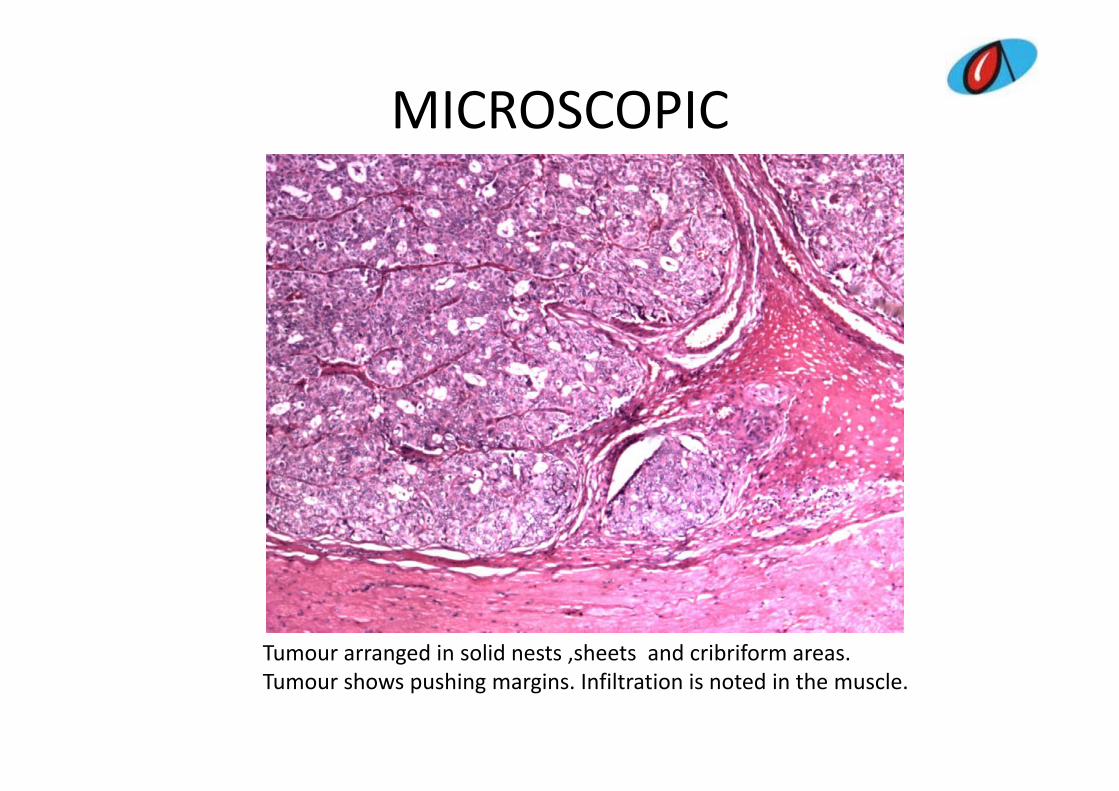
Tumour arranged in solid nests ,sheets and cribriform areas. Tumour shows pushing margins. Infiltration is noted in the muscle.
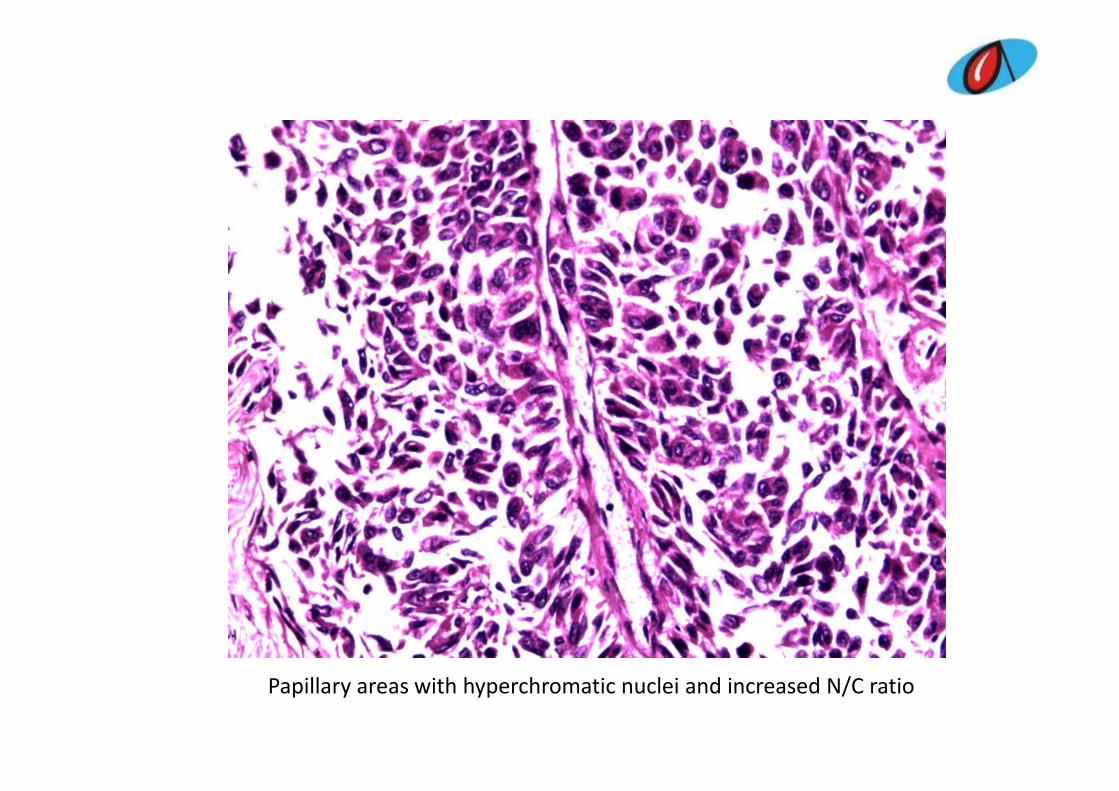
Papillary areas with hyperchromatic nuclei and increased N/C ratio
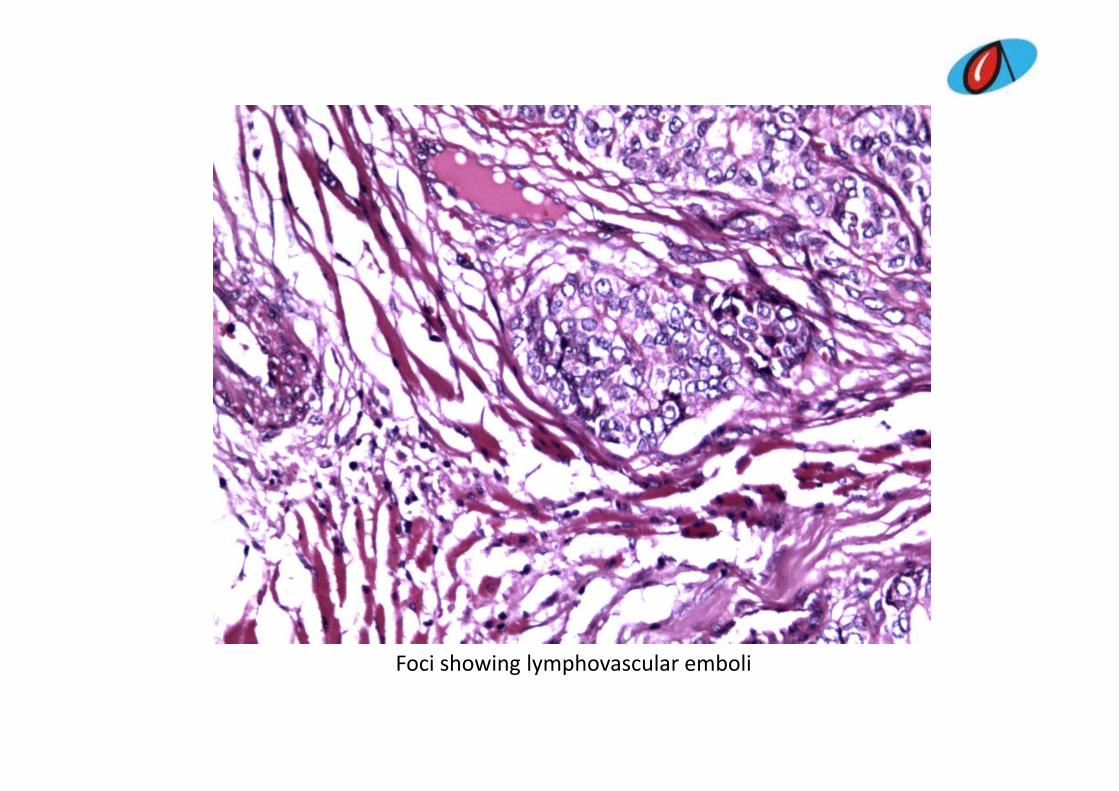
Foci showing lymphovascular emboliFoci showing lymphovascular emboli
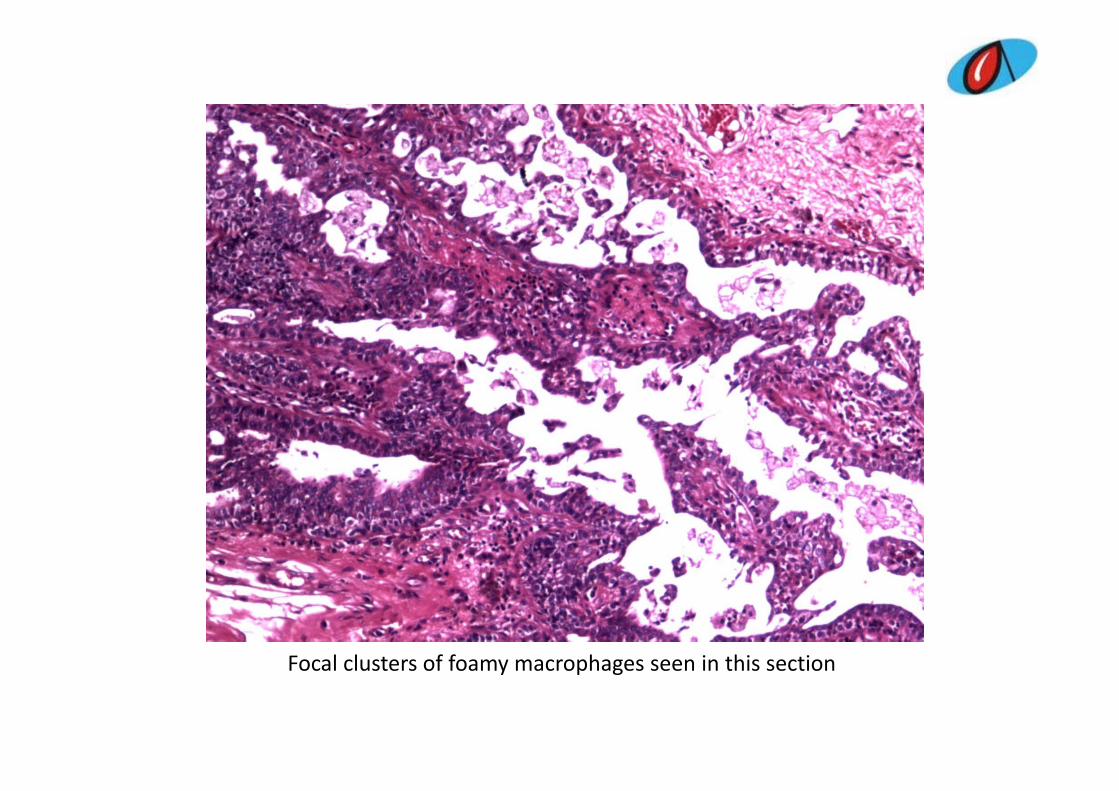
Focal clusters of foamy macrophages seen in this sectionFocal clusters of foamy macrophages seen in this section

Differential diagnosisDifferential diagnosis
ill i• Papillary carcinoma– ? Primary, ? Secondary
• Papillary transitional carcinoma• Papillary carcinoma in situp y• Micropapillary carcinoma with invasion• Invasive papillary carcinoma• Invasive papillary carcinoma• Adenomyoepithelioma• Malignant myoepithelioma• Papillary carcinoma with solid and papillary areas
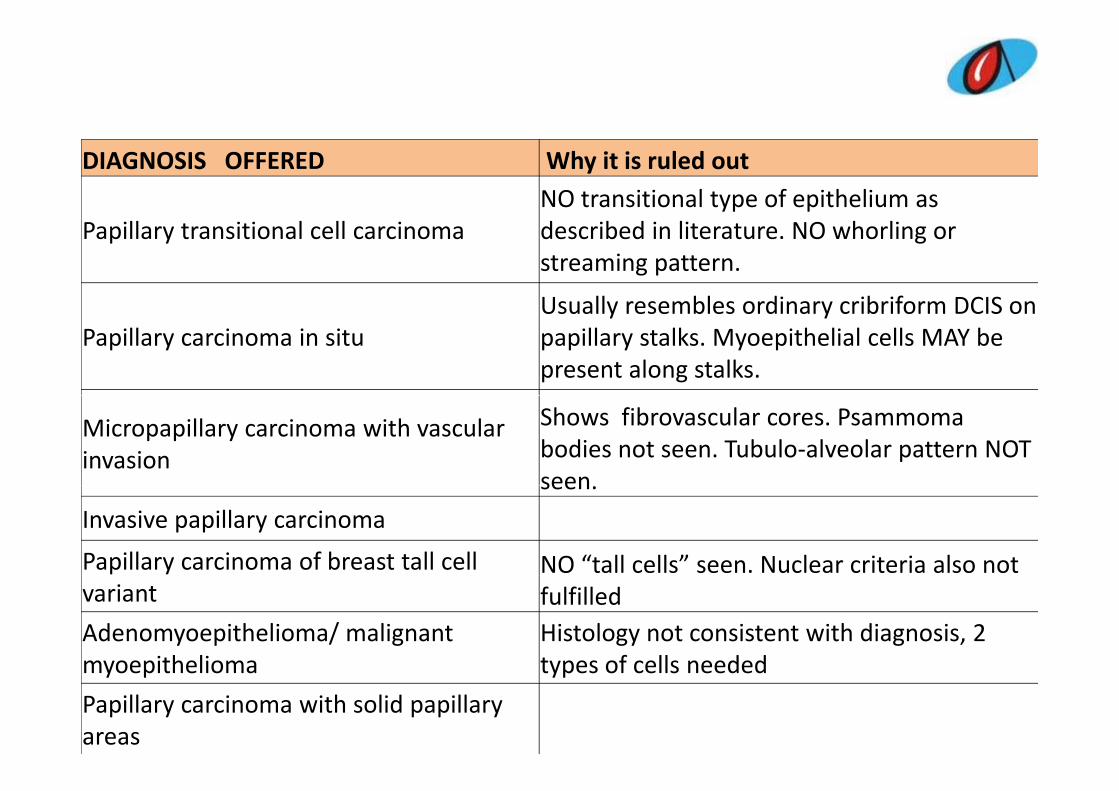
DIAGNOSIS OFFERED Why it is ruled outNO transitional type of epithelium as
Papillary transitional cell carcinoma described in literature. NO whorling or streaming pattern.
Usually resembles ordinary cribriform DCIS onPapillary carcinoma in situ
Usually resembles ordinary cribriform DCIS on papillary stalks. Myoepithelial cells MAY be present along stalks.
Micropapillary carcinoma with vascular invasion
Shows fibrovascular cores. Psammomabodies not seen. Tubulo‐alveolar pattern NOT seenseen.
Invasive papillary carcinoma
Papillary carcinoma of breast tall cell NO “tall cells” seen. Nuclear criteria also not variant fulfilledAdenomyoepithelioma/ malignant myoepithelioma
Histology not consistent with diagnosis, 2 types of cells neededmyoepithelioma types of cells needed
Papillary carcinoma with solid papillary areas
DIAGNOSISDIAGNOSIS
S lid i t f i i ill iSolid variant of invasive papillary carcinoma• Multiple nodules, each representing a duct filled with neoplastic proliferation Cells are ovoid towith neoplastic proliferation. Cells are ovoid to spindle exhibiting solid pattern with fibrovascular networknetwork.
• Other features observed were microcystic spaces and foamy macrophages.and foamy macrophages.
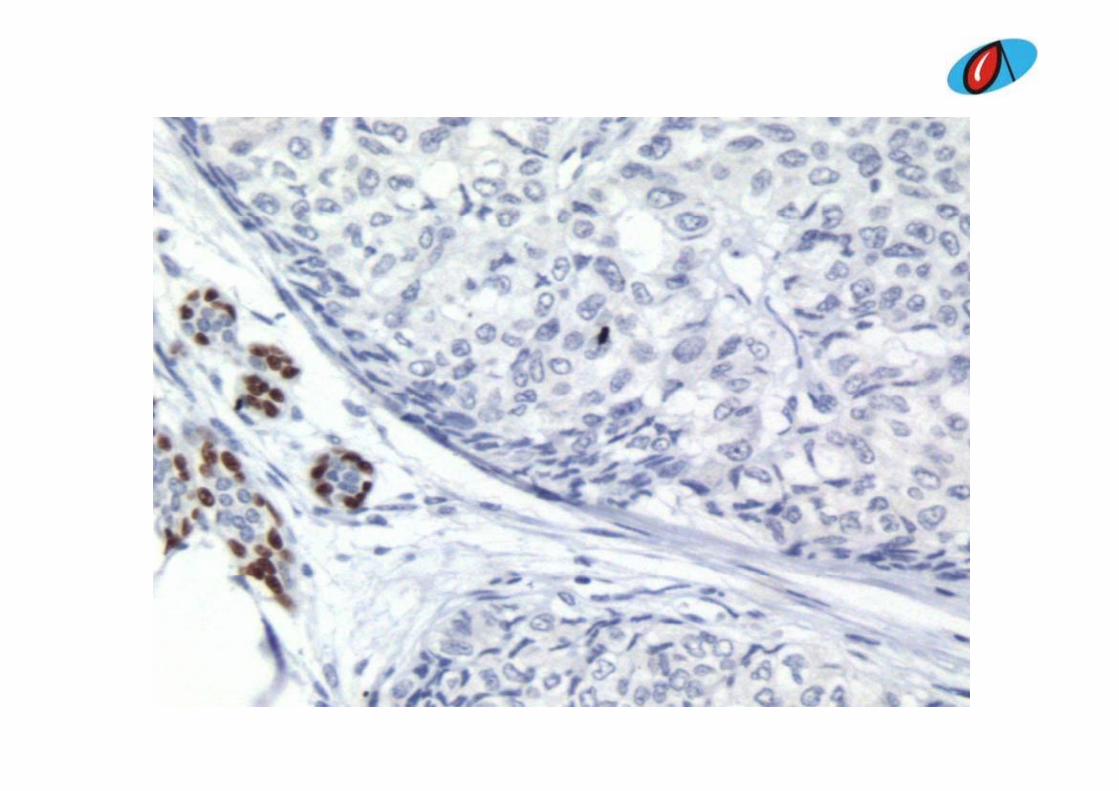
• Well defined pushing borders• ER positive PR focally positive P63 negativeER positive, PR focally positive, P63 negative.
SOLID VARIANT OF INVASIVE PAPILLARY CARCINOMA
A di ti t li i l tit• A distinct clinical entity . • Controversial whether they could be considered low grade tumourslow–grade tumours
• Originate from large or dilated ductsP i ff ld i ll i• Primary affect older women occasionally seen in women below 50 years of age90% il t l d i i th t l f th• 90% unilateral and arise in the central area of the breast
• Present with a bloody nipple discharge• Present with a bloody nipple discharge• Nodular configuration and well circumscribed
SOLID VARIANT OF INVASIVE PAPILLARY CARCINOMA
Mi i ll th t h lti l d l• Microscopically these tumours show multiple nodules, each representing a duct filled with neoplastic proliferation. Cells are ovoid to spindle exhibiting solid p p gpattern with fibrovascular network.
• Other features observed may be organoid pattern, i ti d f hmicrocystic spaces and foamy macrophages
• Well defined pushing borders• Positive for ER and PR• Positive for ER and PR• Negative for CK5/6.• Other markers useful in diagnosis include Calponin• Other markers useful in diagnosis include Calponin, P63, Skeletal muscle myosin heavy chain
ReferencesReferences
• Tavassoli FA, Devilee P. World Health Organization Classification of Tumours, Tumours of the Breast and Female Genital Organs.2nd edition,LyonFrance: IARC Press.
• Gallager HS.Pathological types of breast cancer: their prognosis Cancer 1984;53:623‐629their prognosis.Cancer.1984;53:623‐629.
• Pettinato G, Manivel CJ, Panico L etal.Invasivei ill i f h b Climicropapillary carcinoma of the breast;Am J Clin
Pathol.2004:121(6) 857‐866.
CASE 3CASE 3
21/F, TOTAL THYROIDECTOMY SPECIMEN21/F, TOTAL THYROIDECTOMY SPECIMEN
GROSSGROSS
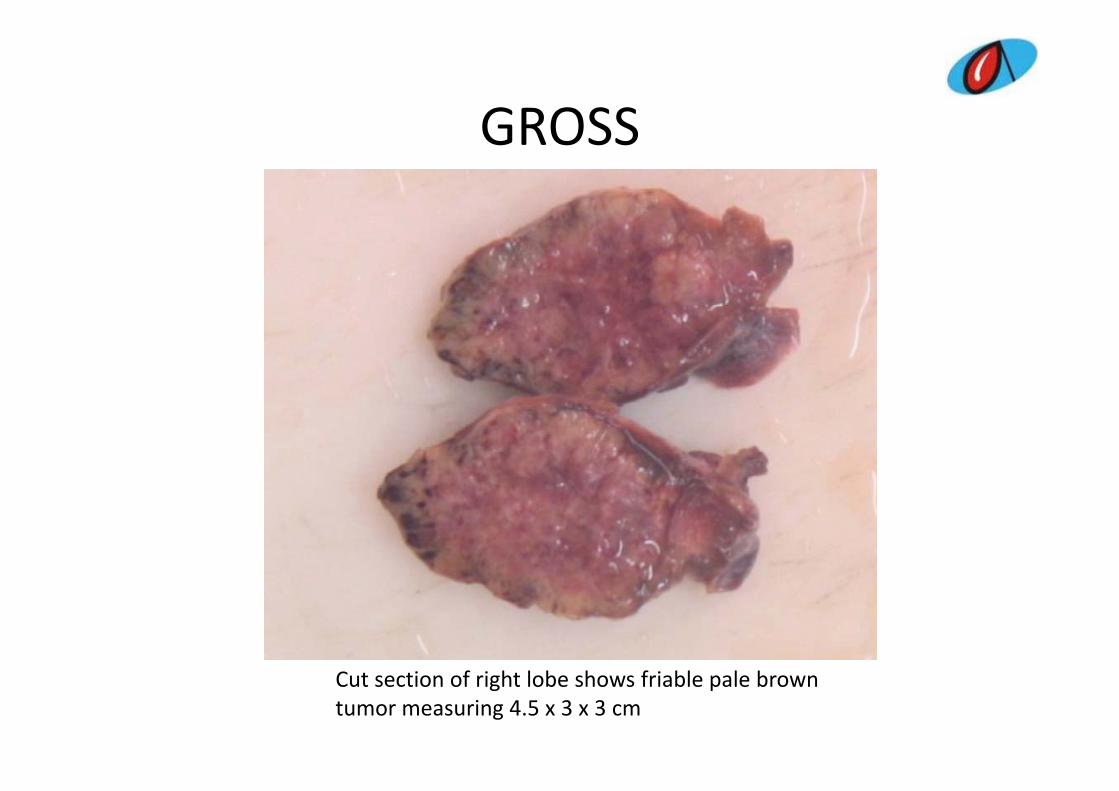
Total Thyroidectomy specimen measuring 7 x 6 x 3 5 cmTotal Thyroidectomy specimen measuring 7 x 6 x 3.5 cmEnlarged right lobe
GROSSGROSS
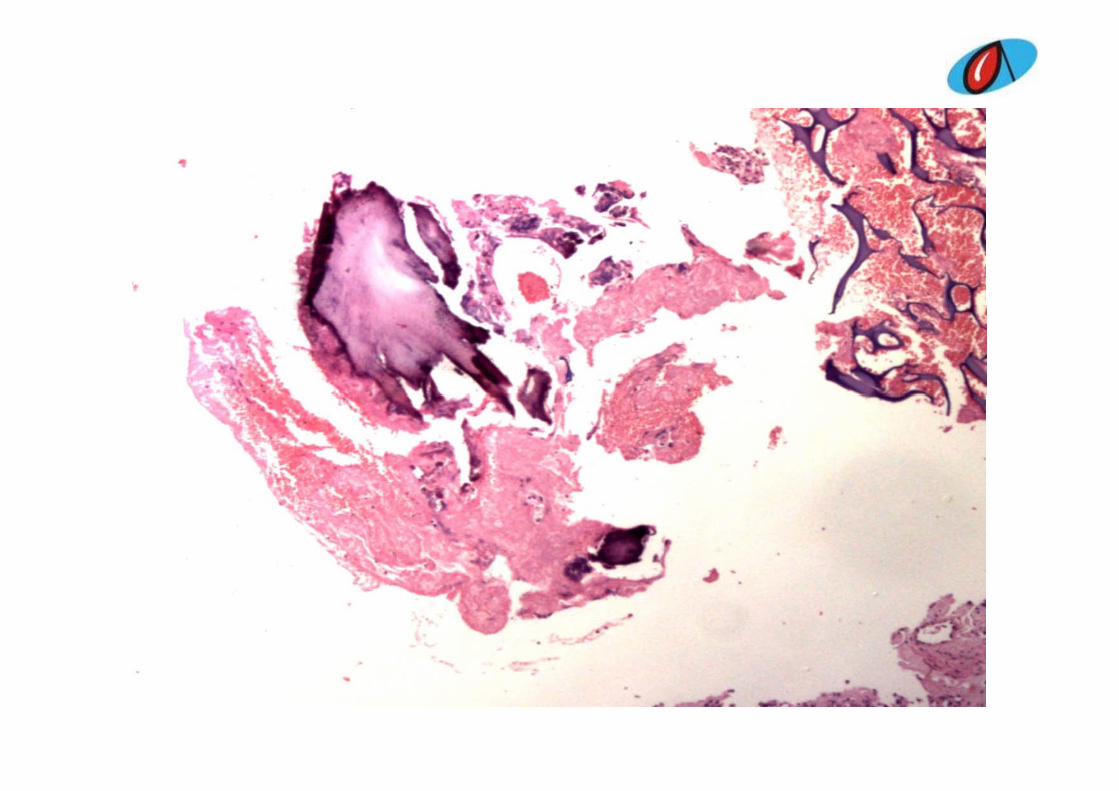
Cut section of right lobe shows friable pale brown tumor measuring 4.5 x 3 x 3 cm
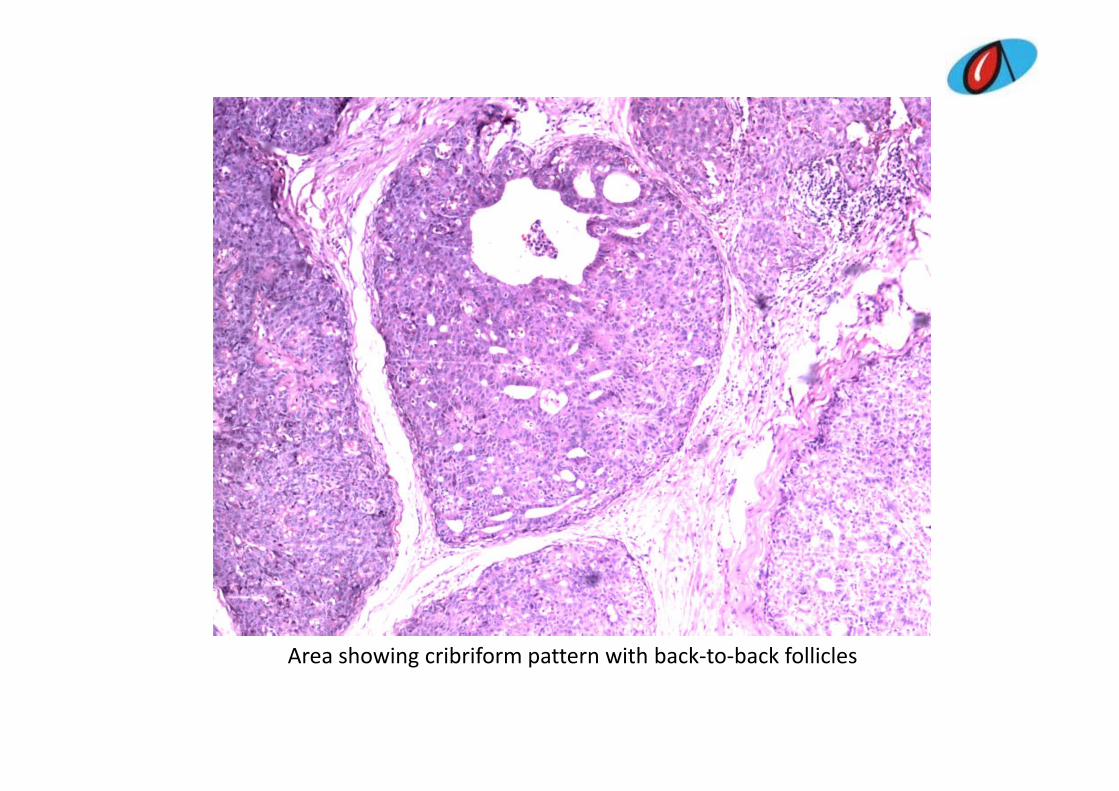
Area showing cribriform pattern with back‐to‐back folliclesg p

Cribriform areas under higher magnificationCribriform areas under higher magnification
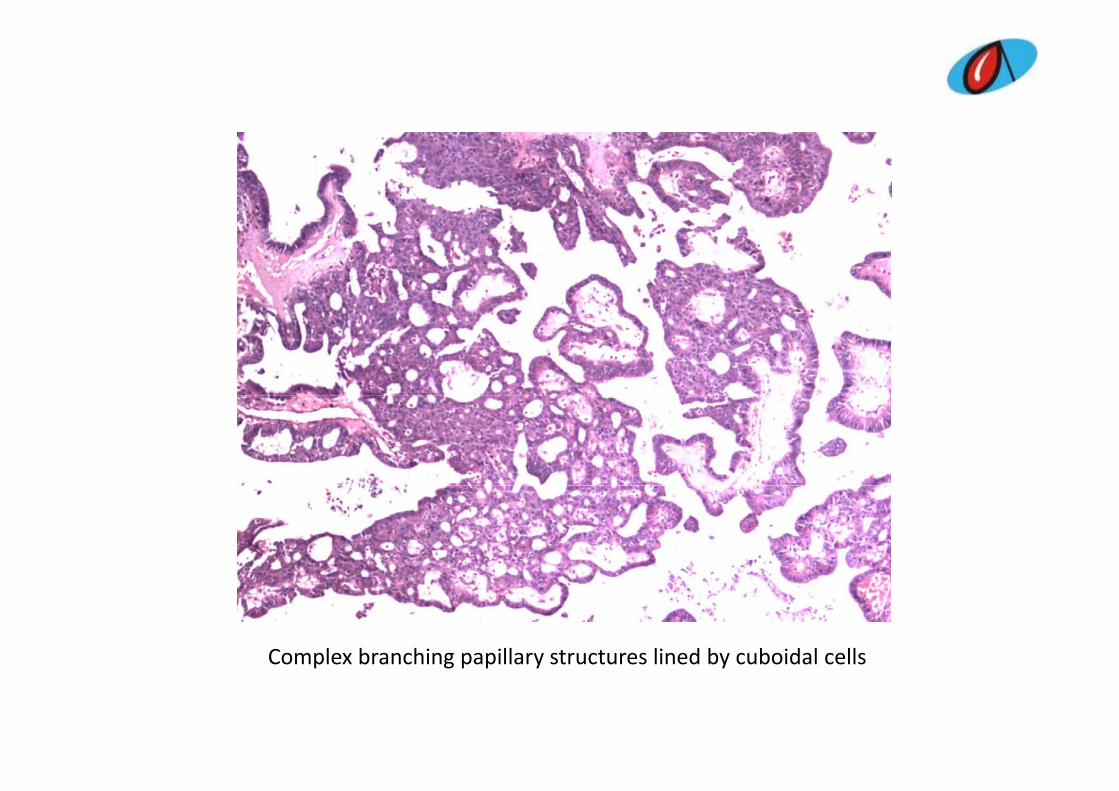
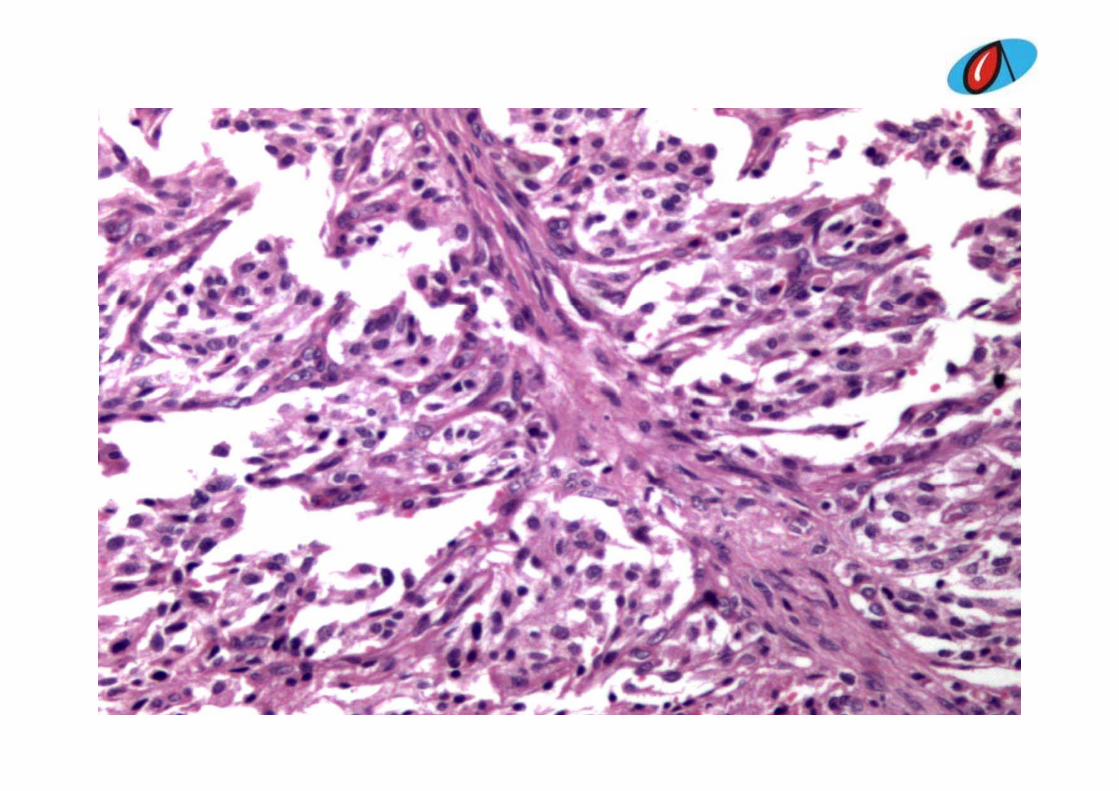
Complex branching papillary structures lined by cuboidal cellsp g p p y y

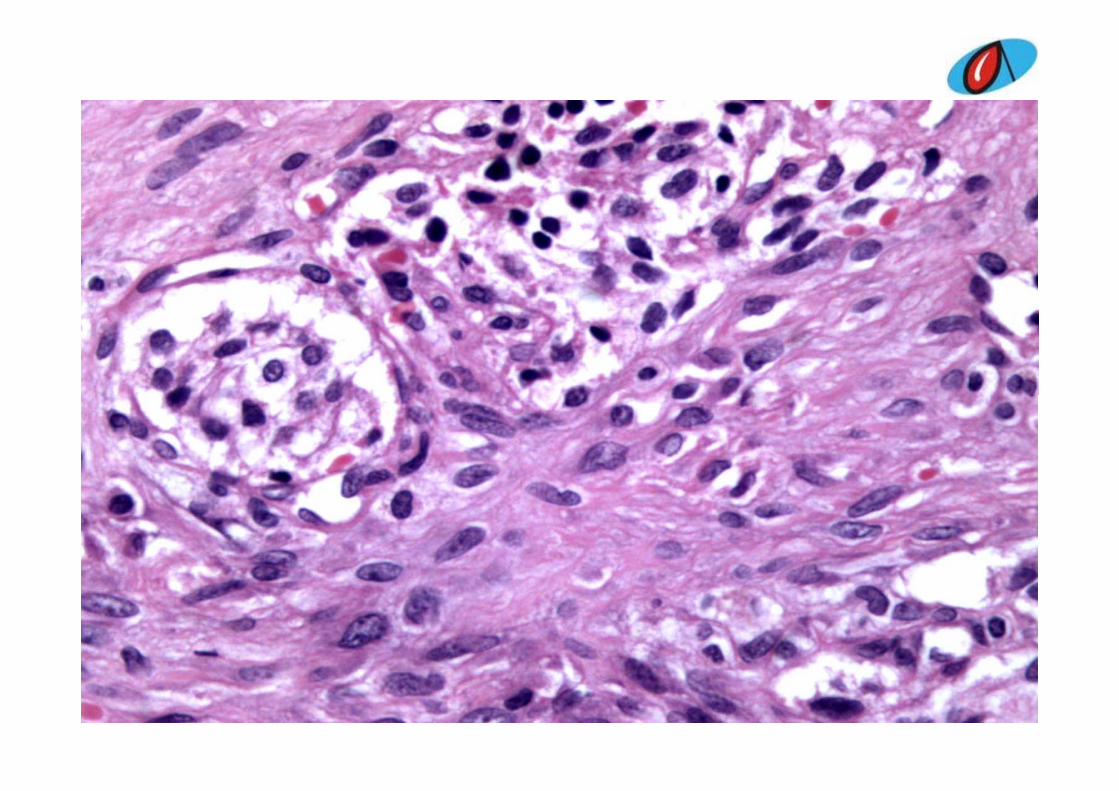
Focal areas showing squamoid nodules without evidence of keratinizationFocal areas showing squamoid nodules without evidence of keratinization
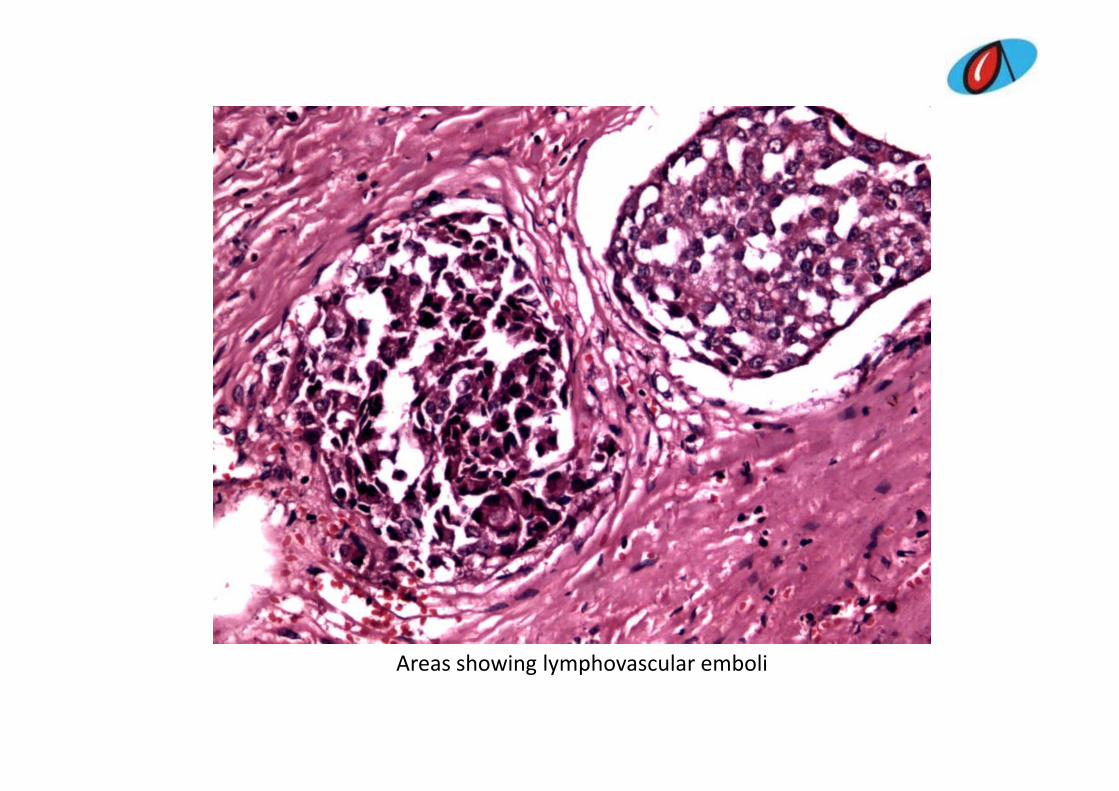
Areas showing lymphovascular emboliAreas showing lymphovascular emboli
Differential diagnosisDifferential diagnosis
• Mixed medullary and papillary carcinoma• Morular cribriform variant of papillary carcinomap p y• Papillary carcinomaC l ll i• Columnar cell carcinoma
• Tall cell variant of papillary carcinoma• Papillary carcinoma follicular variant• Diffuse sclerosing variant• Diffuse sclerosing variant• Papillary variant of medullary carcinoma
DIAGNOSIS OFFEREDDIAGNOSIS OFFEREDDIAGNOSIS OFFERED Why it is ruled outDIAGNOSIS OFFERED Why it is ruled outPapillary cell carcinoma
ll llNuclear features of PTC present.
d ' f f ' llTall cell variant However, doesn't satisfy criteria of 'tall cells'Lymphocytic infiltrate usually seen along
Diffuse sclerosing variant with other features with prominent sclerosing areas.Papillae are lined by multiple layers of
Papillary variant of medullarycarcinoma
p y p yneoplastic cells with small and irregular nuclei containing condensed chromatin. Lack typical nuclear features of papillaryLack typical nuclear features of papillary carcinoma
Papillary thyroid carcinoma‐C ib if l ( ith f i fCribriform morular (with foci of tall cell variant )
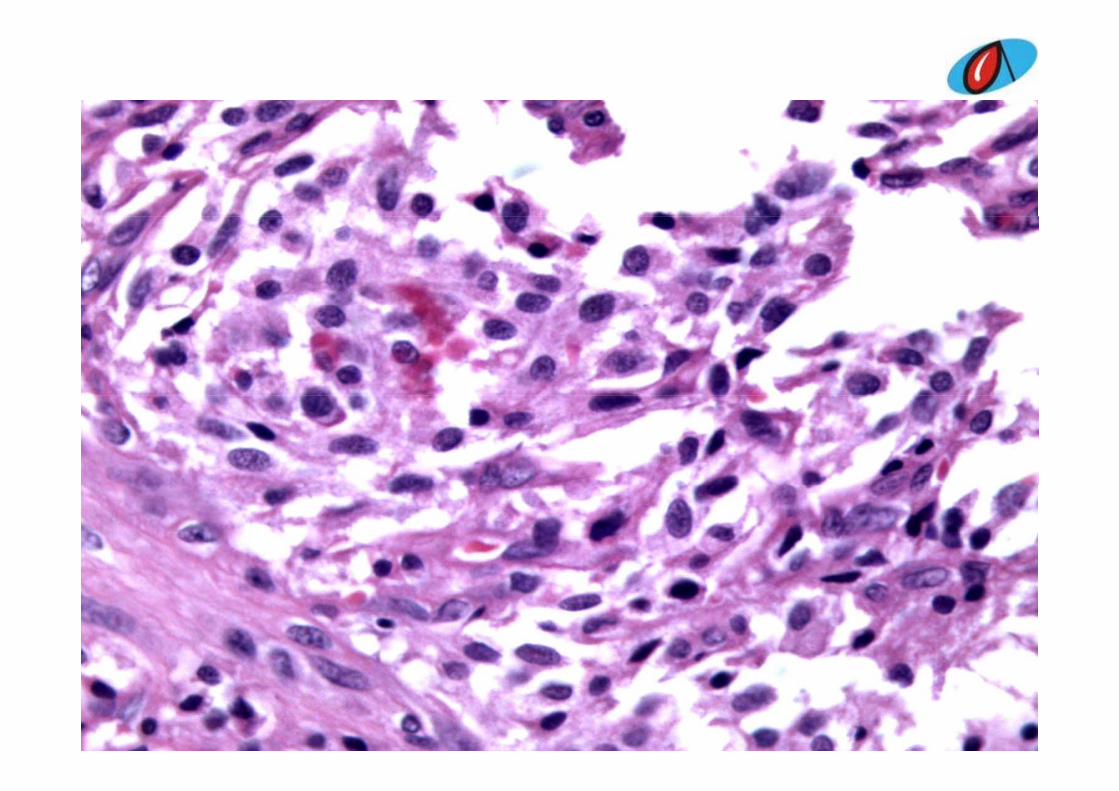
DIAGNOSISDIAGNOSISPapillary Thyroid carcinoma (PTC) Cribriform‐morularPapillary Thyroid carcinoma (PTC) Cribriform morular variant.• Complex branching papillae lined by cuboidal cells• Complex branching papillae, lined by cuboidal cells. Nuclei are hyperchromatic, optically clear, with longitudinal grooves There is a blending of severallongitudinal grooves .There is a blending of several histological patterns .
• Cribriform areas with back to back crowding with• Cribriform areas with back to back crowding, with arches of cells in the absence of intervening fibrovascular stromafibrovascular stroma
• Solid areas consisting of morules of squamoid cells that do not show any keratinization or intercellular bridges.
Papillary Thyroid Carcinoma Cribriform‐Morular Variant
• PTC (C‐MV) is rare morphologic entity• First described by Harach et al in association with FAP ( FAMILIAL
ADENOMATOSIS POLYPOSIS)• Commonly seen in young females usually less than 30 years of
age• Gross well circumscribed, somewhat lobulated mass, ranging
from 1 5 2 cms in size Sometimes show multiple satellitefrom 1.5‐2 cms in size. Sometimes show multiple satellite nodules
• PTC (C‐MV) carries a better prognosis than other aggressive• PTC (C‐MV) carries a better prognosis than other aggressive variants of PTC ( tall cell, columnar, diffuse sclerosing and diffuse follicular types) yp )
REFERENCESREFERENCES
• Harach HR, Williams GT, Williams ED. Familial adenomatous polyposis associated with thyroidadenomatous polyposis associated with thyroid carcinoma: a distinct type of follicular cell neoplasm Histopathology 1994;6: 549‐561neoplasm. Histopathology.1994;6: 549 561.
• Cameselle‐TeijeiroJ Chan JK Cribriform‐morular• Cameselle‐TeijeiroJ, Chan JK. Cribriform‐morular vriant of papillary carcinoma; a distinctive variant presenting the sporadic counterpart of familial p g p p f fadenomatous polyposis associated thyroid carcinoma? Mod Pathol.1999;4: 400‐411.

CASE 4CASE 4CASE 4CASE 4
CLINICAL PRESENTATIONCLINICAL PRESENTATION
Female , 39 years old
Complaints of fever and cough since 2 months
P t hi t f l t b l i 4 b k Past history of pulmonary tuberculosis 4 years back
LAB INVESTIGATIONSLAB INVESTIGATIONS
BronchoscopyBronchoscopy
Bronchial wash – AFB and cytology
CT scan
RML biopsy
Bronchoscopy - mass occluding right middle lobe bronchus
Bronchial wash – AFB – negative
Cytology – negative for atypical cells
CT scan –
soft tissue density mass measuring 5.4 x 5.7 x 5.8 cms in the right
middle lobe of lung in the perihilar region.
Enlarged pretracheal and subcarinal group of lymph nodes Enlarged pretracheal and subcarinal group of lymph nodes
largest measuring 2.1 x 1.3 cms.
Features suggestive of BRONCHOGENIC CARCINOMA with
metastasis to pretracheal and subcarinal lymphnodes.
Biopsy –
Gross - grey white tissue fragment measuring 0.2x0.2x0.1 cms.
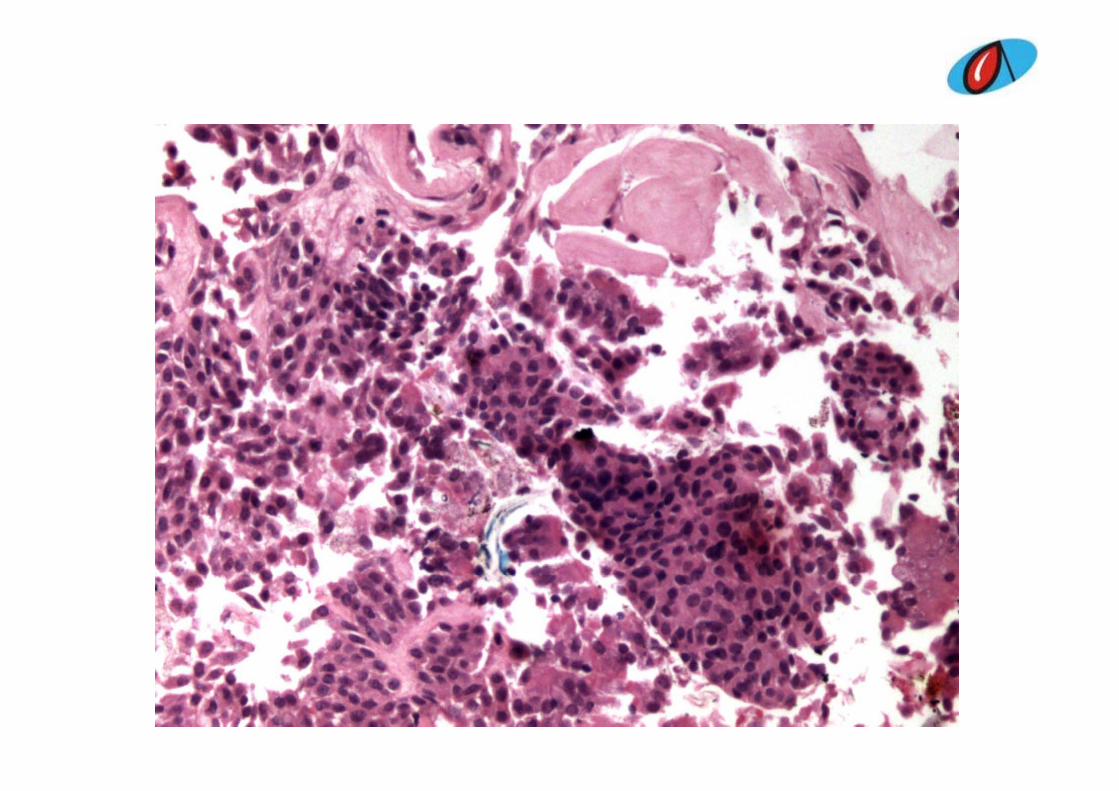
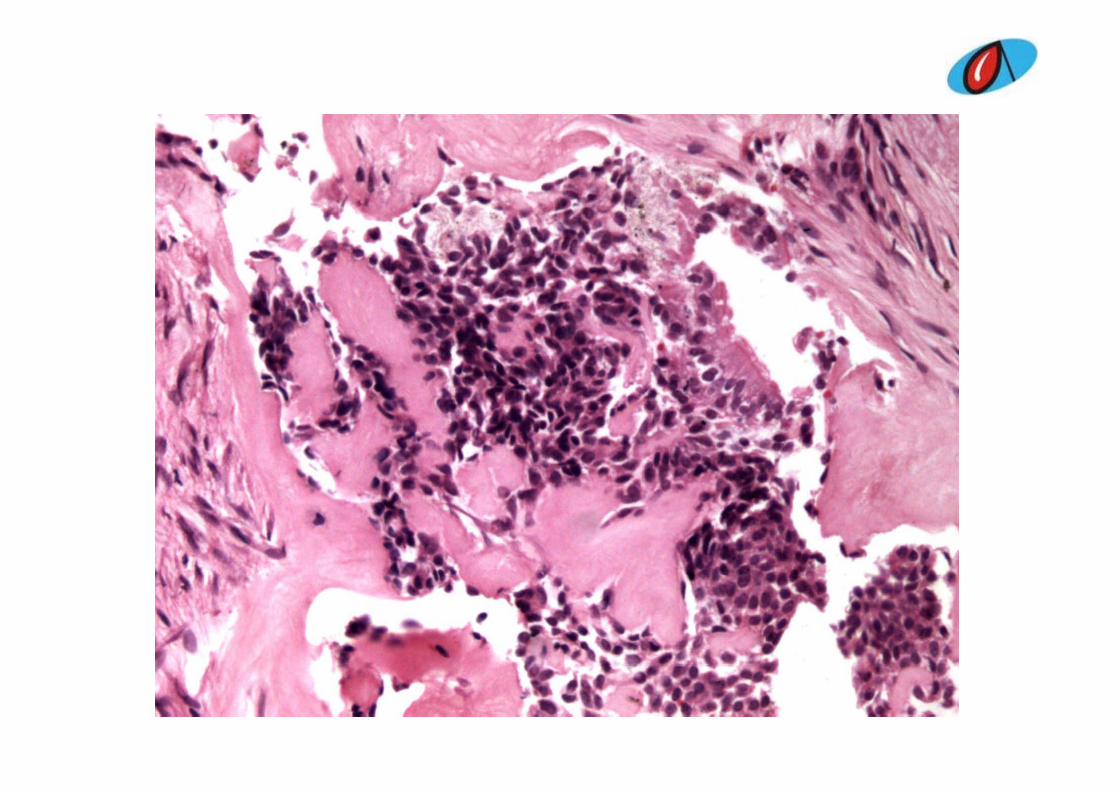
Microscopy – small sized bland appearing tumor cells with
round to oval nucleus arranged in sheets and separated by
hyalinized stroma. y
I i F t f i b i l f li Impression – Features favoring a benign neoplasm of salivary
gland type; possibility of myoepithelioma is suggested.
PERPER‐‐OPERATIVEOPERATIVE
Right posterolateral thoracotomy, bilobectomy and lymph node clearance
Per operative findings – hard mass measuring about 6 x 4 cms
in right middle lobe. Mutiple subcarinal and paratracheal
lymphnodes.
HISTOPATHOLOGYHISTOPATHOLOGY
Gross – right middle and lower lobes of lung. Tumor with pushing
margins in the middle lobe with occlusion of bronchus. Tumorg
6 x 5 x 4 cms. Yellow white appearance. Lymph node
dissection , largest node 2.5 x 1.0 x 0.5 cms.



Microscopy -
Tumor composed of squmaous cells, intermediate cells and
mucin secreting cells.
All lymph nodes exhibit reactive changes All lymph nodes exhibit reactive changes.
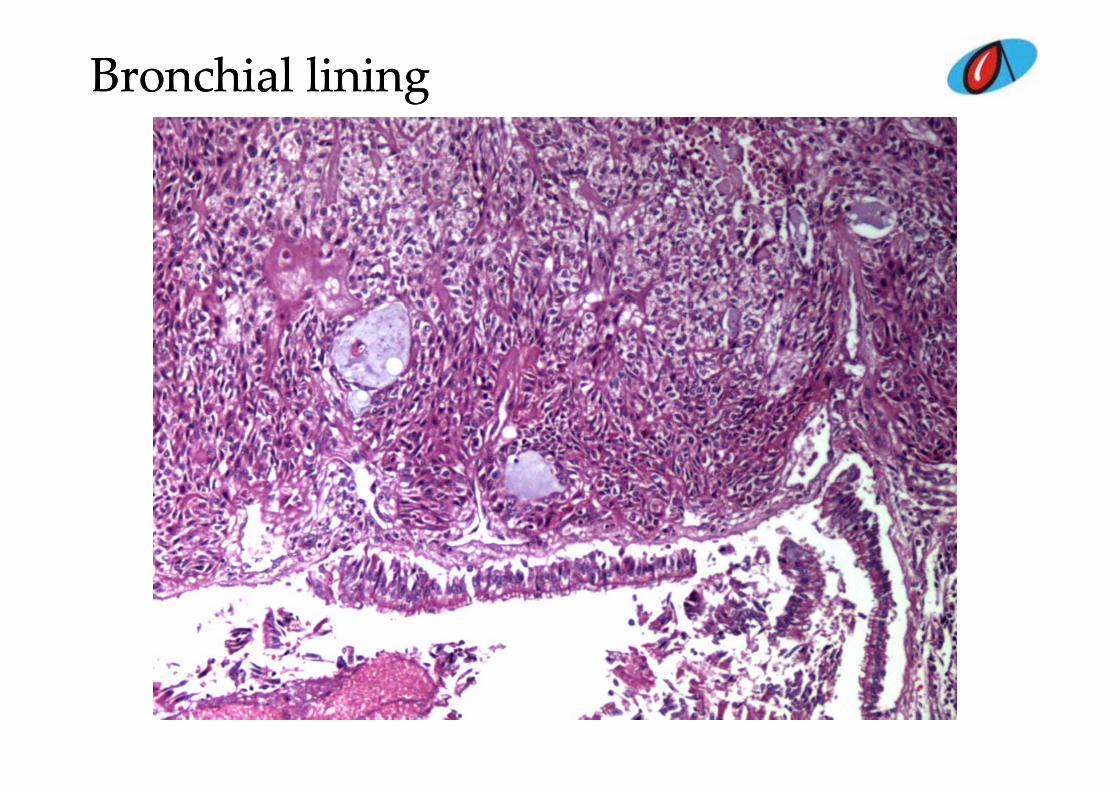
Bronchial lining Bronchial lining
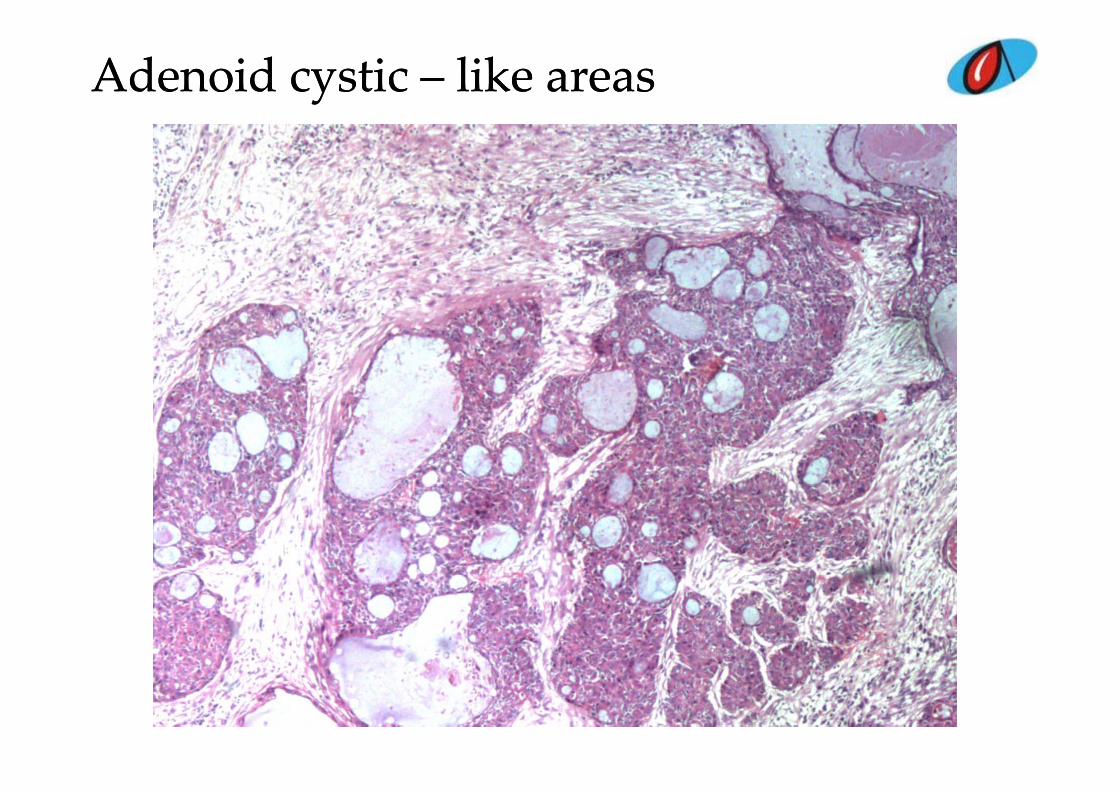
Adenoid cystic Adenoid cystic –– like areaslike areas
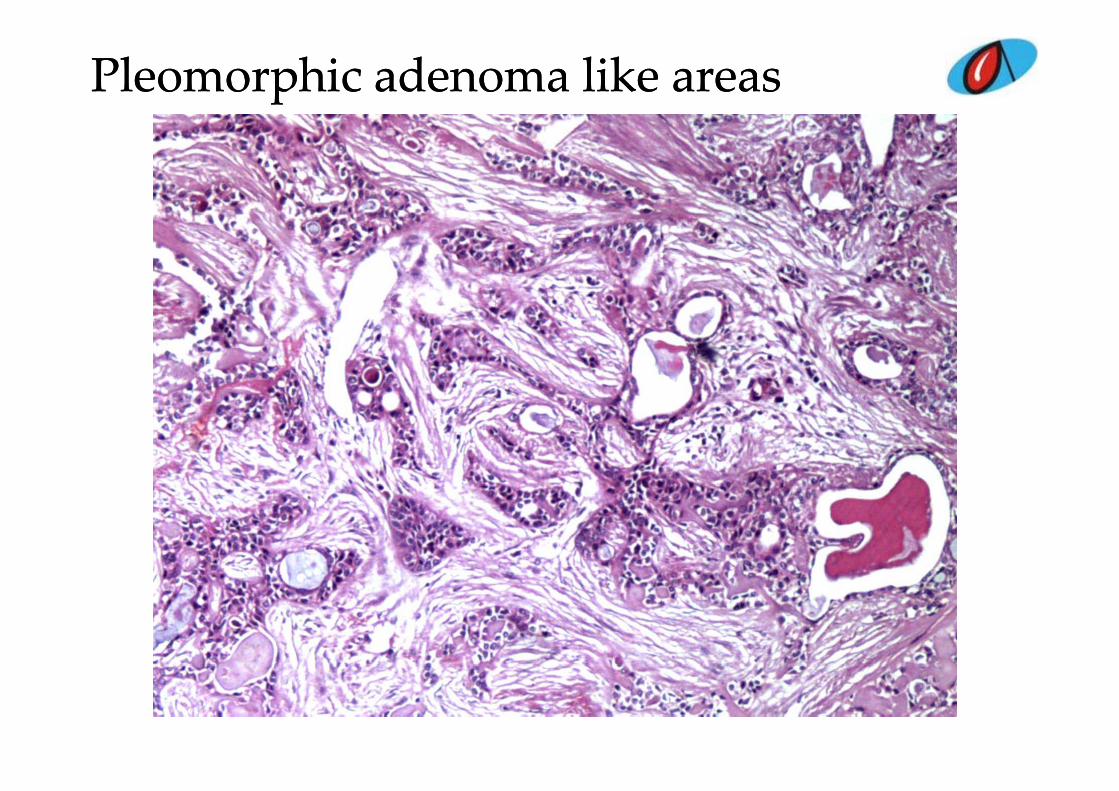
PleomorphicPleomorphic adenoma like areasadenoma like areas
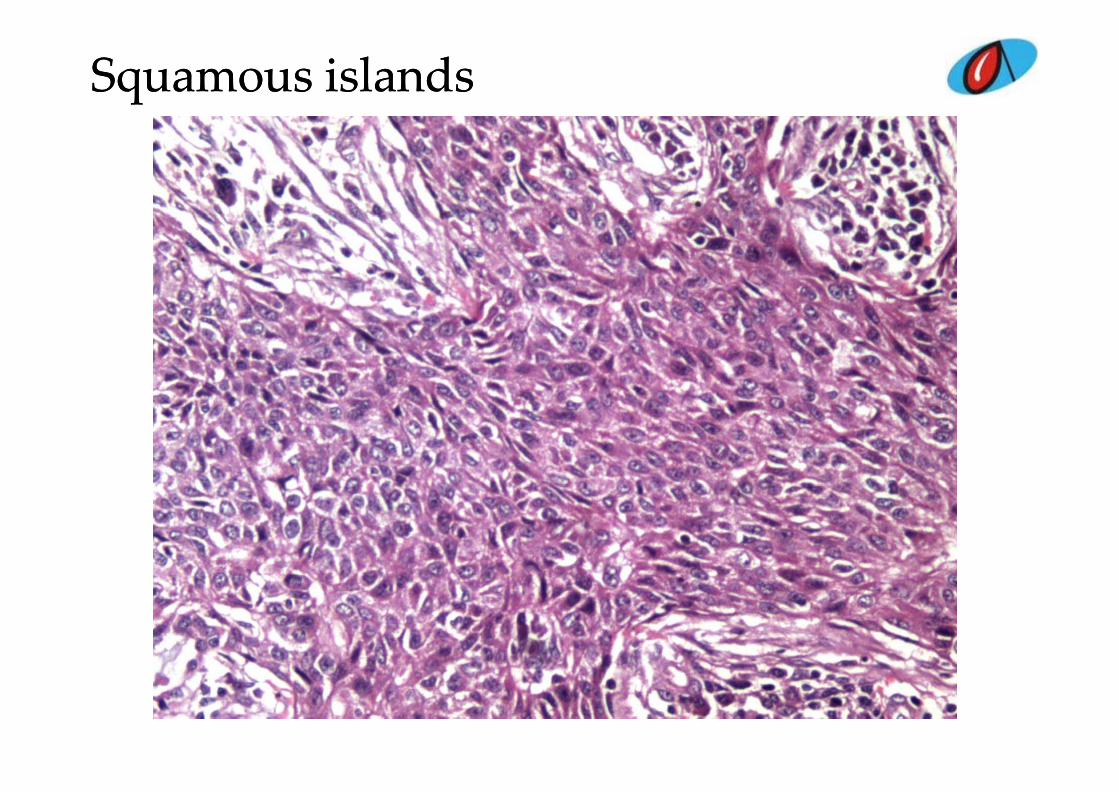
SquamousSquamous islandsislands
DIFFERENTIALS DIFFERENTIALS
L ll diff ti t d i• Large cell undifferntiated carcinoma• Large cell neuroendocrine carcinoma• Mucoepidermoid carcinomaMucoepidermoid carcinoma• Squamous cell carcinoma• Lymphoepithelioma like carcinoma• Adenoid cystic carcinoma• Neuroendocrine tumor
Ad i• Adenosquamous carcinoma• Adenoid cystic variant of diffuse malignant mesothelioma-
biphasic type with ? Asbestosisp yp• Neuroendocrine carcinoma mixed variant
Impression –
low grade salivary epithelial neoplasm, ? Low grade
mucoepidermoid carcinoma , ? Pleomorphic adenoma.
IMMUNOHISTOCHEMISTRYIMMUNOHISTOCHEMISTRY
Pan CK – positive in tumor cells
S-100 – negative in tumor cells
Vimentin – negative in tumor cells
GFAP ( t NIMHANS ) ti i t ll GFAP ( courtesy NIMHANS ) – negative in tumor cells
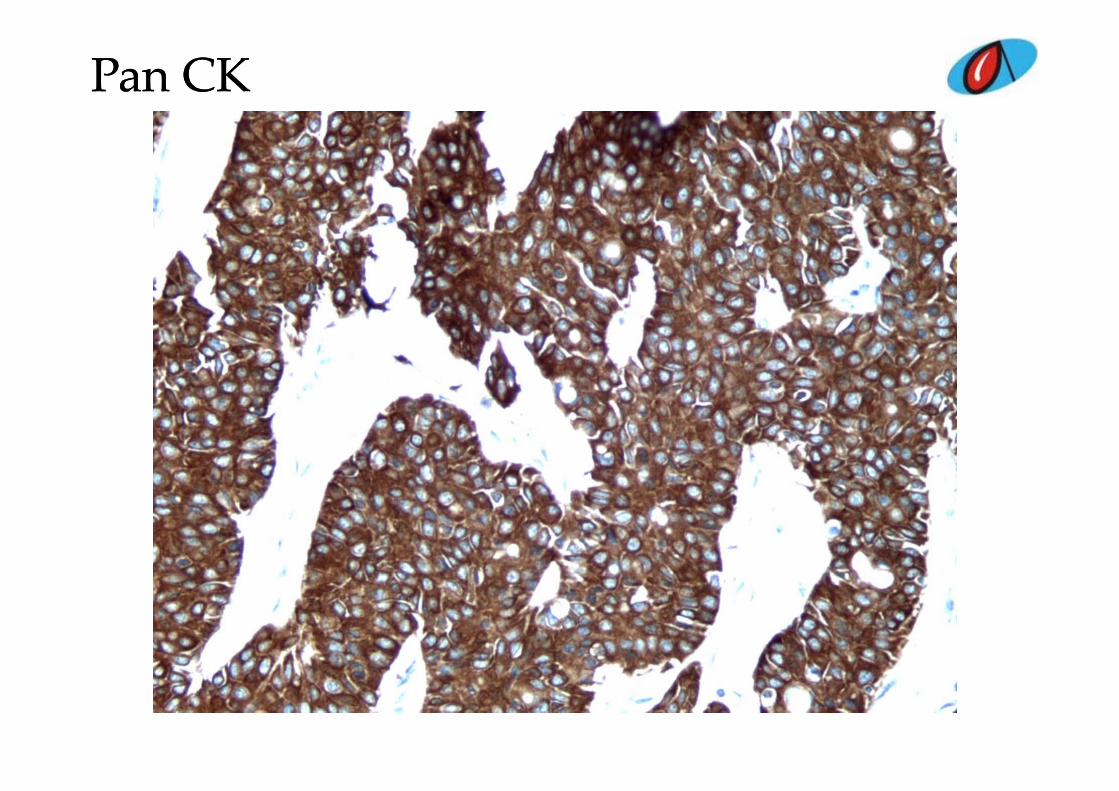
Pan CKPan CK
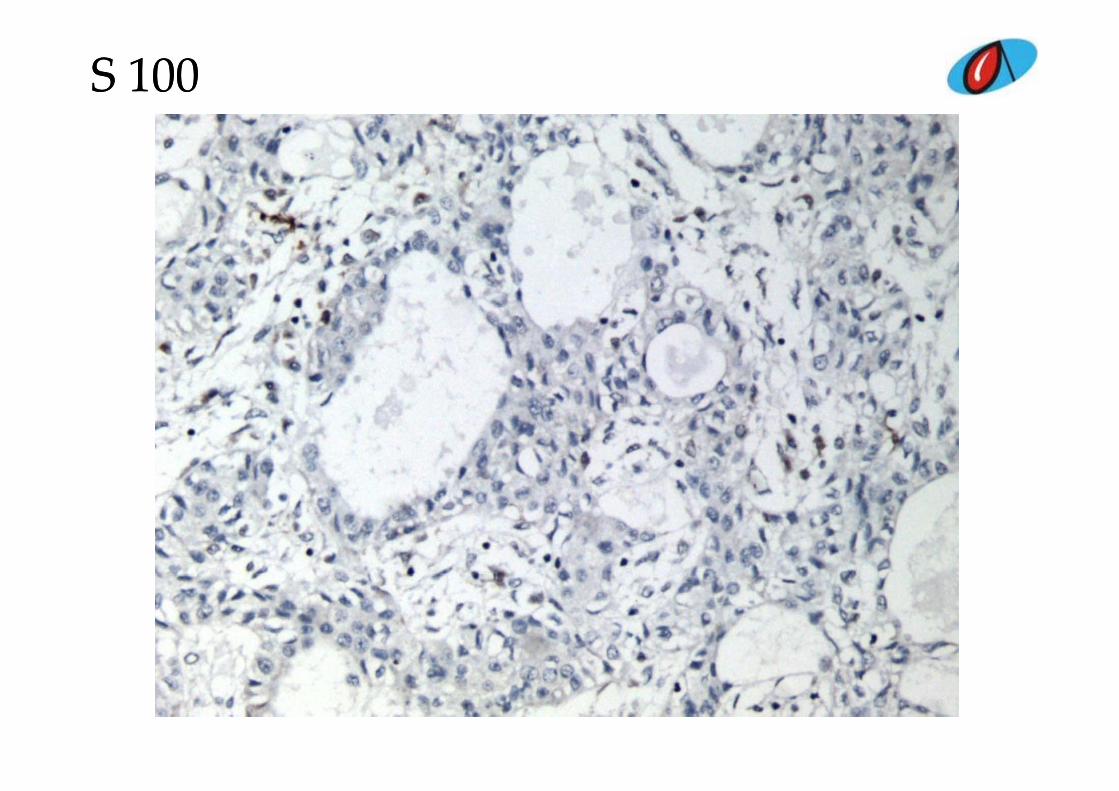
S 100S 100
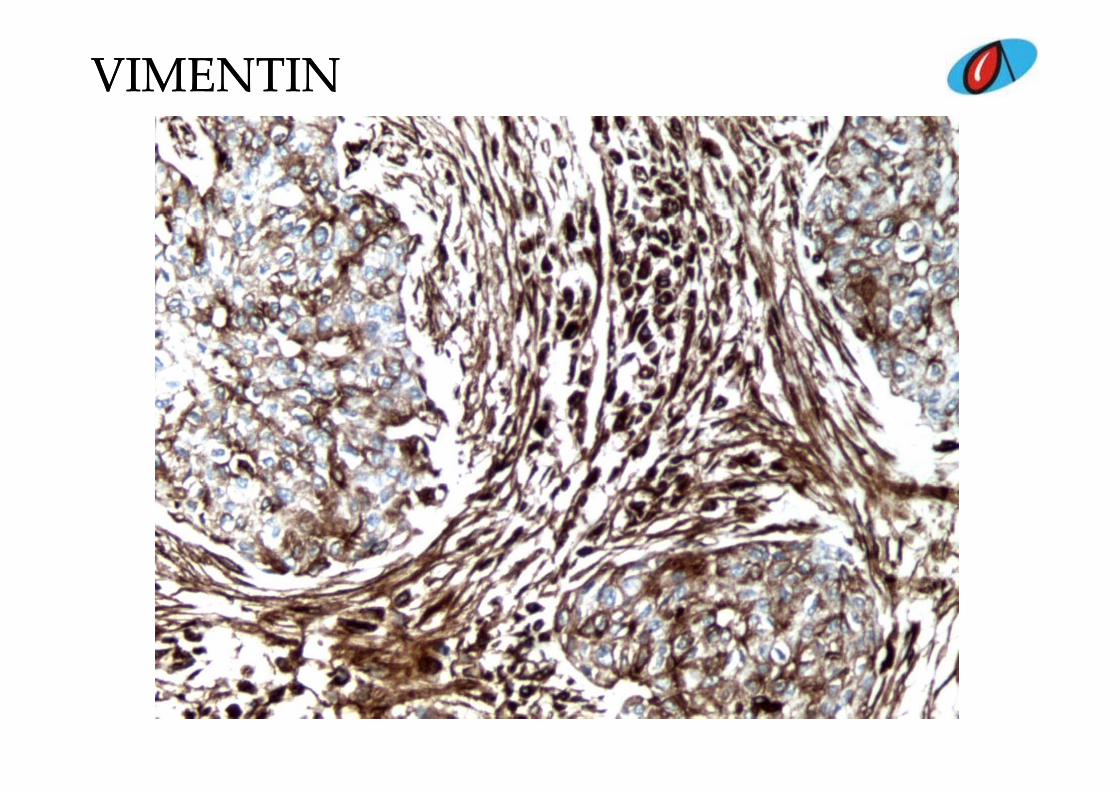
VIMENTINVIMENTIN
Final diagnosisFinal diagnosis
• Mucoepidermoid carcinoma of the lung – Low gradeg
DISCUSSIONDISCUSSION
Rare primar t mor of l ng 0 1 0 2 %• Rare primary tumor of lung – 0.1 – 0.2 %• Wide age range – mean age 40 years • Slow growing tumor• Slow growing tumor• Main bronchus- submucosal glands of the
bronchusbronchus• Classified under salivary gland neoplasms of
the lung• Lobectomy, local resection or endoscopic
removal – excellent prognosisDiff ti l di i i d d • Differential diagnosis is adenosquamous and adenocarcinoma of lung
REFERENCESREFERENCES
• Respiratory Medicine Case Reports 9 (2013) 18-20
• Arch Pathol Lab Med – Vol 131, ,September 2007
• The new World Health Organization classification of lung tumourE. Brambilla 1 , W.D. classification of lung tumour ,Travis 2 , T.V. Colby 3 , B. Corrin 4 and Y. Shimosato 5ERJ December 1 2001 vol 18 no 6 1059‐1068December 1, 2001 vol. 18 no. 6 1059 1068
CASE 5CASE 5CASE 5CASE 5
CLINICAL PRESENTATIONCLINICAL PRESENTATION
Male 25 years old Male, 25 years old
Mass per abdomen since 4 months
Bilateral undescended testes
Radiological finding – mass in right lumbar region measuring 20
x 20 cms Extension upto liver superiorly pelvis inferiorly and x 20 cms. Extension upto liver superiorly, pelvis inferiorly and
crossing midline laterally.
PER OPERATIVEPER OPERATIVE
Persistant mullerian duct syndrome with left sided large
testicular tumor and right sided small testicular tumor

HISTOPATHOLOGYHISTOPATHOLOGY
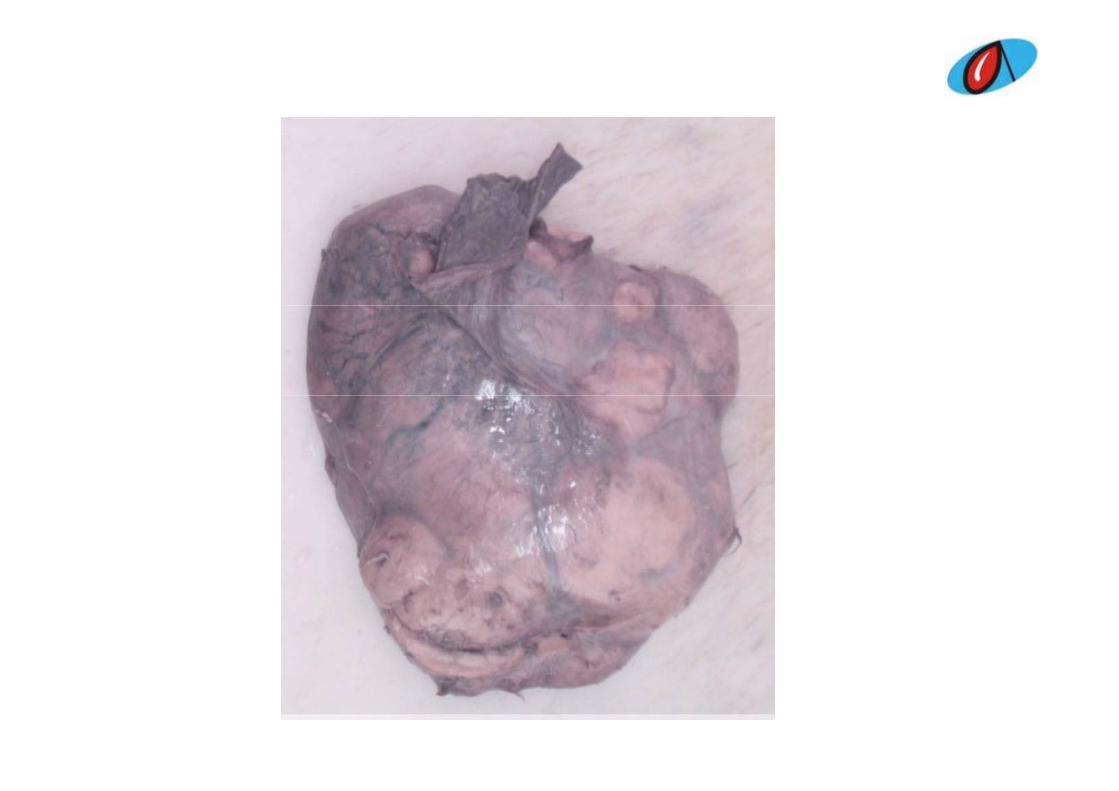
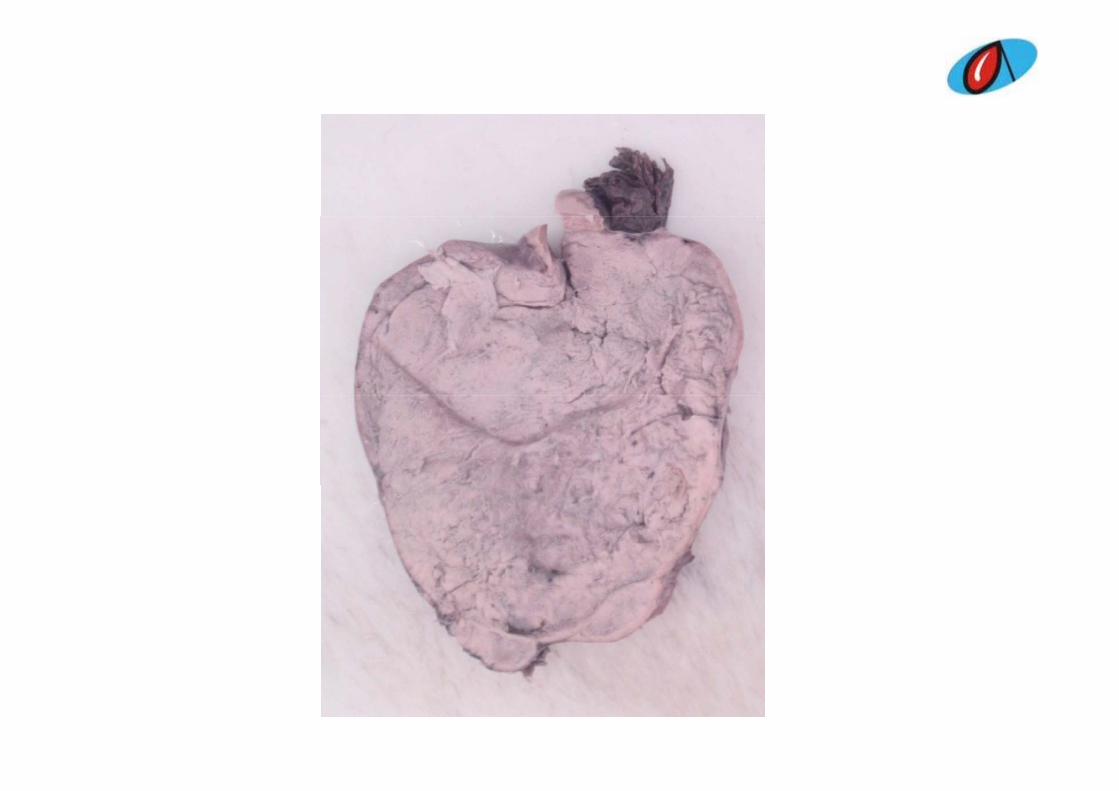
Gross – specimen altogether weighed 2140 grams and
measured 21 x 17 x 7 cms. Specimen consisted of a large, solid
pale brown tumor mass, spermatic cord, omentum and a
smaller tumor mass. Mid segment of spermatic cord showed a g p
nodular area measuring 2 cms.

Microscopy – Features of classical seminoma in both nodular masses Features of classical seminoma in both nodular masses.
Adjacent testicular parenchyma from the smaller testicuar
mass exhibit features of intratubular germ cell neoplasia.
Nodular area in spermatic cord exhibits endometrial glands ,
endometrial stroma and smooth muscle.
Omentum exhibiting features of reactive mesothelial
h perplasia hyperplasia.
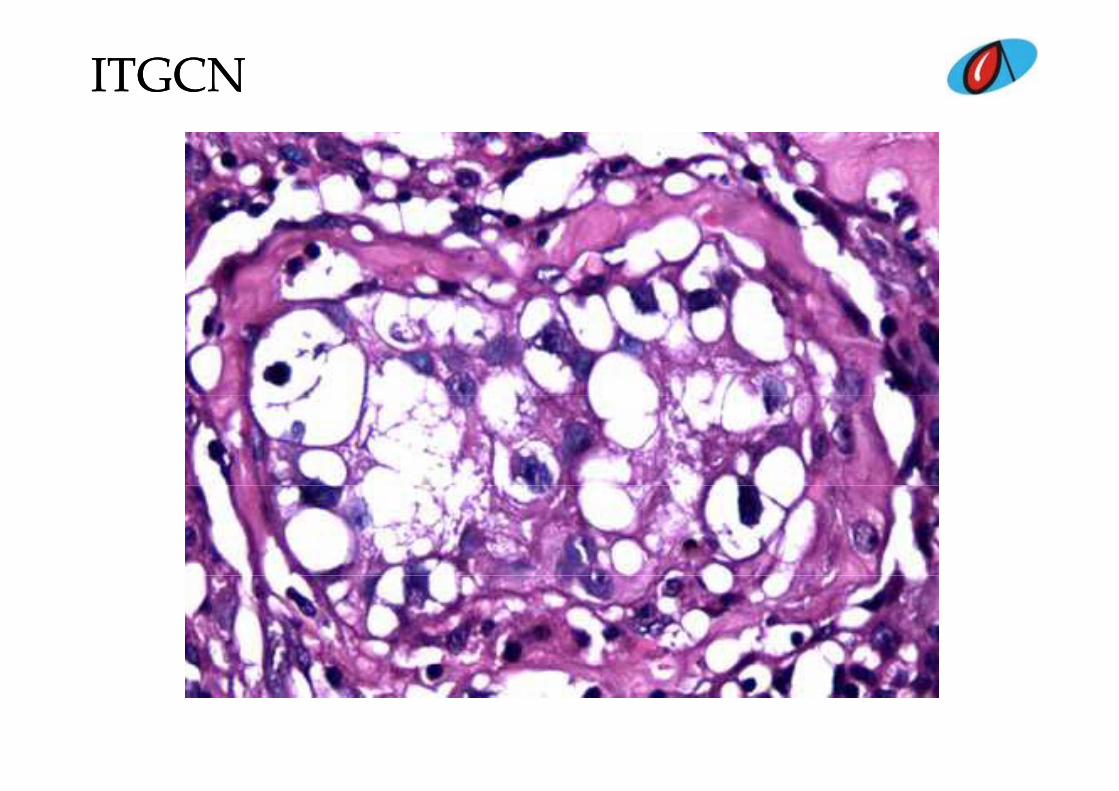
ITGCNITGCN
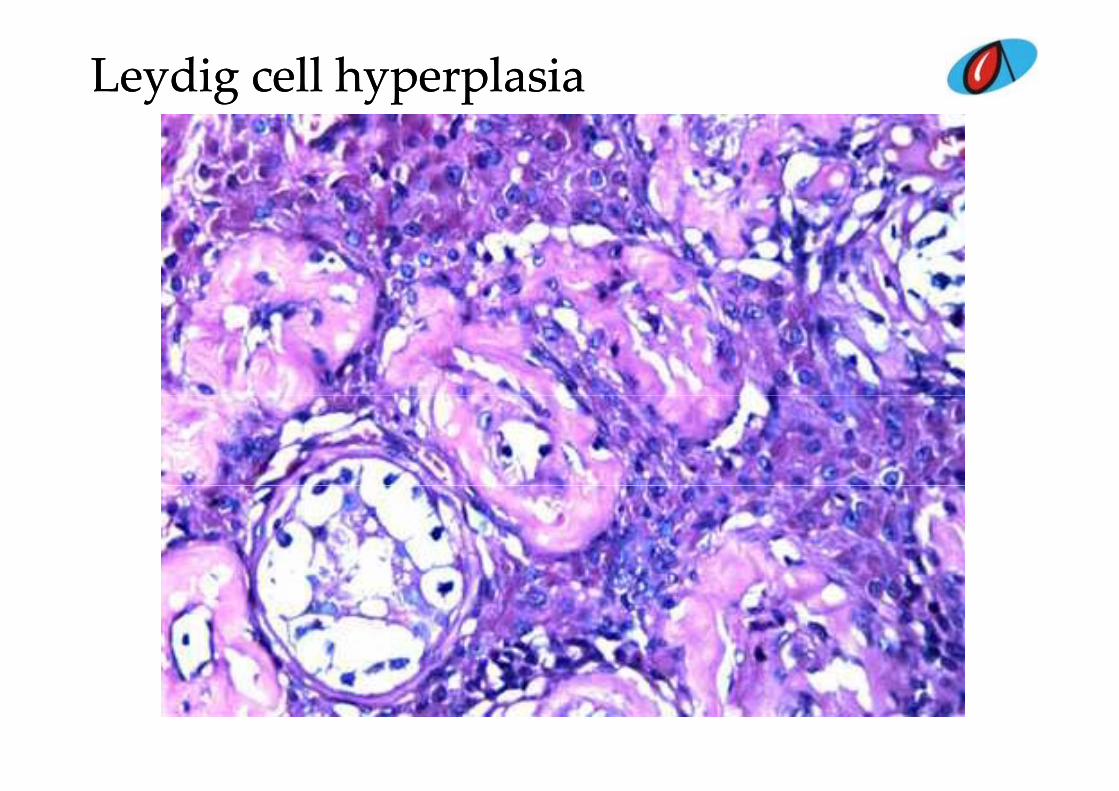
Leydig cell hyperplasiaLeydig cell hyperplasia
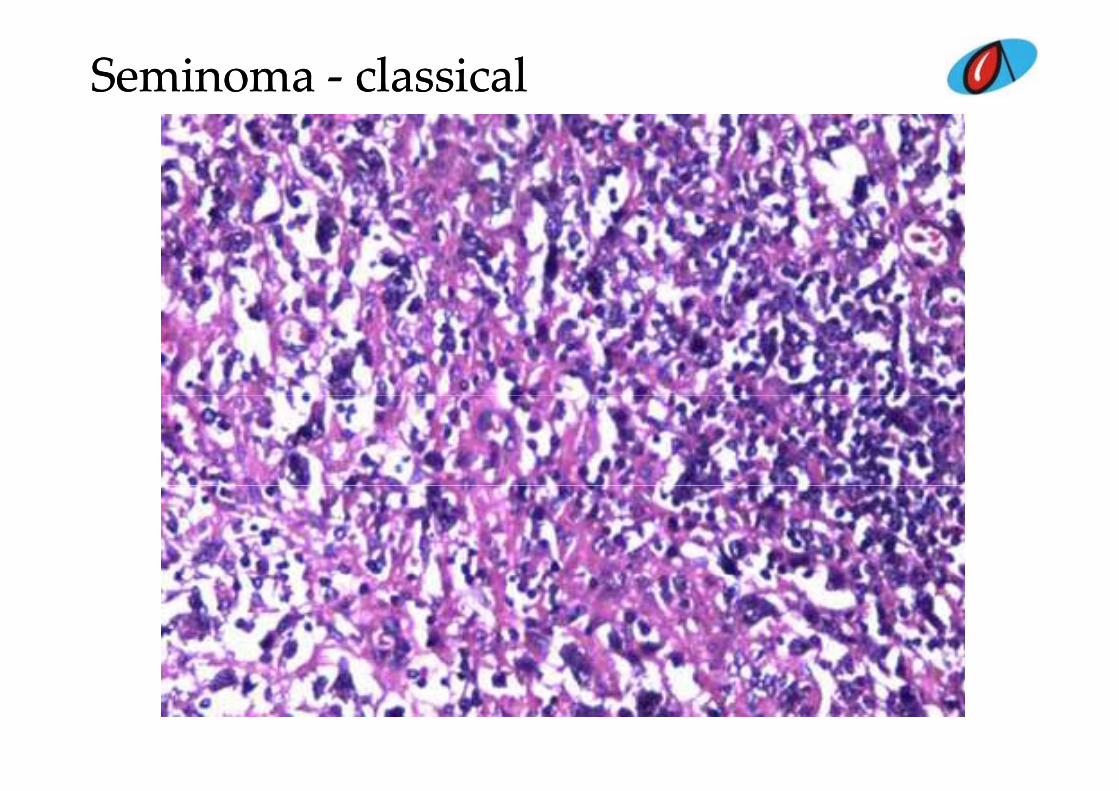
SeminomaSeminoma ‐‐ classicalclassical
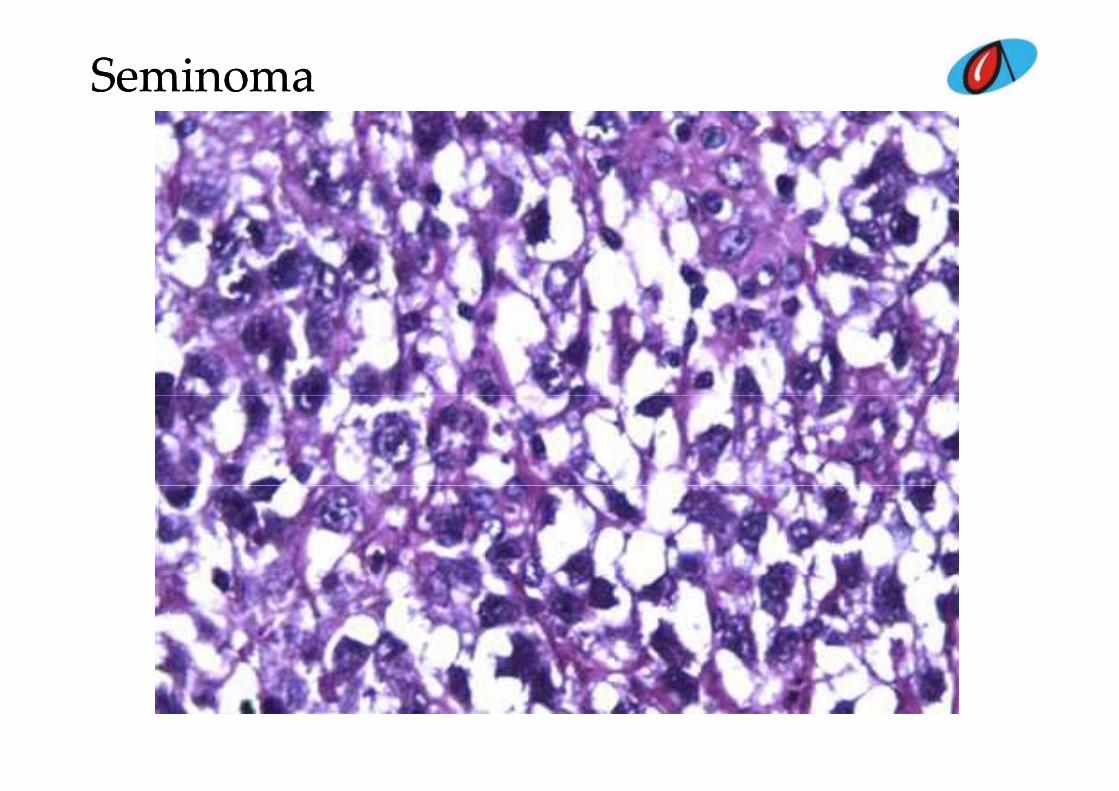
SeminomaSeminoma
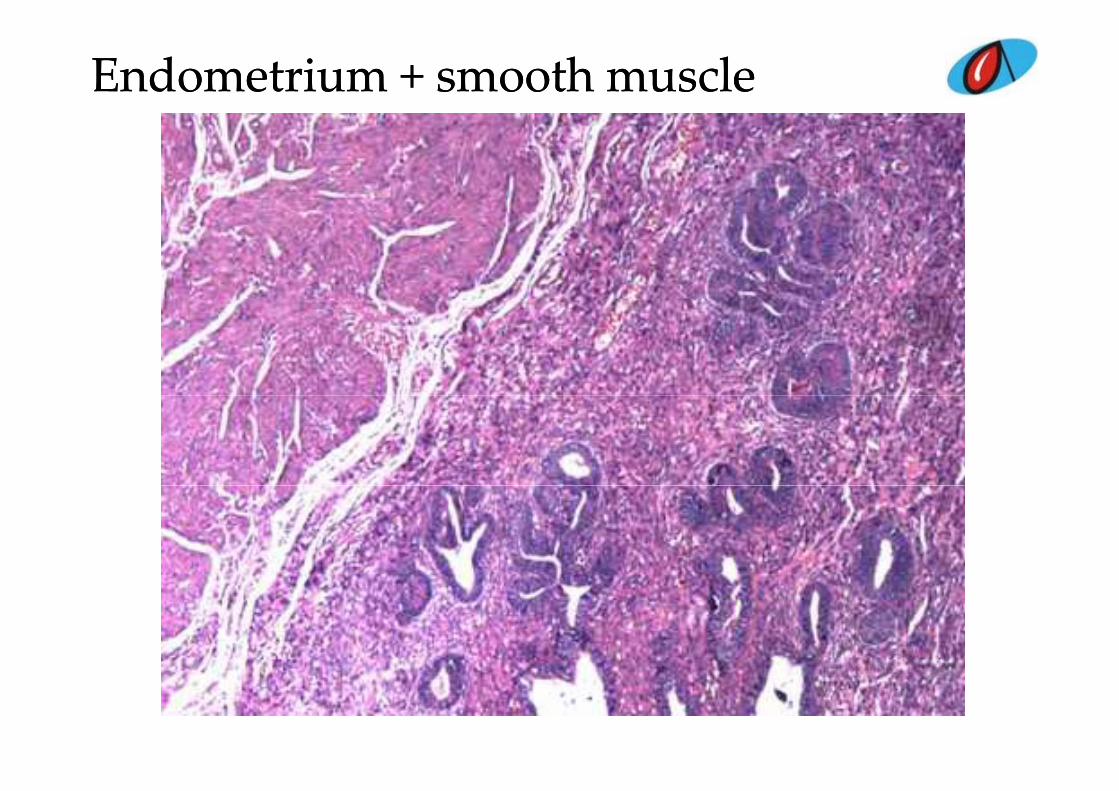
Endometrium + smooth muscleEndometrium + smooth muscle
DIFFERENTIALSDIFFERENTIALS
L di ll h l i ith t hi t b l d ll • Leydig cell hyperplasia with atrophic tubules and germ cell tumor- seminoma
• Persistent mullerian duct syndrome with seminoma and leydigy y gcell hyperplasia
• Persistent mullerian duct syndrome with cryptorchidism and ITGCN and seminomaITGCN and seminoma
• Gonadal dysgenesis• True hermaphroditep• Anaplastic seminoma• Spermatocytic seminoma
Impression –
Classical seminoma – bilateral testes
Intratubular germ cell neoplasia – right testis
P i t t M ll i d t d Persistent Mullerian duct syndrome
DISCUSSIONDISCUSSION
R f f l d h h diti i ( 46 XY)• Rare form of male pseudohermaphroditisim ( 46 XY)• Persistence of mullerian duct structures due to lack of anti-
mullerian hormone• X linked or autosomal recessive• Phenotypically male• Unilateral or bilateral cryptorchidism• 15% risk of germ cell neoplasms and ITGCN
Case 6Case 6
CLINICAL DETAILSCLINICAL DETAILS
• Male patient aged 37 years
• Fracture of L5 vertebra
• Blocks for opinion

MicroscopyMicroscopy
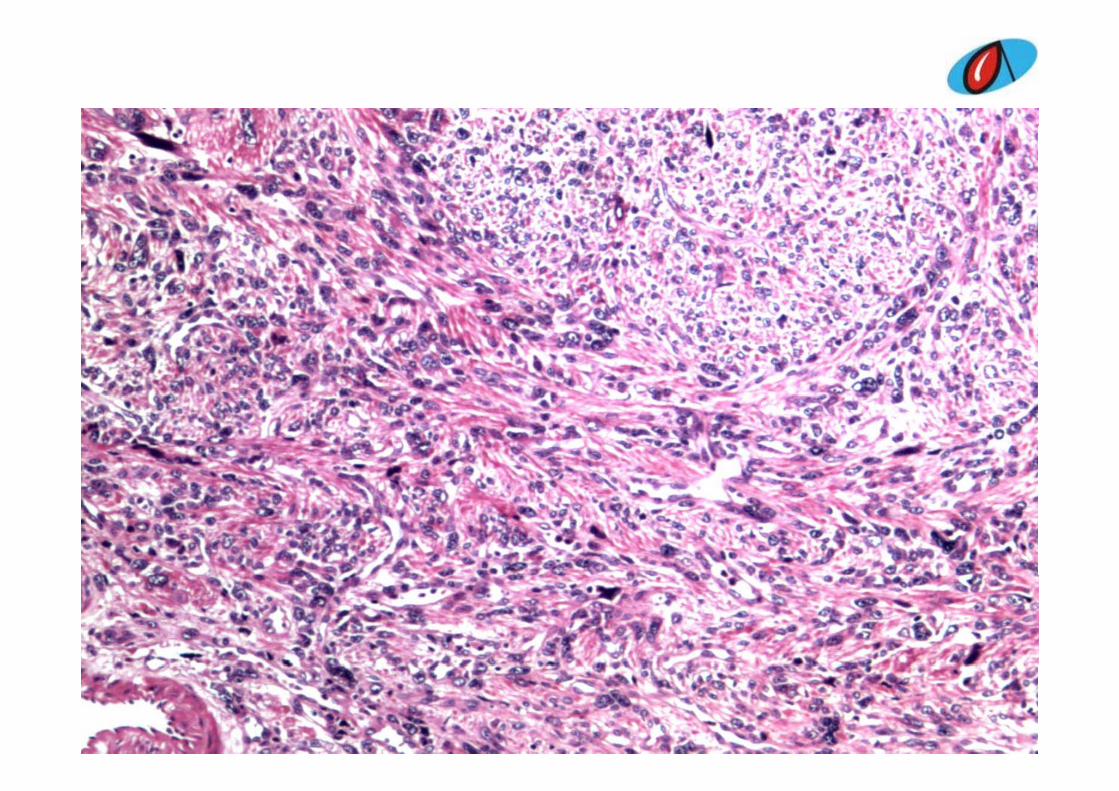
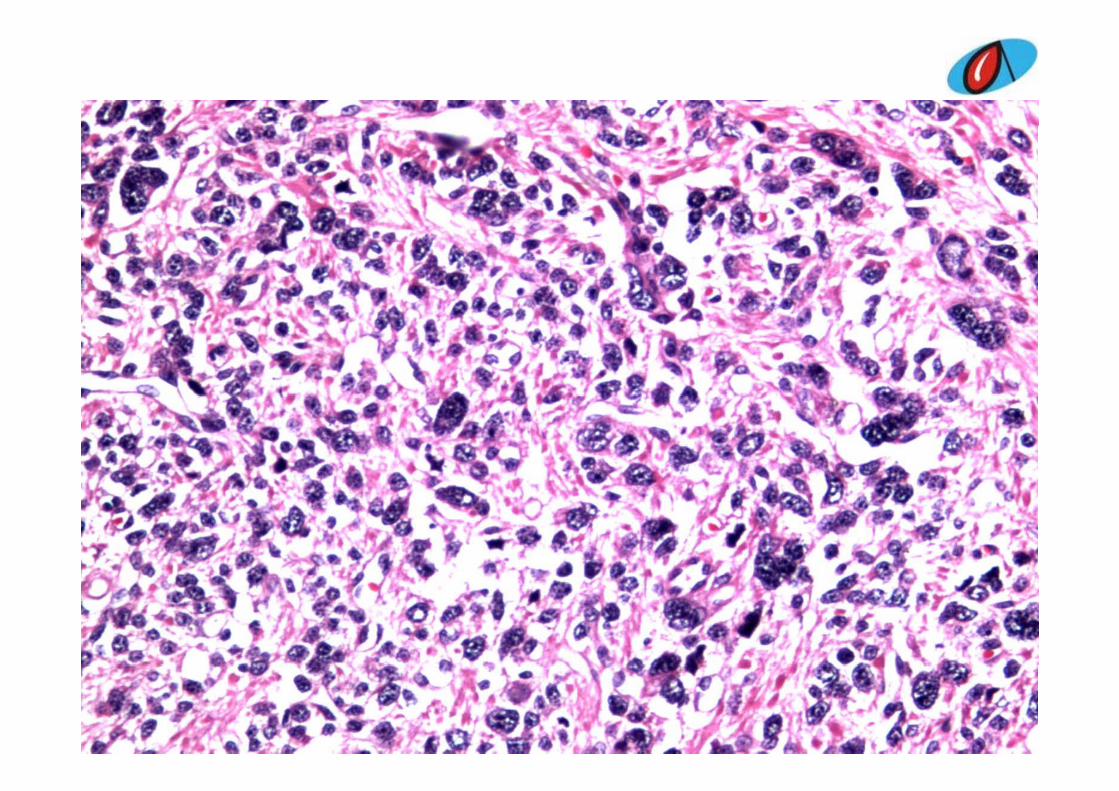
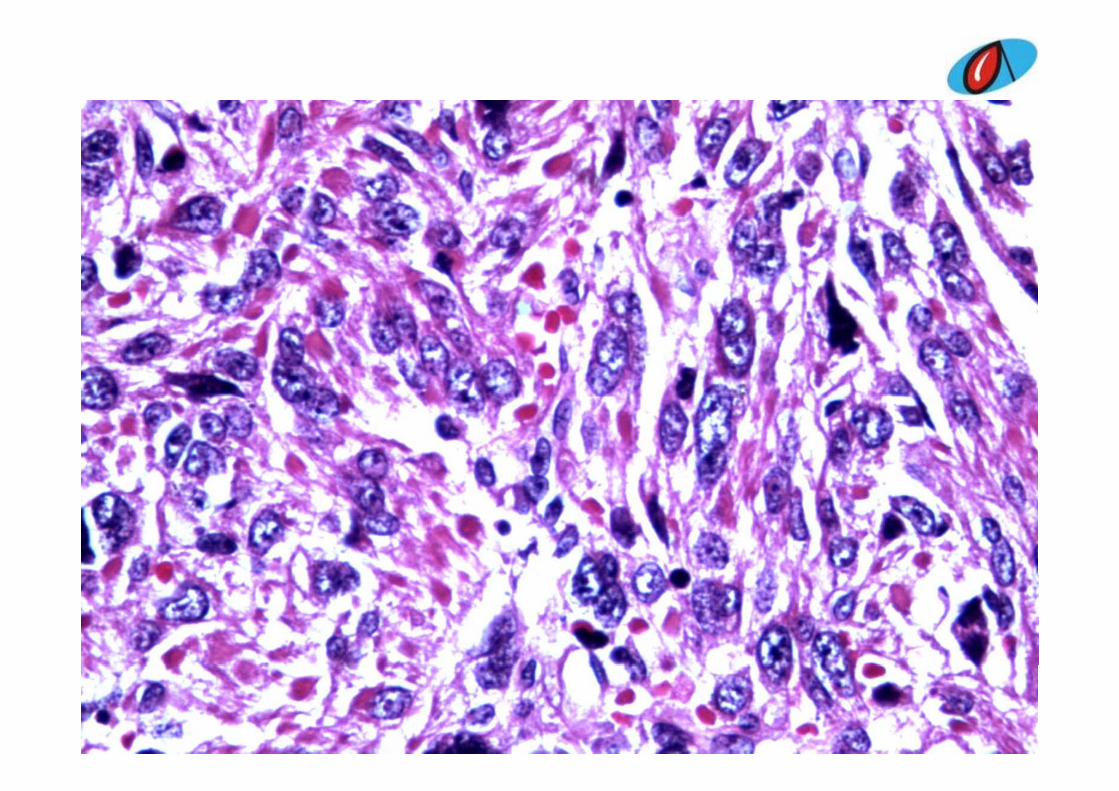
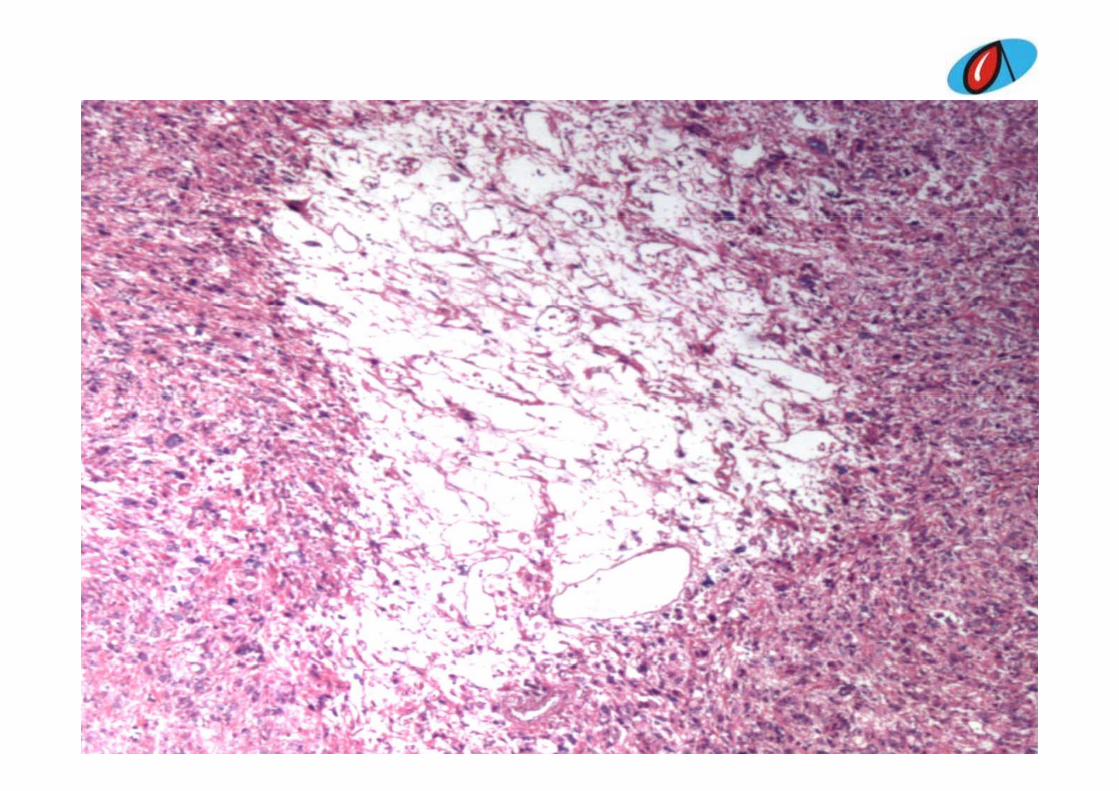
• Tumor cells are polygonal to ovalTumor cells are polygonal to oval
• Arranged in distinctive organoid patternArranged in distinctive organoid pattern
• Separated by fibrocollagenous stroma and Sepa ated by b oco age ous st o a a dsurrounded by blood vessels
Initial diagnosisInitial diagnosis
• Neuroendocrine tumor• Neuroendocrine tumor
Differential diagnosisDifferential diagnosisHe angioendothelio a• Hemangioendothelioma
• PNET of vertebra • Mesenchymal chondrosarcomaMesenchymal chondrosarcoma• Angiomatous meningioma• Capillary hemangioblastomap y g• Paraganglioma• Epithelioid hemangioendothelioma• Metastatic RCC• Multiple myeloma
Metastatic carcino a• Metastatic carcinoma• Telangiecatic Osteosarcoma
IHCIHC
COURTESY NIMHANSCOURTESY - NIMHANS
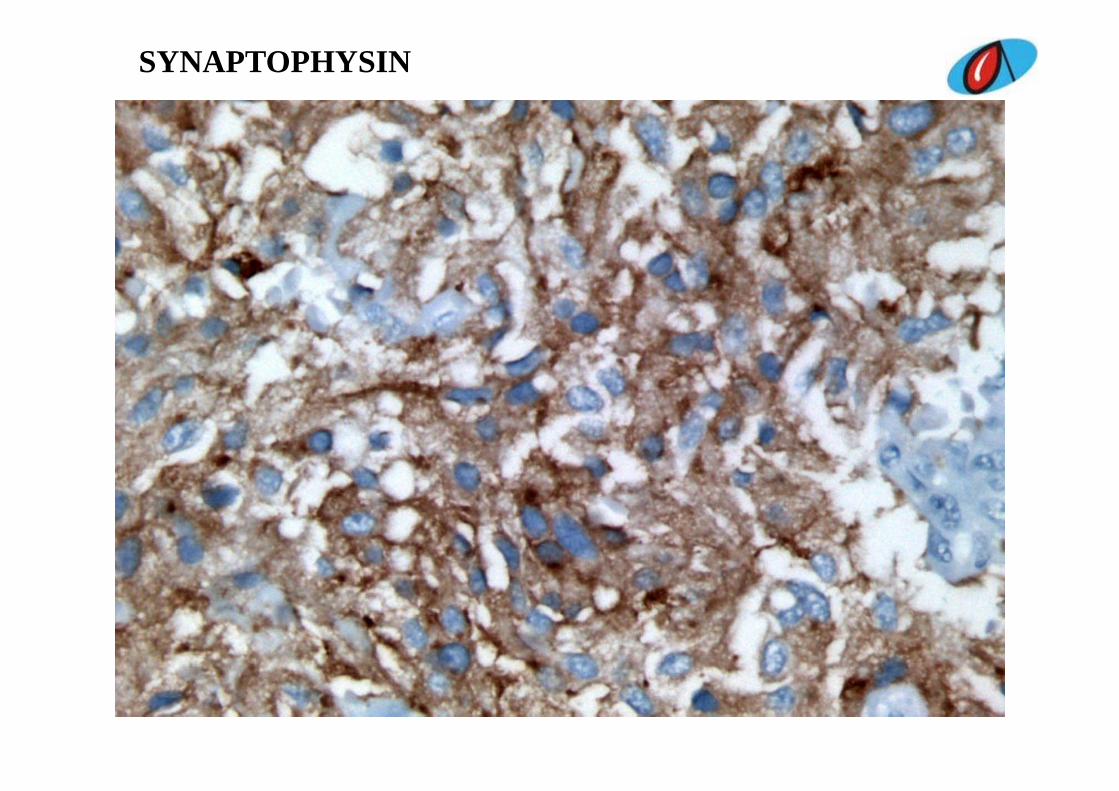
SYNAPTOPHYSIN
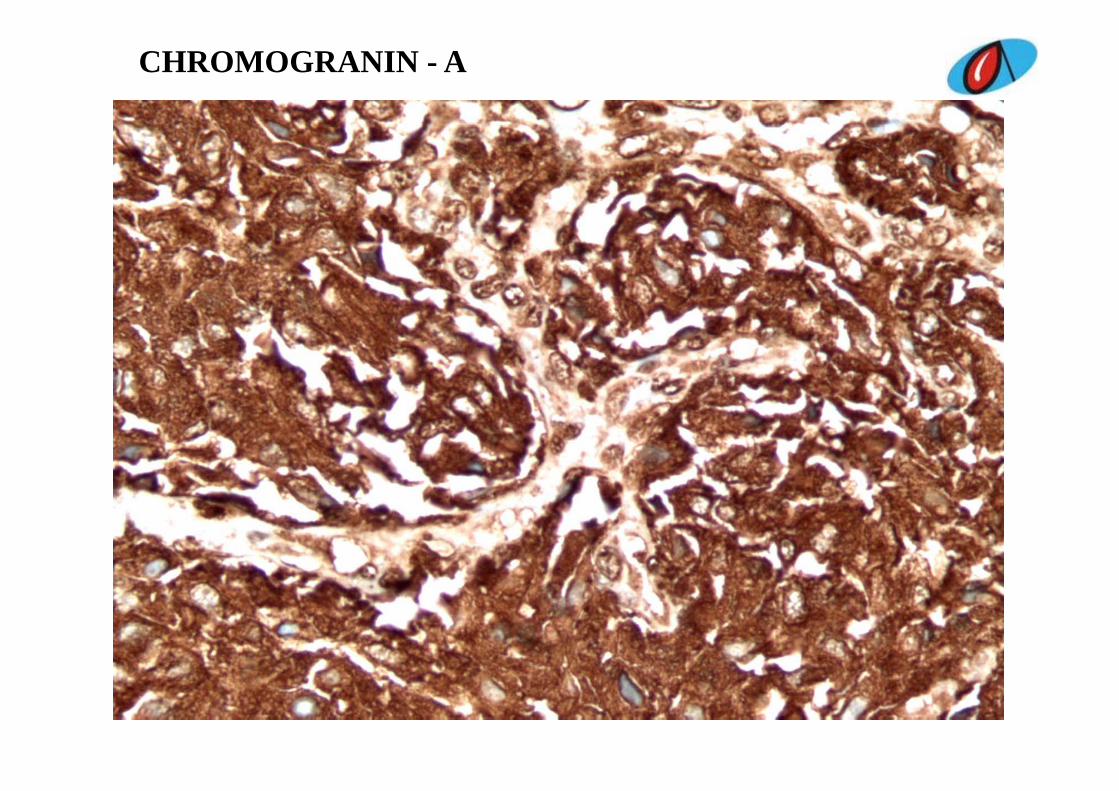
CHROMOGRANIN - A
PARAGANGLIOMAPARAGANGLIOMA
• Primary / metastatic• Primary / metastatic
• No clinical evidence of primaryNo clinical evidence of primary
• No history of sweating palpitations hypertensionNo history of sweating, palpitations, hypertension
• Primary paragangliomas of craniospinal axis arise in cauda equina
• Encapsulated intradural masses attached to filumterminale or less commonly the spinal roots
• Functionally silent
• Erosion into the neighbouring bone
• Osseous metastases
• Good number of cases of primary paragangliomas of th i l l h b bli h dthe spinal canal have been published
Immunohistochemistry
• Chief cells - chromogranin, synaptophysin, neuron ifi l i fil d lspecific enolase, serotonin, neurofilament and neural
cell adhesion molecule
• S-100 protein negative
REFERENCESREFERENCES
1. Rosai J. Surgical pathology. 9th ed. 19(2): 2586 to 2587
2. Lmejjati M, Parker F, Lacroix C et al. “Paraganglioma of sacral spine”. Neurosciences 2011;16(3):270-272.; ( )
3. Shin JY, lee SM, Hwang MY et al. “ MR findings of spinal paraganglioma:report of 3 cases” J Korean Med Sci 2001;16:522-6paraganglioma:report of 3 cases . J Korean Med Sci. 2001;16:522 6.
4. Moran Ca, Rush W, Mena H. “primary spinal paragangliomas:aclinicopathological and immunohistochemical study of 30 cases”clinicopathological and immunohistochemical study of 30 cases . Histopathology. 1997;31(2):167-173
CASE 7CASE 7

CLINICAL DETAILS
• Female patient aged 56 yearsp g y
• ? Ovarian mass
• Blocks for opinionp

MICROSCOPYMICROSCOPY
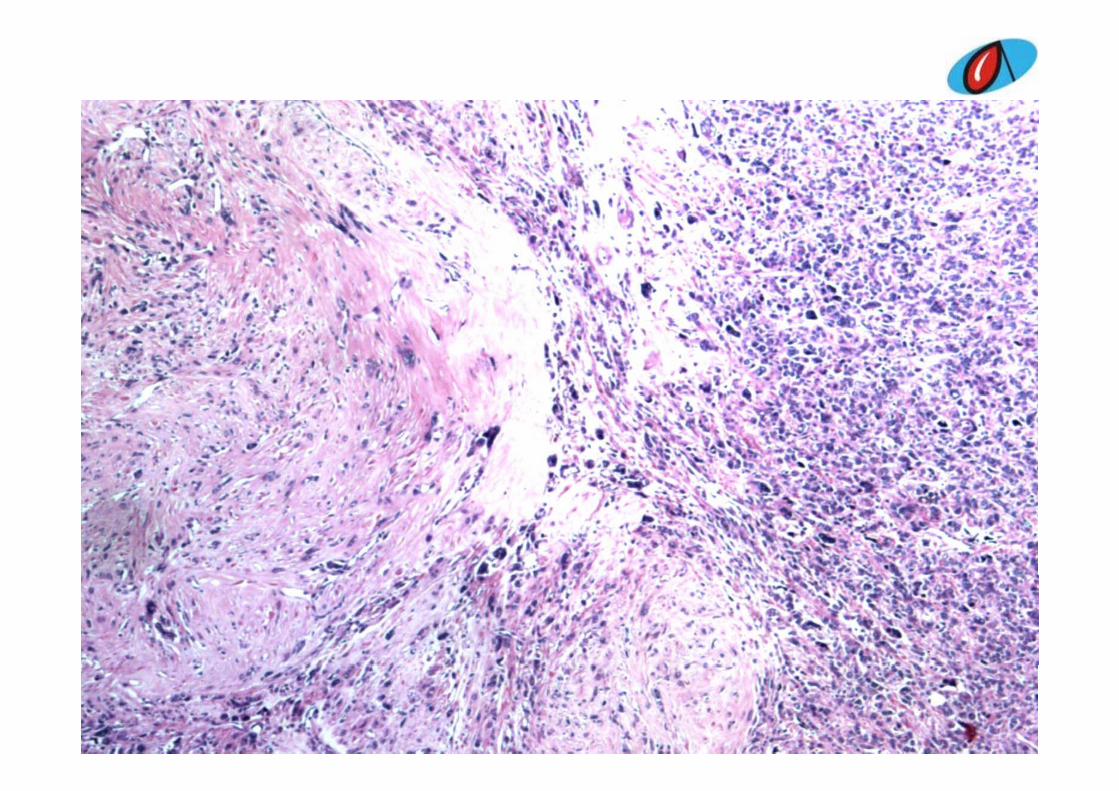
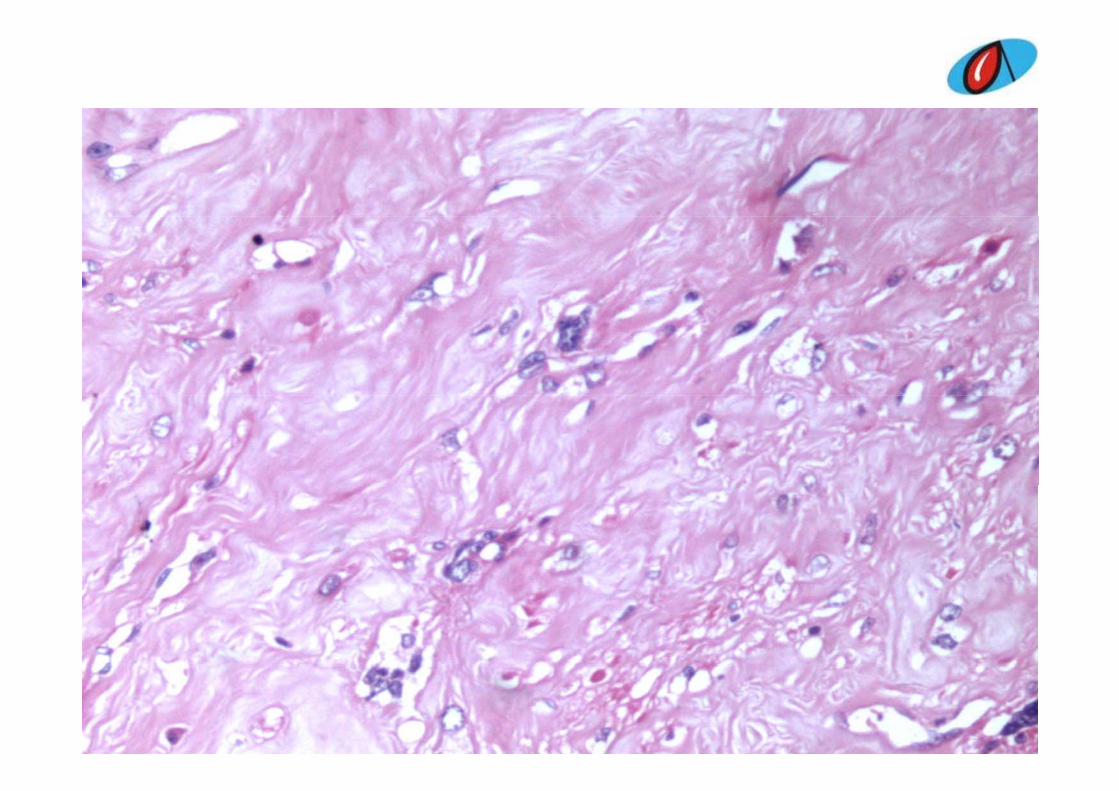
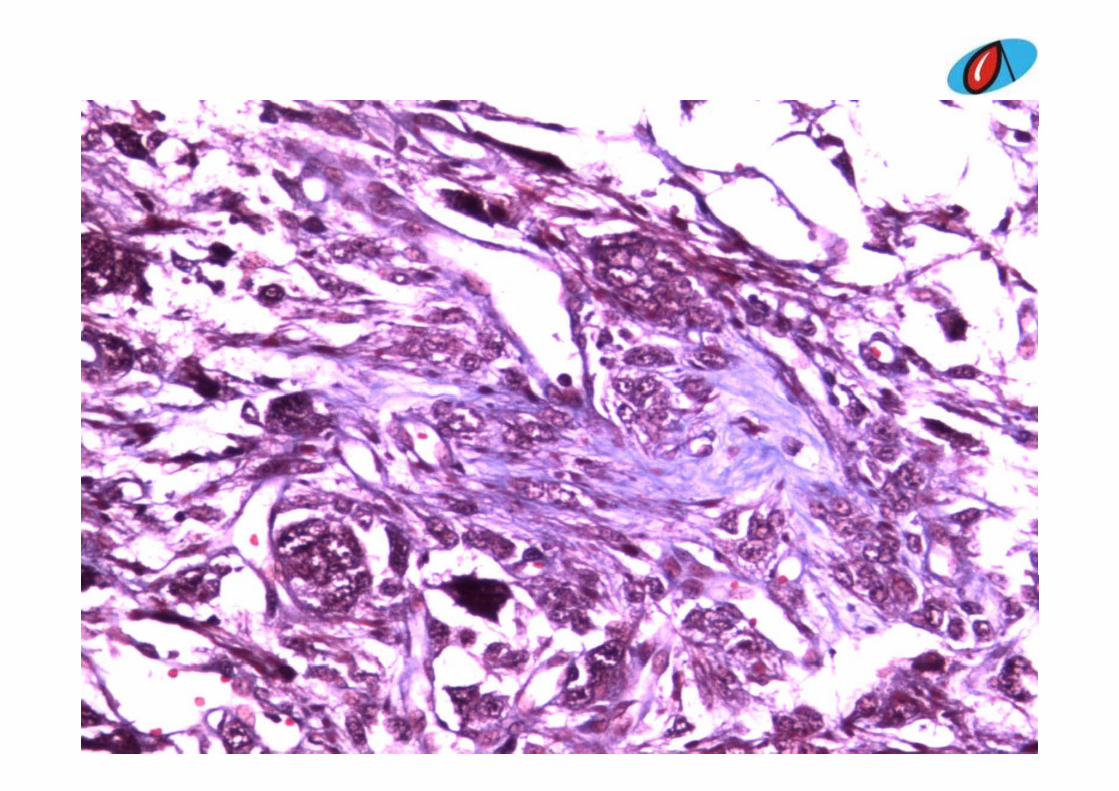
• Tumor with spindle cellsTumor with spindle cells• Hyalinized and oedematous stroma• Bizarre hyperchromatic nucleiBizarre hyperchromatic nuclei• Clumped chromatin• Prominent nucleoliProminent nucleoli• Multinucleated forms• No necrosisNo necrosis• Occasional mitosis (0-1/10HPF)• Ovarian stroma not identifiedOvarian stroma not identified
Differential diagnosisDifferential diagnosis
E b l i• Embryonal carcinoma• Sarcomatous variant of yolk sac tumory• Sarcomatoid transformation of stromal tumor• Fibrosarcoma• Fibrosarcoma• Poorly differentiated ovarian carcinoma• Angiosarcoma• Nodular fascitisNodular fascitis• Leiomyosarcoma
• Atypical bizarre cellular leiomyoma• Symplastic leiomyoma• Metastatic krukenberg tumor• Metastatic krukenberg tumor• Sex cord stromal tumor• Sclerosing stromal tumor of ovary• Endometrial stromal sarcoma• Endometrial stromal sarcoma• Malignant mixed mullerian tumor• Retroperitoneal Kaposi’s sarcoma
Signed out reportSigned out report
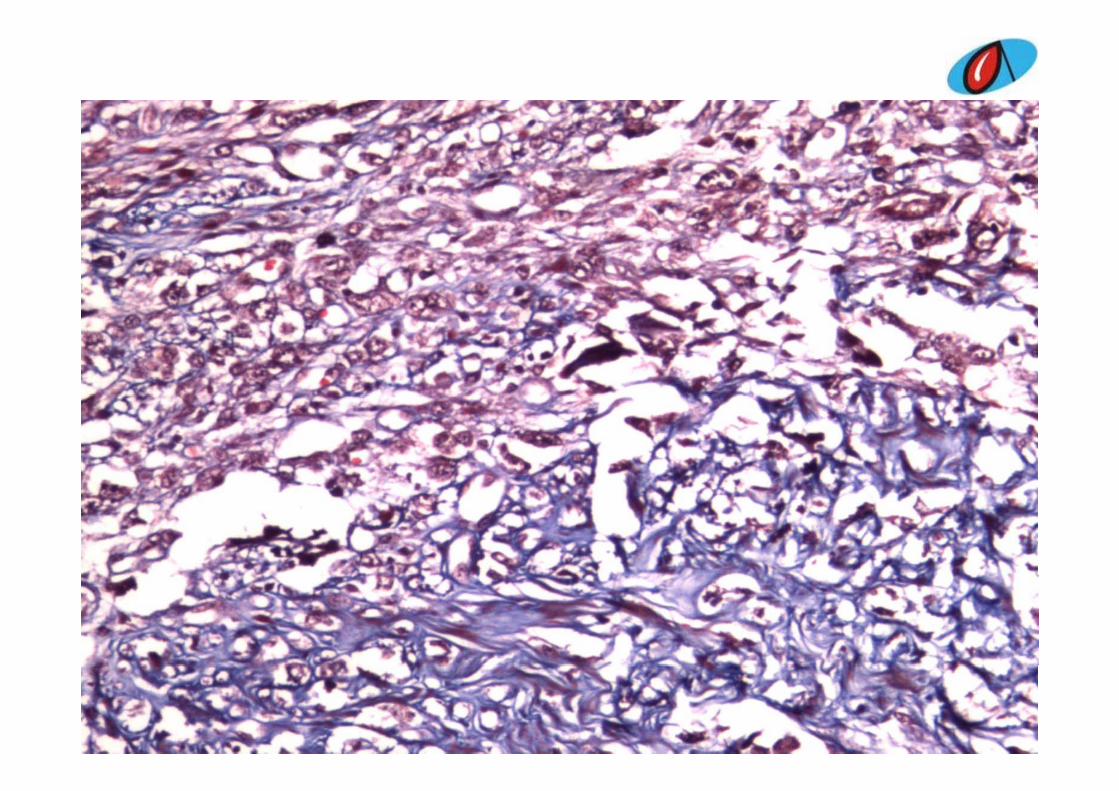
• Smooth muscle origin• Smooth muscle origin• Benign nature
Symplastic leiomyomaSymplastic leiomyoma
GROSS
1. Specimen of uterus cervix 8x3.5x3cmp
E/S - Uterus – cauterized cavity yC/S – Endometrium – atrophicCervix – nabothian cysty
2. Irregular yellow tissue 4x3x3cm
C/S – Whorled appearance
Ovary not identified


Final diagnosisFinal diagnosis
Symplastic leiomyoma
• Atypical, bizarre, symplastic or pleomorphicAtypical, bizarre, symplastic or pleomorphic leiomyomas
• Spontaneously or in patients taking progestin compoundscompounds
• Electron microscopy demonstrates actin filaments with associated dense bodies as well as incomplete basal lamina (features characteristic of smooth muscle cells)
• Low risk of recurrence

REFERENCESREFERENCES
1. Rosai J. Surgical pathology. 9th ed. 19(2):1569-1636
2 Fechner RE Atypical leiomyomas and synthetic progestin therapy Am J2. Fechner RE. Atypical leiomyomas and synthetic progestin therapy. Am J
Clin Pathol. 1968,49:697-703
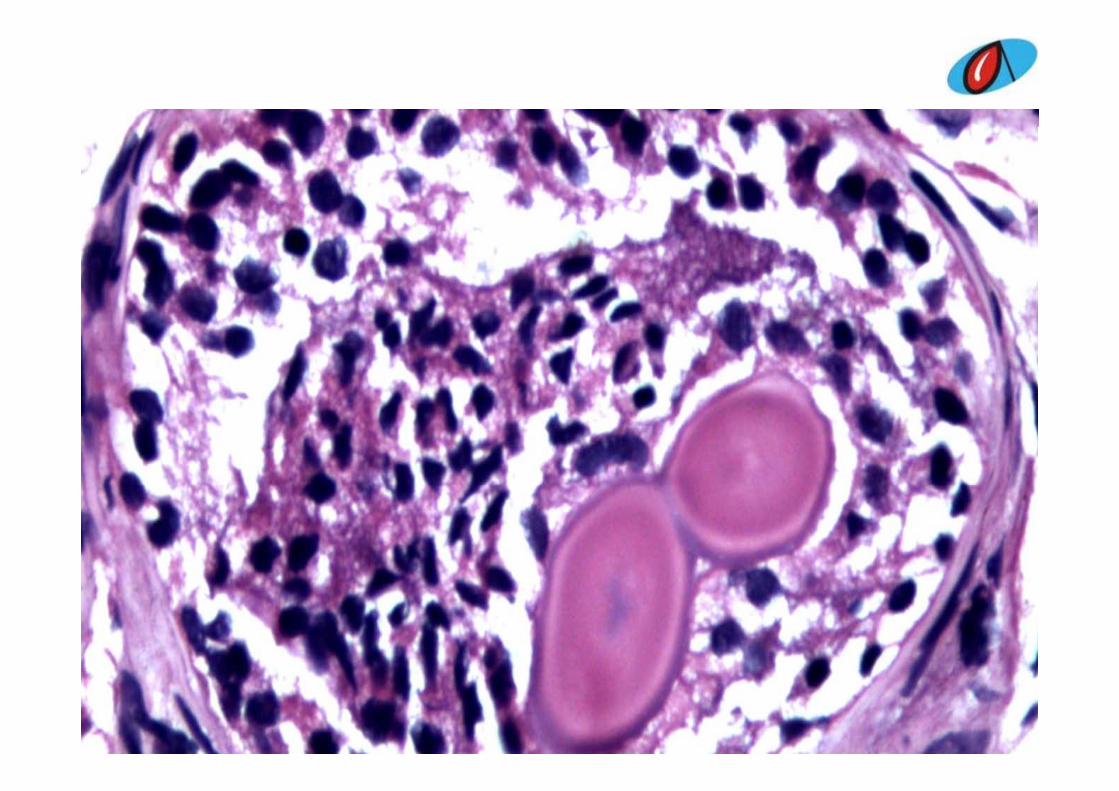
Case 8Case 856/F, case of intermittent
painless hematuria.TURBT from l l ll f i bl ddlateral wall of urinary bladder
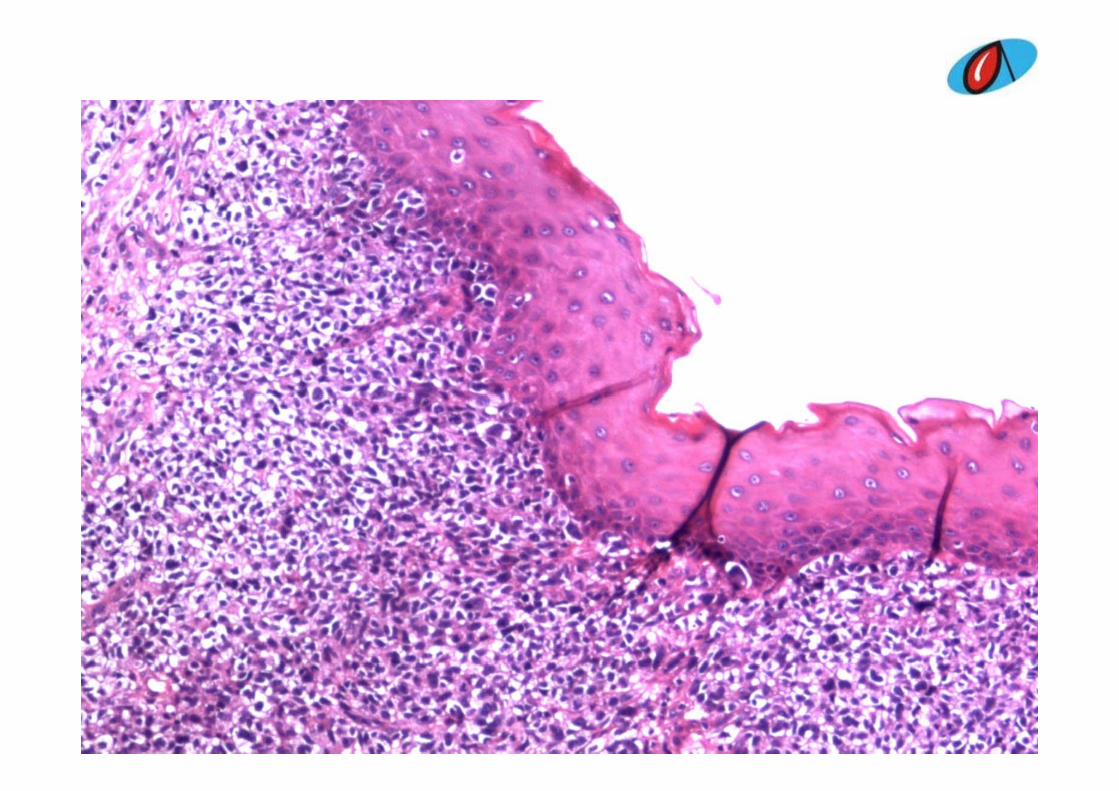


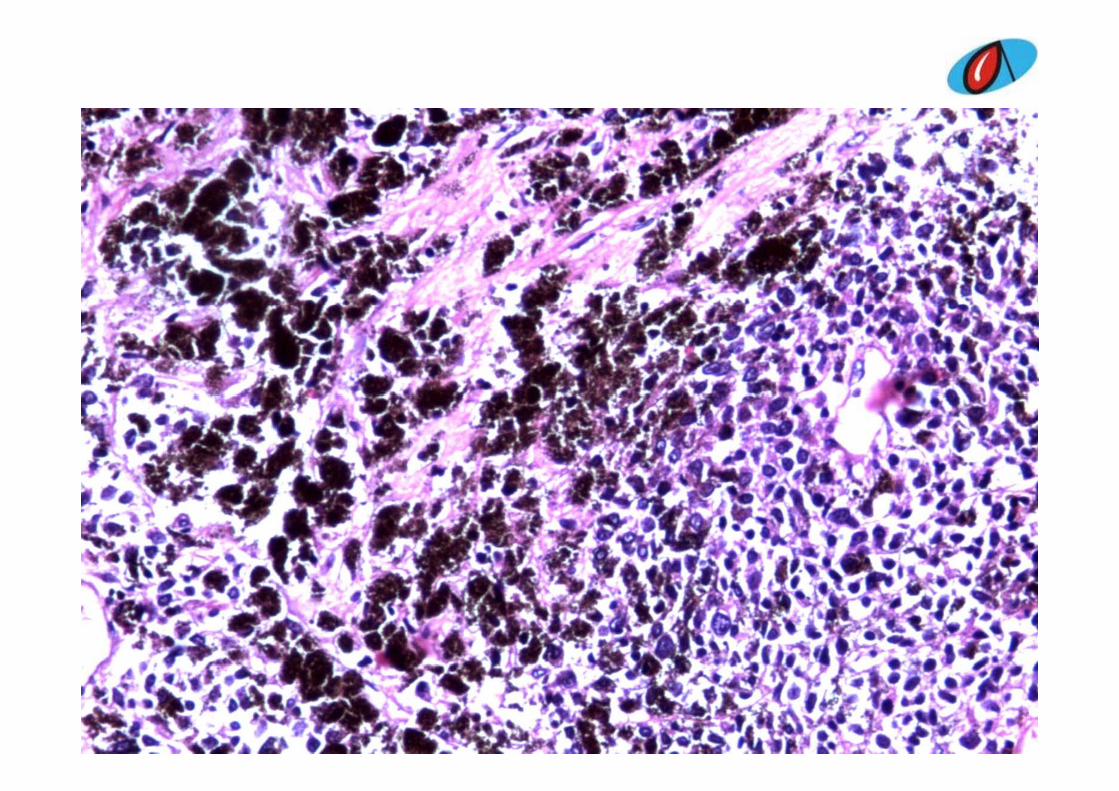
Differential diagnosisDifferential diagnosis
Li id i t f i i th li l i• Lipoid variant of invasive urothelial carcinoma• Transitional cell carcinoma• Primary small cell carcinoma• Clear cell carcinoma• Malignant melanoma• High grade urothelial carcinoma• Neuroendocrine tumor of bladder• Metastatic RCC• Pigmented paraganglioma
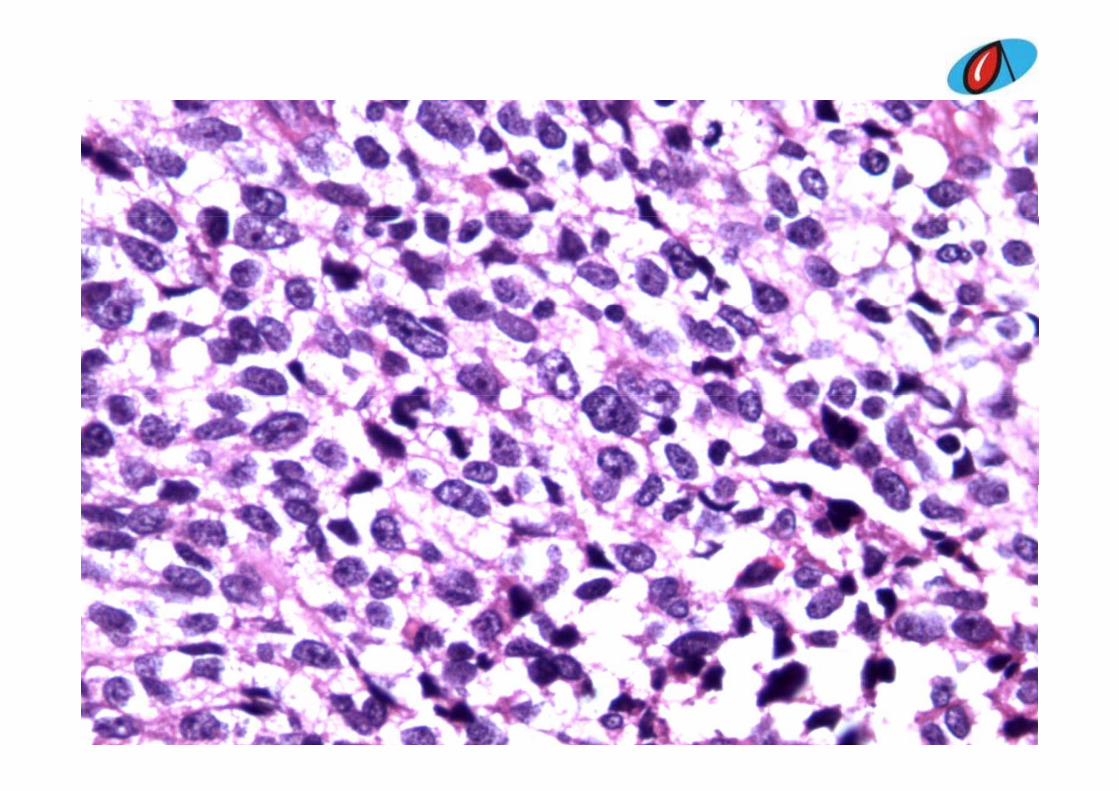
Thought processThought process
• ??? Malignant melanoma

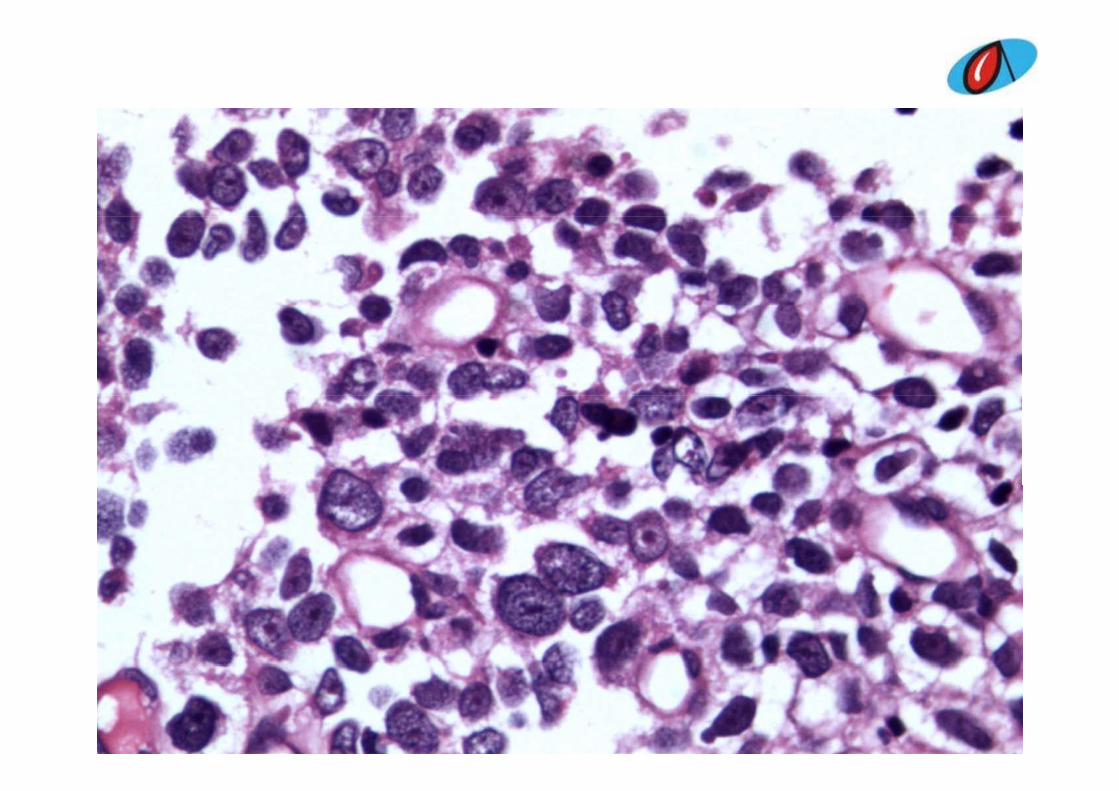
Perl’s stain for ironPerl s stain for iron
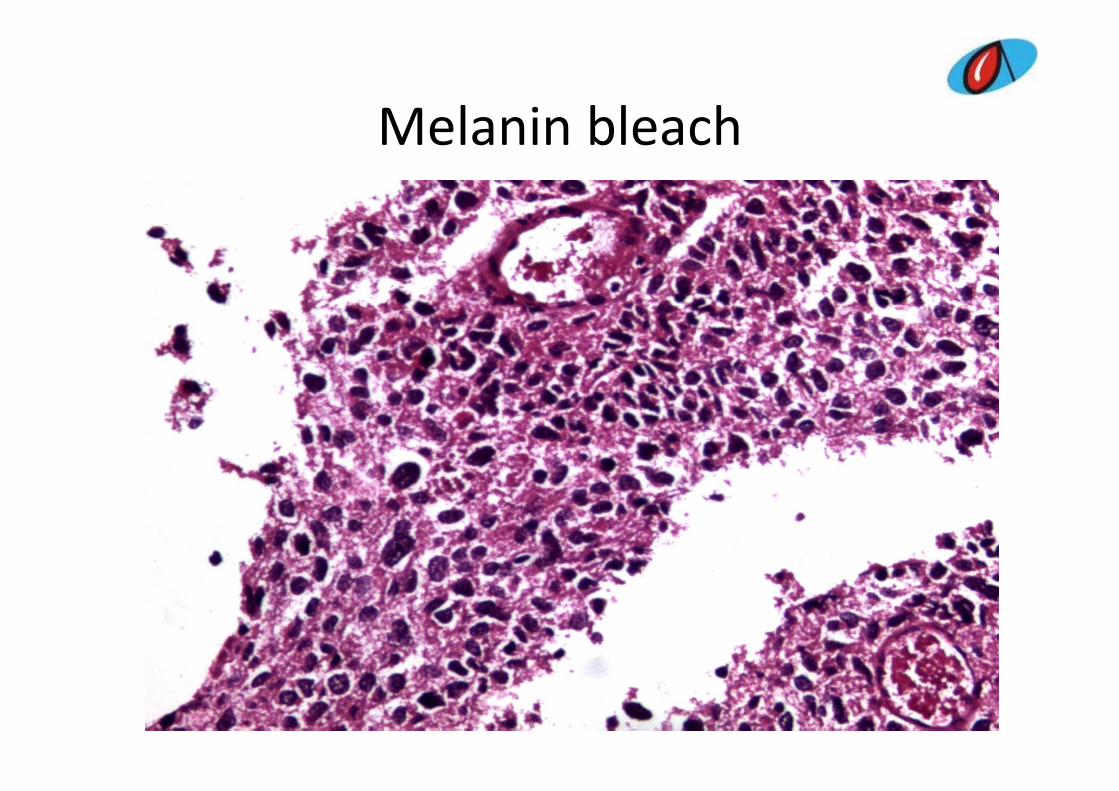
Melanin bleachMelanin bleach
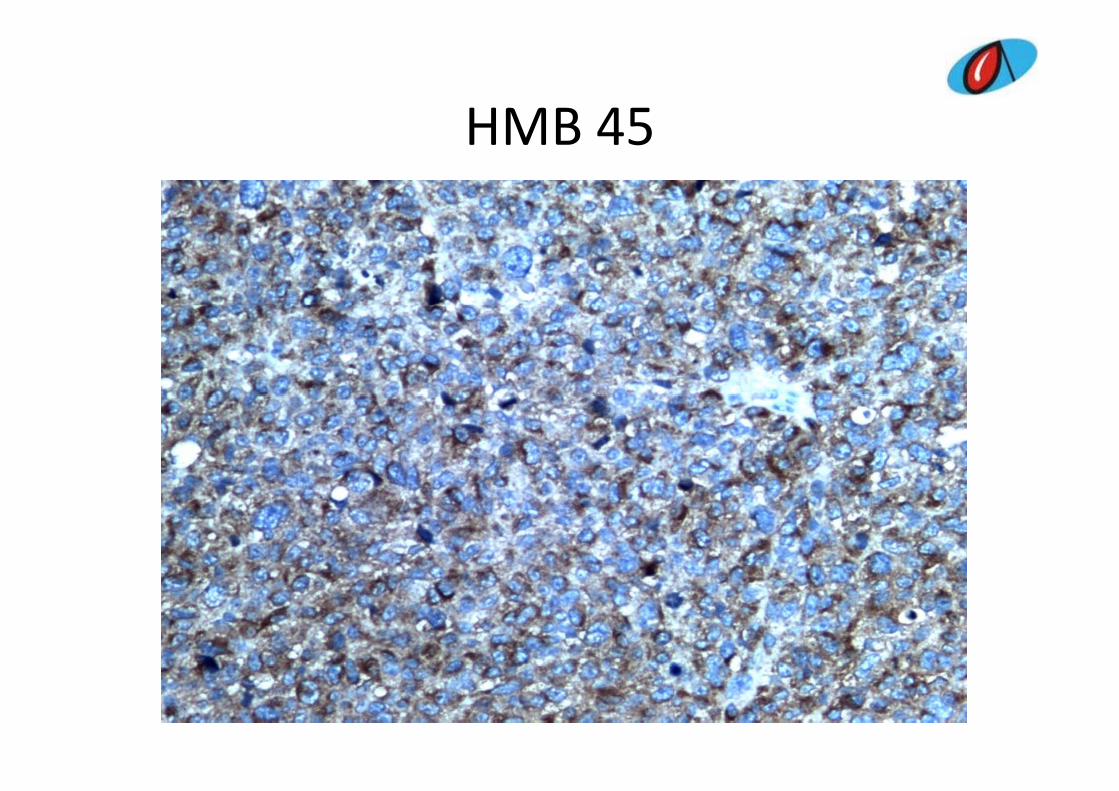
HMB 45HMB 45
Final diagnosisFinal diagnosis
• Malignant melanoma– ? Primaryy– ? Metastatic
DiscussionDiscussion
• Primary melanoma of bladder is very rare• 19 odd cases reported in literature19 odd cases reported in literature• Mostly metastatic from the skin or urethra
Criteria for primary melanoma of bladder
i h i i• Ainsworth criteria• Careful physical examination including the skin p y gwith Wood’s light together with detailed history to exclude cutaneous melanomay
• Exclusion of visceral melanoma• Pattern of recurrence consistent with primary• Pattern of recurrence consistent with primary melanoma of bladder
• Histologically proved primary atypical melanocytes
Treatment and prognosisTreatment and prognosisR di l ti• Radical resection
• Poor prognosisR f• References
• Jalal Eddine El Ammari et al, “Primary malignant melanoma of the bladder,” Case reports in urology,vol.2011
• B S Stein and A R Kendall “Malignant melanoma of the genitourinary tract ” Journal ofB. S. Stein and A. R. Kendall, Malignant melanoma of the genitourinary tract, Journal of Urology, vol. 132, no. 5, pp. 859–868, 1984. View at Scopus
• A. M. Ainsworth, et al., “Primary malignant melanoma of the urinary bladder,” Cancer, vol. 37, no. 4, pp. 1928–1936, 1976. View at Scopus
• B Helpap “Nonepithelial neoplasms of the urinary bladder” Virchows Archiv vol 439 no 4• B. Helpap, Nonepithelial neoplasms of the urinary bladder, Virchows Archiv, vol. 439, no. 4, pp. 497–503, 2001. View at Publisher ∙ View at Google Scholar ∙ View at Scopus
• M. C. Wheelock, “Sarcoma of the urinary bladder,” The Journal of Urology, vol. 48, p. 628, 1942.
• N M Anichkov and A A Nikonov “Primary malignant melanomas of the bladder” The• N. M. Anichkov and A. A. Nikonov, Primary malignant melanomas of the bladder, The Journal of Urology, vol. 128, no. 4, pp. 813–815, 1982.
• C. T. Su and C. L. Prince, “Melanoma of the bladder,” The Journal of Urology, vol. 87, pp. 365–367, 1962.
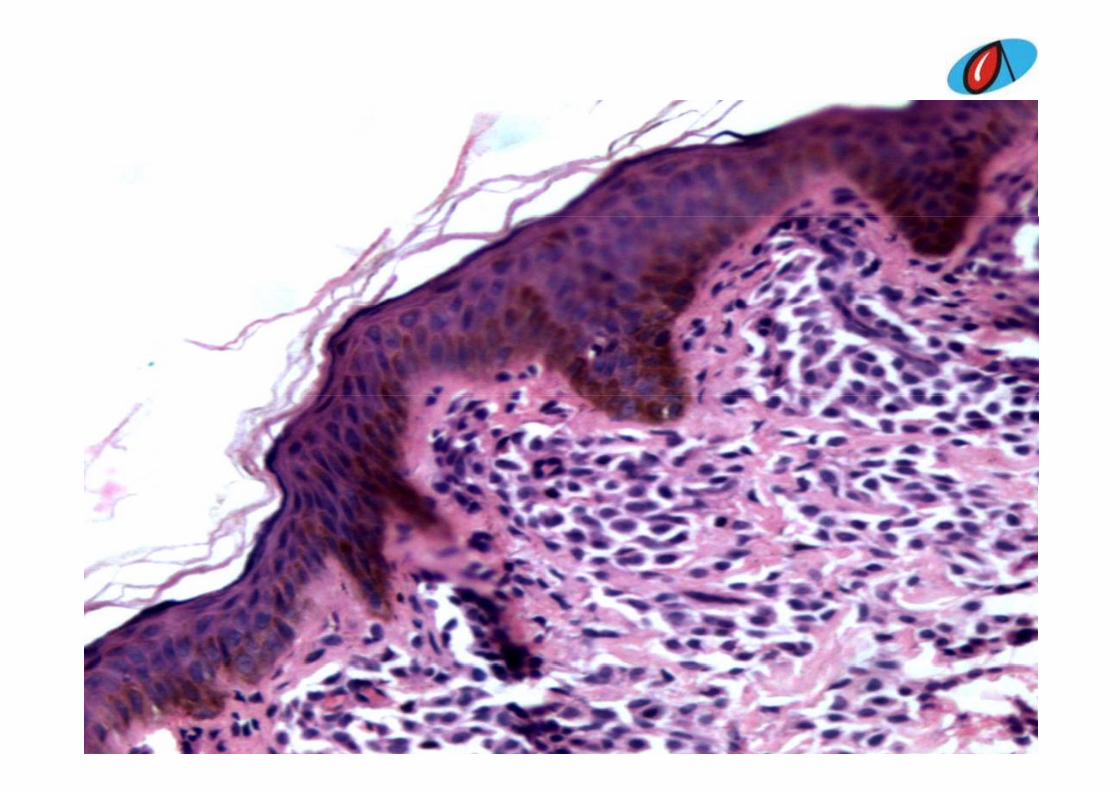
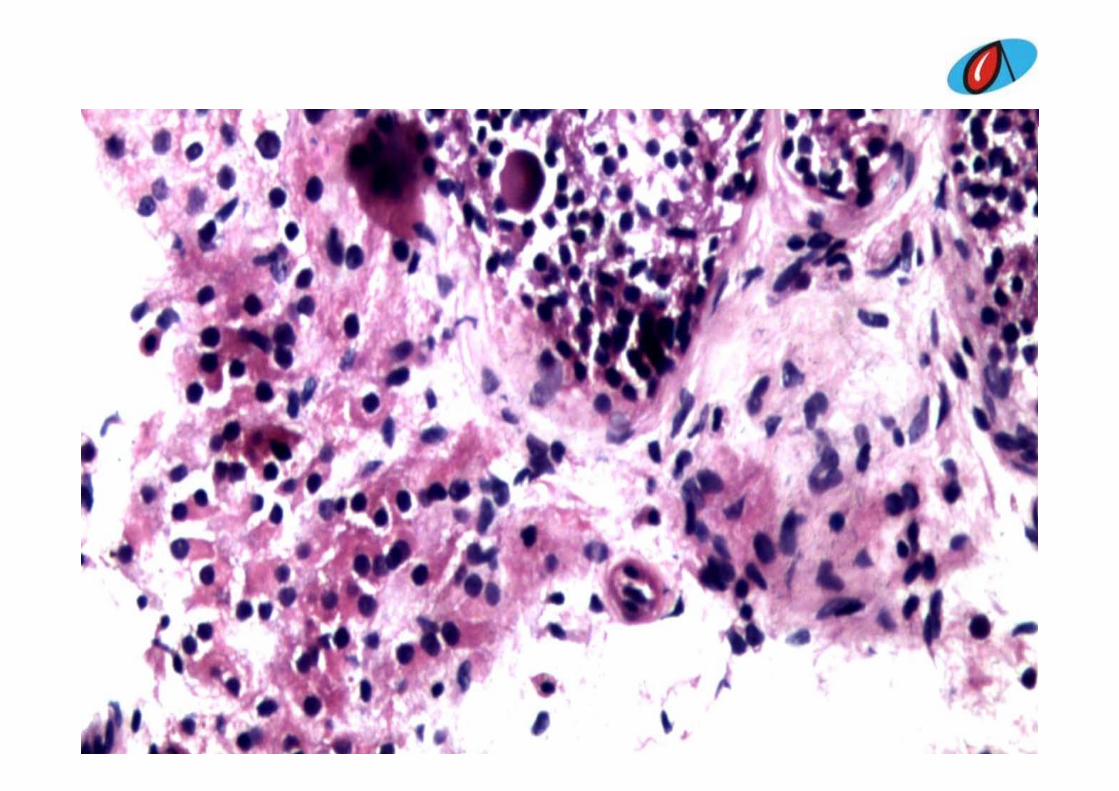
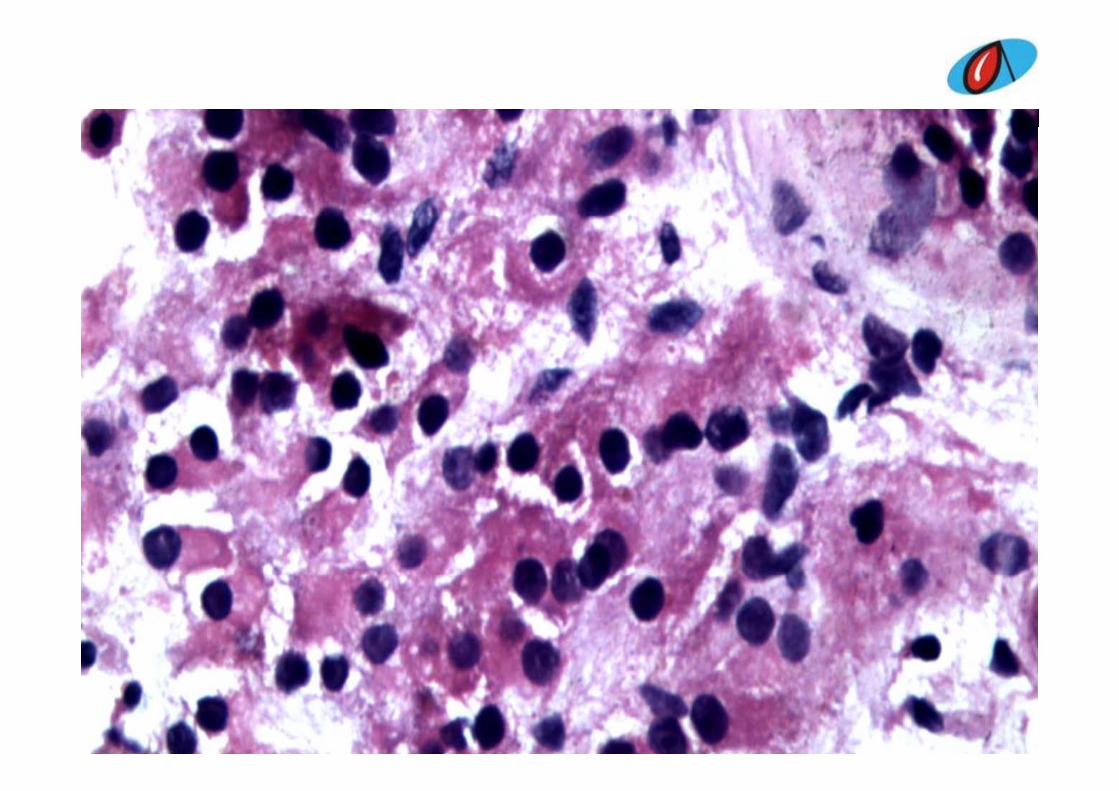
Case 9Case 9
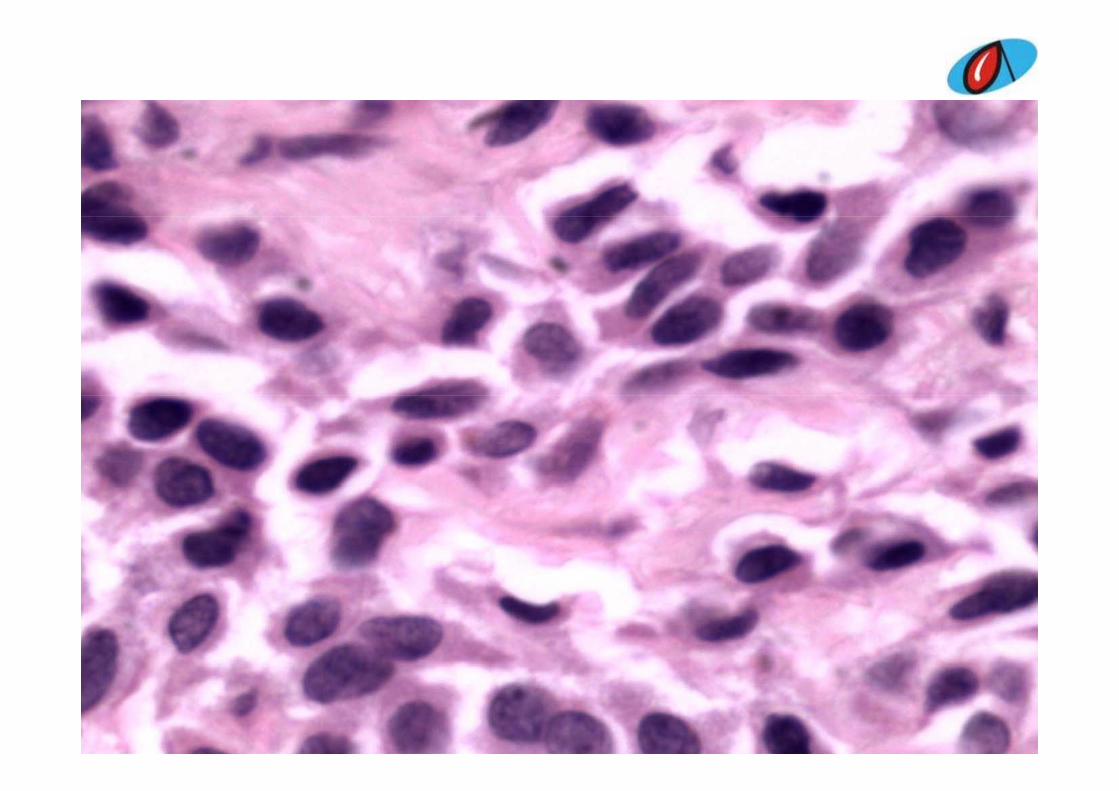
• Skin biopsy in a male patient• Age not knownAge not known
Differential diagnosisDifferential diagnosis
C t t t i• Cutaneous mastocytosis• Dermal nevus• Glomus tumor• Leukaemic infiltration• Cutaneous plasmacytoma• Lymphomatoid papillomatosis, DLE• ???• Urticaria pigmentosap g• Metastatic cutaneous deposit‐ Adenocarcinoma
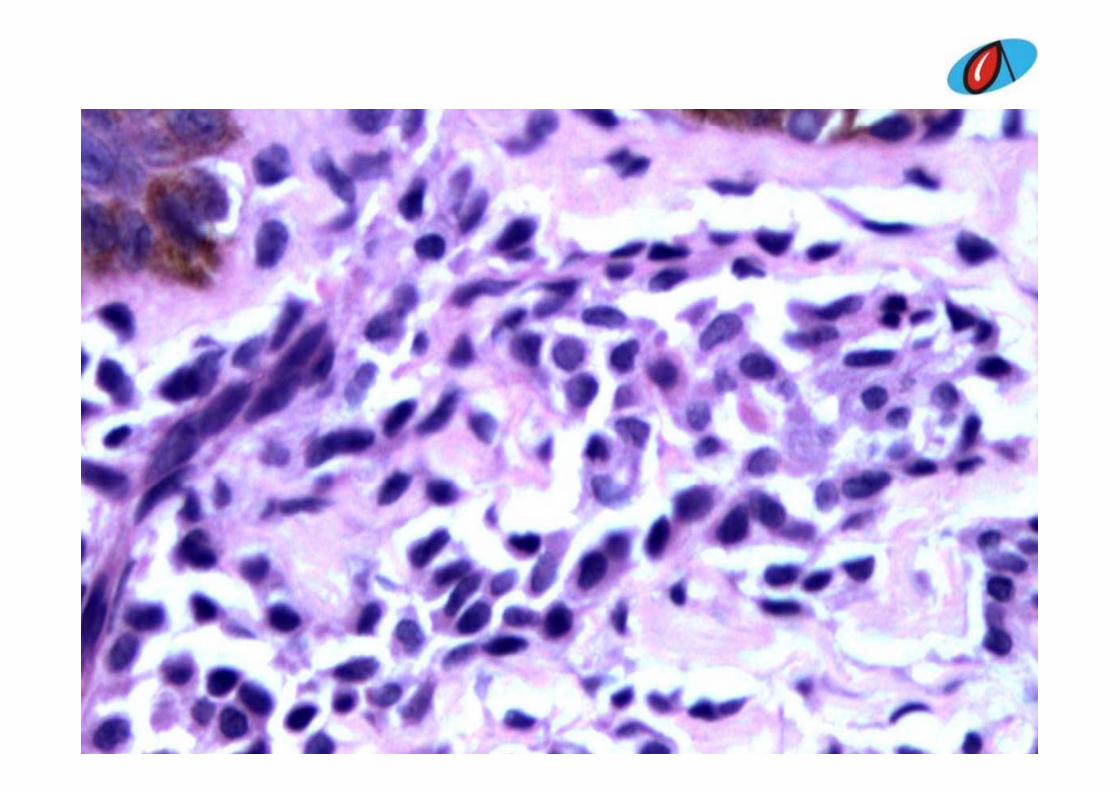
Final diagnosisFinal diagnosis
• Cutaneous mastocytosis
Cutaneous mastocytosisCutaneous mastocytosis
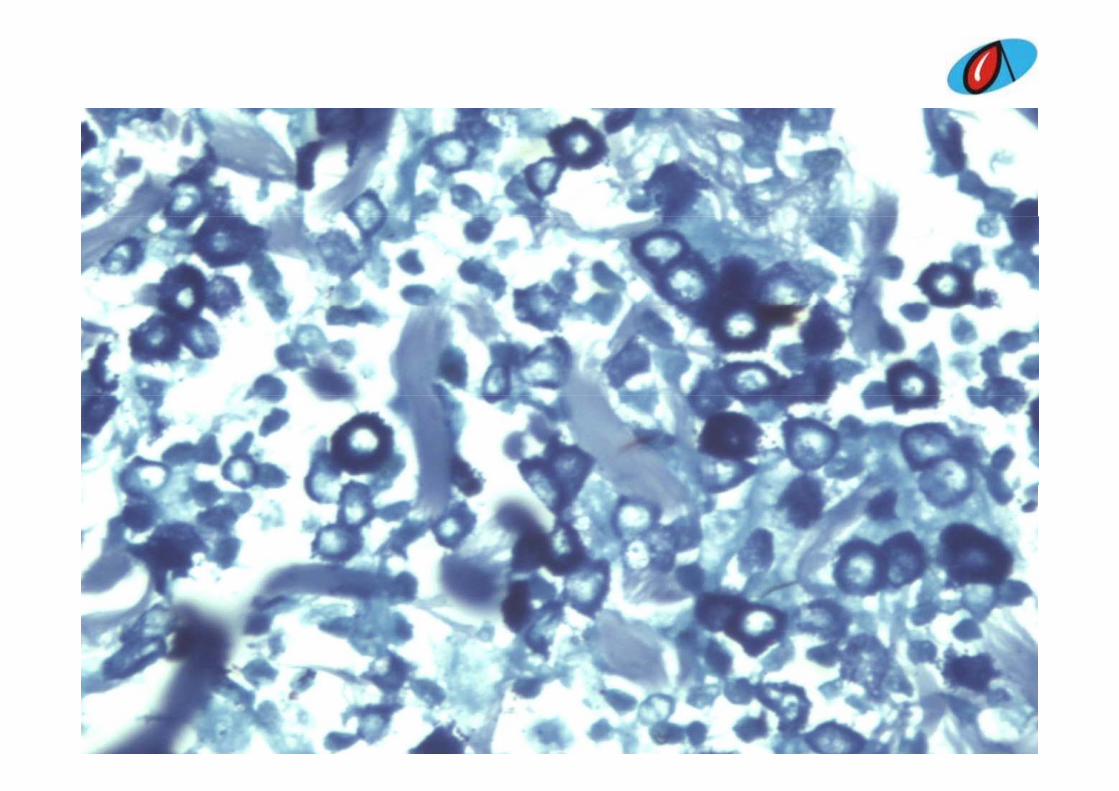
% f i i i• 80% of cases are urticaria pigmentosa• Mast cells
– 8‐15 microns in diameter– Round or oval or fusiform in shapeRound or oval or fusiform in shape– Granular cytoplasmGranules stain metachromatically with toludene– Granules stain metachromatically with toludeneblue or giemsaGranules are modified lysosomes containing– Granules are modified lysosomes containing histamines and leukotrienes
Clinical symptomsClinical symptoms
• Release of histamines and leucotrienes– Pruritis– ItchingFlushes– Flushes
– Syncope
WHO classification of mastocytosisWHO classification of mastocytosis• Cutaneous mastocytosis• Cutaneous mastocytosis
– Maculopapular CM– Diffuse CM
Mastocytoma of skin– Mastocytoma of skin• Indolent systemic mastocytosis(SM)
– Smoldering SMIsolated bone marrow mastocytosis– Isolated bone marrow mastocytosis
• Systemic mastocytosis with an associated clonal hematological non‐mast cell lineage disease
• Aggressive systemic mastocytosis• Aggressive systemic mastocytosis– With eosinophilia
• Mast cell leukaemiaAleukaemic MCL– Aleukaemic MCL
• Mast cell sarcoma• Extracutaneous mastocytoma
Case 10Case 10
• 34 yr old male• Azoospermia for evaluation.Azoospermia for evaluation.• Left and right testicular biopsy was done
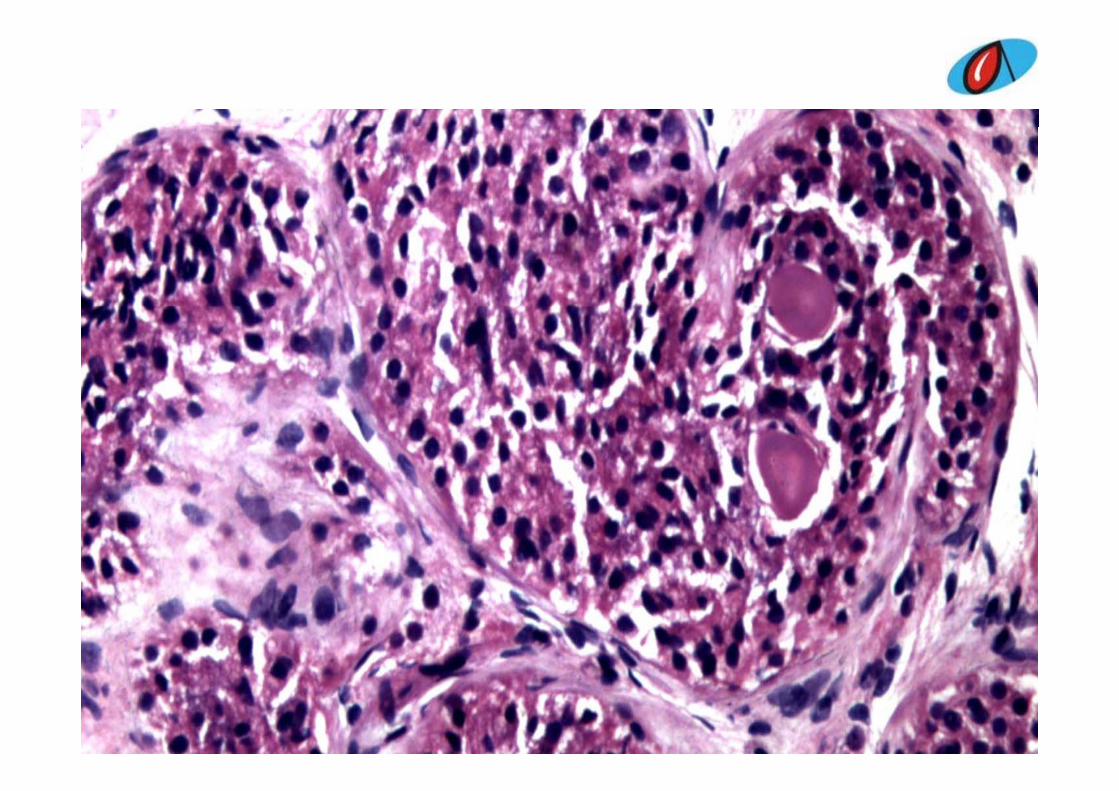
GrossGross
• Pale brown tissue bit measuring 0.6x0.3x0.3cm
Differential DiagnosisDifferential Diagnosis
S t li ll d l i t hi t ti• Sertoli cell nodule in atrophic testis.• Gonadoblastoma• Sex cord stromal tumor with annular tubules .• Testicular microlithiasis• Complete maturation arrest with corpora amylacea and microlithiasis.
• Partial maturation arrest with testicular microlithiasis
• Parasitic cysts• ITGCN
Final diagnosisFinal diagnosis
• Hamartomatous nodule in probable Androgen insensitivity syndromey y
DiscussionDiscussion
• Male AIS is a very rare disorder, affecting fewer than 1 in 100,000 births
• Two types‐ complete and incompleteX li k d l d h h di i• X‐ linked male pseudohermaphroditism
StatisticsStatistics• Affects 1 in 20,400 peopleAffects 1 in 20,400 people
– 2/3 of cases inherited from mother– 1/3 of cases come from a spontaneous mutation in1/3 of cases come from a spontaneous mutation in the egg
• No effect on life expectancyp y• No racial differences• A genetic condition where affected people have male g p p
chromosomes and male gonads with complete or partial feminization of the external genitals
• An inherited X linked recessive disease with a mutation• An inherited X‐linked recessive disease with a mutation in the Androgen Receptor (AR) gene resulting in:– Functioning Y sex chromosomeg– Abnormality on X sex chromosome
Androgen Receptor Gene• AIS results from mutations in the androgen receptor gene, located on the long arm of the X chromosome (Xq11‐q12).
• The AR gene provides instructions to make the protein called androgen receptor, which allows cells to respond to androgens, such as
d di l ltestosterone, and directs male sexual development.A d l l h i h d d i• Androgens also regulate hair growth and sex drive
• Mutations include complete or partial gene d l ti i t t ti d ll i tideletions, point mutations and small insertions or deletions.
ReferencesReferences
• 1991;10(2):126‐44.• The androgen insensitivity syndromeThe androgen insensitivity syndrome (testicular feminization): a clinicopathologicstudy of 43 casesstudy of 43 cases.
• Rutgers JL, Scully RE. University of California, Los Angeles
• Forty three patients with the androgen insensitivity syndrome (AIS) ages• Forty‐three patients with the androgen insensitivity syndrome (AIS), ages 14 to 83 (average 27) years, were studied.
• Forty patients had complete AIS and three patients had incomplete AIS.• Microscopic examination of the testes revealed immature tubules which• Microscopic examination of the testes revealed immature tubules, which
contained rare spermatogonia in 28% of the cases.• Prominent Leydig cells and a spindle‐cell stroma resembling ovarian
stroma were found in a majority of casesstroma were found in a majority of cases. • The organization of the testicular parenchyma could be classified into one
of four patterns: diffuse tubulostromal, lobular tubulostromal, mixed tubulostromal, or stromal‐predominant., p
• Hamartomas were present in 63% and Sertoli cell adenomas in 23% of the cases.
• Malignant tumors developed in 9% of the patients and comprised two g p p pseminomas, one intratubular germ cell neoplasm with early stromalinvasion, and a malignant sex cord tumor
ReferencesReferences
• Arch Pathol Lab Med‐ Vol 123, March 1999• Ackerman’s Surgical Pathology, MaleAckerman s Surgical Pathology, Male reproductive system , Pg 1438‐ 1439
Case 11Case 11
• 1 yr 4 months female baby presented with chronic renal failure and failure to thrive
• Renal biopsy was sent for light microscopy and immunofluorescenceimmunofluorescence.
GrossGross
• Single linear grey brown tissue measuring 1.5 cm in length.g

ImmunofluorescenceImmunofluorescence
• One core with 6 glomeruli, all of which are negative for IgG, IgA, IgM, C3C, C1q, kappa g g g g q ppand lambda.
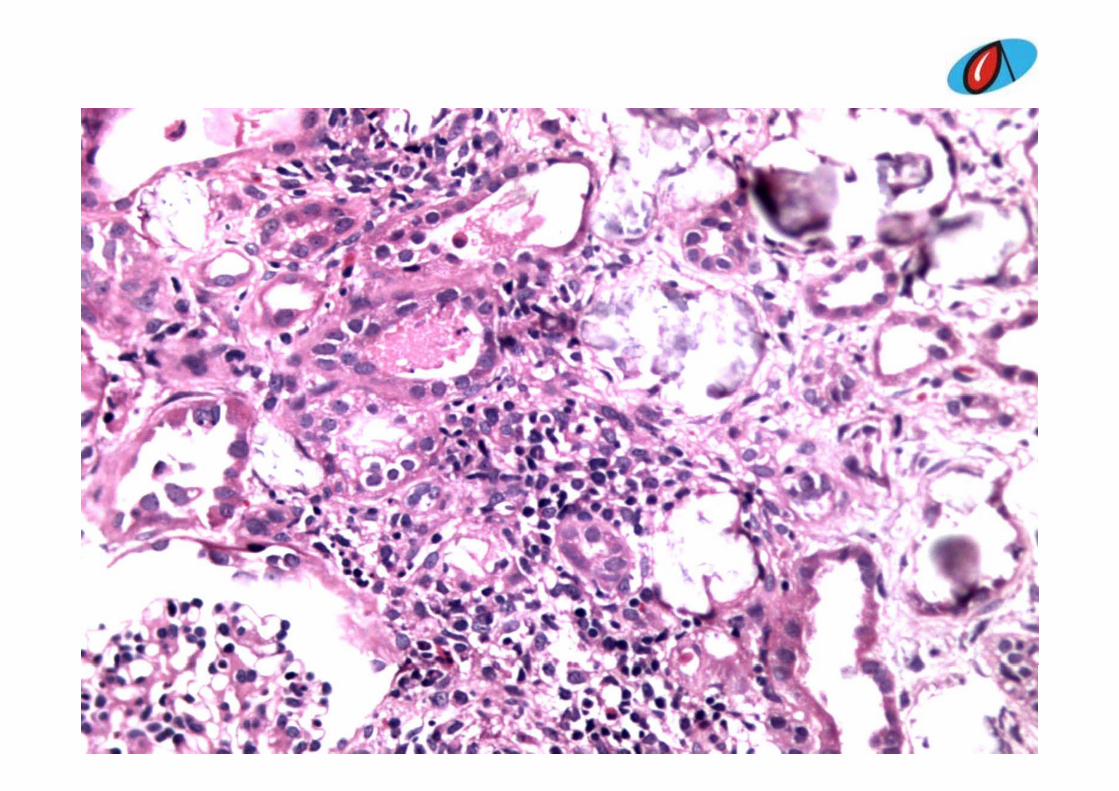
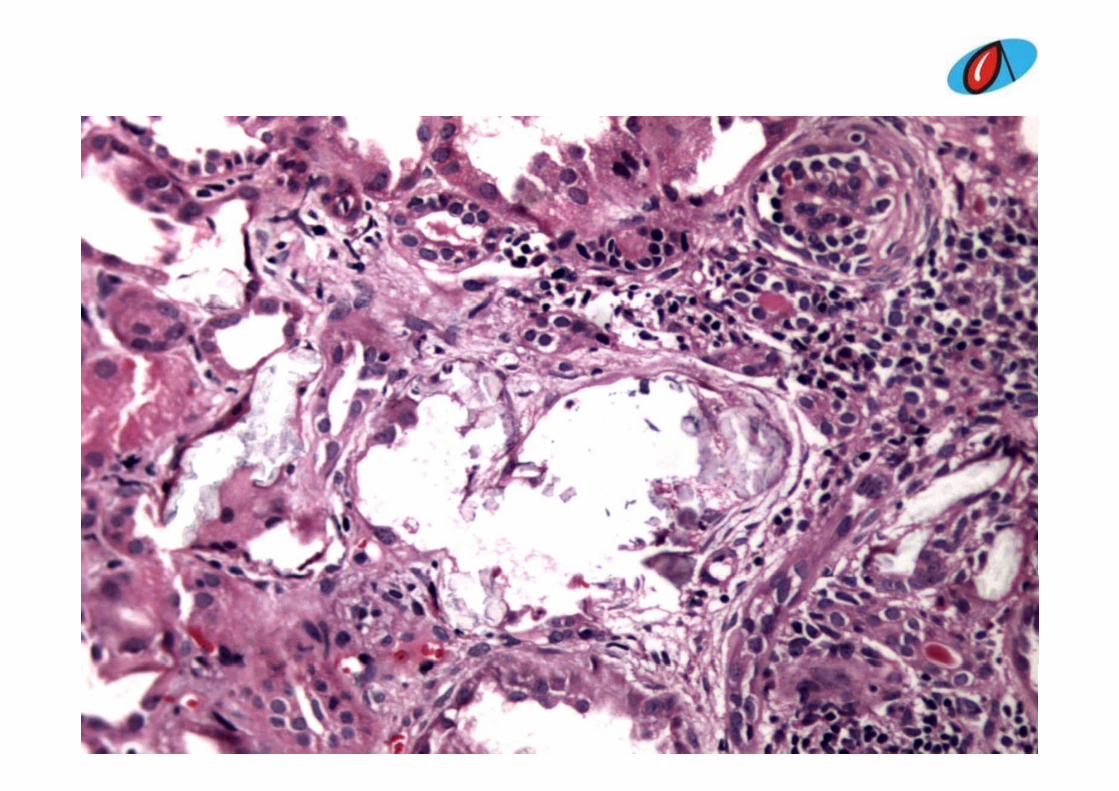
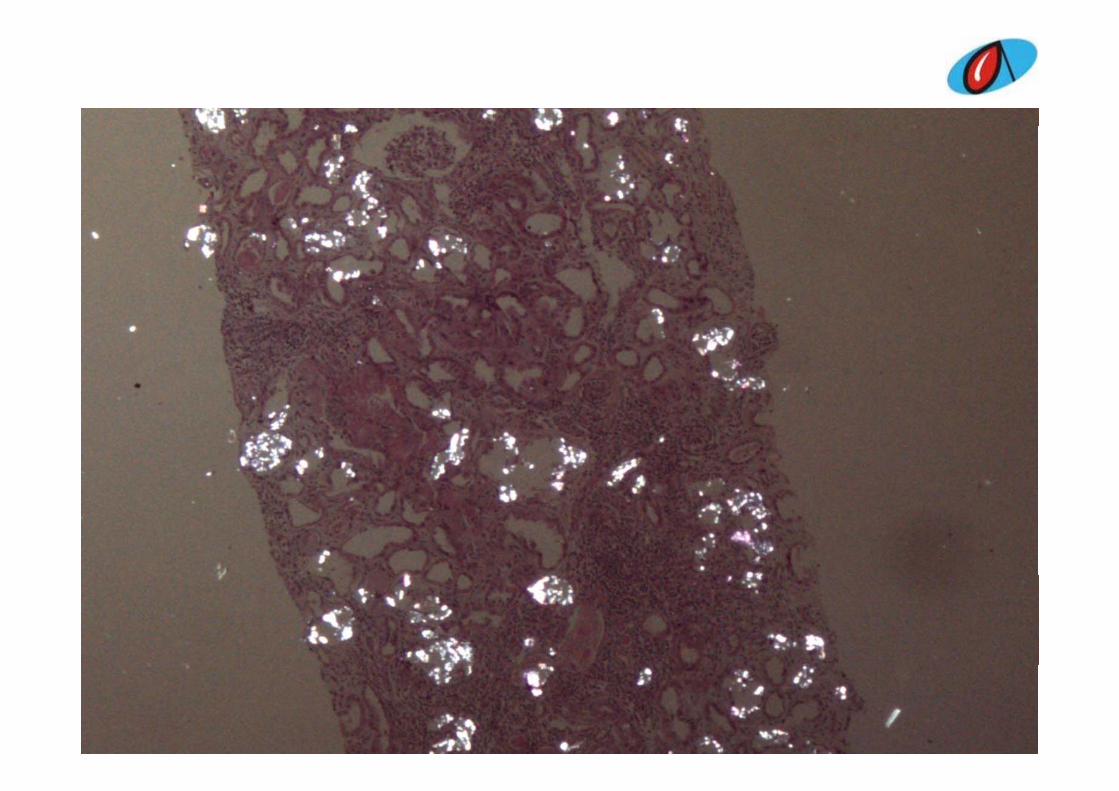
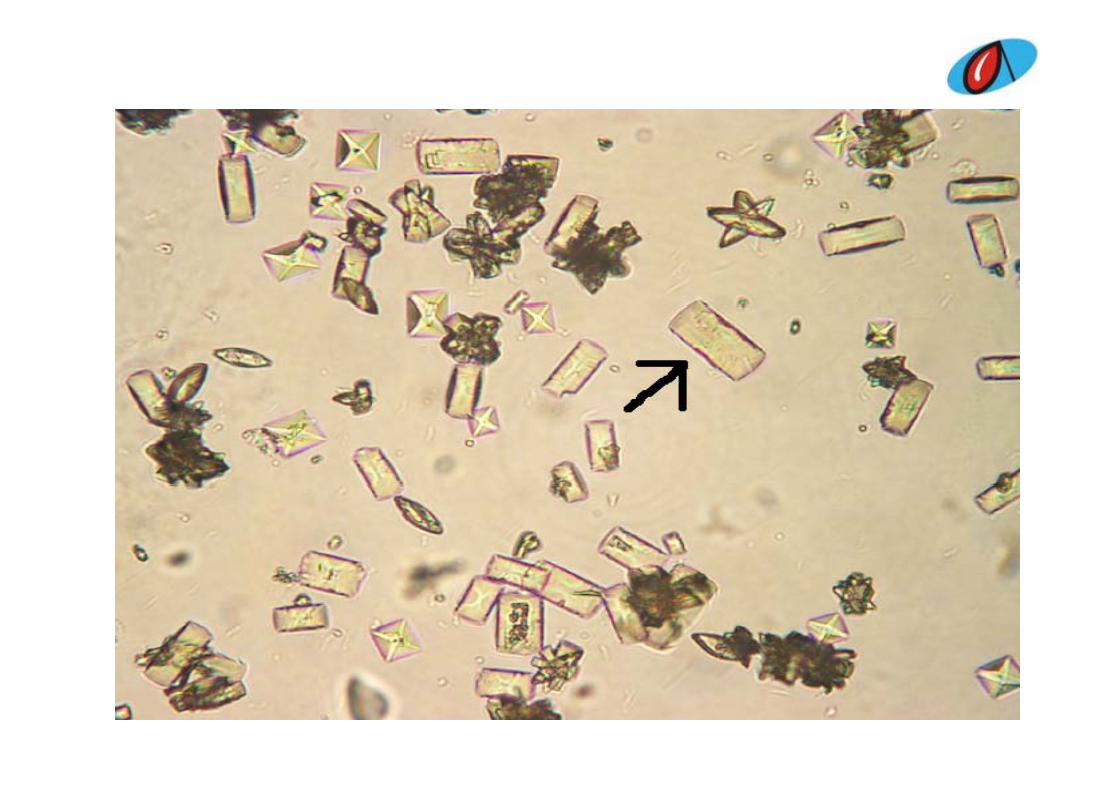
Differential diagnosisDifferential diagnosisC t lli h th• Crystalline nephropathy
• Crystalline nephropathy‐ post chemotherapy for leukemia / lymphomay p
• Crystalluria – Urate• Oxalosis• Infantile nephropathic cystinosis• Nephrocalcinosis
T b l i t titi l h iti i t d ith t b l i• Tubulointerstitial nephritis associated with tubular necrosis• Nephrocalcinois• Storage disease ?• Storage disease ?• Multicystic renal dysplasia• Nephronophthisisp p
Final diagnosisFinal diagnosis
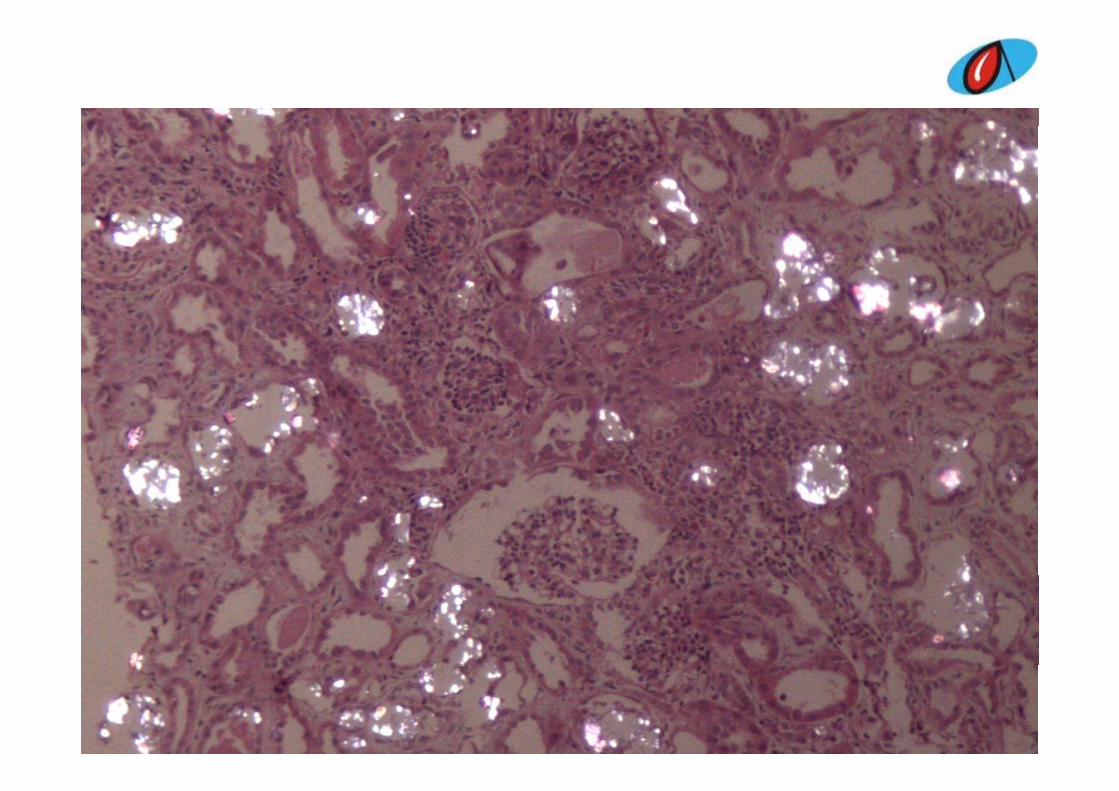
• Chronic tubulointerstitial nephritis secondary to crystalluria morphology favoring Oxaluria.y p gy g
HyperoxaluriaHyperoxaluria
i l i h d 0• Urinary oxalate excretion that exceeds 40 mg/day.
• Primary ( rare genetic disease)
• Enteric
• Dietary
• Idiopathic or mild hyperoxaluria
Primary hyperoxaluria
Type I mutation of AGXT gene on chromosome 2 that codes for alanine glyoxylate aminotransferasealanine glyoxylate aminotransferase
Type IImutation of GRHPR gene on chromosome 9 that codesType II mutation of GRHPR gene on chromosome 9 that codes for glyoxylate reductase and hydroxypyruvate reductase.
ReferencesReferences
• Shekarriz B et al ; Hyperoxaluria ,emedicine, Apr 2010p
• Ackerman’s Surgical Pathology, Urinary tract, Pg 1231Pg‐ 1231
• Diagnostic pathology kidney disease , Colvin‐Pg4‐ 106
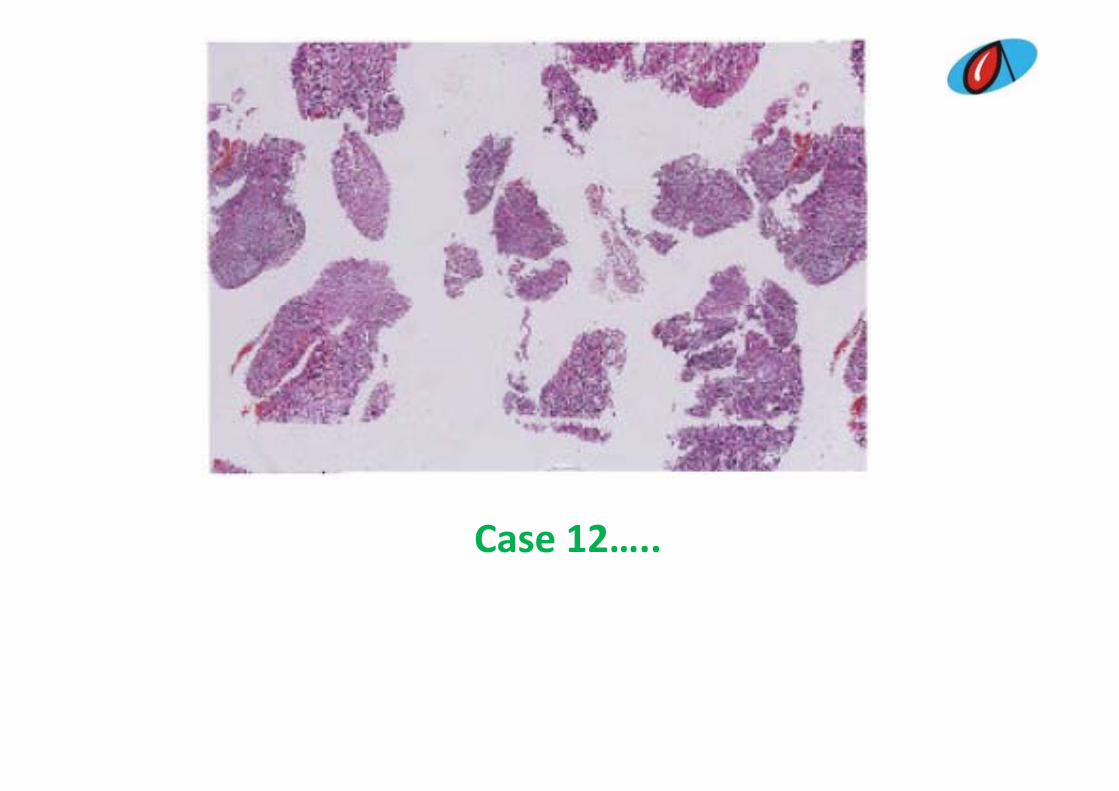
Case 12…..
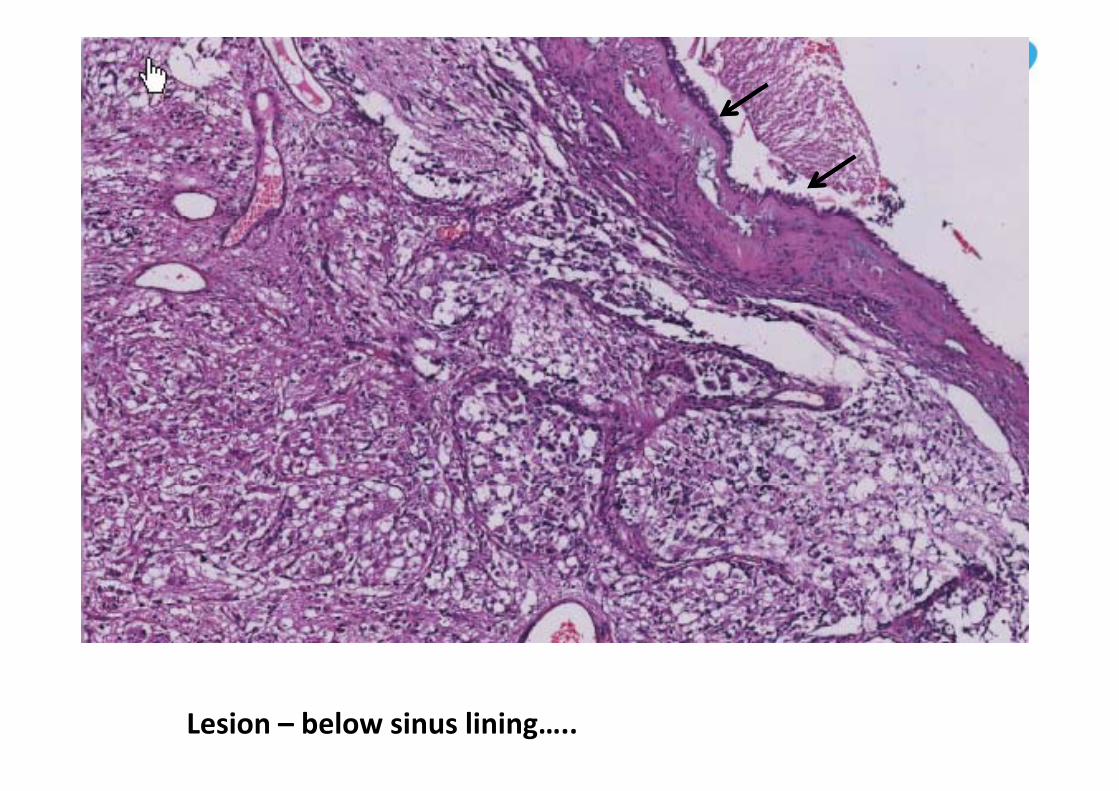
Lesion – below sinus lining…..
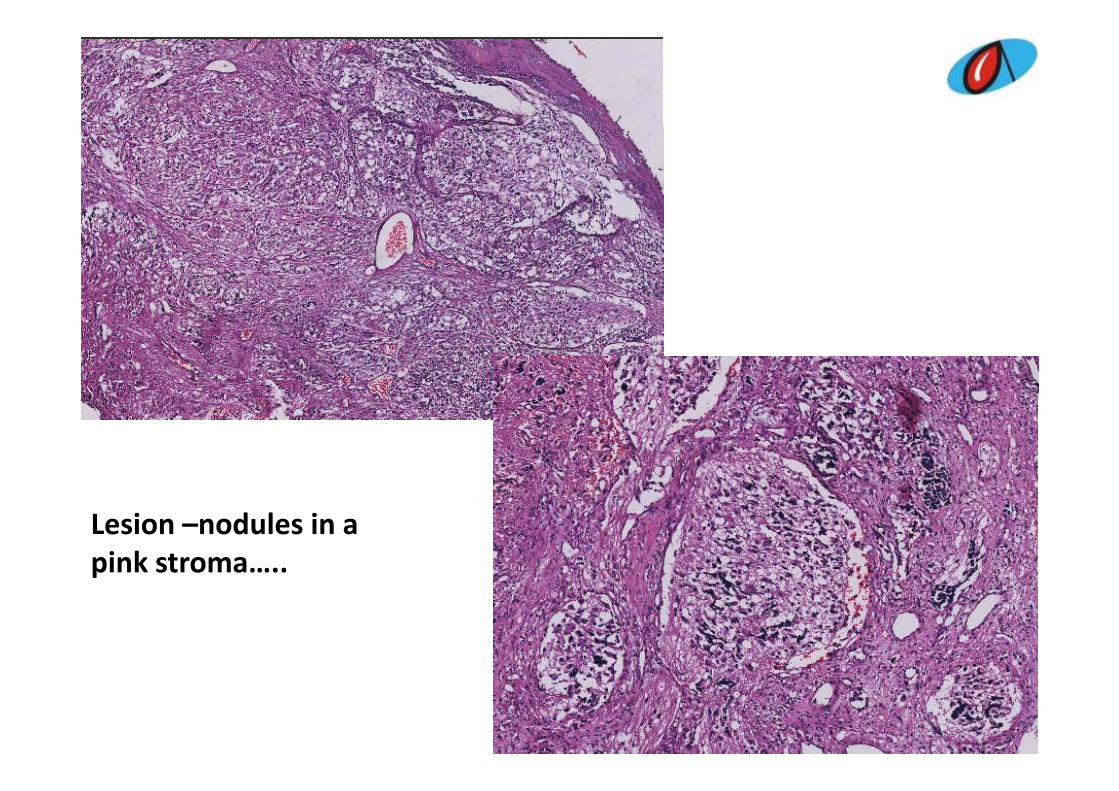
Lesion –nodules in a pink stroma…..p
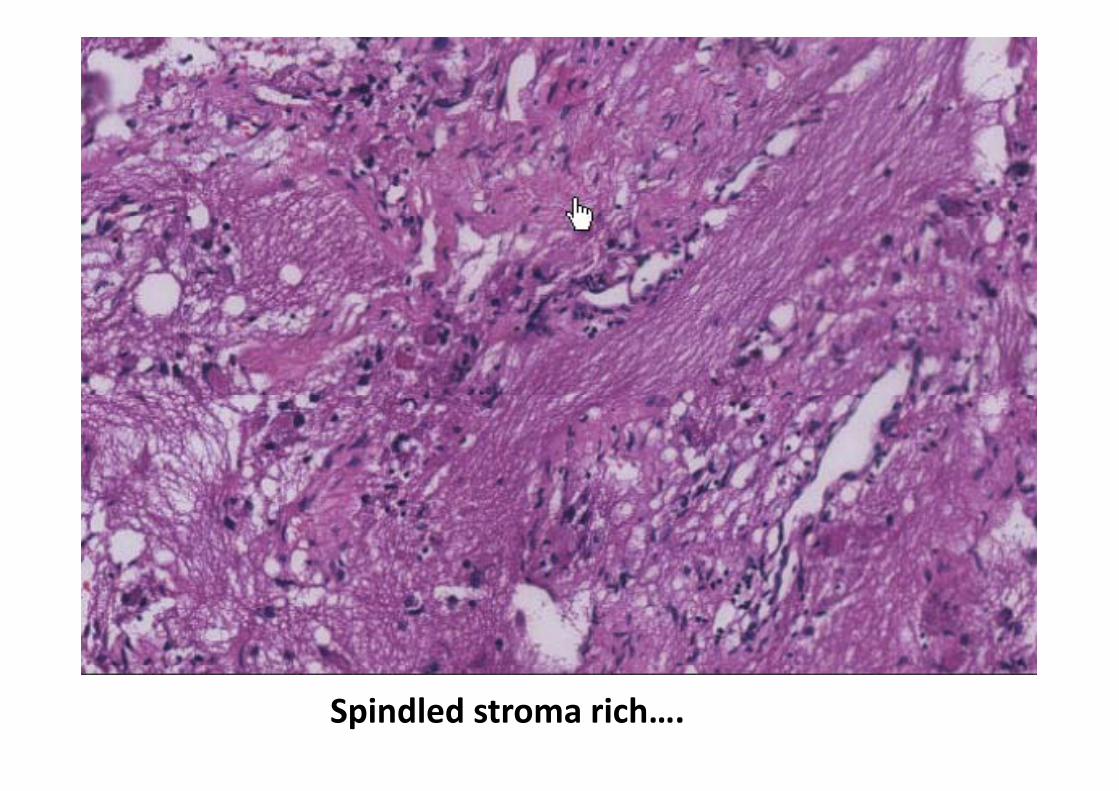
Spindled stroma rich….
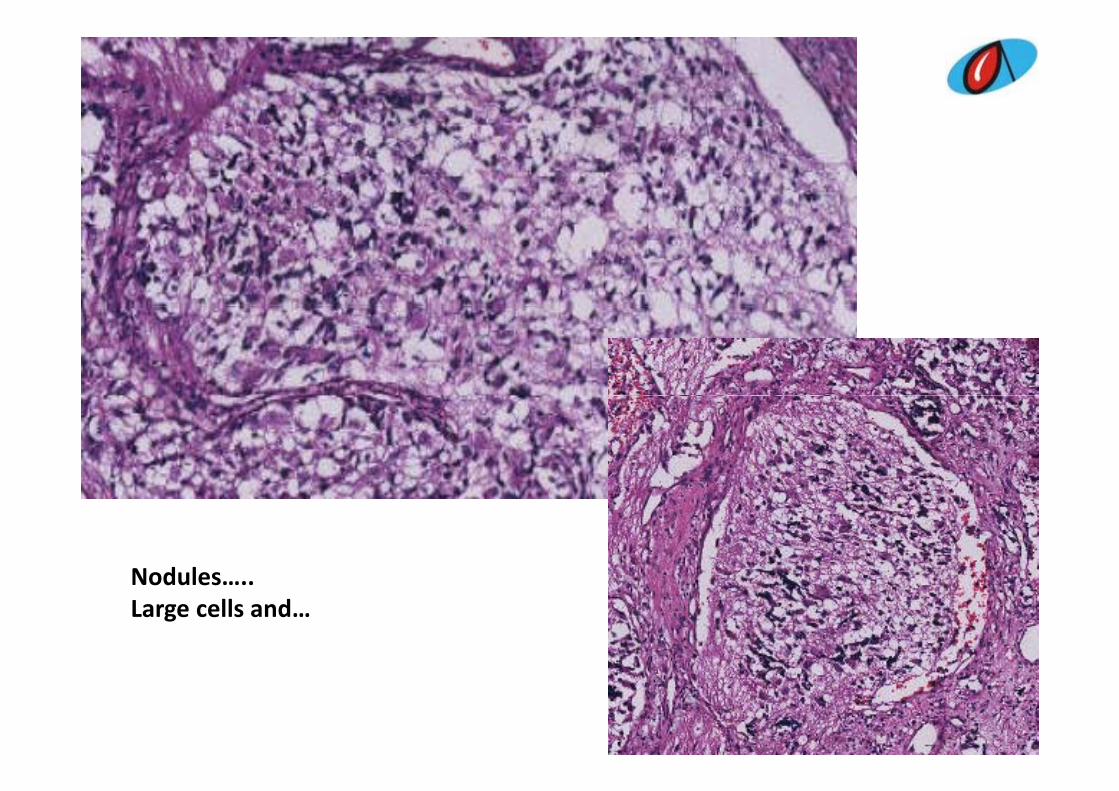
NodulesNodules…..Large cells and…
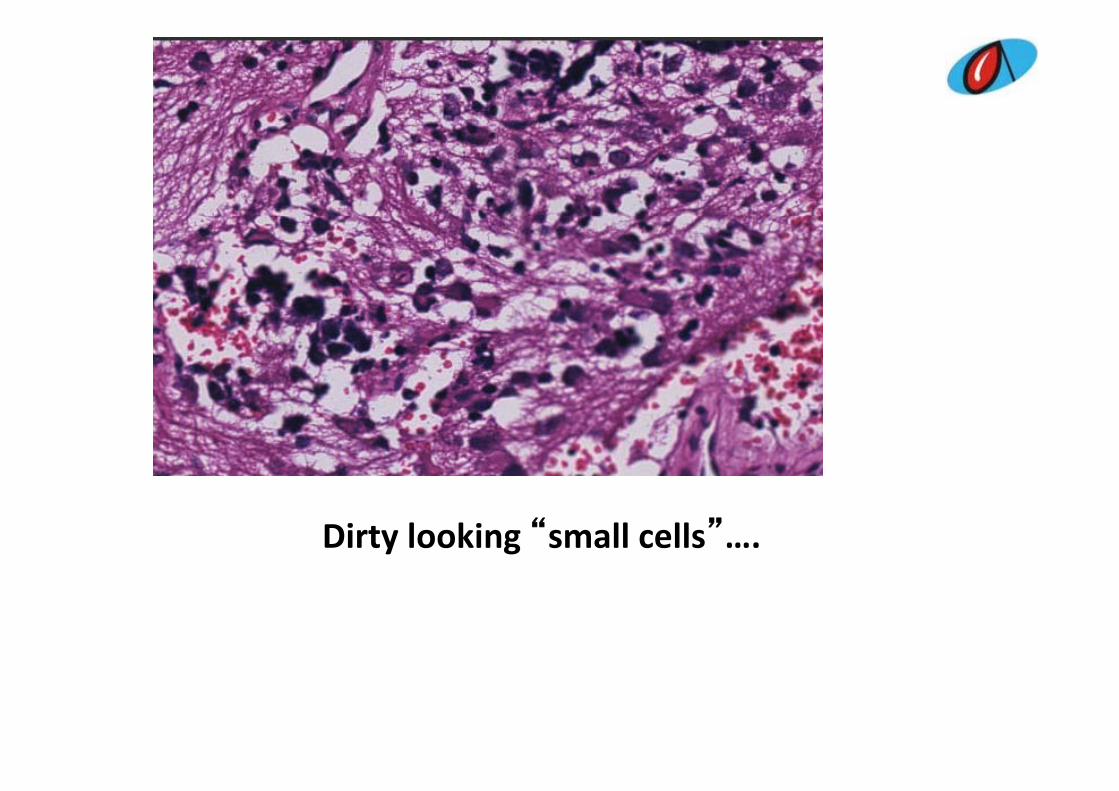
Dirty looking “small cells”….
SoSo…..
• Poorly circumscribed, submucosal lesion in sinus
• Nodules + spindled stromaN d l• Nodules: – large cells with prominent nucleoli– Component of dirty looking small cells in aggregatesaggregates
DiagnosesDiagnoses…..
b l h bd• Embryonal rhabdomyosarcoma ‐ 2• Olfactory neuroblastoma‐ 2y• Ganglioglioma ‐2• Astrocytoma 2• Astrocytoma ‐2• Carcinosarcoma ‐1• Rhinoscleroma ‐1• Melanoma ‐1Melanoma 1• Ganglioneuroblastoma‐ 1
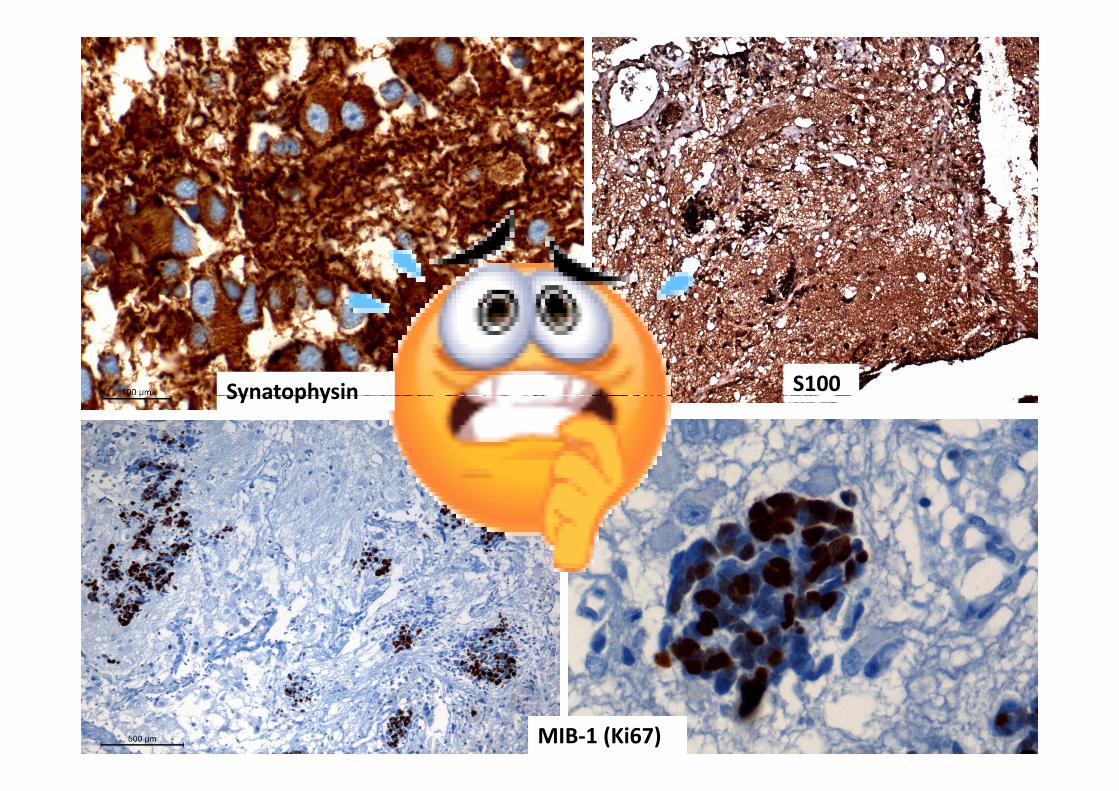
Synatophysin S100Synatophysin
MIB‐1 (Ki67)
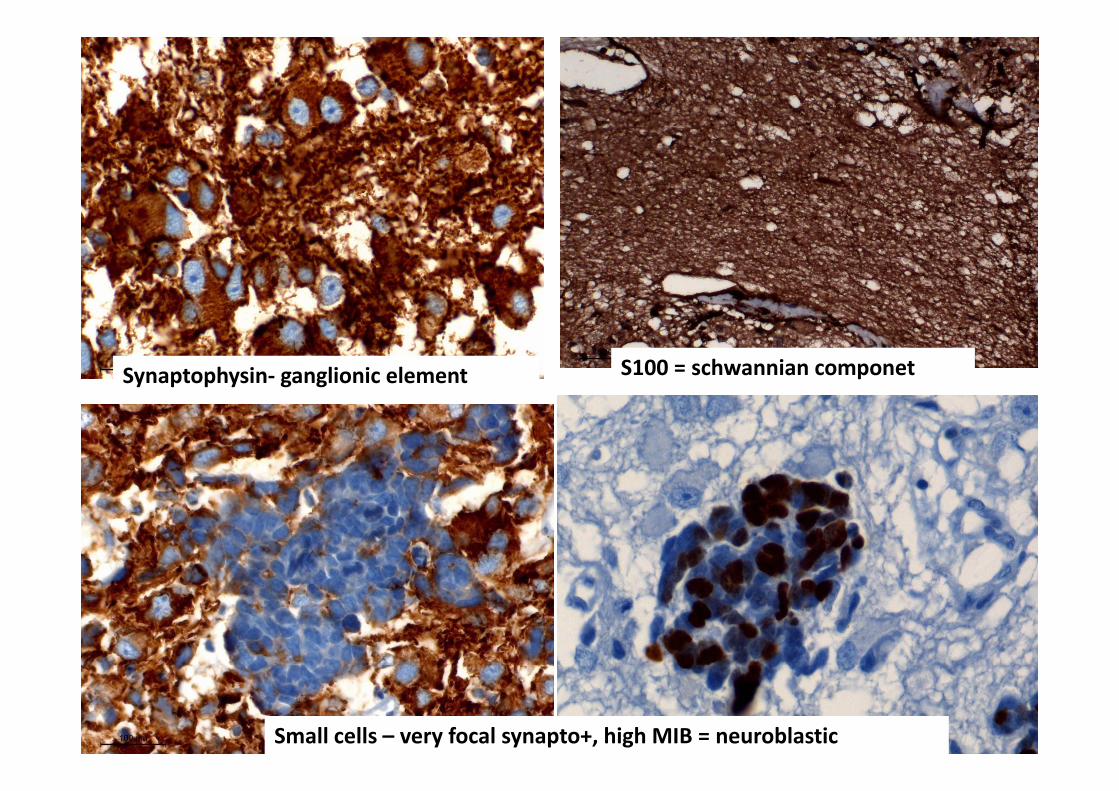
Synaptophysin‐ ganglionic element S100 = schwannian componet
Small cells – very focal synapto+, high MIB = neuroblastic
SoSo…..• Poorly circumscribed submucosal lesion in sinus• Poorly circumscribed, submucosal lesion in sinus• Nodules + spindled stroma• Stroma: schwannian (S100 pos)• Nodules:Nodules:
– large cells with prominent nucleoli: ganglionic(neuronal marker synaptophysin pos)(neuronal marker synaptophysin pos)
– Component of dirty looking small cells in aggregates (neuroblastic: synapto focal pos high MIB 1)(neuroblastic: synapto focal pos, high MIB‐1)
Ganglioneuroblastoma
Peripheral neuroblastic tumors Not so grey….
Cl ifi i• Classification…….• Staging……• Risk stratification……• Closely related to the molecular/geneticClosely related to the molecular/genetic properties of the tumors of individual cases not –tumor margins/necrosis/vascular invasion/tumor margins/necrosis/vascular invasion/ spread…as in other tumors
Players….pathology…..behaviour (pathobiology…)
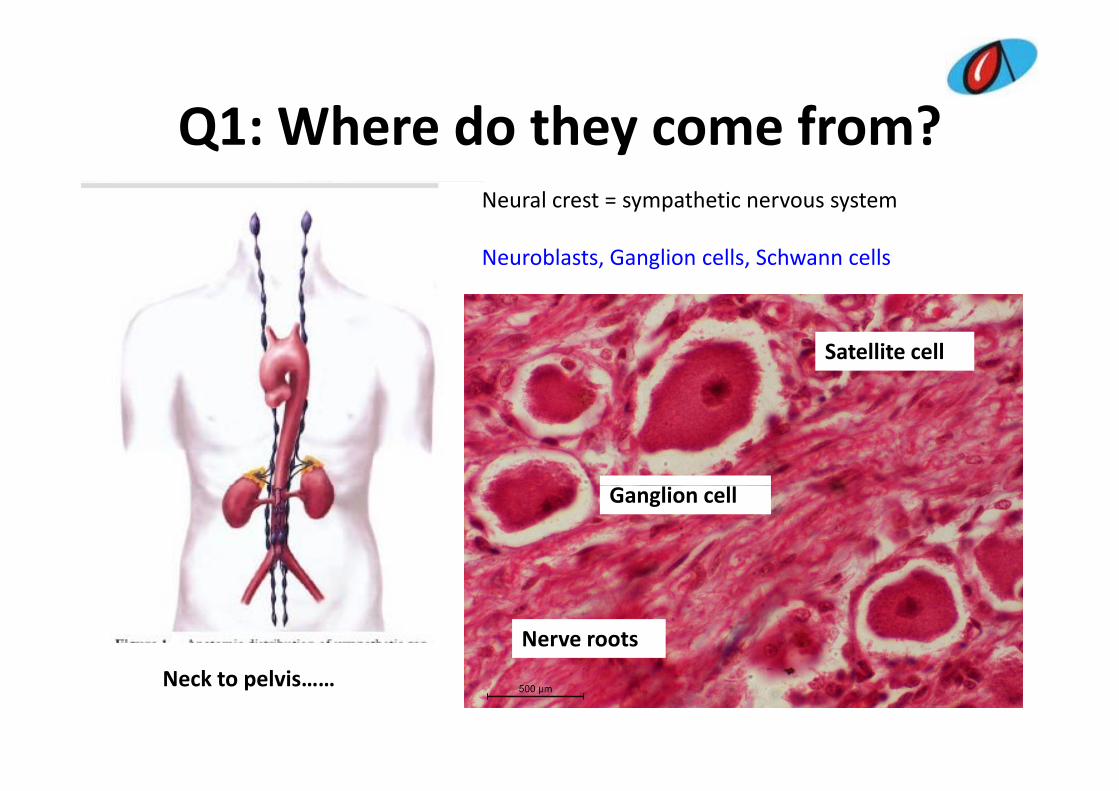
Q1: Where do they come from?Q1: Where do they come from?Neural crest = sympathetic nervous system
Neuroblasts, Ganglion cells, Schwann cells
Satellite cell
Ganglion cell
Nerve roots
Neck to pelvis……
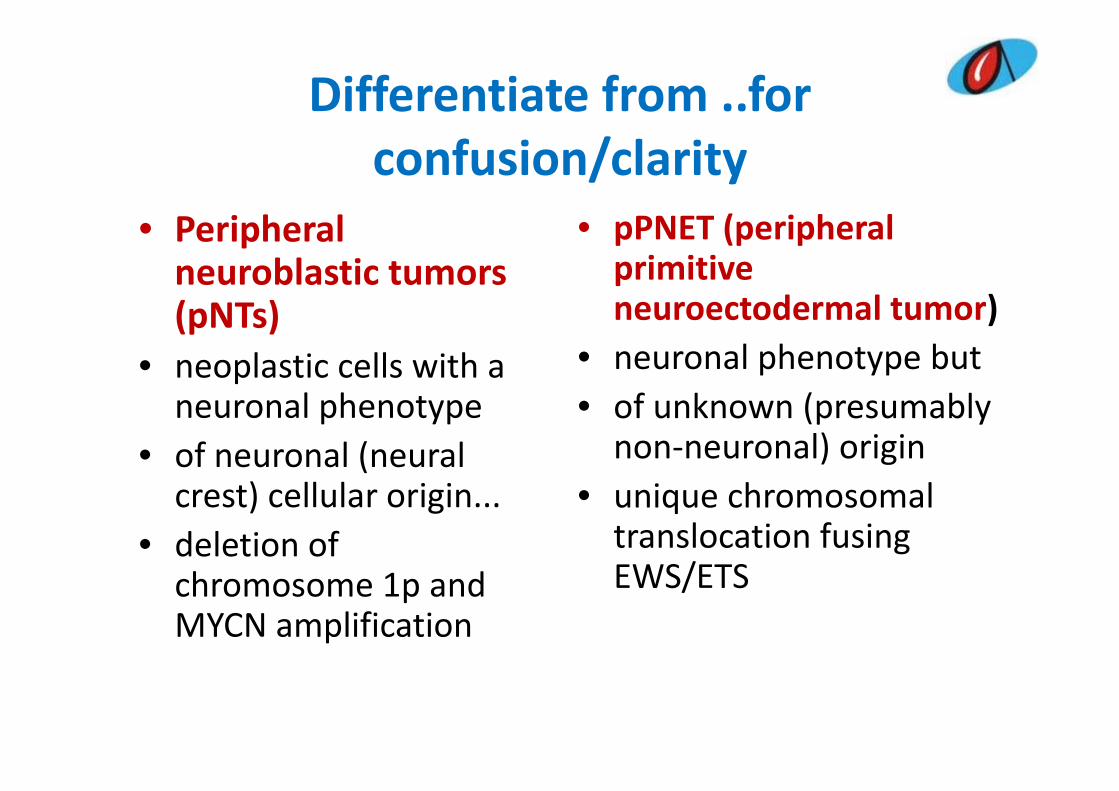
Differentiate from ..for confusion/clarity
i h l PNET ( i h l• Peripheral neuroblastic tumors ( NT )
• pPNET (peripheral primitive neuroectodermal tumor)(pNTs)
• neoplastic cells with a l h
neuroectodermal tumor)• neuronal phenotype but
f k ( blneuronal phenotype • of neuronal (neural
t) ll l i i
• of unknown (presumably non‐neuronal) origin
i h lcrest) cellular origin... • deletion of
h 1 d
• unique chromosomal translocation fusing EWS/ETSchromosome 1p and
MYCN amplificationEWS/ETS
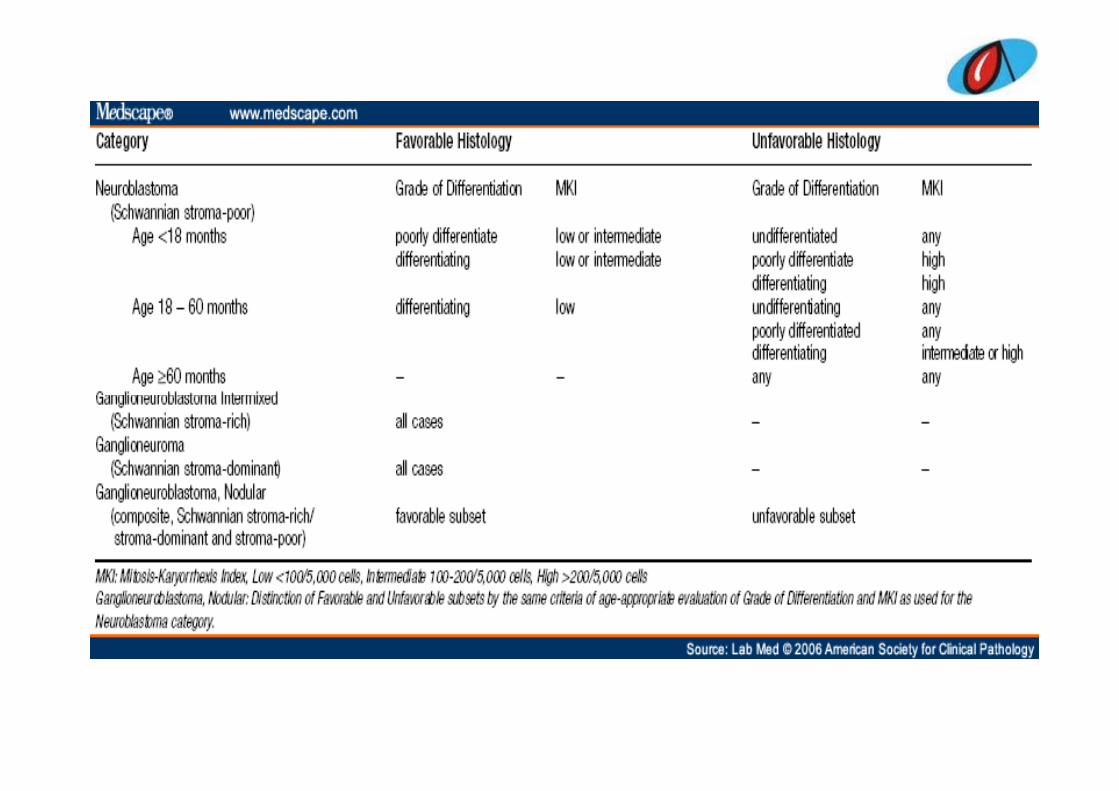
How do they look? I t ti l N bl t P th l Cl ifi tiInternational Neuroblastoma Pathology Classification
(INPC ‐ Shimada system)• Four categories are discriminated according to the degree of
differentiation[ganglionic cells 'organoid' maturation with the development[ganglionic cells, organoid maturation with the development of a Schwann cell stroma, and co‐existence of clones of different maturity or of distinct aggressiveness]:
Neuroblastoma (Schwannian stroma‐poor) (undifferentiated, poorly differentiated, dfferentiating)Ganglioneuroblastoma intermixed (Schwannian stroma‐rich)Ganglioneuroblastoma nodular g(composite Schwannian stroma‐rich/and stroma‐poor)Ganglioneuroma (Schwannian stroma‐dominant) (maturing mature)(maturing, mature)
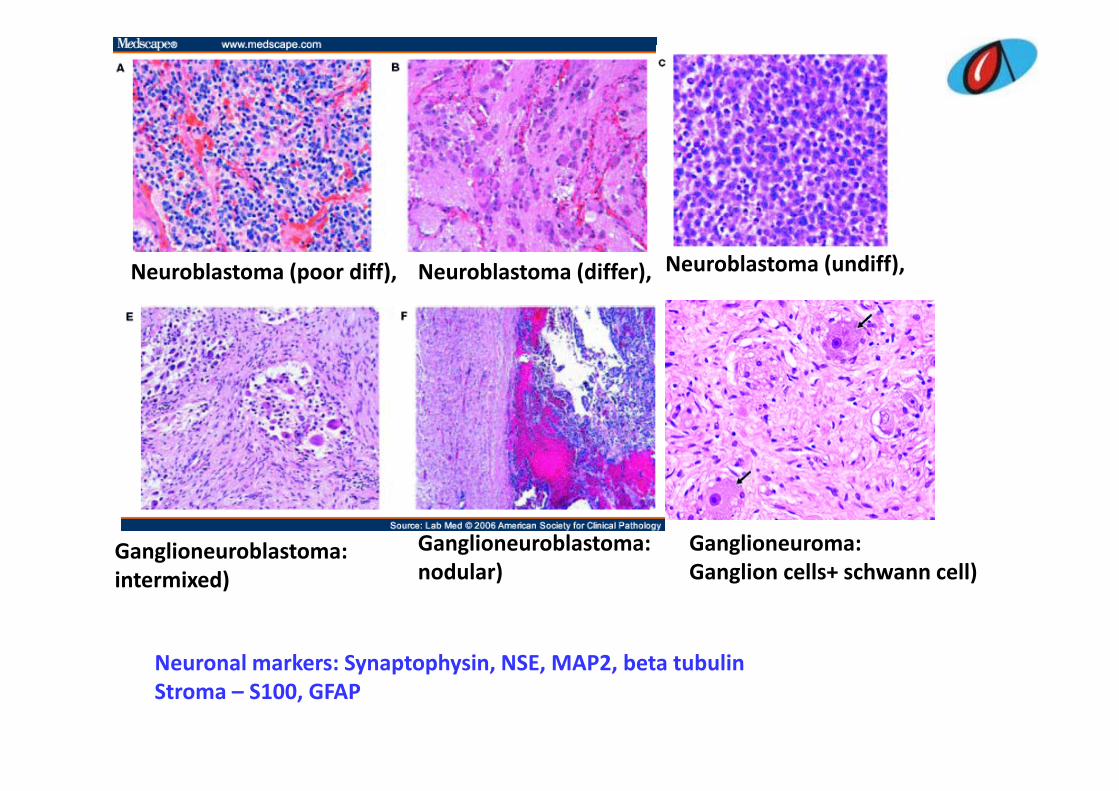
Neuroblastoma (poor diff), Neuroblastoma (differ), Neuroblastoma (undiff),
Ganglioneuroma: Ganglion cells+ schwann cell)
Ganglioneuroblastoma: i t i d)
Ganglioneuroblastoma: nodular) Ganglion cells+ schwann cell)intermixed) nodular)
Neuronal markers: Synaptophysin NSE MAP2 beta tubulinNeuronal markers: Synaptophysin, NSE, MAP2, beta tubulinStroma – S100, GFAP
How do they behave? stratificationHow do they behave? stratification….• Clear stratification – “favourable”/Clear stratification favourable / “unfavourable” clinical/biological behaviors:
• Favourable (with/without treatment)Favourable (with/without treatment)– involution, spontaneous regression– spontaneous regression,
– tumor maturation, • Unfavorable: OR aggressive progression• Unfavorable: OR aggressive progression,• Closely related to the molecular/genetic
i f h f i di id lproperties of the tumors of individual cases not –tumor margins/necrosis/vascular invasion/
dspread…
How do they behave? stratificationHow do they behave? stratification
I t ti l N bl t Ri k G i• International Neuroblastoma Risk Grouping, INRG: Prior to any treatment patients will be put into a risk categoryinto a risk category
• Favourable/unfavourable histology– Age– Age– Mitosis/karryorhhexis index (MKI)
• Low: <100/5000 cells/• Intermediate: 100‐200/5000 cells• High: >200/5000 cells
DNA l id (FISH)– DNA ploidy (FISH)– MYCN amplification status
Why bother? treatmentWhy bother?...treatment
i h f• In European countries , the treatment of neuroblastoma patients depends on – age at diagnosis (below or over 1 year of age), – extent of the disease (stage) g– a genetic parameter, i.e. the amplification of the MYCN oncogene
• In United States and Australia, DNA Index of the tumour cells and histopathology (INPC)the tumour cells and histopathology (INPC) are also included in therapy stratification
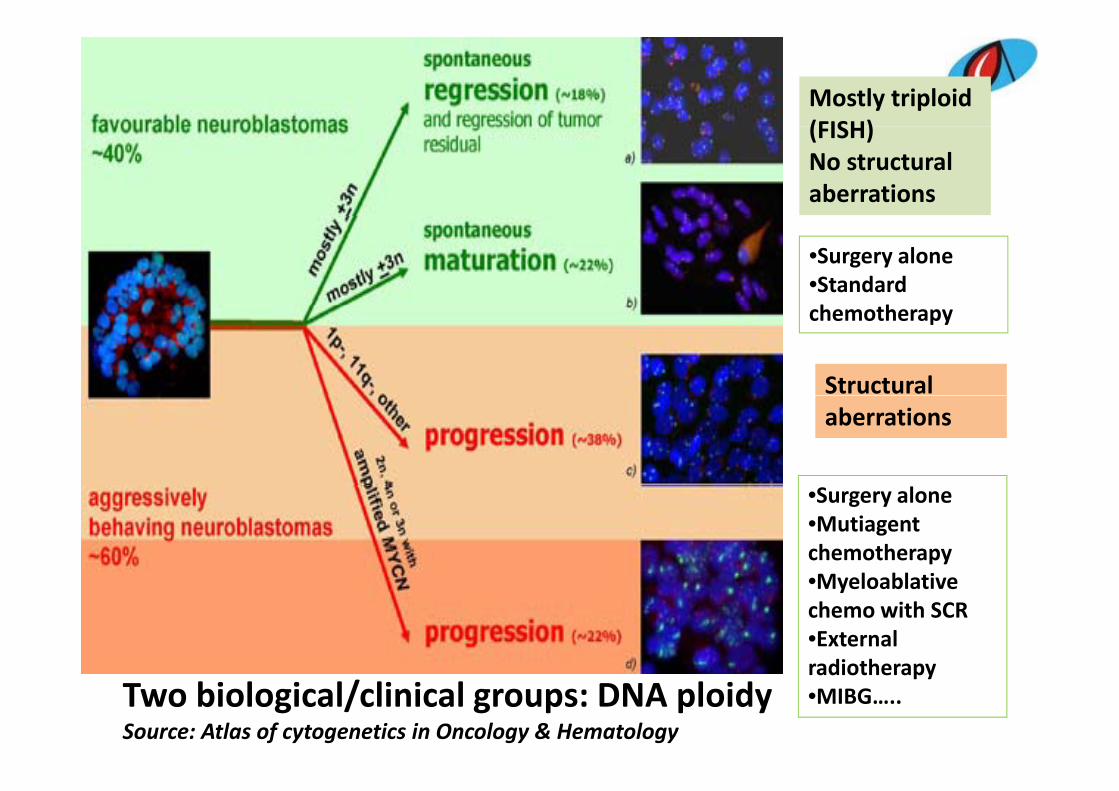
Mostly triploid(FISH)(FISH)No structural aberrations
•Surgery alone•Standard h h
Structural
chemotherapy
aberrations
•Surgery alone•Mutiagent chemotherapyM l bl ti•Myeloablative chemo with SCR•External radiotherapy
Two biological/clinical groups: DNA ploidySource: Atlas of cytogenetics in Oncology & Hematology
radiotherapy•MIBG…..
Bottom lineBottom line….
• Our case– Ganglioneuroblastoma, intermixedg ,– MKI: ?Favourable histology– Favourable histology
The Wrong RightI screened the slide back and forthAs I peeked through the microscopeA furious looking cell stared at meEureka! I exclaimed with pride and gleep g‘Carcinoma’ was my undoubted decreeMy adamant colleague refused to agreeHe made a mockery of my grey cell abilityHe made a mockery of my grey cell abilityAs he dismissed my verdict with a tinge of hostility‘Tis just a inflammatory cell, buddyAs benign as a dead flea!As benign as a dead flea!My expertise doubted, my self‐esteem trampledA severe blow to my medical arroganceI k i h llI took it up as a challengeMy insult I needed to avengeHow can “I” be proven erroneous?Both of us sought the counsel of Big BossWhose eyes can swoop on a cell like a hawkI prayed my belligerent colleague be proven wrongp y y g g p gAnd my joy knew no bounds“It is malignancy” he assertively pronounced

My battered ego appeasedOut of the hospital stormed an egotistEcstatic at being proven a whizI deserved to treat myself to a drinkThree cheers for me –An adept pathologist!On my way I glanced at the lady, frail and oldAwaiting her young son’s report with hopeI did not to notice her, of coursed d o o o ce e , o cou seCoz I wasn’t going to be the one to give her the newsThat her young son had only a few tomorrowsI sat in my car and pondered where to party that eveningI sat in my car and pondered where to party that eveningBut something gnawed at my heart; an intense achingHot Tears poured down my cheeks sans warningUndid the façade I was sportingUndid the façade I was sportingThe wee bit of a human hidden in me startled my beingLate into the sleepless night I had a dream
d h d f lBig Boss admonished me, yet on my face I saw a gleamA single streak of the whitener fluid he drewTo erase my reporting and write one anewDo early morning dreams really come true?
Reeta Subramaniam Mani
Thank youThank you





























