Embed Size (px)
Citation preview

Anatomy , Physiology& Basic Concepts of IV Fluids
Dr.Ravindar Bethi, MDSpecialist , Anesthesia & ICU,Al Rass General Hospital, KSA.
IV THERAPY - AN OVERVIEW

IV THERAPY - AN OVERVIEW
Intravenous therapy or IV therapy is the giving of liquid substances
directly into a vein.

IV THERAPY - AN OVERVIEW
Compared with other routes of administration, the intravenous route is
the fastest way to deliver fluids and medications throughout the body.

IV THERAPY - AN OVERVIEW
It is commonly referred to as a drip because it employs a
drip chamber, which prevents
air entering the blood stream (air embolism)
and allows an estimate of flow rate.

FLUIDS AND ELECTROLYTES
ANATOMY AND PHYSIOLOGY
IV THERAPY - AN OVERVIEW

ANATOMY AND PHYSIOLOGY
Dorsal venous arch

ANATOMY AND PHYSIOLOGY
Basilic vein

ANATOMY AND PHYSIOLOGY
Cephalic vein

ANATOMY AND PHYSIOLOGY
dorsal veins of forearm

ANATOMY AND PHYSIOLOGY

ANATOMY AND PHYSIOLOGY
Medial cubital vein

ANATOMY AND PHYSIOLOGY
Medial cubital vein
Brachial artery

ANATOMY AND PHYSIOLOGY
Medial cubital vein
Brachial artery
Median Nerve

ANATOMY AND PHYSIOLOGY
Dorsal venous arch
Great Saphenous Vein
Femoral Vein

ANATOMY AND PHYSIOLOGY
Scalp Veins

…the new access site has to be proximal to the "blown" area to prevent extravasation of medications through the damaged vein…

…for this reason it is advisable to site the first cannula at the most distal site on the vein.

Interosseous Route The only alternative in emergency that is equally
reliable

ANATOMY AND PHYSIOLOGY

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.
ADVANTAGES• Fluids irritating to peripheral veins can
be given• Chemotherapy• Total parenteral nutrition
• Medications reach the heart
immediately, and are quickly distributed to the rest of the body.
• Central venous pressure can be
measured

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.
DISADVANTAGES
• Risks of bleeding, infection, air embolism.
• Technically difficult– • needs experienced clinician
knowing the appropriate landmarks and/or
• using an ultrasound probe to safely locate and enter the vein.
• Pleura and carotid artery are at risk of damage with the potential for pneumothorax or puncture/ cannulation of the artery.

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.
INTERNAL JUGULAR• Nursing care• Be cautious with potassium

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.
SUBCLAVIAN• Nursing care is easier• Open even in shock• Incompressible

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.
FEMORAL
• Emergency situations where it is difficult to cannulate Internal jugular vein or Subclavian vein
• High risk of infection
• Preferred for potassium infusions

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.

Central Venous Line Vs Pulmonary Artery Catheter

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.
Peripherally inserted central catheterADVANTAGES
• Safer to insert with a relatively low risk of uncontrollable bleeding no risks of damage to the lungs or major blood vessels.
• With proper hygiene, care, can be left in place for several weeks for patients who require extended treatment.
Some special types of

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.
Peripherally inserted central catheterDISADVANTAGES
• Must travel through a relatively small peripheral vein which can take a less predictable course on the way to the superior vena cava . Hence, more technically difficult to place in some patients.
• Travels through the axilla.
Hence, can become kinked causing poor function.
Some special types of

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.
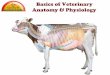
Tunneled LinesHickman line or Broviac catheter
• “Tunneled" under the skin to emerge a short distance away. from the central vein
• Reduced risk of infection, since bacteria from the skin surface are not able to travel directly into the vein;
• Catheters are also made of materials that resist infection and clotting.
A Hickman line in a leukemia patient.
It is tunneled under the skin to the jugular vein
Some special types of

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.
Implantable ports• Silicone rubber reservoir, implanted
under the skin. • Medication is injected via its silicone
cover, into the reservoir. • The cover can accept several
hundreds of needle sticks during its lifetime. It is possible to leave the ports in the patient's body for years.
Some special types of

Central Venous LinesCentral Lines flow through a catheter with its tip
within a large vein, usually the superior vena cava or inferior vena cava, or within
the right atrium of the heart.
Implantable ports
• Needs regular maintenance. If it is plugged a thrombus can form with the accompanying risk of embolisation
• Commonly used for patients on long-term intermittent treatment.
Some special types of

IV Fluids
• Colloids

IV Fluids
• Crystalloids

IV Fluids
• Colloids
• Contain larger insoluble molecules, such as albumen.
• Preserve a high colloid osmotic pressure in the blood
• Blood itself is a colloid.

IV Fluids
• Colloids

IV Fluids
• Crystalloids
• Aqueous solutions of water-soluble molecules.
• The most commonly used crystalloid fluid is normal saline=, a solution of sodium chloride at 0.9% concentration, which is close to the concentration in the blood (isotonic).
• What is isotonic? • What is Iso-osmolar ?

IV Fluids
• Crystalloids

IV Fluids
• Crystalloids

IV Fluids
• Crystalloids
• Fluid of choice in multiple situations• Trauma• Metabolic alkalosis
• Not to be given in hyperchloremic acidosis
isotonic

IV Fluids
• Crystalloids
hypotonic

IV Fluids
• Crystalloids
? Isotonic/ Hypotonic
• Isotonic in vitro• Hypotonic in vivo
• Iso-osmolar , compared to Normal Saline • Hypotonic to the human cells due to Insulin
• Hypertonic in insulin deficiency

IV Fluids
• Crystalloids
? Isotonic/ Hypertonic ?

IV Fluids
• Crystalloids
Contains calcium, potassium and Lactate
• Don’t give in alkalosis• Don’t give in hyperkalemia• Don’t give with Blood• Mind its Calcium content, when
giving with Mg therapy
Nearly Isotonic

• Don’t give potassium therapy with Dextrose containing solutions
IV Fluids
• Crystalloids
• When giving Dextrose containing solutions, add KCl to prevent hypokalemia
• When giving KCl in the treatment of hypokalemia, don’t add it to solutions containing Dextrose.

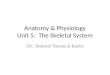
Distribution of fluid in human body
Colloids stay here
Crystalloids move up to
here

Risks and complications of IV THERAPY
1. Infection2. Phlebitis3. Infiltration and extravasation4. Embolism5. Fluid overload6. Electrolyte Imbalance

Electrolytes
• Sodium 135 – 145 mmol/L
• Potassium 3.5 – 5.0 mmol/L
• Calcium 2.12 – 2.75 mmol/L ( Ionised calcium 1.0-1.3 mmol/L) • Magnesium 1.5 – 2.2 m Eq/L
• Phosphorous 0.81 – 1.20 mmol/L

Electrolytes
• Sodium 135 – 145 mmol/L
• Potassium 3.5 – 5.0 mmol/L
• Calcium 2.12 – 2.75 mmol/L • Magnesium 1.5 – 2.2 m Eq/L
• Phosphorous 0.81 – 1.20 mmol/L
Low sodium – lower osmolality
High sodium – higher osmolality

• Sodium 135 – 145 mmol/L
• Potassium 3.5 – 5.0 mmol/L
• Calcium 2.12 – 2.75 mmol/L ( Ionised calcium 1.0-1.3 mmol/L) • Magnesium 1.5 – 2.2 m Eq/L
• Phosphorous 0.81 – 1.20 mmol/L
Electrolytes
Hypokalemia
Hyperkalemia

Hyperkalemia
• Sodium 135 – 145 mmol/L
• Potassium 3.5 – 5.0 mmol/L
• Calcium 2.12 – 2.75 mmol/L ( Ionised calcium 1.0-1.3 mmol/L) • Magnesium 1.5 – 2.2 m Eq/L
• Phosphorous 0.81 – 1.20 mmol/L
BE GOOD IN CLINICALSKILLS
KEEPDRUGSAWAY
• Bicarbonate• Glucose +• Insulin• Calcium• Sorbitol
• Keyexalate• Dialysis• Albuterol
ACLS - 2006

Electrolytes
• Sodium 135 – 145 mmol/L
• Potassium 3.5 – 5.0 mmol/L
• Calcium 2.12 – 2.75 mmol/L ( Ionised calcium 1.0-1.3 mmol/L) • Magnesium 1.5 – 2.2 m Eq/L
• Phosphorous 0.81 – 1.20 mmol/L

THANK YOURAVINDAR BETHI