Embed Size (px)
Citation preview

www.kidney-international.org r ev i ew
Renal perfusion in sepsis: from macro- tomicrocirculation
Emiel Hendrik Post1, John A. Kellum2, Rinaldo Bellomo3 and Jean-Louis Vincent11Department of Intensive Care, Erasme University Hospital, Université Libre de Bruxelles, Brussels, Belgium; 2Center for Critical CareNephrology, Department of Critical Care Medicine, University of Pittsburgh, Pittsburgh, Pennsylvania, USA; and 3Centre for IntegratedCritical Care, School of Medicine, The University of Melbourne, Parkville, Melbourne, Australia
The pathogenesis of sepsis-associated acute kidney injuryis complex and likely involves perfusion alterations, adysregulated inflammatory response, and bioenergeticderangements. Although global renal hypoperfusion hasbeen the main target of therapeutic interventions, its rolein the development of renal dysfunction in sepsis iscontroversial. The implications of renal hypoperfusionduring sepsis probably extend beyond a simple decrease inglomerular filtration pressure, and targeting microvascularperfusion deficits to maintain tubular epithelial integrityand function may be equally important. In this review, weprovide an overview of macro- and microcirculatorydysfunction in experimental and clinical sepsis and discussrelationships with kidney oxygenation, metabolism,inflammation, and function.Kidney International (2016) -, -–-; http://dx.doi.org/10.1016/
j.kint.2016.07.032
KEYWORDS: acute kidney injury; renal hypoperfusion; sepsis
Copyright ª 2016, International Society of Nephrology. Published by
Elsevier Inc. All rights reserved.
Correspondence: Jean-Louis Vincent, Department of Intensive Care, ErasmeHospital, Route de Lennik 808, 1070 Anderlecht, Belgium. E-mail: [email protected]
Received 13 May 2016; revised 1 July 2016; accepted 7 July 2016
Kidney International (2016) -, -–-
S epsis is considered a dysregulated host response to asevere infection.1 This immune response can causepronounced systemic hypotension, which has led to
formulation of a hypothesis of ischemic acute kidney injury inseptic shock.2,3 Indeed, in the case of suspected compromisedtissue perfusion, early restoration of organ perfusion pressureis of paramount importance, yet patients can still die frommultiorgan failure even when blood pressure has beenadequately restored.4 Thus, perfusion alterations are morelikely to be of microcirculatory origin, a phenomenon thathas been observed in virtually every organ, including thekidney. In this article, we review the role of hemodynamics inthe development of renal dysfunction during sepsis, fromwhole-organ renal blood flow (RBF) to the microcirculationand even beyond.
Renal blood flow in sepsisExperimental studies. The behavior of whole-organ RBF
during sepsis and septic shock remains a subject of contro-versy. Models of renal ischemia using total renal arterial stop-flow do not accurately reproduce the clinical scenario of sepsis,and the literature on experimental sepsis and infusion oflipopolysaccharide or live bacteria shows marked heter-eogeneity (Table 1).5 For example, in a sheep model of infu-sion of live bacteria, Di Giantomasso et al. reported that sepsiswas associated with increased RBF.6 In the same model,Langenberg and colleagues demonstrated that this renal hy-peremia did not prevent renal dysfunction.7 By contrast, Beneset al. demonstrated in 2 different pig models of septic shockthat renal vascular resistance increased in animals with renaldysfunction.8 This renal vasoconstrictive response occurred inthe presence of vasodilation in other parts of the body, sug-gesting blood flow redistribution. Indeed, systemic flowredistribution has been observed in a number of animalmodels of sepsis and septic shock,9,10 and may be caused byseveral factors, including increased renal sympathetic nerveactivity (RSNA) and the release of vasoactive molecules, suchas angiotensin II,11 endothelin-1, thromboxane A2, and leu-kotrienes.12–14 The intrinsic properties of renal autoregulationalso comply with the concept of flow redistribution. In health,RBF is autoregulated at renal perfusion pressures (RPP)greater than approximately 60–100 mm Hg, depending onthe species.15–17 This value is higher than for the heart18 andthe brain,19 and allows a rapid reduction in RBF in case ofhypovolemia, thus retaining circulating blood volume and
1

Table 1 | Experimental studies of renal perfusion in sepsis
First author, year Species Model Fluid and vasopressors Intervention Observation Key findings
Ravikant, 197782 Pig i.m. P. multicoda Balanced solution,titrated to MAP
- 24 h RBF, cortical and medullaryflow increased at
24 h. No intrarenal redistribution.Cronenwett, 197884 Dog i.v. P. aeruginosa - - 60 min RBF maintained,
intrarenal flowredistribution toward thecorticomedullary junction.
Stone, 197983 Dog Septic bloodtransfusion
NaCl 0.45%, 2 ml/min - 60 min RBF increased,intrarenal redistrubtiontoward the outer cortex.
Auguste, 198085 Dog E. coli perfusate NA - 75 min RBF unchanged,no signs of intrarenalflow redistribution.
Gullichsen, 1991146 Dog i.v. LPS - - 4 h RBF decreased, renal VO2
and cortical tPO2 initiallydecreased, restored thereafter.
Lactate uptake andglucose consumption unchanged.
Weber, 1992151 Sheep i.v. LPS Ringer’s lactate, 50 ml/h - 72 h RBF decreased, partially restoredafter 24 h. Renal VO2 reduced,restoration after 24 h. TNaþ/VO2
persistently reduced.Bersten, 199550 Sheep i.p. E. coli and B.
fragillis- Epinephrine, DA 4 h RBF increased with
DA in healthy animals.Effect attenuated in sepsis.
Heemskerk, 1997153 Rat i.v. LPS and E. colia - - 3 h RBF decreased, renalVO2 unchanged, VO2/TNa
þ
increased.Cohen, 200188 Pig i.v. LPS NaCl 0.9%, titrated to PAOP L-NAME, SMT 6 h RBF increased, intrarenal redistribution
towards medulla. L-NAME and SMTboth decreased RBF, cortical
and medullary flow,redistribution unchanged.
Di Giantomasso,20036
Sheep i.v. E. coli Unknown, 2 ml/kg/hand gelofusine boluses
titrated to CVP
NE 30 min RBF increased, no clearredistribution. NE administration
increased RBF further and augmentedmedullary flow.
Albert, 200441 Rabbit i.v. LPS NaCl 0.9%, 4 ml/kg/h AVP 90 min With increasing dose: increaseddiastolic RBF velocity, increased cortical
flow, minor increasemedullary flow. Cortical flow values
depressed at highest dose.Boffa, 200414 Mouse i.p. LPS NaCl 0.9%, 10 ml/kg at baseline TXA2-R k/o,TXA2
antagonist14 h RBF decrease attenuated in
TXA2-R k/o andTXA2-antagonist treated mice.
Boffa, 200542 Mouse i.p. LPS NaCl 0.9%, 10 ml/kg at baseline NE, Ang II, L-NAME, AVP 3 h RBF decreased furtherwith Ang II and L-NAME,
but was largelyunaffected by NE and AVP.
revie
wEH
Postet
al.:Renalmacro-
andmicrocirculation
insep
sis
2Kid
ney
Intern
atio
nal(2016)-,-–-

GFR changed inthe same direction.
Faivre, 200589 Rabbit i.v. LPS - Levosimendan, AVP, NE 36 h No effect on RBF, corticalor medullary flow with
levosimendanalone. NE alone increased, and AVP,
with or without levosimendan, depressed,medullary flow.
Tiwari, 2005113 Mouse i.p. LPS - L-NIL, Z-VAD 24 h L-NIL and Z-VAD improvedperitubular capillary flow
impairment, cortical injury, renalapoptosis, plasma creatinine
and BUN after 18 h.Langenberg, 20067 Sheep i.v. E. coli NaCl 0.9%, 1 ml/kg/h - 48 h RBF increased, creatinine
clearance and UO reduced.Johannes, 2006133 Rat i.v. LPS NA HES130/0.4, HES200/0.5,
Ringer’s lactate90 min Decrease in RBF, VO2 maintained,
VO2/TNaþ increased,
cortical and medullary mPO2
minimally affected. RBF partiallyrestored by all fluids,
oxygenation differentially affected.Yasuda, 2006130 Mouse CLP NaCl 0.9%, 1.5 ml at
6 and 12 hSimvastatin 24 h Interstitial edema at 6 h in control
group. Edema, capillary flowimpairment and tubularhypoxia attenuated after
pretreatment with simvastatin.Wu, 2006114 Mouse i.p. LPS NaCl 0.9%, 1 ml after CLP, 1ml
after 6 hL-NIL 24 h L-NIL attenuated peritubular
capillary flow impairment,tubular epithelial ROS/RNS generation
and tubular injury.Wu, 200697 Mouse i.p. LPS - - 48 h Peritubular capillary flow
impairment from 2 h onward,significant spatial correlation between
peritubular flow impairment andtubular epithelial redox-alterations.
Gupta, 2007139 Rat i.p. LPS - APC 24 h Peritubular capillary flow impairmentat 3 h improved with APC, improved
BUN at 24 h.Wu, 2007115 Mouse CLP NaCl 0.9%, 1 ml after
CLP, 1.5 mlafter 6 h
L-NIL 22 h L-NIL attenuated peritubular capillaryflow impairment and tubular injury.
Chvojka, 200899 Pig Peritonitis HES 130/0.4, 10 ml/kg/h,NE if shock
- 22 h RBF and renal VO2 maintained,cortical flow decreased andrenal vein L/P ratio increased
from 12 h onward.Fenhammar, 2008138 Pig i.v. LPS NaCl 0.9%, 20 ml/kg/h Tezosentan 5 h Attenuation of the decrease
in RBF and cortical flowwith tezosentan.
Wan, 200946 Sheep i.v. E. coli - Ang II 8 h RBF decreased withAng II but increased UOand creatinine clearance.
(Continued on next page)
EHPost
etal.:Renal
macro-
andmicrocirculation
insep
sisre
vie
w
Kidney
Intern
atio
nal(2016)-,-–-
3

Table 1 | (Continued)
First author, year Species Model Fluid and vasopressors Intervention Observation Key findings
Johannes, 2009117 Rat i.v. LPS HES 130/0.4, 5 ml/kg/h DXM supplemented fluid 5 h RBF and cortical mPO2
decrease further attenuated withdexamethasone suppletion, renal VO2
normalized.Johannes, 2009118 Rat i.v. LPS HES 130/0.4, 5 ml/kg/h NTG, 1400W 5 h RBF decreased, renal
VO2, cortical and outer medullamPO2 decreased.
Unaffected by NO donationor iNOS-inhibition.
Johannes, 2009154 Rat i.v. LPS HES 130/0.4, 5 ml/kg/h Flow reduction healthy rats 60 min Flow reduction in healthdecreased renal VO2 without
signs of microcirculatory hypoxia.Microcirculatory hypoxia in
septic controls partially alleviatedby fluid resuscitation.
Johannes, 2009136 Rat i.v. LPS HES 130/0.4, 5 ml/kg/h Iloprost 5 h RBF decrease unaffected. RenalVO2 and VO2/TNa
þ
restored. Cortical andmedullary mPO2 increased:
increased oxygenextraction by improvedmicrovascular function.
Benes, 20118 Pig i.v. P. aeruginosa andperitonitisa
HES 130/0.4, titrated to CVPand PAOP, NE if shock
- 22 h RBF decreased andRVR increased in
septic animals with,but not without, AKI.
Dyson, 2011152 Rat i.v. LPS Ringer’s lactate, 20 ml/kg/h - 4 h RBF decreased. Renal VO2
unchanged. Cortical and outermedulla mPO2 decreased and interstitial
PO2 in cortex and medulladecreased: gradient unchanged.
Legrand, 2011100 Rat i.v. LPS NA HES 130/0.4 from baseline,2-hour delay
5 h Late correction of RBFdid not affect corticalmicrovascular perfusion
and mPO2.Seely, 201198 Rat CLP NaCl 0.9%, 1 ml after
CLP, 1.5 mlafter 6 h
- 22 h RBF decreased after 2 h,perivascular perfusiondeficits followed at
6 hours, signs of capillaryleakage present after 10 h.
Aksu, 2012134 Rat i.v. LPS NA HES-RA, HES-NaCl 4-5 h HES-RA, but not HES-NaCl,attenuated the decrease in RBF
and cortical microvascular perfusion.Increased cortical flow heterogeneity
attenuated by both.Holthoff, 2012116 Mouse CLP NaCl 0.9%, 1 ml after CLP,
40 ml/kg after 6Resveratrol 18 h RBF decrease attenuated, perivascular
perfusion deficits attenuated, tubularepithelial RNS formation andtubular injury attenuated.
revie
wEH
Postet
al.:Renalmacro-
andmicrocirculation
insep
sis
4Kid
ney
Intern
atio
nal(2016)-,-–-

Ishikawa, 201144 Sheep i.v. E. coli NaCl 0.8%, 1 ml/kg/h Intrarenal L-NAME 8 h RBF increase attenuated inboth mild sepsis and
septic shock, renal functionnot affected in both groups.
Ishikawa, 201245 Sheep i.v. E. coli NaCl 0.9%, 1 ml/kg/h Intrarenal 1400W,AG and L-NAME
8 h RBF increase attenuated andUO increased with L-NAME, no
effect on creatinine clearance fromany of the three NOS inhibitors.
Ishikawa, 201243 Sheep i.v. E. coli NaCl 0.9%, 1 ml/kg/h Terlipressin single andmultiple dose
6 h RBF increase attenuatedwith single-dose terlipressin. Increased
UO and creatinine clearance. Attenuated effecton creatinine clearance with multiple doses.
Wang, 2012120 Mouse CLP NaCl 0.9%, 1 ml after CLP,40 ml/kg after 6 h
MnTMPyP 18 h RBF decreased, interstitialedema evident at 2 h,
capillary flow impairment after4 h. Only delayed MnTMPyPimproved capillary leakageand capillary dysfunction.
Almac, 2013140 Rat i.v. LPS HES 130/0.4, 5ml/kg/h low and high dose APC 3 h RBF and cortical andmedullary mPO2 unaffected.
TNaþ/VO2 improved with APC.Holthoff, 2013137 Mouse CLP NaCl 0.9%, 1 ml after CLP,
1.5 ml after 6 hRolipram 18 h RBF decrease, perivascular
capillary leakage, peritubularcapillary dysfunction, tubular
hypoxia and injury attenuated withdelayed rolipram. RNS generation
unaffected.Burban, 201323 Rat CLP Gelatin 4% after CLP,
titrated to MAPMAP reductions by
acute bleeding5–6 h RBF decreased by NE.
Renal autoregulation unchanged insepsis, with or without NE.
Patil, 2014121 Mouse CLP NaCl 0.9%, 1 ml after CLP MitoTEMPO 24 h MitoTEMPO reduced mitochondrialoxygen radical production and
improved mitochondrial function.Peritubular capillary dysfunction attenuated.
Yang, 2014145 Dog i.v. LPS NaCl 0.9%, 4.3 ml/kg/h, titrated toCVP and PAOP
- 6 h Renal DO2 maintained,renal VO2 decreased,
renal ATP levels decreased.Calzavacca, 201587 Sheep i.v. E. coli NaCl 0.9%, 1 ml/kg/h - 72 h RBF increased, cortical
flow maintained, medullaryperfusion and medullary tPO2
decreased.Wang, 2015132 Mouse CLP NaCl 0.9%, 1 ml after CLP,
1.5 ml after 6 hS1P1-agonist 18 h Pretreatment with S1P1-agonist
reduced signs of capillaryleakage but did not preventearly capillary hypoperfusion.
Delayed treatment improved both.Ergin, 2016135 Rat i.v. LPS NA HES-RA, AQIX, NaCl 0.9% 7 h RBF decrease attenuated
with HES-RA, but not withAQIX or NaCl, cortical and medullary
(Continued on next page)
EHPost
etal.:Renal
macro-
andmicrocirculation
insep
sisre
vie
w
Kidney
Intern
atio
nal(2016)-,-–-
5

Table
1|(Continued
)
Firstau
thor,y
ear
Species
Mod
elFluidan
dvasopressors
Interven
tion
Observation
Key
find
ings
mPO2unaffected
.HES
may
have
increasedrenal
oxidativestress.
Lankadeva,20
1690
Shee
pi.v.E.coli
NaC
l0.9%
,1ml/kg
/hNE
32h
RBFunchan
ged
withNE.
Cortical
oxygen
ationunaffected
,med
ullary
flow
and
tPO2decreased
withNE.
Maiden
,201
6143
Shee
pi.v.E.coli
NaC
l0.9%
,3ml/kg
/h,N
EifMAP
<75
mm
Hg
-48
hRB
Fmaintained
,minim
alsignsof
renal
injury
onlig
htan
delectronmicroscopy.
1400
W,selective
iNOSinhibitor;AG,aminoguan
idine(partiallyselectiveiNOSinihibitor);A
KI,acute
kidney
injury;A
ngII,an
giotensinII;APC
,activated
protein
C;A
QIX,fully
balan
cedcrystalloid
solution;A
VP,
argininevasopressin;
BUN,b
loodureanitrogen
;CLP,cecallig
ationan
dpuncture;C
VP,centralvenouspressure;D
A,d
opam
ine;DXM,d
exam
ethasone;GFR
,glomerularfiltrationrate;H
ES,h
ydroxyethylstarch;H
ES-NaC
l,unbalan
cedHES
solution;H
ES-RA,
balan
ced
HES
solution;iNOS,
inducible
nitricoxidesynthase;
L/P,
lactate/pyruvate;L-NAME,
nonselectiveNOSinhibitor;
L-NIL,selectiveiNOSinhibitor;
LPS,
lipopolysaccharide;
MAP,
mean
arterial
pressure;MitoTEMPO
,mitochondria-targeted
antioxidan
t;MnTM
PyP,
superoxidescaven
ger;mP
O2,m
icrovascularPO
2;N
A,n
otap
plicab
le;N
E,norepinep
hrine;
NTG
,nitroglycerin;PA
OP,
pulm
onaryartery
balloon-occluded
pressure;RO
S/RN
S,reactive
oxygen
species/reactive
nitrogen
species;RV
R,renalvascularresistan
ce;S1P
1,sphingosine-1-phosphate-1;SM
T,selectiveiNOSinhibitor;Tn
aþ,sodium
reab
sorption;tPO
2,tissuePO
2;TXA2-R
k/o,thromboxaneA2receptorkn
ock-
out;UO,u
rineoutput;VO2,o
xygen
consumption;Z-VAD,nonselectivecaspaseinhibitor.
aTw
omodels.
r ev i ew EH Post et al.: Renal macro- and microcirculation in sepsis
6
diverting blood toward more vital organs.20 The situation insepsis is, however, less clear. Bellomo et al. studied renalpassive pressure-flow relationships in dogs and foundthat ohmic renal resistance decreased after approximately45 minutes of endotoxemia.21 However, these measurementswere taken using a 5-second time frame, which is too shortfor the full renal autoregulatory response to occur.22
Burban et al. investigated renal autoregulation in a rodentmodel of abdominal sepsis by bleeding the animals to reduceRPP.23 They found that early sepsis did not alter the rela-tionship between RBF and mean arterial pressure (MAP).However, blood loss can shift the lower autoregulatorythreshold to higher pressures, which may have confoundedtheir results.24
Clinical studies. Measurement of RBF at the bedside ischallenging, and the available data in human sepsis arelimited and often unreliable. Most studies have reported adecrease in RBF in human sepsis.25–27 Brenner et al. used athermodilution technique to measure RBF in 6 patients withseptic shock, 5 of whom had low to normal RBF. RelativeRBF, or the fraction of cardiac output directed to the kidneys,was reduced in all patients and correlated well with theglomerular filtration rate (GFR).28 Redfors et al. measuredRBF using retrograde thermodilution in 12 patients who haddeveloped vasodilatory shock after cardiac surgery and alsofound low to normal RBF in all.29 Using renal Doppler atintensive care unit (ICU) admission in 34 patients with septicshock, Lerolle et al. found that the renal resistive index washigher in patients who later developed acute kidney injury(AKI),30 although indices derived from renal Doppler mea-surements may poorly reflect actual changes in renal hemo-dynamics.31 Prowle et al. reported a consistent reduction inrelative RBF estimated by phase-contrast magnetic resonanceimaging in 10 patients with sepsis and fully established AKI.32
However, absolute RBF did not correlate with GFR, andwhether alterations in renal resistive index or RBF are thecause or consequence of AKI, or even just an epiphenom-enon, remains unclear.
Systemic hemodynamics, RBF, and kidney functionObservational clinical studies. Many observational clinical
studies have reported significant associations between sys-temic hemodynamic instability and renal dysfunction inseptic shock (Table 2). In septic shock patients treated withnorepinephrine, Martin et al. showed that adequate restora-tion of MAP was associated with restored urine output andimproved creatinine clearance.33 In 274 patients with sepsis,Dünser et al. found an association between the time spentwith an MAP of less than 60 mm Hg during the first 24 hoursof ICU stay and lower urine output, higher maximum plasmacreatinine and increased need for renal replacement therapy.34
Badin et al. also demonstrated that patients with septic shockhad a lower MAP during the first 12 hours of ICU stay whenAKI was present at 72 hours than when it was not.35 Similarly,the FINNAKI trial found an association between the timespent in relative hypotension and the development of AKI in
Kidney International (2016) -, -–-

Table 2 | Clinical observational studies of MAP and renal function in sepsis
First author, year Design Patients Number Key findings
Brenner, 199028 Prospective descriptive Septic shock 6 Decreased RBF during shock, depressedRBF/CO that correlated well with GFR.
Martin, 199033 Retrospective cohort Septic shock treated with NE 24 Mean MAP from 52 to 89 mm Hg. UO restoredat 3 h after start NE, creatinine clearance after 48 h.
Lerolle, 200630 Prospective cohort Septic shock 34 Early increase in RRI in patients with AKI after 5 d.Dünser, 200934 Retrospective cohort Sepsis and septic shock 274 Correlation hourly time integral of MAP and need
for RRT, maximum plasma creatinine and UO.Badin, 201135 Prospective cohort Shock 217 Time-averaged MAP between 72-82 mm Hg associated
with higher incidence of AKI in septic shock withinitial renal insult. Not in other shock types.
Prowle, 201232 Prospective descriptive Septic AKI 10 Mostly reduced RBF, consistently reducedRBF/CO in all patients.
Poukkanen, 201336 Retrospective cohort Sepsis 423 Association between time spent in relative hypotensionduring first 24 h of shock and development of AKI.
Legrand, 201337 Retrospective cohort Sepsis 137 Association between low mean DAP and high CVPover the first 24 h of ICU stay and the occurrence
of new or persistent AKI.Wong, 201538 Retrospective cohort Septic shock 107 Greater mean perfusion pressure deficit, mostly
due to increased CVP, in patients with AKI.
AKI, acute kidney injury; CO, cardiac output; CVP, central venous pressure; DAP, diastolic arterial pressure; GFR, glomerular filtration rate; MAP, mean arterial pressure; NE,norepinephrine; RBF, renal blood flow; RRI, renal resistive index; RRT, renal replacement therapy; UO, urine output.
EH Post et al.: Renal macro- and microcirculation in sepsis r ev i ew
patients with sepsis.36 In a retrospective study of 137 patientswith sepsis, lower mean diastolic arterial pressures over thefirst 24 hours following ICU admission were associated withan increased risk of developing AKI.37 However, the degree ofhypotension may simply be a marker of disease severity, andsome studies did not report an independent association ofMAP or mean perfusion pressure with AKI.37,38 Moreover,AKI is also common in less severe sepsis. For example, inpatients hospitalized for community-acquired pneumonia,Murugan and colleagues found that AKI occurred in morethan one-third of patients despite the fact that only 16% wereadmitted to the ICU and fewer than 10% requiredvasopressors.39
Interventional experimental studies. Most experimentalstudies have suggested an attenuation of renal dysfunctionwith the administration of vasopressors in septic shock(Table 1).40–43 However, attempts to increase RBF indepen-dently from RPP have not always been effective. For example,when Ishikawa et al. infused a nonspecific nitric oxide syn-thase inhibitor into the renal artery of septic sheep, the in-crease in RBF was attenuated but renal function did notimprove.44 In the same model, intrarenal infusion of a specificinducible nitric oxide synthase (iNOS) inhibitor failed toinfluence RBF or kidney function.45 On the other hand, theeffect of angiotensin II infusion on urine output and creati-nine clearance in a sheep model of hyperdynamic sepsis wasstriking.46 The use of dopamine has long been advocated topreserve RBF and prevent AKI in critical illness, includingsepsis. Several experimental studies showed an increase inRBF and attenuation of renal dysfunction with dopamine inendotoxemia,47–49 but others did not.50 Recent work by ourgroup showed that the selective dopamine-1 receptor agonist,fenoldopam, was ineffective at preserving RBF in a sheepmodel of septic shock.51
Kidney International (2016) -, -–-
Interventional clinical studies. Several small, nonblinded,interventional studies in human septic shock have reporteda beneficial effect on urine output52–54 and creatinineclearance55–57 when using norepinephrine to increase RPP(Table 3). Other vasopressors, such as vasopressin or terli-pressin, appear equally effective in improving urine outputand creatinine clearance.58–63 However, the effects ofincreasing MAP to levels greater than 60–65 mm Hg are lessclear. Deruddre and colleagues observed that increasingMAP from 65 to 75 mm Hg improved urine output, butincreasing MAP to levels greater than 85 mm Hg yielded nofurther benefit.64 Several other studies have failed to showany beneficial effect of increasing RPP to levels greater than65 mm Hg.65–67 The randomized, controlled SEPSISPAMtrial, which included 776 patients with septic shock, showedno overall effect on renal function or the need for renalreplacement therapy of increasing MAP to 80–85 mm Hgcompared to a target of 70–75 mm Hg.68 There was, how-ever, a notable exception in a predefined subpopulation ofpatients with chronic arterial hypertension, in whom ahigher MAP resulted in lower plasma creatinine levels and areduced need for renal replacement therapy. Chronic arte-rial hypertension is associated with compromised renalautoregulation, which could explain the altered relationbetween hemodynamics and renal function in thesepatients.69
The use of fluids to improve renal perfusion in sepsis issurrounded by similar controversy.70 Intravascular fluidadministration may be counterproductive once intravascularvolume has been restored, because fluid overload can furtherinjure the kidney.71 Saline, in particular, may compromiserenal perfusion and worsen AKI through a chloride-inducedincrease in renal vascular resistance.72,73 Indeed, in the Pro-tocolized Care for Early Septic Shock (ProCESS) trial,
7

Table 3 | Clinical interventional studies of MAP and renal hemodynamics in sepsis
First author, year Design Patients Number (int/ctrl) Baseline MAP Intervention Key findings
Desjars, 198752 Open-label, nonrandomized,uncontrolled
Hyperdynamicseptic shock
12 / – 48 � 11/ – NE, 0.5 and 1.0 mg/kg/m Mean MAP to 59 and 78 mm Hg.Increased UO with NE infusion.
Hesselvik, 198953 Open-label, nonrandomized,uncontrolled
Hyperdynamicseptic shock
5 / – 50 � 4 / – NE, 0.03–0.5 mg/kg/mintitrated to SAP at100–140 mm Hg
Mean MAP to 69 mm Hg.Average UO over 3 h
during NE infusion increasedin all patients.
Desjars, 198955 Open-label, nonrandomized,uncontrolled
Septic shock 25 / – 54 � 10 / – NE, 0.5–1.5 mg/kg/min Mean MAP to 80 mm Hg.Creatinine clearance showed
persistent improvement duringNE-infusion.
Martin, 199354 Double-blinded, randomized,controlled
Hyperdynamicseptic shock
16 / 16 54 � 10 / 53 � 8 NE, 0.5–5 mg/kg/minand DA, 10–25 mg/kg/m
Mean MAP to 91 mm Hg.Oliguria resolved with NE. Similar
results in DA-responders(approximately one-half of patients).
Redl-Wenzl, 199357 Open-label, nonrandomized,uncontrolled
Septic shock 56 / – 56 � 4 / – NE, 0.1–2.0 mg/kg/min Mean MAP to 82 mm Hg.Mean creatinine clearance from
75 to 102 ml/min after 48 h of NE therapy.Lherm, 199675 Open-label, nonrandomized,
sequentialSepsis andseptic shock
14 / 15a 81 � 20 / 78 � 10 DA infusion, 2.0 mg/kg/m Increased diuresis and creatinineclearance in septic patients without shock.
Juste, 199877 Open-label, nonrandomized,sequential
Septic shock 17 / – 90 � 12 / – DA, 2.5 mg/kg/min Important inotropic effect, increasedurine volume, no effecton creatinine clearance.
Day, 200078 Open-label, nonrandomized,uncontrolled
Severe sepsis 5 / – 91 (67-150) / –d DA, 2.5–10 mg/kg/min Increased RBF with low,but not high, dose DA.
No effect on creatinine clearance or UOat any dose.
LeDoux, 200065 Open-label, nonrandomized,uncontrolled
Septic shock 10 / – 65 � 1 / – NE, titrated to MAP of65, 75, and 85 mm H
No effect on mean UO at eitherpressure level.
Leone, 200459 Open-label, nonrandomized,uncontrolled
Septic shock,unresponsiveto NE and DA
17 / – 54 � 4 / – terlipressin Mean MAP to 69 mm Hgafter 2 h, maintained for 24 h.
UO and creatinine clearance increased.Albanèse, 200456 Open-label, nonrandomized,
controlledSeptic shock 14 / 12 51 � 3 / 81 � 7 NE, titrated to MAP of
70 mm HgImproved UO and creatinine clearance.
Albanèse, 200560 Open-label, randomized,controlled
Septic shock 10 / 10 54 (49–61) / 54 (48–62) NE, terlipressin Mean MAP to 70 mm Hgwith both NE and terlipressin.
UO and creatinine clearance improvedwith both.
Bourgoin, 200566 Open-label, randomized,controlled
Septic shock 14 / 14 65 (62–68) / 66 (62–67) NE, titrated to MAP of65 or 80 mm Hg
MAP at 85 mm Hg did notaffect UO or creatinine clearance.
Morelli, 200576 Double-blinded, randomized,controlled
Sepsis 150 / 150 78 � 11 / 75 � 10 Fenoldopam, 0.09 mg/kg/m Attenuation increase of plasma creatininein patients with sepsis.
Deruddre, 200764 Open-label, nonrandomized,sequential
Septic shock 11 / – – / –e NE, titrated to MAP of65, 75, and 85 mm H
Mean MAP to 75 mm Hgimproved UO and reduced RRI
but did not affect creatinine clearance.No effect at 85 mm Hg.
Morelli, 200962 Double-blinded, randomized,controlled
Septic shock 15 / 15 / 15b 54 � 3 / 53 � 4 / 53 � 6 NE, AVP, terlipressin Similar effect on MAP with all vasopressors.UO unchanged but attenuated rise
revie
wEH
Postet
al.:Renalmacro-
andmicrocirculation
insep
sis
8Kid
ney
Intern
atio
nal(2016)-,-–-
in
,
in
in
g
in
g

inplasm
acreatininewithAVPan
dterlipressin.
Redfors,2
0112
9Open
-label,ran
domized
,cross-over
Vasodilatory
shock
12/12
60�
3/–
NE,
titrated
toMAPof
75or90
mm
Hg
MeanMAPto
75mm
Hg
increasedrenal
DO2,improved
UO
andGFR
.Noeffect
at85
mm
Hg.
Asfar,2
0146
8Open
-label,ran
domized
,controlled
Septicshock
388/38
873
�14
/74
�15
NE,
titrated
toMAPof
65–70
or70
–85
mm
Hg
MeanMAPto
70-85mmHg
noeffect
onUO
orrenal
function.
Reducedinciden
ceofRR
Tan
dattenuated
increase
inplasm
acreatinine
inpatients
withpre-existen
tAHT.
Schneider,2
0146
7Open
-label,n
onrandomized
,uncontrolled
Shock
12c/–
–/–
eNE,
titrated
toMAPof
60–65
or80
–85
mm
Hg
Noeffect
onmeancortical
bloodvo
lume,
largeinter-individual
variab
ility.
AHT,arterialhyp
ertension;A
VP,argininevasopressin;D
A,d
opam
ine;DO2,oxygen
delivery;GFR
,glomerularfiltrationrate;M
AP,meanarterialpressure;N
E,norepinep
hrine;RR
I,renalresistiveindex;RRT
,ren
alreplacemen
ttherap
y;SA
P,systolic
arterial
pressure;UO,u
rineoutput.
aSepsis/septicshock.
bNE/AVP/Terlipressin.
c 10withsepticshock.
dSystolic
pressure.
eNovalues
reported
.
EH Post et al.: Renal macro- and microcirculation in sepsis r ev i ew
Kidney International (2016) -, -–-
protocol-based care in septic shock resulted in more aggres-sive fluid resuscitation but not better renal outcomes.74
Attempts to selectively target RBF in human sepsis havebeen largely unsuccessful. A small nonblinded study in pa-tients with normotensive sepsis and patients with septic shocksuggested a beneficial effect of dopamine infusion on renalfunction only in the normotensive group.75 Similarly, pro-phylactic administration of fenoldopam in 150 septic patientswithout shock attenuated the increase in plasma creatininethat was observed in the control group.76 However, the use ofdopamine was ineffective in 2 small open-label studies inseptic shock and severe sepsis and in 1 larger double-blind,randomized, placebo-controlled trial in patients with sys-temic inflammatory response syndrome.77–79
Intrarenal flow in sepsisAlthough whole-organ RBF can play a role in the developmentof renal dysfunction in sepsis, regional and microcirculatoryflows may be equally relevant. In healthy steady-state condi-tions, approximately 80%ofRBFflows through the renal cortexonly.80 Themedulla does not have a blood supply of its own andreceives about 20% of the cortical blood flow from juxtame-dullary efferent arterioles.81 The few studies available onintrarenal flow distribution during sepsis reported conflictingresults, ranging from increased cortical and medullary flowwithout any clear redistribution,82 to preferentially cortical83 ormedullary flow,84 to no signs of intrarenal flow alterations atall.85,86 Conversely, Calzavacca et al. recently showed in a sheepmodel of septic hyperemic renal dysfunction that reducedmedullary blood flow and oxygen tension preceded thedecrease in urine output and creatinine clearance.87
Studies of the effects of different drugs on intrarenal flowdistribution in sepsis show similar varying results. In endo-toxemic pigs, administration of a nonselective NOS-inhibitorand a selective iNOS-inhibitor worsened cortical flow andattenuated the increase in medullary flow that was observedin nontreated animals.88Albert et al. studied the use ofvasopressin on regional flow in rabbits treated with endotoxinand found that it attenuated the decrease in RBF andincreased cortical flow but left medullary perfusion largelyunaltered.41 Faivre and colleagues studied the effects of lev-osimendan, a calcium sensitizer with vasodilating effects, incombination with norepinephrine and arginine vasopressinon cortical and medullary flow in endotoxemic rabbits.89
Renal and regional blood flows were not affected by levosi-mendan. Administration of vasopressin, however, depressedmedullary flow, whereas norepinephrine increased it. Morerecently, Lankadeva et al. studied the use of norepinephrine inseptic hyperemic renal dysfunction. In this study, norepi-nephrine did not affect whole-organ RBF but diminishedmedullary flow and oxygen tension.90
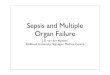
Predicting the consequences of altered intrarenal blood flowdistribution in sepsis is complex. The kidney’s unique vascularanatomical arrangement facilitates arterio-venous oxygenshunting, both diffusive 91 and convective (Figure 1).92 Thisarrangement possibly serves to maintain a stable renal tissue
9

O2
O2
O2
O2
O2
Diffusional shuntingpossibly adds to thedevelopment of medullaryhypoxia in sepsis. Alternatively,decreased shuntingeffectiveness may alsocause tubular injury throughincreased ROS production.
The presence of aperiglomerular circulationoffers an anatomicalpathway for convectionaloxygen shunting duringsepsis.
Figure 1 | Renal oxygen shunting. Enhanced renal oxygen shunting can lead to medullary hypoxia, and a reduction in shunting effectivenessmay also cause renal injury via an ROS-mediated pathway. Either way, a disturbance of the delicate intrarenal oxygen balance likely contributesto the development of renal dysfunction in sepsis and septic shock.
r ev i ew EH Post et al.: Renal macro- and microcirculation in sepsis
PO2 in the presence of variable RBF.93 However, it can alsocause low medullary tissue PO2 when shunting is enhanced,leading to a variable degree of tubular hypoxia. Alternatively, areduction in shunting effectiveness may also cause renal injuryvia an ROS-mediated pathway, a hypothesis that was proposedby O’Connor and colleagues.94 Either way, a disturbance of thedelicate intrarenal oxygen balance is likely to contribute to thedevelopment of renal dysfunction in sepsis and septic shock,although additional studies in this area are needed to elucidatethe exact mechanisms involved.
Renal microcirculation in sepsisMicrocirculatory alterations are also likely to contribute to thedevelopment of AKI in sepsis. Several processes take place inthe microcirculatory environment, including off-loading ofoxygen, delivery of nutrients to the tissues, and regulation offluid movement into the interstitium. Microcirculatoryalterations during sepsis are widespread and can be present invirtually every organ, including the heart, the gut, the liver,and the brain.95 These alterations consist of reduced overallmicrocirculatory flow and increased flow heterogeneity,resulting in increased oxygen diffusion distances and areas oftissue hypoxia. Furthermore, microcirculatory alterations canlead to increased leukocyte transit time through the kidney,possibly potentiating inflammation.96
A large body of data suggests that the renal microcirculationis similarly affected during sepsis. Using intravital video-microscopy in mice, Wu et al. demonstrated that the propor-tion of peritubular vessels showing normal, continuousflowwas significantly decreased after 2 hours of endotoxemia.97
In a pediatric rat cecal ligation and puncture (CLP) model, a
10
decrease in peritubularmicrovascular flowwas evidenced by anincreased proportion of capillary vessels showing sluggish or noflow.98 In a porcine model of severe sepsis, reduced microcir-culatory flow in the renal cortex occurred well before anychanges in RBF were observed.99 These alterations can persistevenwhen systemic hemodynamics are adequately corrected byfluid administration.100
The causes of microcirculatory flow alterations are incom-pletely understood, and a number of mechanisms have beenproposed (Figure 2). Inflammatory cytokines cause increasedexpression of adhesion molecules101 and increased leukocytetrafficking,102 resulting in microthrombi formation and capil-lary plugging.103 The up- and/or down-regulation of a numberof vasoactive compounds may cause a heterogeneous pattern oflocal vasodilation and constriction and areas of hypoxia.104
Additional pathways involve the production of reactive oxygenand nitrogen species, the formation of microparticles,105 andpossibly circulating histones.106Moreover, sepsis causes damageto the glycocalyx107 and disruption of the endothelial barrier,108
which results in capillary leakage and interstitial fluid seques-tration. Interstitial edema contributes to both increased oxygendiffusion distances and decreased microvascular flow.
Role of nitric oxideThe effects of iNOS on the renal microcirculation have beenstudied extensively.109 iNOS catalyzes the production of NOfrom L-arginine and is massively upregulated during sepsis.NO has vasodilatory properties and reacts with superoxide toform reactive nitrogen species. Renal iNOS expression duringsepsis most likely occurs in neutrophils and macrophages,110
in the endothelium111 and in renal tubular epithelial cells.112
Kidney International (2016) -, -–-

NADPH activation and eNOS uncouplingstimulate ROS formation. Upregulation ofiNOS in neutrophils and macrophages resultsin NO release and RNS production. Othermolecules affecting the renal microcirculationinclude: tezosentan, iloprost, rolipramand Z-VAD.
DXML-NIL
iNOS •NOL-arginineMitoTempo
RNS/ROSResveratrol
BH4
eNOS (uncoupled)
O2O2•
O2
NADPH NADP+H+
NADPH oxidase
Hypoxia and upregulation ofiNOS in tubular epithelial cellspromote ROS and RNS production.Signs of tubular injury include theloss of brush border, cast formation,vacuolization, and tubule dilation.Tubular cell swelling may furthercompromise microvascular flow.
Damage to the glycocalyx andrestructuring of junctional proteinsresults in increased capillarypermeability and edema formation,increasing oxygen diffusion distanceand compromising capillary flow.
Simvastatin 4F
eNOS Slit1/Robo4
VE-cadherinβ-catenin
p120
RNS/ROS
MnTMPyP
L-NIL
L-arginine
PO2O2•
•NO
MitoTempo
SEW2871
S1P1
+
+
+
+
Rac GTPase
Loss ofjunctionalintegrity
p120/β-catenin/VE-cadherin
iNOS
Figure 2 | Proposed pathways of renal microvascular dysfunction and tubular injury in sepsis. Compounds studied in the context ofrenal microcirculatory dysfunction in sepsis are marked in red. 4F, synthetic apoliprotein A-I analogue; BH4, tetrahydrobiopterin; DXM,dexamethasone; eNOS, endothelial NOS; iNOS, inducible nitric oxide synthase; L-NIL, selective iNOS inhibitor; p120/b-cadherin/VE-cadherin,adherens junction molecules; RNS/ROS, reactive nitrogen species/reactive oxygen species; S1P1, sphingosine-1-phosphate-1; Slit1/Robo4,junctional proteins; Z-VAD, nonselective caspase inhibitor.
EH Post et al.: Renal macro- and microcirculation in sepsis r ev i ew
Tiwari et al. were the first to report a significant increase inthe total number of perfused cortical peritubular vesselsfollowing the administration of an iNOS-inhibitor, L-NIL, in amouse model of endotoxemia.113 Wu and colleagues observedearly microcirculatory dysfunction and increases in plasma NOmetabolite levels in mice infused with lipopolysaccharide,97
which led them to investigate the temporal relationshipbetween iNOS up-regulation and kidney microcirculatorydysfunction in murine models of endotoxemia and poly-microbial sepsis.114,115 They not only found a temporalrelationship—capillary dysfunction and iNOS up-regulationboth occurred after 10 hours—but a spatial correlation aswell: low flow vessels were colocalized with tubular epithelialcells positively stained for reactive nitrogen species, such asperoxynitrite, and ROS.115 The administration of resveratrol,
Kidney International (2016) -, -–-
a peroxynitrite scavenger, improved peritubular microcircula-tory flow in a murine CLP model.116 Endotoxemic rats treatedwith fluids and low-dose dexamethasone showed lowercortical iNOS expression and increased microvascular PO2.
117
Conversely, when iNOS-inhibition was compared to NOdonation in a lipopolysaccharide-infused ratmodel, cortical andmedullary microvascular PO2 were similar in the 2 groups andunchanged compared to untreated controls.118
Reactive oxygen speciesNADPH oxidase is the most important source of superoxide,the precursor of most reactive oxygen species, in endothelialcells.119 In a mouse CLP model, administration of the super-oxide dismutase analogue MnTMPyP (a superoxide scavenger)resulted in an increased number of peritubular capillaries with
11

r ev i ew EH Post et al.: Renal macro- and microcirculation in sepsis
continuous flow after ROS production in the tubular epithe-lium was reduced to control levels.120 Patil et al. showed anearly beneficial effect of the mitochondria-targeted antioxidantMitoTEMPO (Enzo Life-Sciences, Farmingdale, NY) on therenal microcirculation in murine sepsis.121
Endothelial NOS (eNOS), which produces low amounts ofNO in physiological circumstances, becomes “uncoupled”during experimental sepsis (i.e., it switches to harmful super-oxide production, negatively affecting microvascular flow).122
Tetrahydrobiopterin (BH4) is an important cofactor for theproduction of NO by eNOS and its administration in an ovinemodel of septic shock resulted in improved systemic micro-circulation and organ function, including kidney function.123
Although eNOS deficiency was shown to increase susceptibil-ity to AKI in murine endotoxemia,124 it is unclear whether thiswasmediated through alterations in the renalmicrocirculation.
Capillary leakageSluggish or stopped blood flow is not the only feature ofmicrovascular dysfunction. Leakage from peritubular capil-laries and the resultant renal interstitial edema can be observedas early as two hours after the onset of sepsis.120 The underlyingmechanism is complex and in the case of the glomerularendotheliummost likely results from the increased number andaltered diameter of its fenestrae125,126 and from alterations inglycocalyx composition.127 To our knowledge, the specific ef-fects of sepsis on the endothelial barrier of peritubular vesselshave not yet been investigated. Nevertheless, the syntheticapoliprotein A-I analogue, 4F, did attenuate renal dysfunctionin a rat CLPmodel by restoring the expression of the junctionalproteins, Slit2 and Robo4, and increasing eNOS expression.128
Indeed, eNOS is also involved in the regulation of endothelialpermeability.129 Yasuda et al. showed that the administration ofsimvastatin attenuated kidney dysfunction and renal vascularleakage in a mouse model of abdominal sepsis, possibly viaaltered eNOS-regulation.130 Sphingosine-1-phosphate-1 isanother important regulator of endothelial integrity.131
Recently, Wang et al. found that treatment with a sphingo-sine-1-phosphate-1 agonist, even at 6 hours after induction ofsepsis, enhanced the endothelial permeability barrier, leadingto reduced perivascular leakage and improved peritubularmicrovascular flow.132
Fluids and the renal microcirculationFluids in septic shock are mainly considered a means toimprove RPP and whole-organ RBF, but they have been studiedin the context of renal microcirculation as well. Johannes et al.compared the use of 2 hydroxyethyl starch (HES) solutionswithdifferent molecular weights to Ringer’s lactate in a rat model ofendotoxemia and found that all fluid types increased RBF.133
However, despite the absence of increased renal oxygen con-sumption with high molecular weight HES, renal microvas-cular PO2 remained unaffected in all groups. In the samemodel, Aksu et al. compared HES dissolved in Ringer’s acetate,or balanced HES, with HES dissolved in saline.134 In this study,
12
only balanced HES attenuated the decrease in RBF and miti-gated cortical microvascular perfusion deficits. Conversely,when Ergin et al. compared balanced HES to a balanced crys-talloid solution and saline, they found that none of these fluidsaffected cortical or medullary microvascular PO2.
135
Vasodilators and other moleculesAlthough somewhat counterintuitive, the use of vasodilatorshas been advocated to help recruit constricted microvessels inthe septic kidney. Experimental studies on this subject have,however, shown varying results. As described above, Johanneset al. reported no beneficial effect on microvascular oxygena-tion with the use of the NO donor nitroglycerin.118 In contrast,administration of the prostacyclin analogue iloprost improvedcortical microvascular oxygenation in rat endotoxemia,136 asdid the selective phosphodiesterase-IV inhibitor rolipram in amouse model of CLP.137
Other molecular inhibitors and analogues that have beenstudied in the context of renal microcirculatory dysfunction invarious animalmodels of septic shock include the endothelin-1receptor antagonist tezosentan138 and the nonselective caspaseinhibitor Z-VAD.113 Furthermore, the antithrombotic andanti-inflammatory drug, activated protein C, improved peri-tubular perfusion in a rat model of endotoxemia, possiblythrough downregulation of renal iNOS,139 but failed toimprove cortical and medullary microvascular PO2 in another,more severe model.140
Early versus late sepsisInterestingly, some data suggest that the factors involved inrenal microcirculatory dysfunction may change as sepsis pro-gresses. In a pediatric rat model of septic renal dysfunction,Seely et al. showed that reduced whole-organ RBF preceded thedecrease in microcirculatory flow,98 suggesting that earlymicrocirculatory flow impairment may just be a manifestationof an upstream deficit. When Legrand et al. compared early anddelayed fluid administration in a rat model of endotoxemia,they found that early resuscitation maintained RBF at normallevels and attenuated microcirculatory deficiencies, whereasdelayed initiation restored RBF but did not affect microcircu-latory flow.100 These observations may imply that microcir-culatory dysfunction ismaintained by different pathways in lateversus early sepsis. Indeed, when the effects of sphingosine-1-phosphate-1 as a regulator of endothelial permeability wereinvestigated in murine septic shock, early administration didnot benefit capillary flow despite an improvement in vascularpermeability, whereas delayed administration improved capil-lary permeability and restored microvascular perfusion tobaseline levels.132 The authors explained these findings byattributing the early sluggish microcirculatory flow to a lowRPP and late dysfunction to capillary leakage and interstitialedema, whichwas in this case prevented by the intervention.132
Similarly, only delayed administration of the superoxide-scavenger MnTMPyP reversed peritubular microcirculatoryalterations in this model.120
Kidney International (2016) -, -–-

EH Post et al.: Renal macro- and microcirculation in sepsis r ev i ew
Renal metabolism and tubular injury in sepsisThe primary function of the capillaries is oxygen delivery,which suggests that the chain of events leading from micro-circulatory dysfunction to organ failure should include cellularhypoxia. However, renal histological findings in sepsis are notconsistent with signs of widespread structural damage or celldeath,141–143 and results from studies on kidneymetabolism aresomewhat contradictory. For example, kidney ATP levelsremained constant during a 4-hour infusion of live Escherichiacoli in sheep144 but were significantly reduced after 6 hours ofendotoxemia in dogs.145 Conversely, in 2 studies using caninemodels of short-term endotoxemia, the kidney was found to bea net consumer, not producer, of lactate.146,147
In health, renal oxygen consumption (VO2) correlates wellwith RBF because Naþ reabsorption (TNaþ), and thus Naþ-delivery, is the primary determinant of renal VO2.
148 Thistheoretically implies that renal hypoperfusion and decreasedGFR in sepsis will result in reduced renal oxygen demand.Furthermore, mitochondrial downregulation could also adapttubular oxygen demand to decreased oxygen delivery.149 Thiseffect, however,may depend on the vasoactive agent that is usedto manipulate renal hemodynamics.150 Moreover, in sepsis,many studies have reported that renal VO2 was maintained,even when RBF was reduced.29,146,151,152 An increased VO2/TNaþ-ratio has been reported in different experimental sepsismodels, suggesting that either TNaþ is less efficient or thatoxygen-consuming processes unrelated to filtration becomeactive.133,151,153 Indeed, Johannes et al. demonstrated thathypoperfusion associated with endotoxemia induced areas ofmicrocirculatory hypoxia, whereas there were almost nooxygenation deficits in flow-matched healthy controls.154
These findings suggest that renal hypoperfusion in sepsisresults in a perfusion–metabolism mismatch that possiblywarrants treatment. Indeed, in experimental septic renaldysfunction, low tubular cell oxygen tension has been evi-denced by positive pimonidazole staining of tubular epithelialcells.120,130 Moreover, the consistent observation of an alteredredox state in tubular cells adjacent to no-flow capillary vesselsfurther supports this hypothesis.97,114,115 How these oxygena-tion deficits translate to tubular injury in the absence of ne-crosis, or even changes on electron microscopy,143 is not clear,although hypoxia-induced ROS formation96,155 appears to bethe most plausible mechanism.113,115,116 Furthermore, deter-mining causality between microcirculatory flow deficits andtubular injury can be difficult because interventions almostnever act specifically on the renal microcirculation alone, andresults from experimental studies thus remain fundamentallyassociative in nature. Because of this, the temporal relationshipbetweenvariables is often used to support the claim of causality.In this context, all experimental studies that have assessedmicrocirculatory dysfunction and renal functional failure insepsis show that the former precedes, or coincides with, thelatter,8,98,99,115 as was true for tubular injury.113,115,116 More-over, any beneficial effect on kidney function in experimentalsepsis was associated with a similar functional improvement inthe renal microcirculation.113,115,116,120,130,137,138
Kidney International (2016) -, -–-
Summary and conclusionThe contribution of renal hypoperfusion to sepsis-associatedAKI is more complex than previously thought, and reducedRPP and local microvascular deficits may both play pivotalroles. A considerable body of evidence shows that thecorrection of low RPP in septic shock may be effective inraising glomerular filtration pressure and restoring urineoutput and GFR in some patients.68 Whether restoring RPPwith judicious use of fluids and vasopressors also benefits thetubular epithelium is unknown. To our knowledge, there areno clinical studies in septic shock that have measured theeffects of altering RPP on tubular injury. Furthermore,the relationship between tubular injury and diminishedGFR in sepsis remains unclear, although a role of tubulo-glomerular feedback or vascular conducted responses hasbeen proposed.96,156 Nevertheless, given the associationbetween microvascular hypoperfusion, cellular hypoxia, ROSformation, and tubular injury, targeting the tubular epitheliumthrough the alleviation of peritubular perfusion deficits wouldseem to be a rational strategy, especially early in the course ofAKI. Difficulties related to the early detection of AKI and tomonitoring renal microcirculation in vivo, as well as the largenumber of possible mediators involved, make identificationand application of renal microvascular therapy a daunting task.Finally, factors that affect the nature of microvascular perfusiondeficits, such as the stage of sepsis and the presence ofcomorbidities, also need to be taken into account.
DISCLOSUREAll the authors declared no competing interests.
REFERENCES1. Singer M, Deutschman CS, Seymour CW, et al. The Third International
Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA.2016;315:801–810.
2. Schrier RW, Wang W. Acute renal failure and sepsis. N Engl J Med.2004;351:159–169.
3. Bonventre JV, Yang L. Cellular pathophysiology of ischemic acutekidney injury. J Clin Invest. 2011;121:4210–4221.
4. Vincent J-L, Sakr Y, Sprung CL, et al. Sepsis in European intensive careunits: results of the SOAP study. Crit Care Med. 2006;34:344–353.
5. Langenberg C, Bellomo R, May C, et al. Renal blood flow in sepsis. CritCare. 2005;9:R363.
6. Di Giantomasso D, May CN, Bellomo R. Vital organ blood flow duringhyperdynamic sepsis. Chest. 2003;124:1053–1059.
7. Langenberg C, Wan L, Egi M, et al. Renal blood flow in experimentalseptic acute renal failure. Kidney Int. 2006;69:1996–2002.
8. Benes J, Chvojka J, Sykora R, et al. Searching for mechanisms thatmatter in early septic acute kidney injury: an experimental study. CritCare. 2011;15:R256.
9. Lang CH, Bagby GJ, Ferguson JL, Sptizer JJ. Cardiac output andredistribution of organ blood flow in hypermetabolic sepsis. Am JPhysiol. 1984;246:R331–R337.
10. Schneider AJ, Groeneveld AB, Teule GJ, et al. Total body bloodvolume redistribution in porcine E. coli septic shock: effect of volumeloading, dobutamine, and norepinephrine. Circ Shock. 1991;35:215–222.
11. White FN, Gold EM, Vaughn DL. Renin-aldosterone system in endotoxinshock in the dog. Am J Physiol. 1967;212:1195–1198.
12. Cumming AD, Driedger AA, McDonald JW, et al. Vasoactive hormonesin the renal response to systemic sepsis. Am J Kidney Dis. 1988;11:23–32.
13. Badr KF. Sepsis-associated renal vasoconstriction: potential targets forfuture therapy. Am J Kidney Dis. 1992;20:207–213.
13

r ev i ew EH Post et al.: Renal macro- and microcirculation in sepsis
14. Boffa J-J, Just A, Coffman TM, Arendshorst WJ. Thromboxane receptormediates renal vasoconstriction and contributes to acute renal failurein endotoxemic mice. J Am Soc Nephrol. 2004;15:2358–2365.
15. Arendshorst WJ, Finn WF, Gottschalk CW. Autoregulation of blood flowin the rat kidney. Am J Physiol. 1975;228:127–133.
16. Ott CE, Vari RC. Renal autoregulation of blood flow and filtration rate inthe rabbit. Am J Physiol. 1979;237:F479–F482.
17. Just A, Wittmann U, Ehmke H, Kirchheim HR. Autoregulation of renalblood flow in the conscious dog and the contribution of thetubuloglomerular feedback. J Physiol. 1998;506:275–290.
18. Dole WP. Autoregulation of the coronary circulation. Prog CardiovascDis. 1987;29:293–323.
19. Lassen NA. Cerebral blood flow and oxygen consumption in man.Physiol Rev. 1959;39:183–238.
20. Schlichtig R, Kramer DJ, Pinsky MR. Flow redistribution duringprogressive hemorrhage is a determinant of critical O2 delivery. J ApplPhysiol. 1991;70:169–178.
21. Bellomo R, Kellum JA, Wisniewski SR, Pinsky MR. Effects of norepinephrineon the renal vasculature in normal and endotoxemic dogs. Am J RespirCrit Care Med. 1999;159:1186–1192.
22. Cupples WA, Braam B. Assessment of renal autoregulation. Am J PhysiolRenal Physiol. 2007;292:F1105–F1123.
23. Burban M, Hamel J-F, Tabka M, et al. Renal macro- and microcirculationautoregulatory capacity during early sepsis and norepinephrineinfusion in rats. Crit Care. 2013;17:R139.
24. Rhee CJ, Kibler KK, Easley RB, et al. Renovascular reactivity measured bynear-infrared spectroscopy. J Appl Physiol. 2012;113:307–314.
25. Prowle JR, Ishikawa K, May CN, Bellomo R. Renal blood flow duringacute renal failure in man. Blood Purif. 2009;28:216–225.
26. Prowle JR, Ishikawa K, May CN, Bellomo R. Renal plasma flow andglomerular filtration rate duringacute kidney injury in man. Ren Fail.2010;32:349–355.
27. Prowle J, Bagshaw SM, Bellomo R. Renal blood flow, fractional excretionof sodium and acute kidney injury: time for a new paradigm? Curr OpinCrit Care. 2012;18:585–592.
28. Brenner M, Schaer GL, Mallory DL, et al. Detection of renal blood flowabnormalities in septic and critically ill patients using a newly designedindwelling thermodilution renal vein catheter. Chest. 1990;98:170–179.
29. Redfors B, Bragadottir G, Sellgren J, et al. Effects of norepinephrine onrenal perfusion, filtration and oxygenation in vasodilatory shock andacute kidney injury. Intensive Care Med. 2011;37:60–67.
30. Lerolle N, Guérot E, Faisy C, et al. Renal failure in septic shock: predictivevalue of Doppler-based renal arterial resistive index. Intensive Care Med.2006;32:1553–1559.
31. Wan L, Yang N, Hiew CY, et al. An assessment of the accuracy of renalblood flow estimation by Doppler ultrasound. Intensive Care Med.2008;34:1503–1510.
32. Prowle JR, Molan MP, Hornsey E, Bellomo R. Measurement of renalblood flow by phase-contrast magnetic resonance imaging duringseptic acute kidney injury: A pilot investigation. Crit Care Med. 2012;40:1768–1776.
33. Martin C, Eon B, Saux P, et al. Renal effects of norepinephrine used totreat septic shock patients. Crit Care Med. 1990;18:282–285.
34. Dünser MW, Takala J, Ulmer H, et al. Arterial blood pressure during earlysepsis and outcome. Intensive Care Med. 2009;35:1225–1233.
35. Badin J, Boulain T, Ehrmann S, et al. Relation between mean arterialpressure and renal function in the early phase of shock: a prospective,explorative cohort study. Crit Care. 2011;15:R135.
36. Poukkanen M, Wilkman E, Vaara ST, et al. Hemodynamic variables andprogression of acute kidney injury in critically ill patients with severesepsis: data from the prospective observational FINNAKI study. CritCare. 2013;17:R295.
37. Legrand M, Dupuis C, Simon C, et al. Association between systemichemodynamics and septic acute kidney injury in critically ill patients: aretrospective observational study. Crit Care. 2013;17:11278.
38. Wong BT, Chan MJ, Glassford NJ, et al. Mean arterial pressure and meanperfusion pressure deficit in septic acute kidney injury. J Crit Care.2015;30:975–981.
39. Murugan R, Karajala-Subramanyam V, Lee M, et al. Acute kidney injuryin non-severe pneumonia is associated with an increased immuneresponse and lower survival. Kidney Int. 2010;77:527–535.
40. Treggiari MM, Romand J-A, Burgener D, et al. Effect of increasingnorepinephrine dosage on regional blood flow in a porcine model ofendotoxin shock. Crit Care Med. 2002;30:1334–1339.
14
41. Albert M, Losser M-R, Hayon D, et al. Systemic and renal macro- andmicrocirculatory responses to arginine vasopressin in endotoxic rabbits.Crit Care Med. 2004;32:1891–1898.
42. Boffa J-J, Arendshorst WJ. Maintenance of renal vascular reactivitycontributes to acute renal failure during endotoxemic shock. J Am SocNephrol. 2005;16:117–124.
43. Ishikawa K, Wan L, Calzavacca P, et al. The effects of terlipressin onregional hemodynamics and kidney function in experimentalhyperdynamic sepsis. PLoS ONE. 2012;7:e29693.
44. Ishikawa K, Bellomo R, May CN. The impact of intrarenal nitric oxidesynthase inhibition on renal blood flow and function in mild and severehyperdynamic sepsis. Crit Care Med. 2011;39:770–776.
45. Ishikawa K, Calzavacca P, Bellomo R, et al. Effect of selective inhibitionof renal inducible nitric oxide synthase on renal blood flow andfunction in experimental hyperdynamic sepsis. Crit Care Med. 2012;40:2368–2375.
46. Wan L, Langenberg C, Bellomo R, May CN. Angiotensin II in experimentalhyperdynamic sepsis. Crit Care. 2009;13:R190.
47. Shanbour LL, Lindeman RD, Archer LT, et al. Improvement of renalhemodynamics in endotoxin shock with dopamine, phenoxybenzamineand dextran. J Pharmacol Exp Ther. 1971;176:383–388.
48. Rao PS, Bhagat B. Effect of dopamine on renal blood flow of baboon inendotoxin shock. Pflüg Arch. 1978;374:105–106.
49. Fink MP, Nelson R, Roethel R. Low-dose dopamine preserves renalblood flow in endotoxin shocked dogs treated with ibuprofen. J SurgRes. 1985;38:582–591.
50. Bersten AD, Rutten AJ. Renovascular interaction of epinephrine,dopamine, and intraperitoneal sepsis. Crit Care Med. 1995;23:537–544.
51. Post EH, Su F, Taccone FS, et al. The effects of fenoldopam on renalfunction and metabolism in an ovine model of septic shock. Shock.2016;45:385–392.
52. Desjars T. A reappraisal of norepinephrine therapy in human septicshock. Crit Care Med. 1987;15:135–137.
53. Hesselvik. Low dose norepinephrine in patients with septic shock andoliguria: Effects on after load, urine flow, and oxygen transport. Crit CareMed. 1989;17:179–180.
54. Martin C, Papazian L, Perrin G, et al. Norepinephrine or dopamine for thetreatment of hyperdynamic septic shock? Chest. 1993;103:1826–1831.
55. Desjars P, Pinaud M, Bugnon D, Tasseau F. Norepinephrine therapy hasno deleterious renal effects in human septic shock. Crit Care Med.1989;17:426–429.
56. Albanèse J, Leone M, Garnier F, et al. Renal effects of norepinephrine inseptic and nonseptic patients. Chest. 2004;126:534–539.
57. Redl-Wenzl DEM, Armbruster C, Edelmann G, et al. The effects ofnorepinephrine on hemodynamics and renal function in severe septicshock states. Intensive Care Med. 1993;19:151–154.
58. Patel BM, Chittock DR, Russell JA, Walley KR. Beneficial effects of short-term vasopressin infusion during severe septic shock. Anesthesiology.2002;96:576–582.
59. Leone M, Albanèse J, Delmas A, et al. Terlipressin in catecholamine-resistant septic shock patients. Shock. 2004;22:314–319.
60. Albanèse J, Leone M, Delmas A, Martin C. Terlipressin or norepinephrinein hyperdynamic septic shock: A prospective, randomized study. CritCare Med. 2005;33:1897–1902.
61. Lauzier F, Lévy B, Lamarre P, Lesur O. Vasopressin or norepinephrine inearly hyperdynamic septic shock: a randomized clinical trial. IntensiveCare Med. 2006;32:1782–1789.
62. Morelli A, Ertmer C, Rehberg S, et al. Continuous terlipressin versusvasopressin infusion in septic shock (TERLIVAP): a randomized,controlled pilot study. Crit Care. 2009;13:R130.
63. Gordon AC, Russell JA, Walley KR, et al. The effects of vasopressin onacute kidney injury in septic shock. Intensive Care Med. 2010;36:83–91.
64. Deruddre S, Cheisson G, Mazoit JX, et al. Renal arterial resistance inseptic shock: effects of increasing mean arterial pressure withnorepinephrine on the renal resistive index assessed with Dopplerultrasonography. Intensive Care Med. 2007;33:1557–1562.
65. LeDoux D, Astiz ME, Carpati CM, Rackow E. Effects of perfusion pressureon tissue perfusion in septic shock. Crit Care Med. 2000;28:2729–2732.
66. Bourgoin A, Leone M, Delmas A, et al. Increasing mean arterial pressurein patients with septic shock: Effects on oxygen variables and renalfunction. Crit Care Med. 2005;33:780–786.
67. Schneider AG, Goodwin MD, Schelleman A, et al. Contrast-enhancedultrasonography to evaluate changes in renal cortical microcirculationinduced by noradrenaline: a pilot study. Crit Care. 2014;18:653.
Kidney International (2016) -, -–-

EH Post et al.: Renal macro- and microcirculation in sepsis r ev i ew
68. Asfar P, Meziani F, Hamel JF, et al. High versus low blood-pressuretarget in patients with septic shock. N Engl J Med. 2014;370:1583–1593.
69. Loutzenhiser R. Renal autoregulation: new perspectives regarding theprotective and regulatory roles of the underlying mechanisms. Am JPhysiol Regul Integr Comp Physiol. 2005;290:R1153–R1167.
70. Mårtensson J, Bellomo R. Are all fluids bad for the kidney? Curr Opin CritCare. 2015;21:292–301.
71. Prowle JR, Echeverri JE, Ligabo EV, et al. Fluid balance and acute kidneyinjury. Nat Rev Nephrol. 2010;6:107–115.
72. Chowdhury AH, Cox EF, Francis ST, Lobo DN. A randomized, controlled,double-blind crossover study on the effects of 2-L infusions of 0.9%saline and Plasma-Lyte� 148 on renal blood flow velocity and renalcortical tissue perfusion in healthy volunteers. Ann Surg. 2012;256:18–24.
73. Zhou F, Peng Z-Y, Bishop JV, et al. Effects of fluid resuscitation with0.9% saline versus a balanced electrolyte solution on acute kidneyinjury in a rat model of sepsis. Crit Care Med. 2014;42:e270–e278.
74. Kellum JA, Chawla LS, Keener C, et al. The effects of alternativeresuscitation strategies on acute kidney injury in patients with septicshock. Am J Respir Crit Care Med. 2016;193:281–287.
75. Lherm T, Troché G, Rossignol M, et al. Renal effects of low-dosedopamine in patients with sepsis syndrome or septic shock treatedwith catecholamines. Intensive Care Med. 1996;22:213–219.
76. Morelli A, Ricci Z, Bellomo R, et al. Prophylactic fenoldopam for renalprotection in sepsis: a randomized, double-blind, placebo-controlledpilot trial. Crit Care Med. 2005;33:2451–2456.
77. Juste RN, Panikkar K, Soni N. The effects of low-dose dopamineinfusions on haemodynamic and renal parameters in patients withseptic shock requiring treatment with noradrenaline. Intensive CareMed. 1998;24:564–568.
78. Day NP, Phu NH, Mai NT, et al. Effects of dopamine and epinephrineinfusions on renal hemodynamics in severe malaria and severe sepsis.Crit Care Med. 2000;28:1353–1362.
79. Bellomo R, Chapman M, Finfer S, et al. Low-dose dopamine in patientswith early renal dysfunction: a placebo-controlled randomised trial.Australian and New Zealand Intensive Care Society (ANZICS) ClinicalTrials Group. Lancet. 2000;356:2139–2143.
80. Takeuchi J, Ishikawa I, Inasaka T, et al. Intrarenal distribution of bloodflow in man a new analytical method for dye-dilution curves.Circulation. 1970;42:347–360.
81. Beeuwkes R III. The vascular organization of the kidney. Annu RevPhysiol. 1980;42:531–542.
82. Ravikant T, Lucas CE. Renal blood flow distribution in septichyperdynamic pigs. J Surg Res. 1977;22:294–298.
83. Stone AM, Stein T, LaFortune J, Wise L. Changes in intrarenal blood flowduring sepsis. Surg Gynecol Obstet. 1979;148:731–734.
84. Cronenwett JL, Lindenauer SM. Distribution of intrarenal blood flowduring bacterial sepsis. J Surg Res. 1978;24:132–141.
85. Auguste LJ, Stone AM, Wise L. The effects of Escherichia coli bacteremiaon in vitro perfused kidneys. Ann Surg. 1980;192:65–68.
86. Di Giantomasso D, Morimatsu H, May CN, Bellomo R. Intrarenal bloodflow distribution in hyperdynamic septic shock: Effect ofnorepinephrine. Crit Care Med. 2003;31:2509–2513.
87. Calzavacca P, Evans RG, Bailey M, et al. Cortical and medullary tissueperfusion and oxygenation in experimental septic acute kidney injury.Crit Care Med. 2015;43:e431–e439.
88. Cohen RI, Hassell A-M, Marzouk K, et al. Renal effects of nitric oxide inendotoxemia. Am J Respir Crit Care Med. 2001;164:1890–1895.
89. Faivre V, Kaskos H, Callebert J, et al. Cardiac and renal effects oflevosimendan, arginine vasopressin, and norepinephrine inlipopolysaccharide-treated rabbits. Anesthesiology. 2005;103:514–521.
90. Lankadeva YR, Kosaka J, Evans RG, et al. Intrarenal and urinaryoxygenation during norepinephrine resuscitation in ovine septic acutekidney injury. Kidney Int. 2016;90:100–108.
91. Schurek HJ, Jost U, Baumgärtl H, et al. Evidence for a preglomerularoxygen diffusion shunt in rat renal cortex. Am J Physiol. 1990;259:F910–F915.
92. Molitoris BA, Sandoval RM. Kidney endothelial dysfunction: ischemia,localized infections and sepsis. Contrib Nephrol. 2011;174:108–118.
93. Leong CL, Anderson WP, O’Connor PM, et al. Evidence that renalarterial-venous oxygen shunting contributes to dynamic regulation ofrenal oxygenation. Am J Physiol Renal Physiol. 2007;292:F1726–F1733.
94. O’Connor PM, Anderson WP, Kett MM, Evans RG. Renal preglomerulararterial-venous O2 shunting is a structural anti-oxidant defence
Kidney International (2016) -, -–-
mechanism of the renal cortex. Clin Exp Pharmacol Physiol. 2006;33:637–641.
95. De Backer D, Orbegozo Cortes D, Donadello K, Vincent JL.Pathophysiology of microcirculatory dysfunction and the pathogenesisof septic shock. Virulence. 2014;5:73–79.
96. Gomez H, Ince C, De Backer D, et al. A unified theory of sepsis-inducedacute kidney injury: inflammation, microcirculatory dysfunction,bioenergetics, and the tubular cell adaptation to injury. Shock. 2014;41:3–11.
97. Wu L, Tiwari MM, Messer KJ, et al. Peritubular capillary dysfunction andrenal tubular epithelial cell stress following lipopolysaccharideadministration in mice. Am J Physiol Ren Physiol. 2006;292:F261–F268.
98. Seely KA, Holthoff JH, Burns ST, et al. Hemodynamic changes in thekidney in a pediatric rat model of sepsis-induced acute kidney injury.Am J Physiol Ren Physiol. 2011;301:F209–F217.
99. Chvojka J, Sykora R, Krouzecky A, et al. Renal haemodynamic,microcirculatory, metabolic and histopathological responses toperitonitis-induced septic shock in pigs. Crit Care. 2008;12:R164.
100. Legrand M, Bezemer R, Kandil A, et al. The role of renal hypoperfusionin development of renal microcirculatory dysfunction in endotoxemicrats. Intensive Care Med. 2011;37:1534–1542.
101. Bevilacqua MP, Stengelin S, Gimbrone MA, Seed B. Endothelialleukocyte adhesion molecule 1: an inducible receptor for neutrophilsrelated to complement regulatory proteins and lectins. Science.1989;243:1160–1165.
102. Alves-Filho JC, Sônego F, Souto FO, et al. Interleukin-33 attenuatessepsis by enhancing neutrophil influx to the site of infection. Nat Med.2010;16:708–712.
103. De Backer D, Donadello K, Favory R. Link between coagulationabnormalities and microcirculatory dysfunction in critically ill patients.Curr Opin Anaesthesiol. 2009;22:150–154.
104. Ince C. The microcirculation is the motor of sepsis. Crit Care. 2005;9:S13.105. Souza ACP, Yuen PST, Star RA. Microparticles: markers and mediators of
sepsis-induced microvascular dysfunction, immunosuppression, andAKI. Kidney Int. 2015;87:1100–1108.
106. Allam R, Scherbaum CR, Darisipudi MN, et al. Histones from dying renalcells aggravate kidney injury via TLR2 and TLR4. J Am Soc Nephrol.2012;23:1375–1388.
107. Chelazzi C, Villa G, Mancinelli P, et al. Glycocalyx and sepsis-inducedalterations in vascular permeability. Crit Care. 2015;19:26.
108. Blum MS, Toninelli E, Anderson JM, et al. Cytoskeletal rearrangementmediates human microvascular endothelial tight junction modulationby cytokines. Am J Physiol. 1997;273:H286–H294.
109. Heemskerk S, Masereeuw R, Russel FGM, Pickkers P. Selective iNOSinhibition for the treatment of sepsis-induced acute kidney injury. NatRev Nephrol. 2009;5:629–640.
110. Tsukahara Y, Morisaki T, Kojima M, et al. iNOS expression by activatedneutrophils from patients with sepsis. J Surg. 2001;71:15–20.
111. Wu F, Tyml K, Wilson JX. iNOS expression requires NADPH oxidase-dependent redox signaling in microvascular endothelial cells. J CellPhysiol. 2008;217:207–214.
112. Bultinck J, Sips P, Vakaet L, et al. Systemic NO production during (septic)shock depends on parenchymal and not on hematopoietic cells: in vivoiNOS expression pattern in (septic) shock. FASEB J. 2006;20:2363–2365.
113. Tiwari MM, Brock RW, Megyesi JK, et al. Disruption of renal peritubularblood flow in lipopolysaccharide-induced renal failure: role of nitricoxide and caspases. Am J Physiol Renal Physiol. 2005;289:F1324–F1332.
114. Wu L, Mayeux PR. Effects of the inducible nitric-oxide synthase inhibitorL-N6-(1-Iminoethyl)-lysine on microcirculation and reactive nitrogenspecies generation in the kidney following lipopolysaccharideadministration in mice. J Pharmacol Exp Ther. 2006;320:1061–1067.
115. Wu L, Gokden N, Mayeux PR. Evidence for the role of reactive nitrogenspecies in polymicrobial sepsis-induced renal peritubular capillarydysfunction and tubular injury. J Am Soc Nephrol. 2007;18:1807–1815.
116. Holthoff JH, Wang Z, Seely KA, et al. Resveratrol improves renalmicrocirculation, protects the tubular epithelium, and prolongs survivalin a mouse model of sepsis-induced acute kidney injury. Kidney Int.2012;81:370–378.
117. Johannes T, Mik EG, Klingel K, et al. Low-dose dexamethasone-supplemented fluid resuscitation reverses endotoxin-induced acuterenal failure and prevents cortical microvascular hypoxia. Shock.2009;31:521–528.
118. Johannes T, Mik EG, Klingel K, et al. Effects of 1400W and/ornitroglycerin on renal oxygenation and kidney function during
15

r ev i ew EH Post et al.: Renal macro- and microcirculation in sepsis
endotoxemia in anaesthetized rats. Clin Exp Pharmacol Physiol.2009;36:870–879.
119. Wu F, Schuster DP, Tyml K, Wilson JX. Ascorbate inhibits NADPHoxidase subunit p47phox expression in microvascular endothelial cells.Free Radic Biol Med. 2007;42:124–131.
120. Wang Z, Holthoff JH, Seely KA, et al. Development of oxidative stress inthe peritubular capillary microenvironment mediates sepsis-inducedrenal microcirculatory failure and acute kidney injury. Am J Pathol.2012;180:505–516.
121. Patil NK, Parajuli N, MacMillan-Crow LA, Mayeux PR. Inactivation of renalmitochondrial respiratory complexes and manganese superoxidedismutase during sepsis: mitochondria-targeted antioxidant mitigatesinjury. Am J Physiol Ren Physiol. 2014;306:F734–F743.
122. Tyml K, Li F, Wilson JX. Septic impairment of capillary blood flowrequires nicotinamide adenine dinucleotide phosphate oxidase but notnitric oxide synthase and is rapidly reversed by ascorbate through anendothelial nitric oxide synthase-dependent mechanism. Crit Care Med.2008;36:2355–2362.
123. He X, Su F, Velissaris D, et al. Administration of tetrahydrobiopterinimproves the microcirculation and outcome in an ovine model of septicshock. Crit Care Med. 2012;40:2833–2840.
124. Wang W. Endothelial nitric oxide synthase-deficient mice exhibitincreased susceptibility to endotoxin-induced acute renal failure. Am JPhysiol Ren Physiol. 2004;287:F1044–F1048.
125. Haraldsson BS. The endothelium as part of the integrative glomerularbarrier complex. Kidney Int. 2014;85:8–11.
126. Xu C, Chang A, Hack BK, et al. TNF-mediated damage to glomerularendothelium is an important determinant of acute kidney injury insepsis. Kidney Int. 2014;85:72–81.
127. Adembri C, Sgambati E, Vitali L, et al. Sepsis induces albuminuria andalterations in the glomerular filtration barrier: a morphofunctional studyin the rat. Crit. Care. 2011;15:R277.
128. Moreira RS, Irigoyen M, Sanches TR, et al. Apolipoprotein A-I mimeticpeptide 4F attenuates kidney injury, heart injury, and endothelialdysfunction in sepsis. Am J Physiol Regul Integr Comp Physiol. 2014;307:R514–R524.
129. Thibeault S, Rautureau Y, Oubaha M, et al. S-Nitrosylation of b-cateninby eNOS-derived NO promotes VEGF-induced endothelial cellpermeability. Mol Cell. 2010;39:468–476.
130. Yasuda H, Yuen PST, Hu X, et al. Simvastatin improves sepsis-inducedmortality and acute kidney injury via renal vascular effects. Kidney Int.2006;69:1535–1542.
131. Zeng Y, Adamson RH, Curry FRE, Tarbell JM. Sphingosine-1-phosphateprotects endothelial glycocalyx by inhibiting syndecan-1 shedding. AmJ Physiol Heart Circ Physiol. 2014;306:H363–H372.
132. Wang Z, Sims CR, Patil NK, et al. Pharmacologic targeting of sphingosine-1-phosphate receptor 1 improves the renal microcirculation duringsepsis in the mouse. J Pharmacol Exp Ther. 2015;352:61–66.
133. Johannes T, Mik EG, Nohé B, et al. Influence of fluid resuscitation onrenal microvascular PO2 in a normotensive rat model of endotoxemia.Crit Care. 2006;10:R88.
134. Aksu U, Bezemer R, Demirci C, Ince C. Acute effects of balanced versusunbalanced colloid resuscitation on renal macrocirculatory andmicrocirculatory perfusion during endotoxemic shock. Shock. 2012;37:205–209.
135. Ergin B, Zafrani L, Kandil A, et al. Fully balanced fluids do not improvemicrovascular oxygenation, acidosis and renal function in a rat modelof endotoxemia. Shock. 2016;46:83–91.
16
136. Johannes T, Ince C, Klingel K, et al. Iloprost preserves renal oxygenationand restores kidney function in endotoxemia-related acute renal failurein the rat. Crit Care Med. 2009;37:1423–1432.
137. Holthoff JH, Wang Z, Patil NK, et al. Rolipram improves renal perfusionand function during sepsis in the mouse. J Pharmacol Exp Ther.2013;347:357–364.
138. Fenhammar J, Andersson A, Frithiof R, et al. The endothelin receptorantagonist tezosentan improves renal microcirculation in a porcinemodel of endotoxemic shock: Renal microcirculation in a porcine modelof endotoxemic shock. Acta Anaesthesiol Scand. 2008;52:1385–1393.
139. Gupta A, Rhodes GJ, Berg DT, et al. Activated protein C amelioratesLPS-induced acute kidney injury and downregulates renal INOS andangiotensin 2. Am J Physiol Renal Physiol. 2007;293:F245–F254.
140. Almac E, Johannes T, Bezemer R, et al. Activated protein C amelioratesimpaired renal microvascular oxygenation and sodium reabsorption inendotoxemic rats. Intensive Care Med Exp. 2013;1:24.
141. Langenberg C, Bagshaw SM, May CN, Bellomo R. The histopathology ofseptic acute kidney injury: a systematic review. Crit Care. 2008;12:R38.
142. Takasu O, Gaut JP, Watanabe E, et al. Mechanisms of cardiac and renaldysfunction in patients dying of sepsis. Am J Respir Crit Care Med.2013;187:509–517.
143. Maiden MJ, Otto S, Brealey JK, et al. Structure and function of thekidney in septic shock: a prospective controlled experimental study. AmJ Respir Crit Care Med. 2016;194:692–700.
144. May CN, Ishikawa K, Wan L, et al. Renal bioenergetics during early gram-negative mammalian sepsis and angiotensin II infusion. Intensive CareMed. 2012;38:886–893.
145. Yang R, Wang X, Liu D, Liu SB. Energy and oxygen metabolism disorderduring septic acute kidney injury. Kidney Blood Press Res. 2014;39:240–251.
146. Gullichsen E. Renal perfusion and metabolism in experimentalendotoxin shock. Acta Chir Scand Suppl. 1991;560:S7–S31.
147. Bellomo R, Kellum JA, Pinsky MR. Transvisceral lactate fluxes duringearly endotoxemia. Chest. 1996;110:198–204.
148. Ricksten S-E, Bragadottir G, Redfors B. Renal oxygenation in clinicalacute kidney injury. Crit Care. 2013;17:221.
149. Tran M, Tam D, Bardia A, et al. PGC-1a promotes recovery after acutekidney injury during systemic inflammation in mice. J Clin Invest.2011;121:4003–4014.
150. Calzavacca P, Evans RG, Bailey M, et al. Variable responses of regionalrenal oxygenation and perfusion to vasoactive agents in awake sheep.Am J Physiol Regul Integr Comp Physiol. 2015;309:R1226–R1233.
151. Weber A, Schwieger IM, Poinsot O, et al. Sequential changes in renaloxygen consumption and sodium transport during hyperdynamicsepsis in sheep. Am J Physiol. 1992;262:F965–F971.
152. Dyson A, Bezemer R, Legrand M, et al. Microvascular and interstitialoxygen tension in the renal cortex and medulla studied in a 4-h ratmodel of LPS-induced endotoxemia. Shock. 2011;36:83–89.
153. Heemskerk AE, Huisman E, Van Lambalgen AA, et al. Renal function andoxygen consumption during bacteraemia and endotoxaemia in rats.Nephrol Dial Transplant. 1997;12:1586–1594.
154. Johannes T, Mik EG, Ince C. Nonresuscitated endotoxemia inducesmicrocirculatory hypoxic areas in the renal cortex in the rat. Shock.2009;31:97–103.
155. Heyman SN, Rosen S, Rosenberger C. A role for oxidative stress. Contrib.Nephrol. 2011;174:138–148.
156. Tyml K, Wang X, Lidington D, Ouellette Y. Lipopolysaccharide reducesintercellular coupling in vitro and arteriolar conducted response in vivo.Am J Physiol Heart Circ Physiol. 2001;281:H1397–H1406.
Kidney International (2016) -, -–-