Embed Size (px)
Citation preview
ME
DA
LL
ME
DA
LL
Integrated Diagnostics – A Unique Epilepsy Approach
Dr. Rama KrishnanDr. Rama Krishnan
Consultant Radiologist
Medall Health Care Private Limited
Chennai
ME
DA
LL
ME
DA
LL
Next 20 minutes…
Basic introduction to epilepsy and the burden of disease in society and the need for investigations.
Imaging modalities - MRI
Clinico-radiologic images.
Integrated Neuro diagnostics.
ME
DA
LL
ME
DA
LL
Seizure & Epilepsy
Seizure - Definite event of altered cerebral function due to excessive and abnormal electrical discharge from brain cells.
Greek word - epilepsia “taking hold of or seizing”
Chronic neurologic disorder
Spontaneous recurrent seizures
First seizure ever 4% of population
Epilepsy 1% of population
Uncontrollable epi 0.4% of population
80% has epileptogenic focuson dedicated MRI
Imaging can be normal
Fever, drugs, dehydration & sleep deprivation
ME
DA
LL
ME
DA
LL
Is investigation really needed?
What is the most effective method?
ME
DA
LL
ME
DA
LL
50 million sufferers in the world today, 85% of whom live in the developing countries
2.4 million new cases each year
50% cases begin in childhood/adolescents
70-80% of people with epilepsy could lead normal lives if properly diagnosed and treated
ME
DA
LL
ME
DA
LL
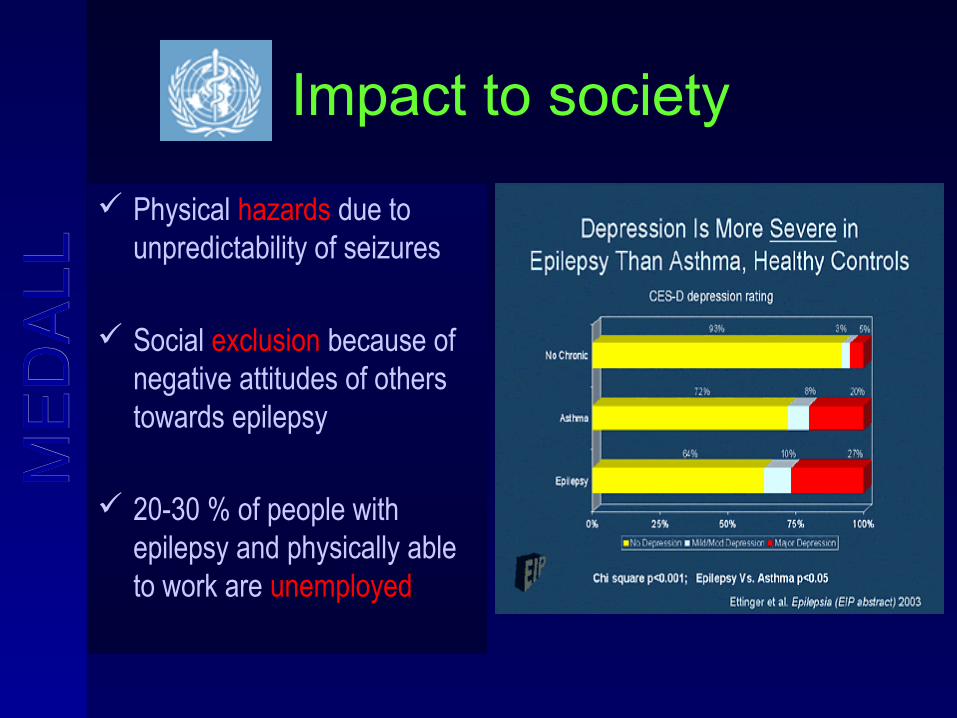
Impact to society
Physical hazards due to unpredictability of seizures
Social exclusion because of negative attitudes of others towards epilepsy
20-30 % of people with epilepsy and physically able to work are unemployed
ME
DA
LL
ME
DA
LL
How is epilepsy treated?
Long term pharmacotherapy - Drugs
Neurosurgery – when removal of epileptogenic focus is possible without unacceptable neurologic deficit
Uncontrollable epi 0.4% of population
80% has epileptogenic focuson dedicated MRI
Lesion resection can lead to seizure freedom in many patients
ME
DA
LL
ME
DA
LL
Role of neuroimaging
To identify underlying structural abnormalities that require specific treatment
Determine functional areas
To aid in formulating a syndromic or etiologic diagnosis
ME
DA
LL
ME
DA
LL
Modalities of neuroimaging
Structural Functional
CT f MRI
MRI MRS
MEG
SPECT
PET
ME
DA
LL
ME
DA
LL
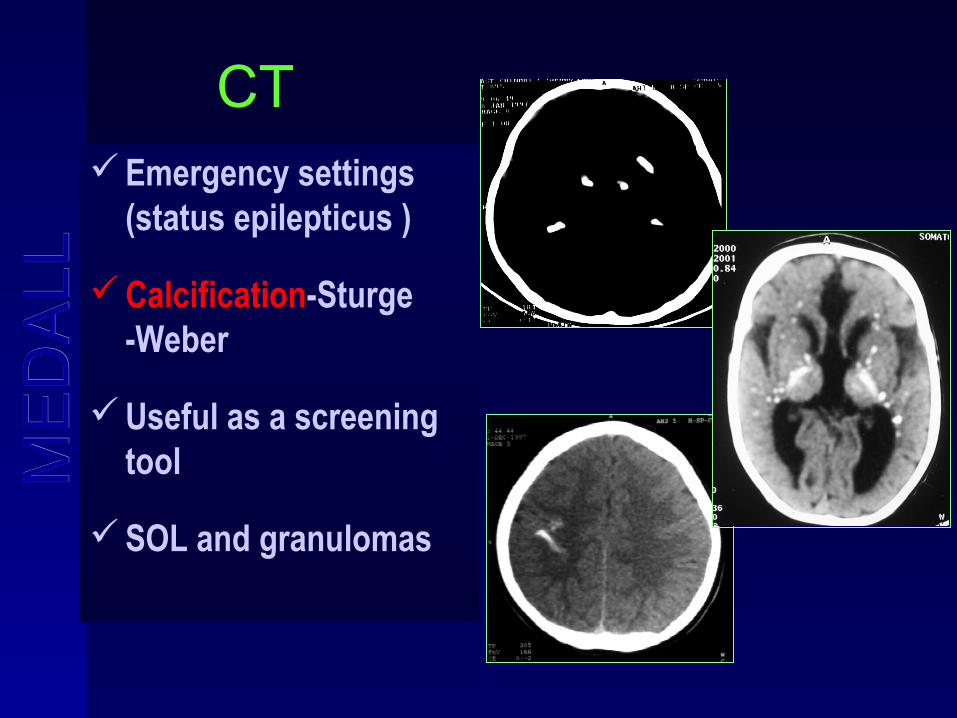
CTEmergency settings
(status epilepticus )
Calcification-Sturge -Weber
Useful as a screening tool
SOL and granulomas
ME
DA
LL
ME
DA
LL
CT – PITFALLS
Sensitivity not more than 30%
Poor resolution in the temporal fossa – not helpful in the diagnosis of MTS
Fails to detect abnormalities upto 50% of patients
ME
DA
LL
ME
DA
LL
ILAE RECOMMENDATIONS
CT can be the diagnostic imaging of choice in patients with epilepsy if MRI is not available
Patients who have intractable seizures should have an MRI study even if CT is normal
ME
DA
LL
ME
DA
LL
MRI
Imaging procedure of choice
Identifies and localizes structural abnormalities like MTS
Surgical planning
Covers both anatomic and physiologic aspects
Post-operative imaging
ME
DA
LL
ME
DA
LL
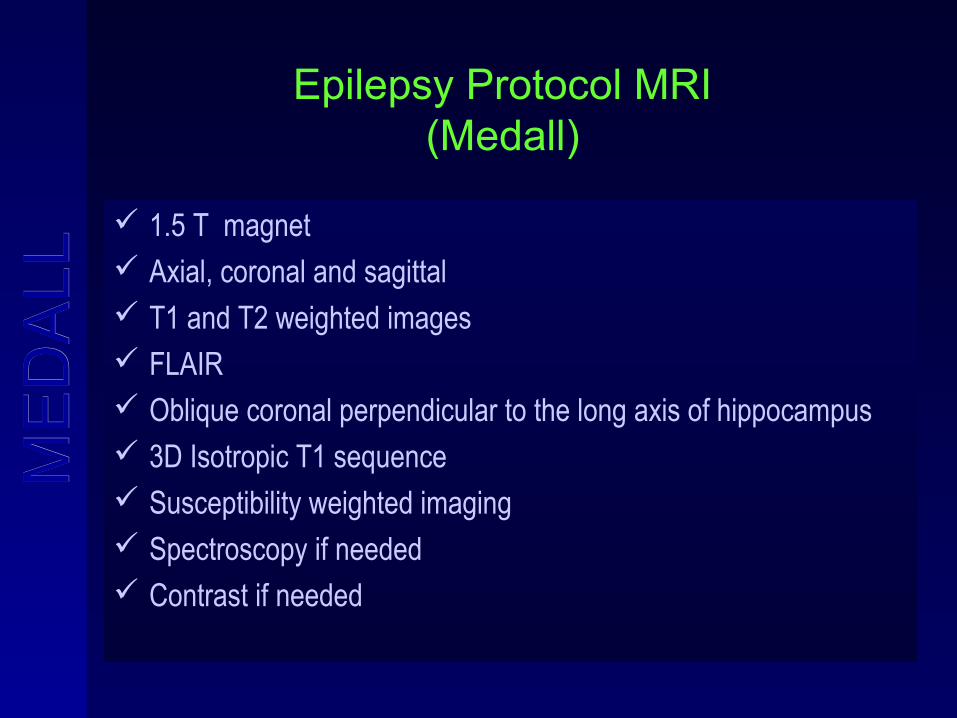
Epilepsy Protocol MRI(Medall)
1.5 T magnet Axial, coronal and sagittal T1 and T2 weighted images FLAIR Oblique coronal perpendicular to the long axis of hippocampus 3D Isotropic T1 sequence Susceptibility weighted imaging Spectroscopy if needed Contrast if needed
ME
DA
LL
ME
DA
LL
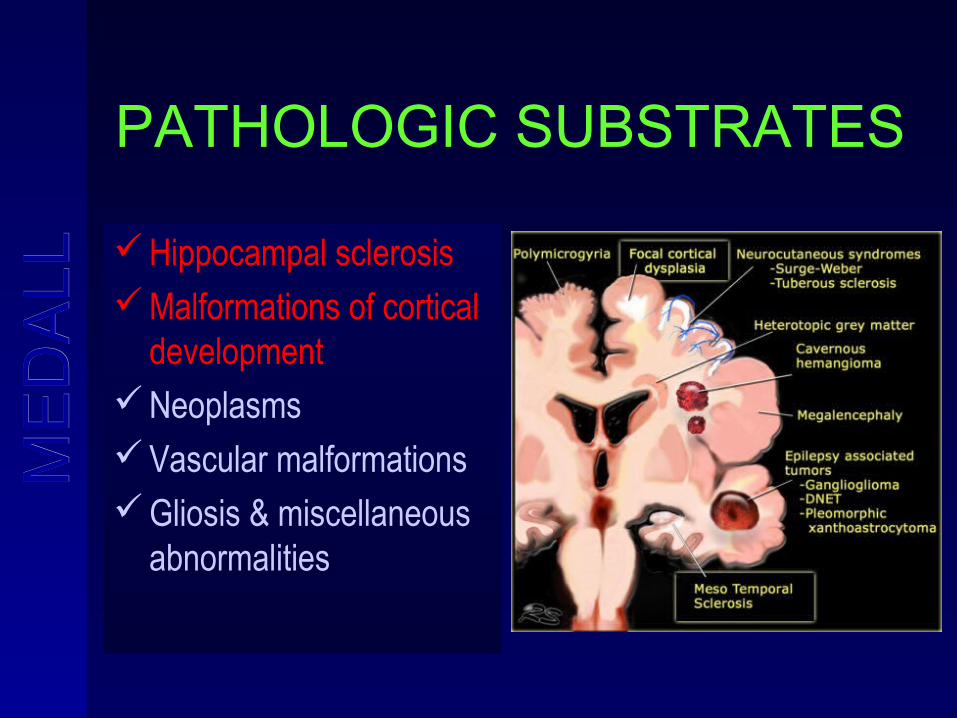
PATHOLOGIC SUBSTRATES
Hippocampal sclerosisMalformations of cortical
developmentNeoplasmsVascular malformationsGliosis & miscellaneous
abnormalities
ME
DA
LL
ME
DA
LL
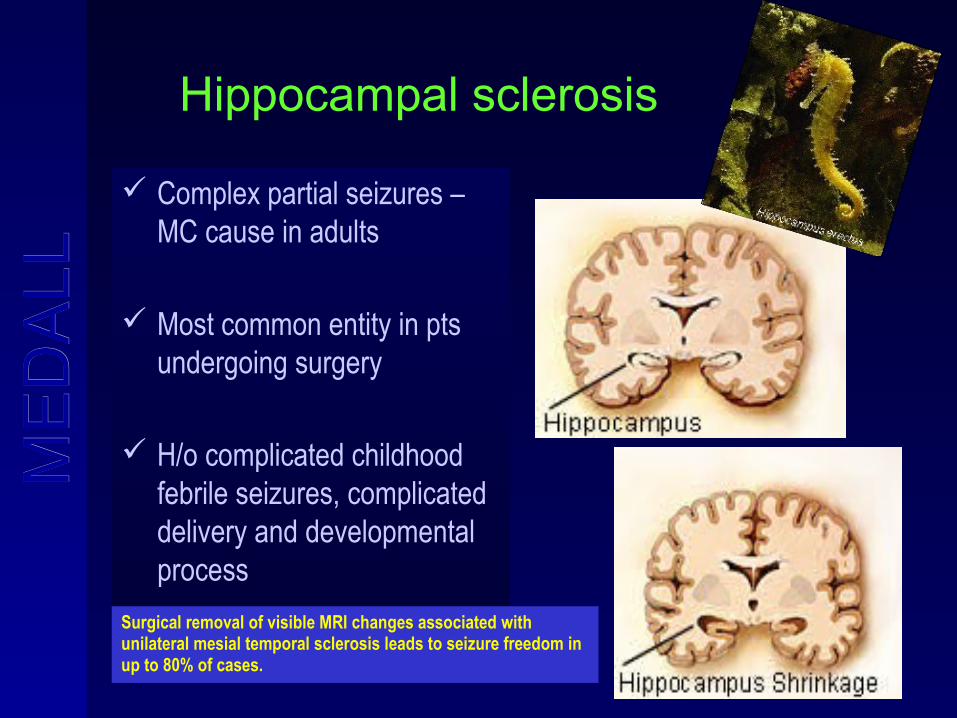
Hippocampal sclerosis
Complex partial seizures – MC cause in adults
Most common entity in pts undergoing surgery
H/o complicated childhood febrile seizures, complicated delivery and developmental process
Surgical removal of visible MRI changes associated with unilateral mesial temporal sclerosis leads to seizure freedom in up to 80% of cases.
ME
DA
LL
ME
DA
LL
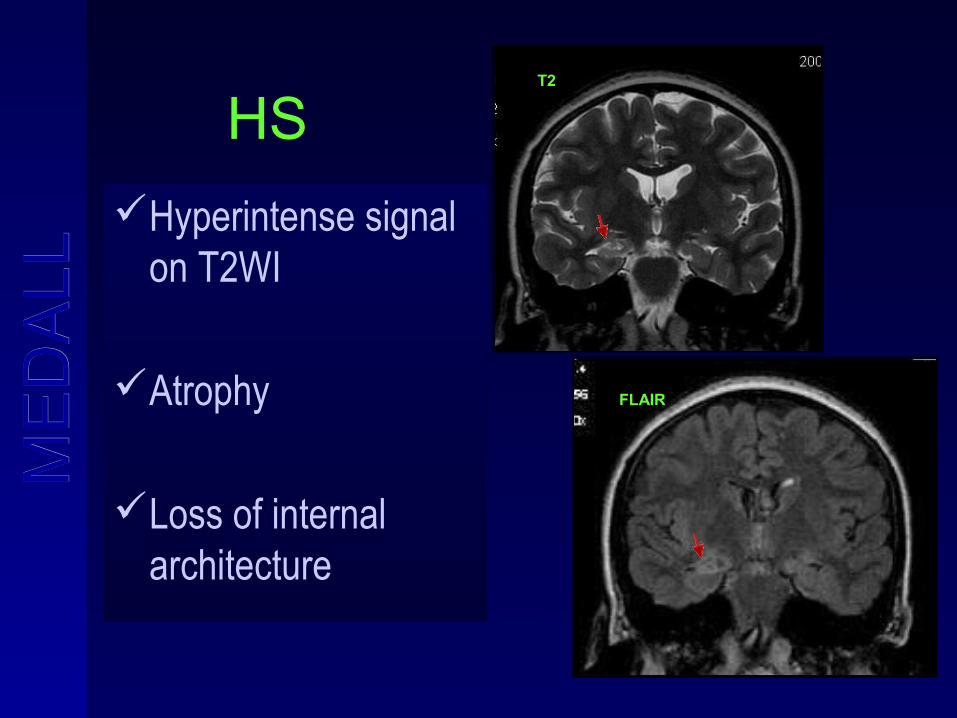
HS
Hyperintense signal on T2WI
Atrophy
Loss of internal architecture
FLAIR
T2
ME
DA
LL
ME
DA
LL
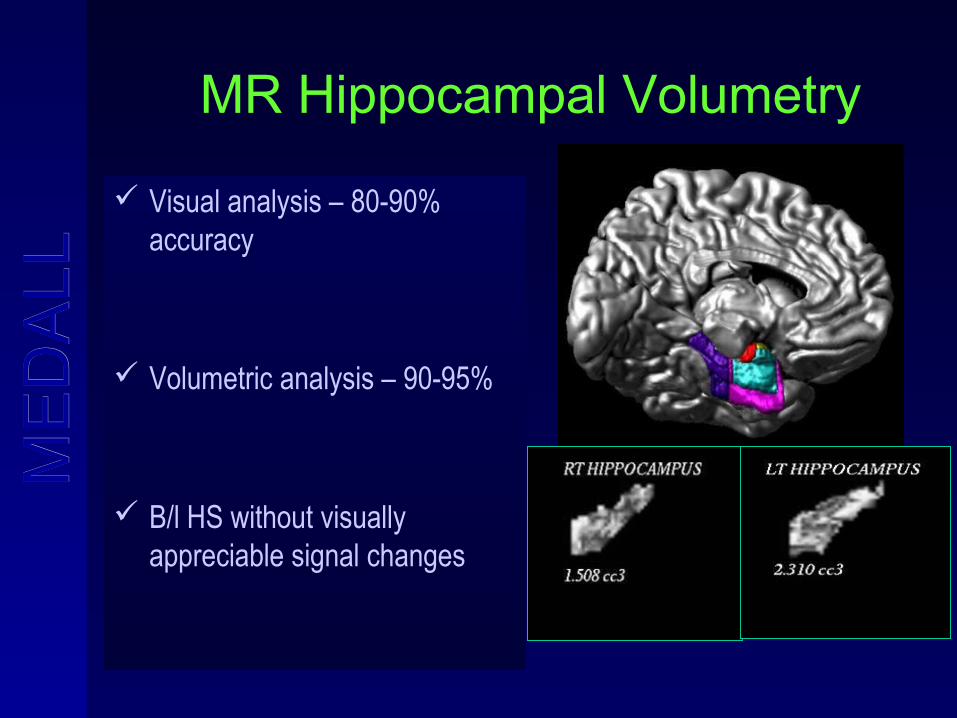
MR Hippocampal Volumetry
Visual analysis – 80-90% accuracy
Volumetric analysis – 90-95%
B/l HS without visually appreciable signal changes
ME
DA
LL
ME
DA
LL
Epilepsy associated tumors
Ganglioglioma – MC tumor of temporal lobe epilepsy
DNET
Pleomorphic xanthoastrocytoma
Hypothalamic hamartoma
MR has 100% sensitivity
ME
DA
LL
ME
DA
LL
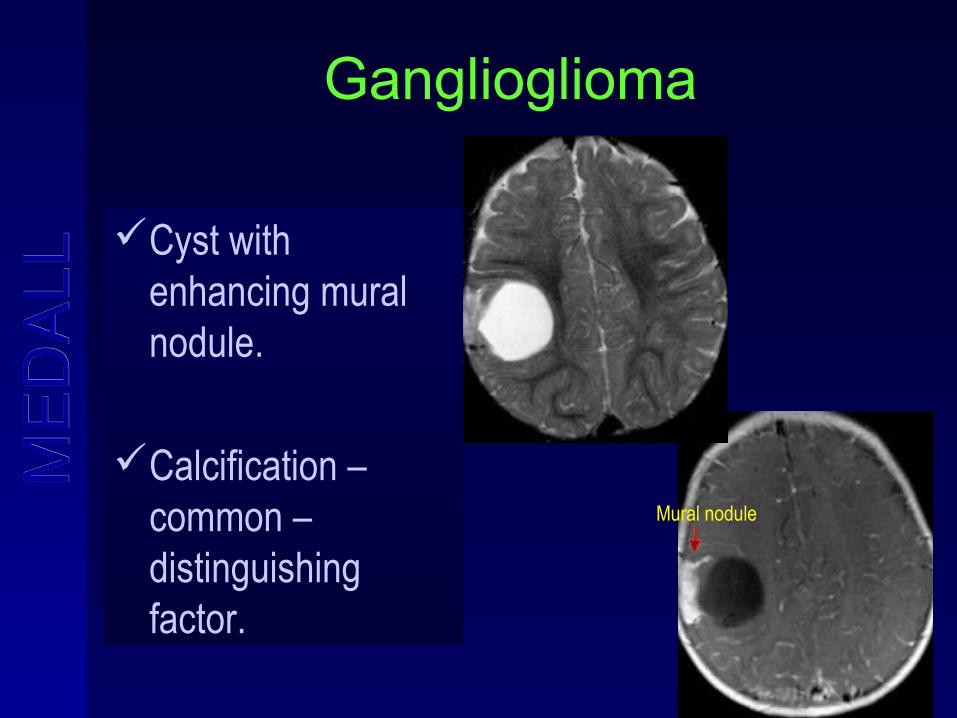
Ganglioglioma
Cyst with enhancing mural nodule.
Calcification – common – distinguishing factor.
Mural nodule
ME
DA
LL
ME
DA
LL
Vascular malformations
AVMCavernous angioma
MR has 100% sensitivity
ME
DA
LL
ME
DA
LL
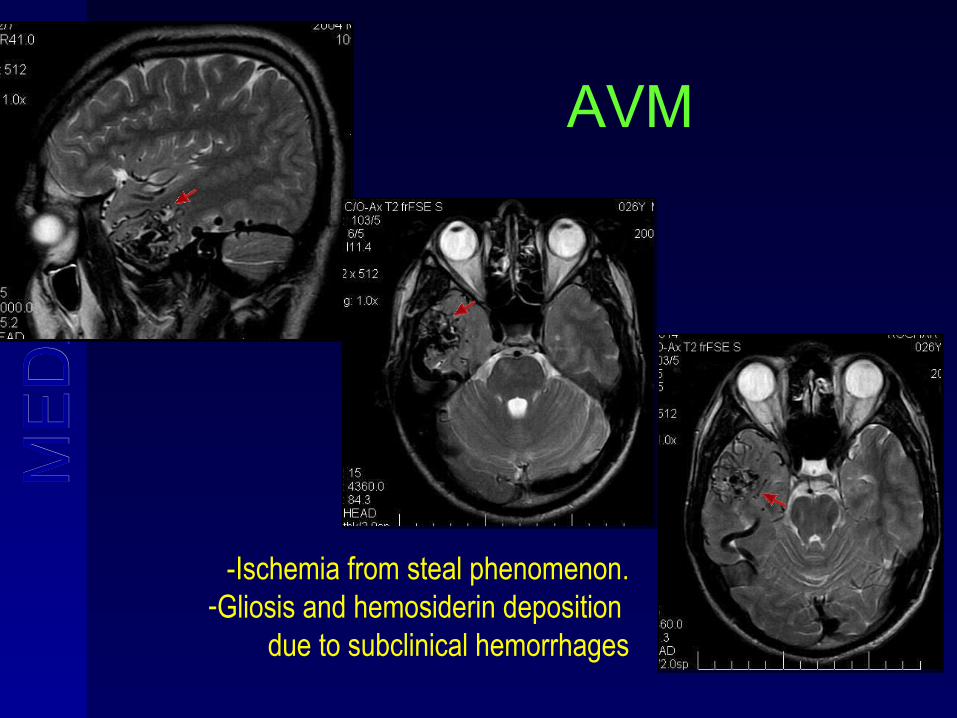
AVM
-Ischemia from steal phenomenon.-Gliosis and hemosiderin deposition
due to subclinical hemorrhages
ME
DA
LL
ME
DA
LL
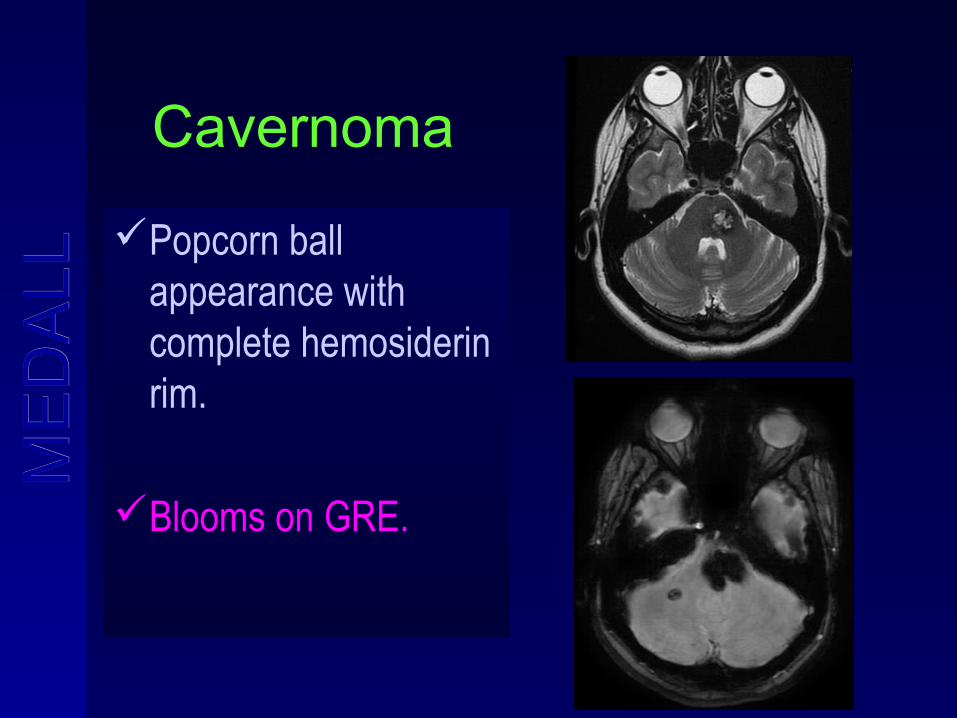
Cavernoma
Popcorn ball appearance with complete hemosiderin rim.
Blooms on GRE.
ME
DA
LL
ME
DA
LL
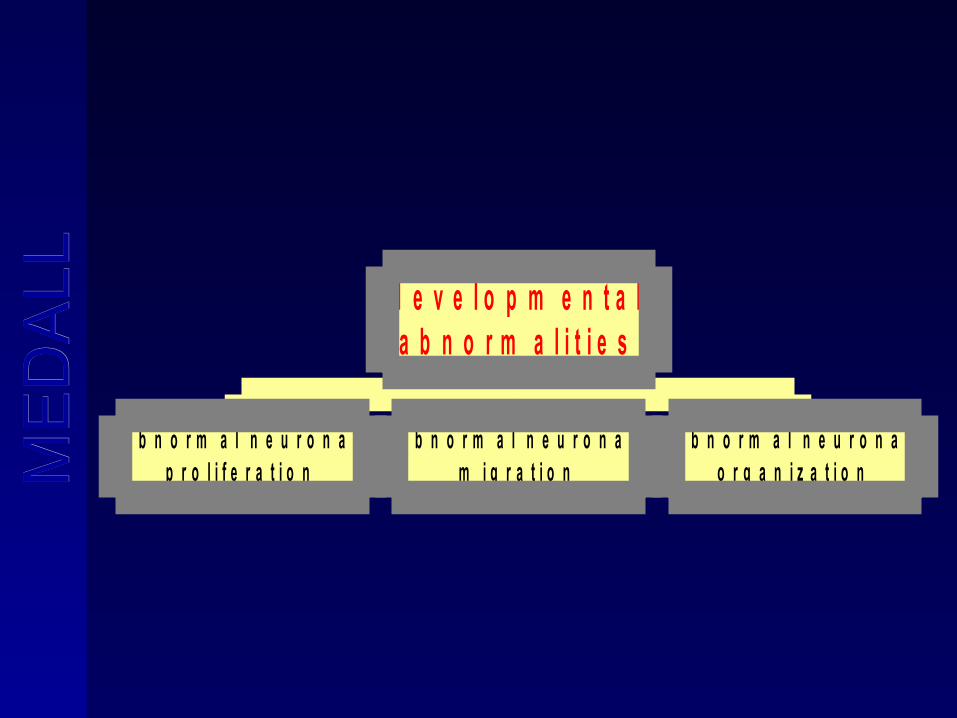
a b n o r m a l n e u r o n a lp r o l i f e r a t i o n
a b n o r m a l n e u r o n a lm i g r a t i o n
a b n o r m a l n e u r o n a lo r g a n i z a t i o n
d e v e l o p m e n t a la b n o r m a l i t i e s
ME
DA
LL
ME
DA
LL
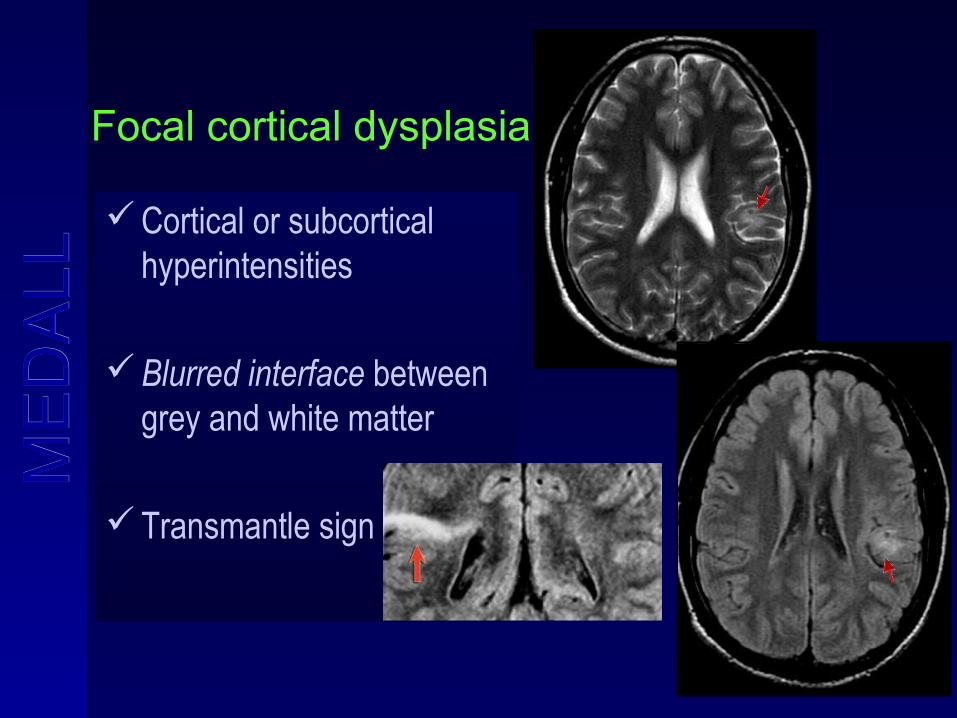
Focal cortical dysplasia
Cortical or subcortical hyperintensities
Blurred interface between grey and white matter
Transmantle sign
ME
DA
LL
ME
DA
LL
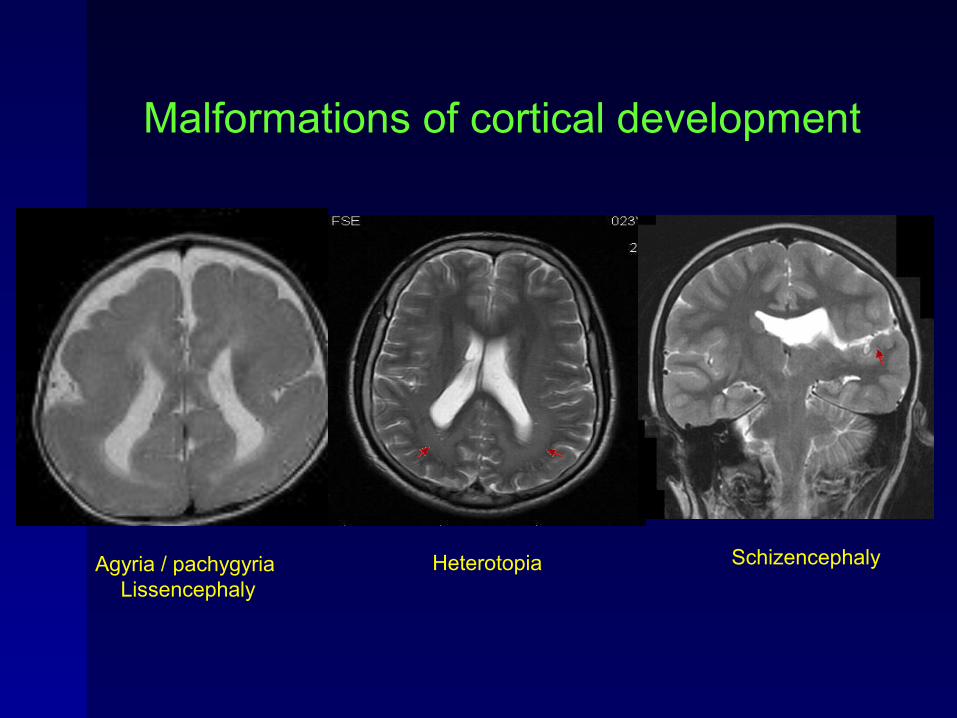
HeterotopiaAgyria / pachygyria Lissencephaly
Schizencephaly
Malformations of cortical development
ME
DA
LL
ME
DA
LL
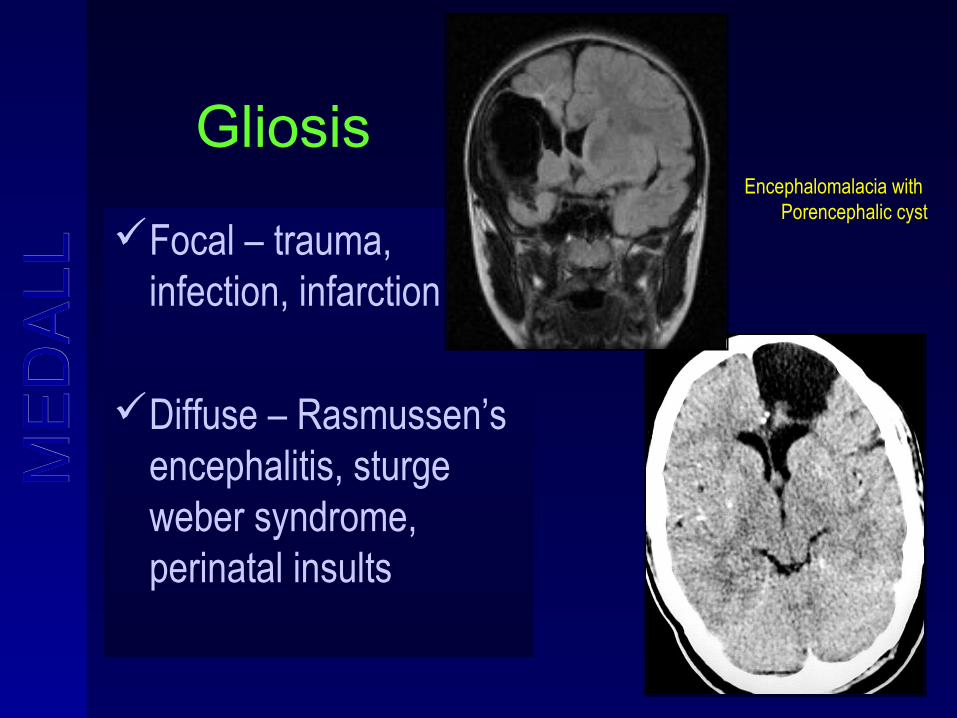
Gliosis
Focal – trauma, infection, infarction
Diffuse – Rasmussen’s encephalitis, sturge weber syndrome, perinatal insults
Encephalomalacia with Porencephalic cyst
ME
DA
LL
ME
DA
LL
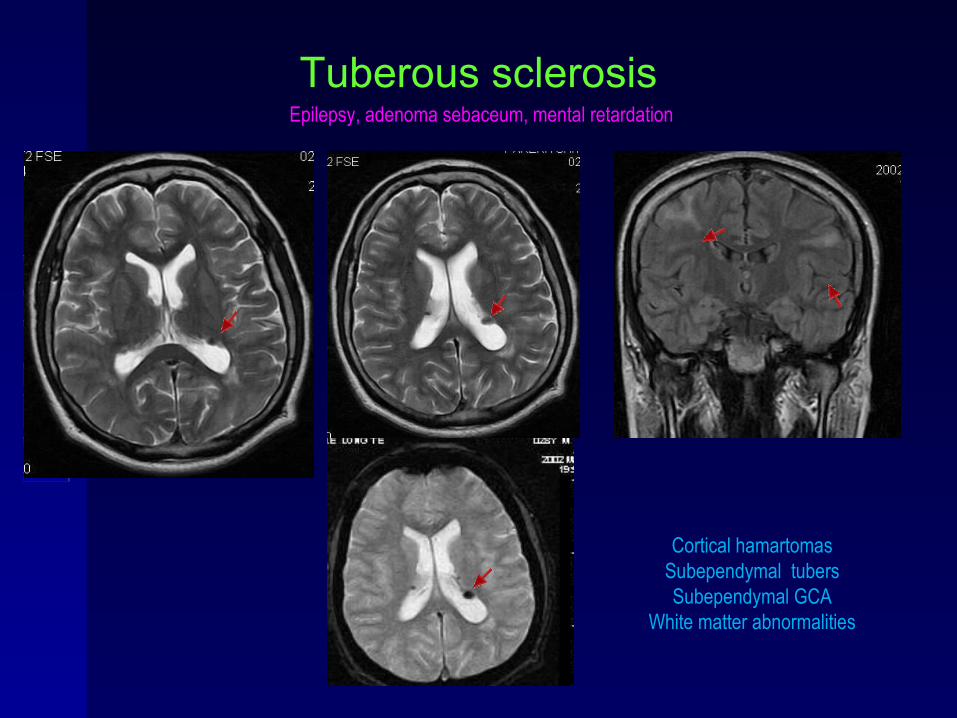
Tuberous sclerosis
Cortical hamartomasSubependymal tubersSubependymal GCA
White matter abnormalities
Epilepsy, adenoma sebaceum, mental retardation
ME
DA
LL
ME
DA
LL
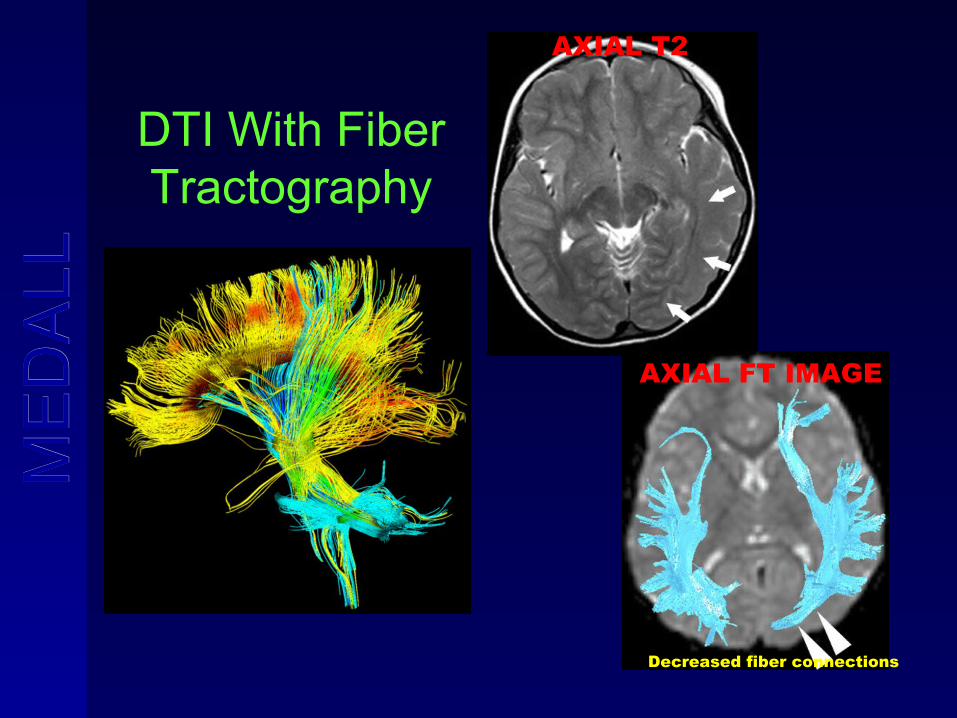
DTI With Fiber Tractography
Decreased fiber connections
AXIAL T2
AXIAL FT IMAGE
ME
DA
LL
ME
DA
LL
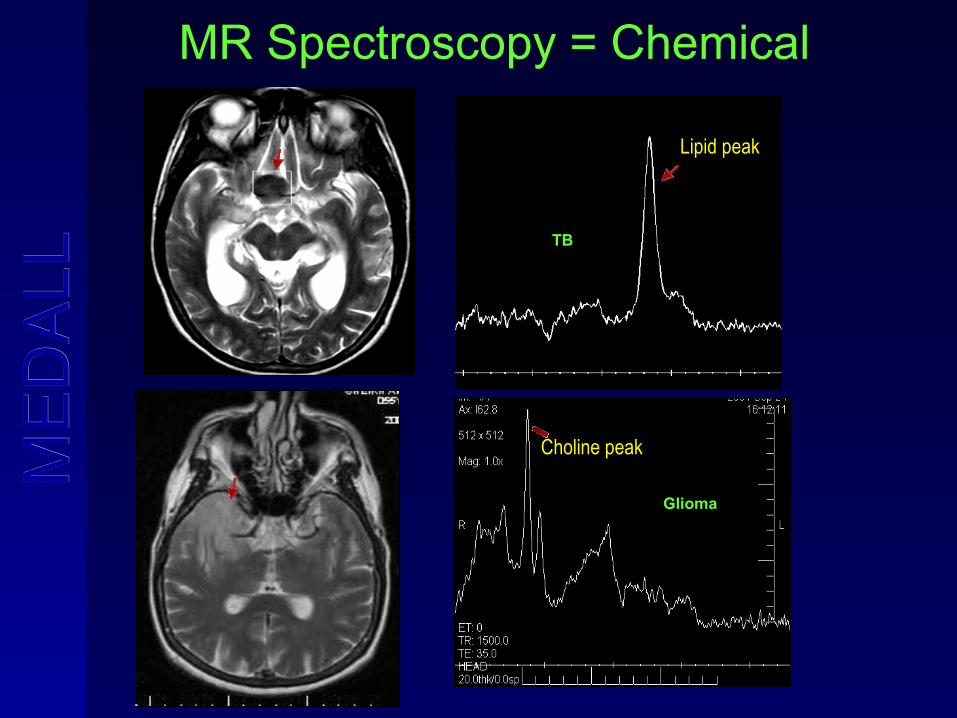
MR Spectroscopy = Chemical
Choline peak
Lipid peak
TB
Glioma
ME
DA
LL
ME
DA
LL
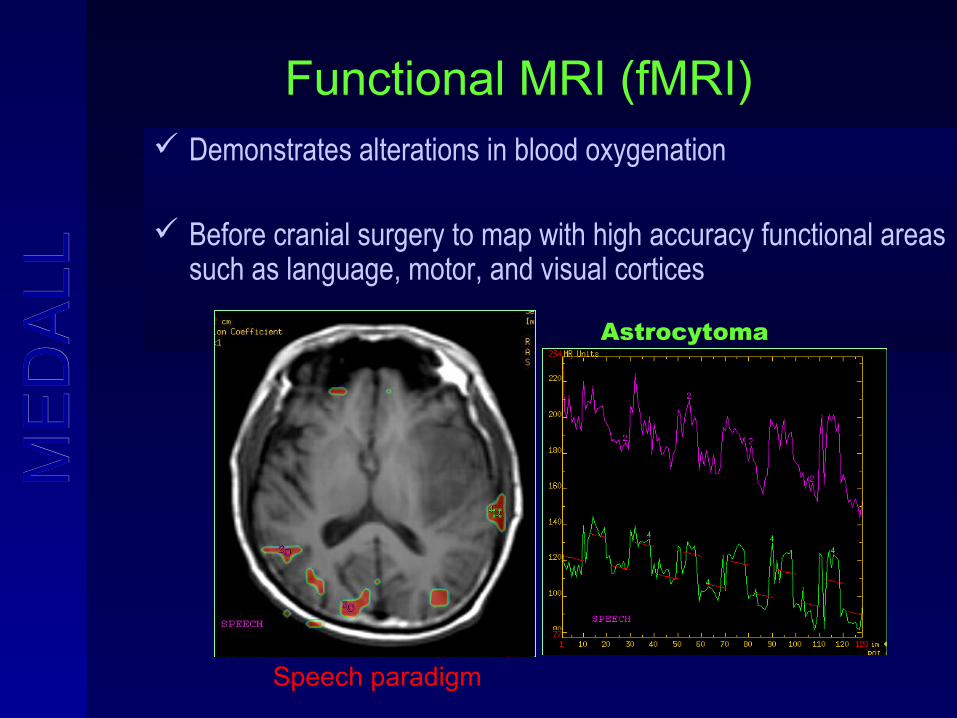
Functional MRI (fMRI) Demonstrates alterations in blood oxygenation
Before cranial surgery to map with high accuracy functional areas such as language, motor, and visual cortices
Speech paradigm
Astrocytoma
ME
DA
LL
ME
DA
LL
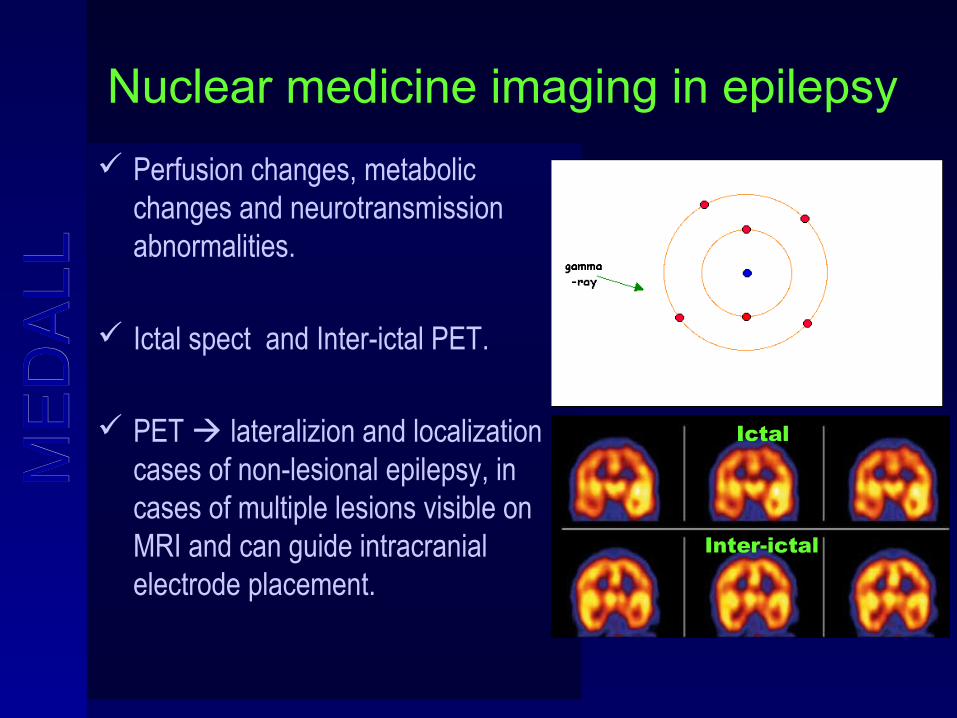
Nuclear medicine imaging in epilepsy
Perfusion changes, metabolic changes and neurotransmission abnormalities.
Ictal spect and Inter-ictal PET.
PET lateralizion and localization in cases of non-lesional epilepsy, in cases of multiple lesions visible on MRI and can guide intracranial electrode placement.
Ictal
Inter-ictal
ME
DA
LL
ME
DA
LL
PET MRI MRI = Anatomy
PET = Function
ME
DA
LL
ME
DA
LL
Lab tests
Metabolic and genetic abnormalities may manifest as seizures without any structural abnormality.
MRI = Normal in early infection.
CBC and the blood chemistry panel.
ME
DA
LL
ME
DA
LL
Complete blood count
Infections
Allergies
Other abnormalities that may affect the choice of appropriate anticonvulsant drugs
Help monitor the possible drug-induced side effects in the future.
ME
DA
LL
ME
DA
LL
Chemistry panel
Sodium, potassium, and blood sugar levels.
RFT & LFT = Complete metabolic panel.
ME
DA
LL
ME
DA
LL
Integrated Neuro diagnostics
EEG MRI LAB
ME
DA
LL
ME
DA
LL
to conclude…
MRI is excellent tool for imaging and for surgical planning.
Integrated neurodiagnostic approach is the most efficient method for evaluating patients with epilepsy.

ME
DA
LL
ME
DA
LL